
Long-Term Outcomes after Pelvic Organ Prolapse Repair in Young Women
 ,
, 
Abstract
1. Introduction
2. Materials and Methods
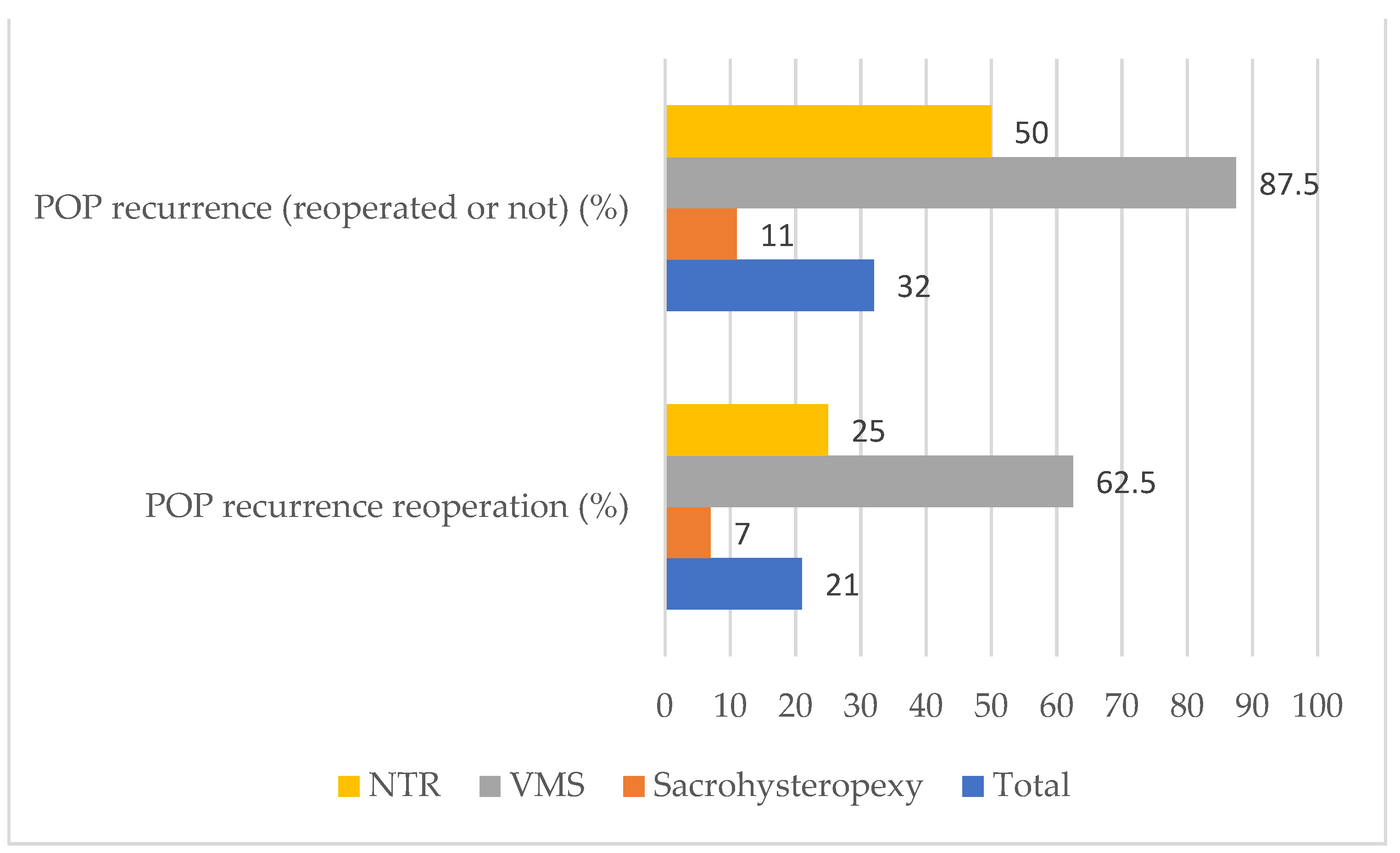
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nygaard, I.; Barber, M.D.; Burgio, K.L.; Kenton, K.; Meikle, S.; Schaffer, J.; Spino, C.; Whitehead, W.E.; Wu, J.; Brody, D.J.; et al. Prevalence of symptomatic pelvic floor disorders in US women. JAMA 2008, 300, 1311–1316. [Google Scholar] [CrossRef]
- Hickman, L.C.; Tran, M.C.; Davidson, E.R.W.; Walters, M.D.; Ferrando, C.A. Pelvic organ prolapse recurrence in young women undergoing vaginal and abdominal colpopexy. Int. Urogynecol. J. 2019, 31, 2661–2667. [Google Scholar] [CrossRef]
- Løwenstein, E.; Møller, L.A.; Laigaard, J.; Gimbel, H. Reoperation for pelvic organ prolapse: A Danish cohort study with 15–20 years’ follow-up. Int. Urogynecol. J. 2018, 29, 119–124. [Google Scholar] [CrossRef]
- Whiteside, J.L.; Weber, A.M.; Meyn, L.A.; Walters, M.D. Risk factors for prolapse recurrence after vaginal repair. Am. J. Obstet. Gynecol. 2004, 191, 1533–1538. [Google Scholar] [CrossRef]
- Barranger, E.; Fritel, X.; Pigne, A. Abdominal sacrohysteropexy in young women with uterovaginal prolapse: Long-term follow-up. Am. J. Obstet. Gynecol. 2003, 189, 1245–1250. [Google Scholar] [CrossRef]
- Shah, A.D.; Kohli, N.; Rajan, S.S.; Hoyte, L. The age distribution, rates, and types of surgery for pelvic organ prolapse in the USA. Int. Urogynecol. J. 2008, 19, 421–428. [Google Scholar] [CrossRef]
- Wattiez, A.; Canis, M.; Mage, G.; Pouly, J.; Bruhat, M. Promontofixation for the treatment of prolapse. Urol. Clin. North Am. 2001, 28, 151–157. [Google Scholar] [CrossRef]
- Cosson, M.; Rajabally, R.; Bogaert, E.; Querleu, D.; Crépin, G. Laparoscopic Sacrocolpopexy, Hysterectomy, and Burch Colposuspension: Feasibility and Short-Term Complications of 77 Procedures. JSLS J. Soc. Laparoendosc. Surg. 2002, 6, 115–119. [Google Scholar]
