

Transgender Males as Potential Donors for Uterus Transplantation: A Survey

 , ,
, , 
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Institutional Approval
2.2. Patient Population
2.3. The Survey
3. Results
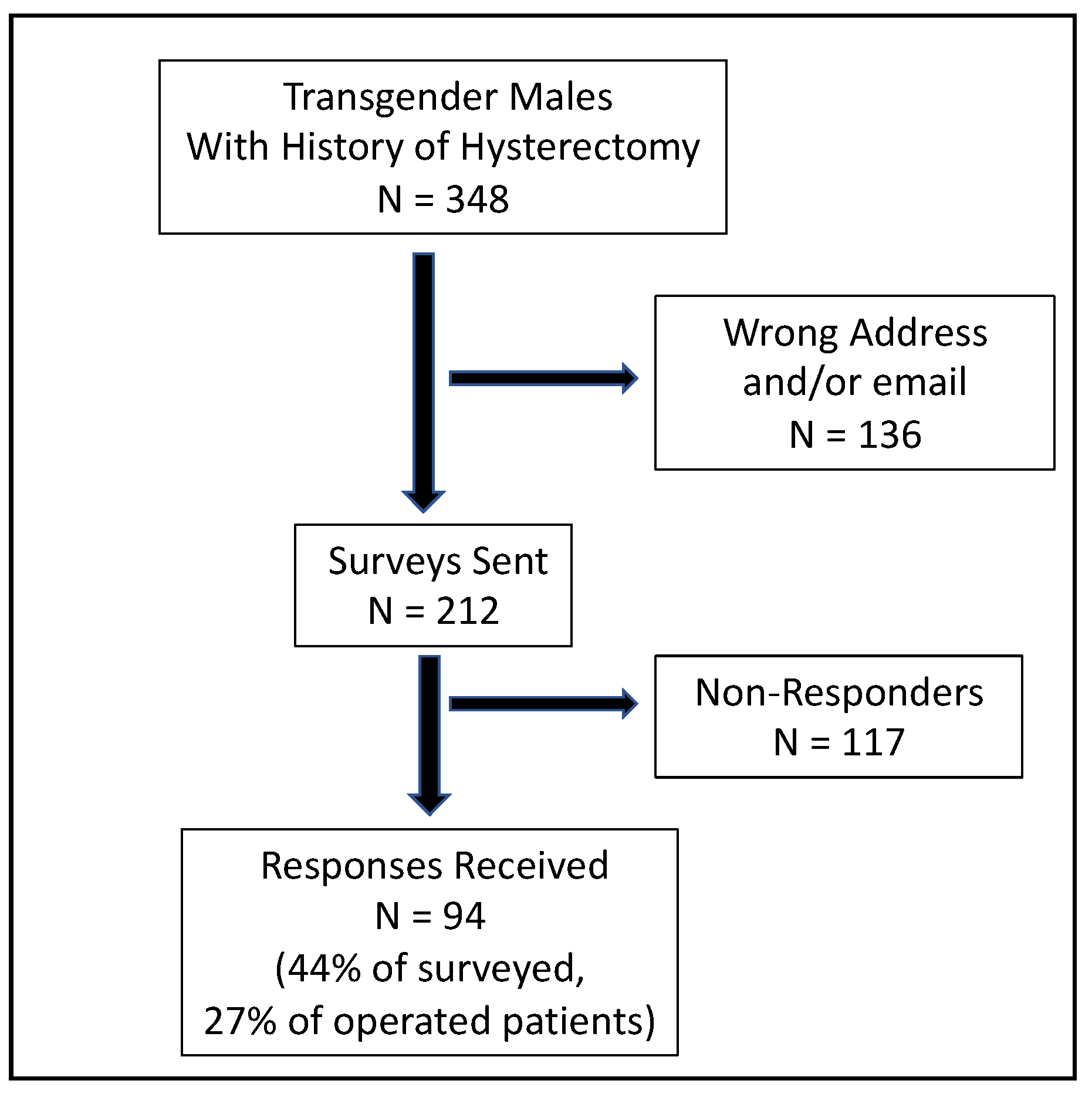
3.1. Response Rate
3.2. Marital and Family Stituation
3.3. Experience of the Hysterectomy
3.4. Willingness to Donate Their Uterus for Transplantation
- -
- Altruism:
- -
- The usefulness of the gesture:
- -
- The understanding of the desire for a child in a biological woman:
- -
- A counter-donation to sperm donation was mentioned by two respondents:
3.5. Gynecologic History
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sieunarine, K.; Zakaria, F.B.P.; Boyle, D.C.M.; Corless, D.J.; Noakes, D.E.; Lindsay, I.; Lawson, A.; Ungar, L.; Del Priores, G.; Smith, J.R. Possibilities for fertility restoration: A new surgical technique. Int. Surg. 2005, 90, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Ledig, S.; Wieacker, P. Clinical and genetic aspects of Mayer–Rokitansky–Küster–Hauser syndrome. Med. Genet. 2018, 30, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Brett, K.M.; Higgins, J.A. Hysterectomy Prevalence by Hispanic Ethnicity: Evidence from a National Survey. Am. J. Public Health 2003, 93, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Brännström, M.; Johannesson, L.; Bokström, H.; Kvarnström, N.; Mölne, J.; Dahm-Kähler, P.; Enskog, A.; Milenkovic, M.; Ekberg, J.; Diaz-Garcia, C.; et al. Livebirth after uterus transplantation. Lancet 2015, 385, 607–616. [Google Scholar] [CrossRef]
- Ayoubi, J.M.; Carbonnel, M.; Racowsky, C.; de Ziegler, D.; Gargiulo, A.; Kvarnstrom, N.; Dahm-Kahler, P.; Brannstrom, M. Evolving clinical challenges in uterus transplantation. Reprod. Biomed. Online, 2022; Online ahead of print. [Google Scholar] [CrossRef]
- Brännström, M.; Belfort, M.A.; Ayoubi, J.M. Uterus transplantation worldwide: Clinical activities and outcomes. Curr. Opin. Organ Transplant. 2021, 26, 616–626. [Google Scholar] [CrossRef]
- Brännström, M.; Johannesson, L.; Dahm-Kähler, P.; Enskog, A.; Mölne, J.; Kvarnström, N.; Diaz-Garcia, C.; Hanafy, A.; Lundmark, C.; Marcickiewicz, J.; et al. First clinical uterus transplantation trial: A six-month report. Fertil. Steril. 2014, 101, 1228–1236. [Google Scholar] [CrossRef]
