
Predictive Validity of Motor Fitness and Flexibility Tests in Adults and Older Adults: A Systematic Review

 ,
,  , , ,
, , ,  and
and
Abstract
1. Introduction
2. Methods
2.1. Selected Health Outcomes
2.2. Search Strategy
2.3. Selection Criteria
2.4. Data Extraction
2.5. Quality Assessment

{kind=link}
| Study | Fitness Components | Non-Selective Population | Clear Health Outcomes | PF and Health Measurement >1 Year | Confounders | SE/CI Information | Total Score |
|---|---|---|---|---|---|---|---|
| Abu et al., 2018 [31] | Motor fitness (Speed) | 1 | 1 | 0 | 0 | 1 | 3 |
| Brach et al., 2012 [32] | Motor fitness (Speed) | 1 | 1 | 0 | 0 | 1 | 3 |
| Sakurai et al., 2017 [33] | Motor fitness (Speed) | 1 | 1 | 0 | 0 | 1 | 3 |
| Dargent-Molina et al., 1999 [34] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 0 | 4 |
| Doi et al., 2013 [35] | Motor fitness (Speed) | 1 | 1 | 0 | 1 | 1 | 4 |
| Kang et al., 2017 [36] | Motor fitness (Speed) | 1 | 1 | 0 | 1 | 1 | 4 |
| Kauppi et al., 2014 [37] | Motor fitness (Speed) | 1 | 1 | 0 | 1 | 1 | 4 |
| Laukkanen et al., 2000 [38] | Motor fitness (Speed) | 1 | 1 | 1 | 0 | 1 | 4 |
| Makizako et al., 2015 [39] | Motor fitness (Speed) | 1 | 1 | 1 | 0 | 1 | 4 |
| Abe et al., 2019 [40] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Adachi et al., 2019 [41] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Andrasfay et al., 2020 [3] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Blain et al., 2010 [42] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Briggs et al., 2019 [43] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Buracchio et al., 2010 [44] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Callisaya et al., 2016 [7] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Camargo et al., 2016 [45] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Deshpande et al., 2013 [46] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Doi et al., 2020 [47] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Elbaz et al., 2013 [48] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Georgiopoulou et al., 2016 [49] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Heiland et al., 2018 [11] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Hoogendijk et al., 2020 [50] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Idland et al., 2013 [51] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Jung et al., 2018 [52] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Lee et al., 2017 [12] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Looker et al., 2015 [53] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Luukinen et al., 1995 [54] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Makizako et al., 2010 [55] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Muraki et al., 2013 [9] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Nakamoto et al., 2015 [56] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Niiranen et al., 2019 [57] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Nofuji et al., 2016 [58] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Ojagbemi et al., 2015 [59] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Osuka et al., 2020 [60] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Quach et al., 2011 [8] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Rosso et al., 2019 [61] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Sabia et al., 2014 [62] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Sanders et al., 2012 [63] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Sanders et al., 2016 [64] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Stenhagen et al., 2013 [6] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Stijntjes et al., 2017 [65] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Tian et al., 2019 [66] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Veronese et al., 2017 [67] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Veronese et al., 2017b [68] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Ward et al., 2016 [69] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Wihlborg et al., 2015 [70] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Zucchelli et al., 2019 [71] | Motor fitness (Speed) | 1 | 1 | 1 | 1 | 1 | 5 |
| Pajala et al., 2008 [72] | Motor fitness (Balance) | 1 | 1 | 0 | 0 | 1 | 3 |
| Austin et al., 2007 [73] | Motor fitness (Balance) | 1 | 1 | 1 | 0 | 1 | 4 |
| Ersoy et al., 2009 [74] | Motor fitness (Balance) | 1 | 1 | 0 | 1 | 1 | 4 |
| Frames et al., 2018 [75] | Motor fitness (Balance) | 1 | 1 | 1 | 0 | 1 | 4 |
| Maki et al., 1994 [76] | Motor fitness (Balance) | 1 | 1 | 0 | 1 | 1 | 4 |
| Muir et al., 2010 [77] | Motor fitness (Balance) | 1 | 1 | 0 | 1 | 1 | 4 |
| Mulasso et al., 2017 [78] | Motor fitness (Balance) | 1 | 1 | 0 | 1 | 1 | 4 |
| Swanenburg et al., 2010 [79] | Motor fitness (Balance) | 1 | 1 | 0 | 1 | 1 | 4 |
| Blain et al., 2010 [42] | Motor fitness (Balance) | 1 | 1 | 1 | 1 | 1 | 5 |
| Breton et al., 2014 [80] | Motor fitness (Balance) | 1 | 1 | 1 | 1 | 1 | 5 |
| Bullain et al., 2016 [81] | Motor fitness (Balance) | 1 | 1 | 1 | 1 | 1 | 5 |
| Cooper et al., 2014 [16] | Motor fitness (Balance) | 1 | 1 | 1 | 1 | 1 | 5 |
| Idland et al., 2013 [51] | Motor fitness (Balance) | 1 | 1 | 1 | 1 | 1 | 5 |