- Debodinance, G.T.P.; Berrocal, J.; Clave, H.; Cosson, M.; Garbin, O.; Jacquetin, B.; Rosenthal, C.; Saletlizee, D.; Villet, R. Changing attitudes on the surgical treatment of urogenital prolapse: Birth of the tension-free vaginal mesh]. J. Gynecol. Obstet. Biol. Reprod. 2004, 33, 577–588. [Google Scholar] [CrossRef]
- de Landsheere, L.; Ismail, S.; Lucot, J.-P.; Deken, V.; Foidart, J.-M.; Cosson, M. Surgical intervention after transvaginal Prolift mesh repair: Retrospective single-center study including 524 patients with 3 years’ median follow-up. Am. J. Obstet. Gynecol. 2012, 206, 83.e1–83.e7. [Google Scholar] [CrossRef]
- Baden, W.F.; Walker, T. Surgical Repair of Vaginal Defects; Lippincott: New York, NY, USA, 1992. [Google Scholar]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of Surgical Complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Maher, C.; Feiner, B.; Baessler, K.; Christmann-Schmid, C.; Haya, N.; Brown, J. Surgery for women with apical vaginal prolapse. Cochrane Database Syst. Rev. 2016, 10, CD012376. [Google Scholar] [CrossRef] [PubMed]
- Wagner, L.; Chevrot, A.; Llinares, E.; Costa, P.; Droupy, S. Long-term anatomic and functional results of laparoscopic sacrocolpopexy: A prospective study. Int. Urol. Nephrol. 2019, 51, 795–802. [Google Scholar] [CrossRef] [PubMed]
- Lucot, J.-P.; Cosson, M.; Verdun, S.; Debodinance, P.; Bader, G.; Campagne-Loiseau, S.; Salet-Lizee, D.; Akladios, C.; Ferry, P.; De Tayrac, R.; et al. Long-term outcomes of primary cystocele repair by transvaginal mesh surgery versus laparoscopic mesh sacropexy: Extended follow up of the PROSPERE multicentre randomised trial. BJOG: Int. J. Obstet. Gynaecol. 2021, 129, 127–137. [Google Scholar] [CrossRef] [PubMed]
- FDA. FDA Takes Action to Protect Women’s Health, Orders Manufacturers of Surgical Mesh Intended for Transvaginal Repair of Pelvic Organ Prolapse to Stop Selling All Devices. 2020. Available online: https://www.fda.gov/news-events/press-announcements/fda-takes-action-protect-womens-health-orders-manufacturers-surgical-mesh-intended-transvaginal (accessed on 11 September 2022).