- Carbonnel, M.; Revaux, A.; Menzhulina, E.; Karpel, L.; Snanoudj, R.; Le Guen, M.; De Ziegler, D.; Ayoubi, J.M. Uterus Transplantation with Live Donors: Screening Candidates in One French Center. J. Clin. Med. 2020, 9, 2001. [Google Scholar] [CrossRef]
- Johannesson, L.; Wallis, K.; Koon, E.C.; McKenna, G.J.; Anthony, T.; Leffingwell, S.G.; Klintmalm, G.B.; Gunby, R.T.; Testa, G. Living uterus donation and transplantation: Experience of interest and screening in a single center in the United States. Am. J. Obstet. Gynecol. 2018, 218, 331.e1–331.e7. [Google Scholar] [CrossRef]
- Fronek, J.; Kristek, J.; Chlupac, J.; Janousek, L.; Olausson, M. Human Uterus Transplantation from Living and Deceased Donors: The Interim Results of the First 10 Cases of the Czech Trial. J. Clin. Med. 2021, 10, 586. [Google Scholar] [CrossRef]
- Herman, J.L.; Flores, A.R.; Gates, G.J.; Bown, T.N.T. How Many Adults Dentify as Transgender in the United States? The Williams Institute: Los Angeles, CA, USA, 2016. [Google Scholar]
- Bretschneider, C.E.; Sheyn, D.; Pollard, R.; Ferrando, C.A. Complication Rates and Outcomes After Hysterectomy in Transgender Men. Obstet. Gynecol. 2018, 132, 1265–1273. [Google Scholar] [CrossRef]
- Api, M.; Boza, A.; Ceyhan, M. Could the female-to-male transgender population be donor candidates for uterus transplantation? J. Turk. Soc. Obstet. Gynecol. 2017, 14, 233–237. [Google Scholar] [CrossRef] [PubMed]
- Ayoubi, J.M.; Carbonnel, M.; Kvarnström, N.; Revaux, A.; Poulain, M.; Vanlieferinghen, S.; Coatantiec, Y.; Le Marchand, M.; Tourne, M.; Pirtea, P.; et al. Case Report: Post-Partum SARS-CoV-2 Infection After the First French Uterus Transplantation. Front. Surg. 2022, 9, 854225. [Google Scholar] [CrossRef] [PubMed]
- Bockting, W.; Coleman, E.; De Cuypere, G. Care of Transsexual Persons. N. Engl. J. Med. 2011, 364, 2559–2560. [Google Scholar] [CrossRef] [PubMed]
- James, S.H.J.; Rankin, S.; Keisling, M.; Mottet, L.; Ma’ayan, A. The Report of the 2015 U.S. Transgender Survey; National Center for Transgender Equality: Washington, DC, USA, 2016. [Google Scholar]
- Canner, J.K.; Harfouch, O.; Kodadek, L.M.; Pelaez, D.; Coon, D.; Offodile, A.C.; Haider, A.H.; Lau, B.D. Temporal Trends in Gender-Affirming Surgery Among Transgender Patients in the United States. JAMA Surg. 2018, 153, 609–616. [Google Scholar] [CrossRef]
- Available online: https://www.legifrance.gouv.fr/loda/id/JORFTEXT000033418805/ (accessed on 25 August 2022).