| Kwan et al., 2012 [82] | Motor fitness (Balance) | 1 | 1 | 1 | 1 | 1 | 5 |
| Luukinen et al., 1995 [54] | Motor fitness (Balance) | 1 | 1 | 1 | 1 | 1 | 5 |
| Makizako et al., 2010 [55] | Motor fitness (Balance) | 1 | 1 | 1 | 1 | 1 | 5 |
| Nakamoto et al., 2015 [56] | Motor fitness (Balance) | 1 | 1 | 1 | 1 | 1 | 5 |
| Nitz et al., 2013 [83] | Motor fitness (Balance) | 1 | 1 | 1 | 1 | 1 | 5 |
| Nofuji et al., 2016 [58] | Motor fitness (Balance) | 1 | 1 | 1 | 1 | 1 | 5 |
| Vellas et al., 1997 [84] | Motor fitness (Balance) | 1 | 1 | 1 | 1 | 1 | 5 |
| Wihlborg et al., 2015 [70] | Motor fitness (Balance) | 1 | 1 | 1 | 1 | 1 | 5 |
| Abu et al., 2018 [31] | Motor fitness (Speed–agility) | 1 | 1 | 0 | 0 | 1 | 3 |
| Sakurai et al., 2017 [33] | Motor fitness (Speed–agility) | 1 | 1 | 0 | 0 | 1 | 3 |
| Austin et al., 2007 [73] | Motor fitness (Speed–agility) | 1 | 1 | 1 | 0 | 1 | 4 |
| Clemson et al., 2015 [85] | Motor fitness (Speed–agility) | 1 | 1 | 1 | 0 | 1 | 4 |
| Davis et al., 2015 [86] | Motor fitness (Speed–agility) | 1 | 1 | 0 | 1 | 1 | 4 |
| Doi et al., 2013 [35] | Motor fitness (Speed–agility) | 1 | 1 | 0 | 1 | 1 | 4 |
| Ersoy et al., 2009 [74] | Motor fitness (Speed–agility) | 1 | 1 | 0 | 1 | 1 | 4 |
| Kang et al., 2017 [36] | Motor fitness (Speed–agility) | 1 | 1 | 0 | 1 | 1 | 4 |
| Mulasso et al., 2017 [78] | Motor fitness (Speed–agility) | 1 | 1 | 0 | 1 | 1 | 4 |
| Asai et al., 2020 [87] | Motor fitness (Speed–agility) | 1 | 1 | 1 | 1 | 1 | 5 |
| Breton et al., 2014 [80] | Motor fitness (Speed–agility) | 1 | 1 | 1 | 1 | 1 | 5 |
| Doi et al., 2019 [88] | Motor fitness (Speed–agility) | 1 | 1 | 1 | 1 | 1 | 5 |
| Donoghue et al., 2017 [89] | Motor fitness (Speed–agility) | 1 | 1 | 1 | 1 | 1 | 5 |
| Kwan et al., 2012 [82] | Motor fitness (Speed–agility) | 1 | 1 | 1 | 1 | 1 | 5 |
| Nitz et al., 2013 [83] | Motor fitness (Speed–agility) | 1 | 1 | 1 | 1 | 1 | 5 |
| Savva et al., 2013 [90] | Motor fitness (Speed–agility) | 1 | 1 | 1 | 1 | 1 | 5 |
| Schroll et al., 1997 [91] | Motor fitness (Speed–agility) | 1 | 1 | 1 | 1 | 1 | 5 |
| Bravell et al., 2017 [92] | Flexibility | 1 | 1 | 1 | 1 | 1 | 5 |
| Luukinen et al., 1995 [54] | Flexibility | 1 | 1 | 1 | 1 | 1 | 5 |
| Ward et al., 2016 [69] | Flexibility | 1 | 1 | 1 | 1 | 1 | 5 |
| Reviews | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Rating | Quality * |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Van Kan et al., (2009) [15] | Yes | Yes | No | No | No | Yes | Yes | Yes | No | N/A | Yes | 6 | Medium |
| Grande et al., (2019) [26] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | No | N/A | Yes | 8 | High |