- Campagna, G.; Vacca, L.; Panico, G.; Caramazza, D.; Lombisani, A.; Scambia, G.; Ercoli, A. Laparoscopic lateral suspension for pelvic organ prolapse: A systematic literature review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 264, 318–329. [Google Scholar] [CrossRef]
- Friedman, T.; Eslick, G.D.; Dietz, H.P. Risk factors for prolapse recurrence: Systematic review and meta-analysis. Int. Urogynecol. J. 2018, 29, 13–21. [Google Scholar] [CrossRef]
- van Lindert, A.C.; Groenendijk, A.G.; Scholten, P.C.; Heintz, A.P. Surgical support and suspension of genital prolapse, including preservation of the uterus, using the Gore-Tex soft tissue patch (a preliminary report). Eur. J. Obstet. Gynecol. Reprod. Biol. 1993, 50, 133–139. [Google Scholar] [CrossRef]
- Sun, Z.; Zhu, L.; Hu, H.; Lang, J.; Shi, H.; Gong, X. Medium-term outcomes after combined trachelectomy and uterosacral ligament suspension among young women with severe uterine prolapse. Int. J. Gynecol. Obstet. 2016, 132, 224–228. [Google Scholar] [CrossRef]
- Kovac, S.R.; Cruikshank, S.H. Successful pregnancies and vaginal deliveries after sacrospinous uterosacral fixation in five of nineteen patients. Am. J. Obstet. Gynecol. 1993, 168, 1778–1783, discussion 1783–1786. [Google Scholar] [CrossRef]
- Vergeldt, T.F.M.; Weemhoff, M.; IntHout, J.; Kluivers, K.B. Risk factors for pelvic organ prolapse and its recurrence: A systematic review. Int. Urogynecol. J. 2015, 26, 1559–1573. [Google Scholar] [CrossRef]
- VandenDriessche, D.; Sussfeld, J.; Giraudet, G.; Lucot, J.-P.; Behal, H.; Cosson, M. Complications and reoperations after laparoscopic sacrocolpopexy with a mean follow-up of 4 years. Int. Urogynecol. J. 2017, 28, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Visco, A.G.; Brubaker, L.; Nygaard, I.; Richter, H.E.; Cundiff, G.; Fine, P.; Zyczynski, H.; Brown, M.B.; Weber, A.M.; Network, P.F.D. The role of preoperative urodynamic testing in stress-continent women undergoing sacrocolpopexy: The Colpopexy and Urinary Reduction Efforts (CARE) randomized surgical trial. Int. Urogynecol. J. 2008, 19, 607–614. [Google Scholar] [CrossRef] [PubMed]
- De Tayrac, R.; Gervaise, A.; Chauveaud-Lambling, A.; Fernandez, H. Combined genital prolapse repair reinforced with a polypropylene mesh and tension-free vaginal tape in women with genital prolapse and stress urinary incontinence: A retrospective case-control study with short-term follow-up. Acta Obstet. Gynecol. Scand. 2004, 83, 950–954. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.T.; Nygaard, I.; Richter, H.E.; Nager, C.W.; Barber, M.D.; Kenton, K.; Amundsen, C.L.; Schaffer, J.; Meikle, S.F.; Spino, C. A Midurethral Sling to Reduce Incontinence after Vaginal Prolapse Repair. N. Engl. J. Med. 2012, 366, 2358–2367. [Google Scholar] [CrossRef] [PubMed]
- Ennemoser, S.; Schönfeld, M.; Von Bodungen, V.; Dian, D.; Friese, K.; Jundt, K. Clinical relevance of occult stress urinary incontinence (OSUI) following vaginal prolapse surgery: Long-term follow-up. Int. Urogynecol. J. 2012, 23, 851–855. [Google Scholar] [CrossRef]