- Committee on Health Care for Underserved Women. Committee Opinion No. 512. Obstet. Gynecol. 2011, 118, 1454–1458. [Google Scholar] [CrossRef]
- Karpel, L.; Bremont-Weil, C.; Revol, M.; Brémont-Weil, C.; Ayoubi, J.-M.; Cordier, B. Le bien-être psycho-social post-opératoire de 207 transsexuels. Ann. Médico-Psychol. Rev. Psychiatr. 2015, 173, 511–519. [Google Scholar]
- Defreyne, J.; Van Schuylenbergh, J.; Motmans, J.; Tilleman, K.L.; T’Sjoen, G.G.R. Parental desire and fertility preservation in assigned female at birth transgender people living in Belgium. Fertil. Steril. 2020, 113, 149–157.e2. [Google Scholar] [CrossRef]
- Ethics Committee of the American Society for Reproductive Medicine. Access to fertility services by transgender persons: An Ethics Committee opinion. Fertil. Steril. 2015, 104, 1111–1115. [Google Scholar] [CrossRef]
- Coleman, E.; Bockting, W.; Botzer, M.; Cohen-Kettenis, P.; DeCuypere, G.; Feldman, J.; Fraser, L.; Green, J.; Knudson, G.; Meyer, W.J.; et al. Standards of Care for the Health of Transsexual, Transgender, and Gender-Nonconforming People, Version 7. Int. J. Transgenderism 2011, 13, 165–232. [Google Scholar] [CrossRef]
- Hembree, W.C.; Cohen-Kettenis, P.T.; Gooren, L.; Hannema, S.E.; Meyer, W.J.; Murad, M.H.; Rosenthal, S.M.; Safer, J.D.; Tangpricha, V.; T’Sjoen, G.G. Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society Clinical Practice Guideline. Endocr. Pract. 2017, 23, 1437. [Google Scholar] [CrossRef]
- De Wert, G.; Dondorp, W.; Shenfield, F.; Barri, P.; Devroey, P.; Diedrich, K.; Tarlatzis, B.; Provoost, V.; Pennings, G. ESHRE Task Force on Ethics and Law 23: Medically assisted reproduction in singles, lesbian and gay couples, and transsexual people. Hum. Reprod. 2014, 29, 1859–1865. [Google Scholar] [CrossRef] [PubMed]
- Křístek, J.; Johannesson, L.; Testa, G.; Chmel, R.; Olausson, M.; Kvarnström, N.; Karydis, N.; Fronek, J. Limited Availability of Deceased Uterus Donors: A Transatlantic Perspective. Transplantation 2019, 103, 2449–2452. [Google Scholar] [CrossRef]
- Johannesson, L.; Testa, G.; Putman, J.M.; McKenna, G.J.; Koon, E.C.; York, J.R.; Bayer, J.; Zhang, L.; Rubeo, Z.S.; Gunby, R.T.; et al. Twelve Live Births After Uterus Transplantation in the Dallas UtErus Transplant Study. Obstet. Gynecol. 2021, 137, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Carbonnel, M.; Karpel, L.; Cordier, B.; Pirtea, P.; Ayoubi, J.M. The uterus in transgender men. Fertil. Steril. 2021, 116, 931–935. [Google Scholar] [CrossRef] [PubMed]
- Voultsos, P.; Zymvragou, C.-E.; Karakasi, M.-V.; Pavlidis, P. A qualitative study examining transgender people’s attitudes towards having a child to whom they are genetically related and pursuing fertility treatments in Greece. BMC Public Health 2021, 21, 378. [Google Scholar] [CrossRef] [PubMed]
- Jones, B.P.; Williams, N.; Saso, S.; Thum, M.; Quiroga, I.; Yazbek, J.; Wilkinson, S.; Ghaem-Maghami, S.; Thomas, P.; Smith, J.R. Uterine transplantation in transgender women. BJOG Int. J. Obstet. Gynaecol. 2019, 126, 152–156. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carbonnel, M.; Karpel, L.; Corruble, N.; Legendri, S.; Pencole, L.; Cordier, B.; Racowsky, C.; Ayoubi, J.-M. Transgender Males as Potential Donors for Uterus Transplantation: A Survey. J. Clin. Med. 2022, 11, 6081. https://doi.org/10.3390/jcm11206081
Carbonnel M, Karpel L, Corruble N, Legendri S, Pencole L, Cordier B, Racowsky C, Ayoubi J-M. Transgender Males as Potential Donors for Uterus Transplantation: A Survey. Journal of Clinical Medicine. 2022; 11(20):6081. https://doi.org/10.3390/jcm11206081
Chicago/Turabian StyleCarbonnel, Marie, Léa Karpel, Ninon Corruble, Sophie Legendri, Lucile Pencole, Bernard Cordier, Catherine Racowsky, and Jean-Marc Ayoubi. 2022. "Transgender Males as Potential Donors for Uterus Transplantation: A Survey" Journal of Clinical Medicine 11, no. 20: 6081. https://doi.org/10.3390/jcm11206081
APA StyleCarbonnel, M., Karpel, L., Corruble, N., Legendri, S., Pencole, L., Cordier, B., Racowsky, C., & Ayoubi, J.-M. (2022). Transgender Males as Potential Donors for Uterus Transplantation: A Survey. Journal of Clinical Medicine, 11(20), 6081. https://doi.org/10.3390/jcm11206081