| Cavanaugh et al., (2018) [14] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | N/A | Yes | 9 | High |
| Wang et al., (2020) [27] | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Yes | Yes | 9 | High |
| Quan et al., (2017) [24] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | 10 | High |
| Peel et al., (2019) [25] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | 10 | High |
2.6. Levels of Evidence
3. Results4
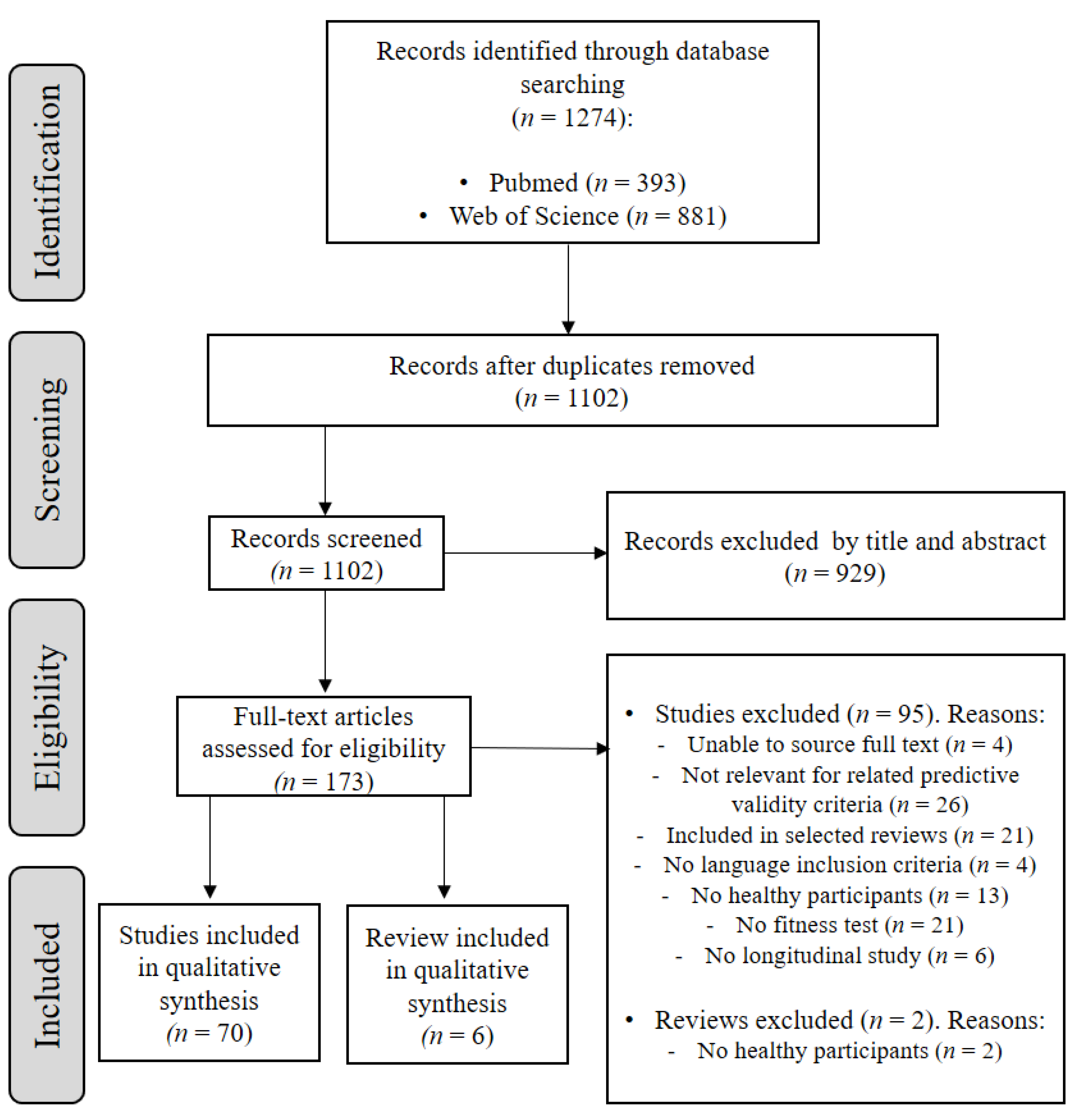
3.1. Study Selection
3.2. Risk of Bias within Studies
3.3. Characteristic of Included Studies
| Author | N (% Female Sex) | Mean (Range) Age | Fitness Test | Health Outcomes | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Gait Speed | Balance | TUG | Flexibility | Other | Falls/Hip fracture | Cognitive Decline/ Impairment | Depression/ Well-Being | Related-Mobility Disability/ Frailty | CVD/Stroke | All-Cause Mortality | Other-Causes Mortality | |||
| Kang et al. 2017 [36] | 541 (57) | 67 (60–86) |  |  | | |||||||||
| Quach et al., 2011 [8] | 763 (64) | 78 | | | ||||||||||
| Callisaya et al., 2016 [7] | 509 (52) | 75 (60–105) | | | ||||||||||
| Abu et al., 2018 [31] | 325 (55) | 68 (60–89) | | | | |||||||||
| Kwan et al., 2012 [82] | 280 (43) | 75 (65–91) | | | | | ||||||||
| Muraki et al., 2013 [9] | 2215 (66) | 68 | | | ||||||||||
| Sanders et al., 2016 [64] | 4112 (53) | 74 (≥65) |  | | | | ||||||||
| Luukinen et al., 1995 [54] | 1016 (63) | 76 (70–92) | | | | | | |||||||
| Doi et al., 2013 [35] | 57 (74) | 80 (≥65) | | | | |||||||||
| Stenhagen et al., 2013 [6] | 1763 (48) | 76 (60–93) | | | ||||||||||
| Dargent-Molina et al., 1999 [34] | 5895 (100) | 80 (≥75) | | | ||||||||||
| Kauppi et al., 2014 [37] | 2300 (58) | 66 (≥55) | | | ||||||||||
| Wihlborg et al., 2015 [70] | 1044 (100) | 75 | | | | |||||||||
| Ersoy et al., 2009 [74] | 125 (100) | 61 (50–79) | | | | |||||||||
| Muir et al., 2010 [77] | 90 (37) | 80 (60–90) | | | ||||||||||
| Austin et al., 2007 [73] | 1282 (100) | 75 (70–85) | | | | |||||||||
| Vellas et al., 1997 [84] | 267 (58) | 73 (≥60) | | | ||||||||||
| Mulasso et al., 2017 [78] | 19 (62) | 73 (≥65) | | | | |||||||||
| Nitz et al., 2013 [83] | 449 (100) | 59 (40–80) | | | | |||||||||
| Swanenburg et al., 2010 [79] | 270 (83) | 73 (60–90) | | | ||||||||||
| Maki et al., 1994 [76] | 100 (83) | 83 (62–96) | | | ||||||||||
| Pajala et al., 2008 [72] | 434 (100) | 70 (63–76) | | | ||||||||||
| Frames et al., 2018 [75] | 98 (66) | 75 | | | ||||||||||
| Asai et al., 2020 [87] | 649 (65) | 76 (≥60) | | | ||||||||||
| Clemson et al., 2015 [85] | 1000 (53) | 73 (65–94) | | | ||||||||||
| Doi et al., 2020 [47] | 3696 (53) | 71 (≥65) | | | ||||||||||