- De Tayrac, R.; Sentilhes, L. Complications of pelvic organ prolapse surgery and methods of prevention. Int. Urogynecol. J. 2013, 24, 1859–1872. [Google Scholar] [CrossRef] [PubMed]
- Maher, C.; Feiner, B.; Baessler, K.; Christmann-Schmid, C.; Haya, N.; Brown, J. Surgery for women with anterior compartment prolapse. Cochrane Database Syst. Rev. 2016, 11, CD004014. [Google Scholar] [CrossRef]
- Dietz, V.; Maher, C. Pelvic organ prolapse and sexual function. Int. Urogynecol. J. 2013, 24, 1853–1857. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Population Characteristics | n = 43 |
|---|---|
| Age (years) | 35 ± 4 (28–40) |
| BMI (kg/m2) | 25.3 ± 5.3 (17.2–42) |
| Parity | 2 (0–6) |
| Length of followup (months) | 83 ± 52 (22–226) |
| POP stage (Baden and Walker classification) in at least one compartment: | |
| Stage 2 | 12 (28) |
| Stage ≥ 3 | 31 (72) |
| Type of POP repair | |
| Sacrohysteropexy | 28 (65) |
| Anterior and posterior meshes | 27 (96) |
| Posterior mesh only | 1 (4) |
| Laparoscopic surgery | 27 (96) |
| Laparotomy surgery | 1 (4) |
| Vaginal mesh surgery | 8 (19) |
| Anterior and posterior meshes | 3 (37.5) |
| Posterior mesh only | 5 (62.5) |
| Native tissue repair | 8 (19) |
| Posterior sacrospinofixation according to Richter | 1 (14) |
| Richardson’s procedure | 5 (71) |
| Posterior colporrhaphy and perineorrhaphy | 1 (14) |
| Concomitant total hysterectomy | 16 (37) |
| Associated SUI surgery | 11 (26) |
| Total n = 43 | Sacrohysteropexy n = 28 | VMS n = 8 | NTR n = 8 | |
|---|---|---|---|---|
| Intraoperative complications | 0 | |||
| Grade I and II | ||||
| Vaginal hematoma | 1 (2) | 0 | 1 (12.5) | 0 |
| Dyspareunia | 2 (4) | 1 (4%) | 1 (12.5) | 0 |
| Non-reoperated POP recurrence | 5 (12) | 1 (4%) | 2 (25) | 2 (25) |
| Mesh exposure | 1 (2) | 1 (12.5) | ||
| Grade III | ||||
| Global reoperation | 10 (23) | 2 (7) | 6 (75) | 2 (25) |
| POP recurrence reoperation | 9 (21) | 2 (7) | 5 (62.5) | 2 (25) |
| Mesh related reoperation | 1 (2) | 0 | 1 (12.5) | 0 |
| Grade IV or V | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lallemant, M.; Clermont-Hama, Y.; Giraudet, G.; Rubod, C.; Delplanque, S.; Kerbage, Y.; Cosson, M. Long-Term Outcomes after Pelvic Organ Prolapse Repair in Young Women. J. Clin. Med. 2022, 11, 6112. https://doi.org/10.3390/jcm11206112
Lallemant M, Clermont-Hama Y, Giraudet G, Rubod C, Delplanque S, Kerbage Y, Cosson M. Long-Term Outcomes after Pelvic Organ Prolapse Repair in Young Women. Journal of Clinical Medicine. 2022; 11(20):6112. https://doi.org/10.3390/jcm11206112
Chicago/Turabian StyleLallemant, Marine, Yasmine Clermont-Hama, Géraldine Giraudet, Chrystèle Rubod, Sophie Delplanque, Yohan Kerbage, and Michel Cosson. 2022. "Long-Term Outcomes after Pelvic Organ Prolapse Repair in Young Women" Journal of Clinical Medicine 11, no. 20: 6112. https://doi.org/10.3390/jcm11206112
APA StyleLallemant, M., Clermont-Hama, Y., Giraudet, G., Rubod, C., Delplanque, S., Kerbage, Y., & Cosson, M. (2022). Long-Term Outcomes after Pelvic Organ Prolapse Repair in Young Women. Journal of Clinical Medicine, 11(20), 6112. https://doi.org/10.3390/jcm11206112