| Makizako et al., 2015 [39] | 948 (49) | 78 (≥75) | | | ||||||||||
| Heiland et al., 2018 [11] | 1756 (66) | 71 (≥60) | | | * | |||||||||
| Abe et al., 2019 [40] | 973 (48) | 75 (≥65) | | | | |||||||||
| Makizako et al., 2010 [55] | 265 (55) | 79 (68–96) | | | * | |||||||||
| Adachi et al., 2019 [41] | 516 (81) | 79 (76–82) | | | | |||||||||
| Laukkanen et al., 2000 [38] | 388 (67) | 77 (75–80) | | | ||||||||||
| Nakamoto et al., 2015 [56] | 961 (48) | 60 (40–79) | | * | | |||||||||
| Brach et al., 2012 [32] | 552 (61) | 79 (≥65) | | | ||||||||||
| Deshpande et al., 2013 [46] | 622 (?) | 67 (50–85) | | | ||||||||||
| Rosso et al., 2019 [61] | 337 (51) | 78 (70–79) | | | ||||||||||
| Jung et al., 2018 [52] | 1348 (55) | 76 (≥65) | | | | |||||||||
| Breton et al., 2014 [80] | 1265 (52) | 73 (68–82) | | | | | ||||||||
| Ward et al., 2016 [69] | 391 (67) | 77 (≥65) | | | | |||||||||
| Savva et al., 2013 [90] | 1814 (51) | 70 (≥65) | | | ||||||||||
| Schroll et al., 1997 [91] | 259 (56) | 77 (75–80) | | * | ||||||||||
| Elbaz et al., 2013 [48] | 6267 (29) | 45 (35–55) | | | ||||||||||
| Zucchelli et al., 2019 [71] | 3363 (65) | 75 (≥60) | | | ||||||||||
| Andrasfay et al., 2020 [3] | 887 (48) | 70 (≥60) | | | ||||||||||
| Niiranen et al., 2019 [57] | 3453 (54) | 55 (45–74) | | | ||||||||||
| Hoogendijk et al., 2020 [50] | 4220 (53) | 72 (≥55) | | | ||||||||||
| Nofuji et al., 2016 [58] | 1085 (?) | 77 (65–89) | | | | | | |||||||
| Lee et al., 2017 [12] | 911 (45) | 65 | | | | |||||||||
| Blain et al., 2010 [42] | 1548 (100) | 79 (77–81) | | | | |||||||||
| Sabia et al., 2014 [62] | 4016 (?) | 73 (65–85) | | | ||||||||||
| Georgiopoulou et al., 2016 [49] | 2935 (52) | 74 (70–79) | | | | |||||||||
| Idland et al., 2013 [51] | 113 (100) | 79 (75–92) | | | | | ||||||||
| Camargo et al., 2016 [45] | 2176 (54) | 63 (35–84) | | | ||||||||||
| Looker 2015 [53] | 2975 (49) | ≥50 | | | ||||||||||
| Cooper et al., 2014 [16] | 2766 (51) | 53 | | | ||||||||||
| Bravell et al., 2017 [92] | 585 (59) | 67 (60–91) | | | ||||||||||
| Ojagbemi et al., 2015 [59] | 2179 (?) | ≥65 | | | ||||||||||
| Stijntjes et al., 2017 [65] | 2979 (55) | 72 (55–90) | | * | ||||||||||
| Osuka et al., 2020 [60] | 725 (62) | 77 (73–80) | | | ||||||||||
| Tian et al., 2019 [66] | 201 (46) | 79 | | | ||||||||||
| Buracchio et al., 2010 [44] | 204 (58) | 79 (≥65) | | | ||||||||||
| Sakurai et al., 2017 [33] | 223 (48) | 73 (65–85) | | | ||||||||||
| Bullain et al., 2016 [81] | 578 (70) | 93 (≥90) | | | ||||||||||
| Doi et al., 2019 [88] | 4086 (52) | 72 (≥65) | | | ||||||||||
| Donoghue et al., 2017 [89] | 2250 (52) | 72 (65–98) | | | ||||||||||
| Briggs et al., 2019 [43] | 3615 (?) | 63 (≥50) | | | ||||||||||
| Veronese et al., 2017 [67] | 1732 (28) | 69 (≥50) | | | ||||||||||
| Veronese et al., 2017b [68] | 970 (55) | 72 (65–96) | | * | ||||||||||
| Sanders et al., 2012 [63] | 1459 (47) | 69 (≥65) | | * | ||||||||||
| Davis et al., 2015 [86] | 308 (63) | ≥70 | | | ||||||||||
= significant association; = not associated or non-significant association; = association found only in some outcomes. ? = female and male sample size are presented together. 3.4. Predictive Validity for Falls and Fall-Related Outcomes
3.4.1. Gait Speed Tests
3.4.2. Postural Balance Tests
3.4.3. Multidimensional Measurement Tests
3.4.4. Flexibility Tests
3.5. Predictive Validity for Cognitive Decline and Impairment
3.5.1. Gait Speed Tests
3.5.2. Postural Balance Tests
3.5.3. Multidimensional Measurements
3.6. Predictive Validity for Depressive Symptoms and Well-Being
3.6.1. Gait Speed Tests
3.6.2. Multidimensional Measurement Tests
3.7. Predictive Validity for Mobility Limitations, Disability and Frailty
3.7.1. Gait Speed Tests
3.7.2. Postural Balance Tests
3.7.3. Multidimensional Measurement Tests
3.7.4. Flexibility Tests
3.7.5. Other Tests
3.8. Predictive Validity for Cardiovascular Disease Risk and Mortality
3.8.1. Gait Speed Tests
3.8.2. Postural Balance Tests
3.8.3. Flexibility Tests
3.9. Predictive Validity for Institutionalization or Hospitalization
3.9.1. Gait Speed Tests
3.9.2. Postural Balance Tests
4. Discussion
4.1. Predictive Validity of Gait Speed Tests
4.2. Predictive Validity of Balance Tests
4.3. Predictive Validity of Multidimensional Measurement Tests
4.4. Predictive Validity of Flexibility Tests
4.5. Limitations and Strengths
4.6. Perspective
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Beard, J.R.; Officer, A.; De Carvalho, I.A.; Sadana, R.; Pot, A.M.; Michel, J.-P.; Lloyd-Sherlock, P.; Epping-Jordan, J.E.; Peeters, G.G.; Mahanani, W.R. The World report on ageing and health: A policy framework for healthy ageing. Lancet 2016, 387, 2145–2154. [Google Scholar] [CrossRef]
- Murray, C.J.; Lopez, A.D.; World Health Organization. The Global Burden of Disease: A Comprehensive Assessment of Mortality and Disability from Diseases, Injuries, and Risk Factors in 1990 and Projected to 2020: Summary; World Health Organization: Geneva, Switzerland, 1996.
- Andrasfay, T. Changes in Physical Functioning as Short-Term Predictors of Mortality. J. Gerontol. Ser. B-Psychol. Sci. Soc. Sci. 2020, 75, 630–639. [Google Scholar] [CrossRef] [PubMed]
- Briggs, A.M.; Cross, M.J.; Hoy, D.G.; Sanchez-Riera, L.; Blyth, F.M.; Woolf, A.D.; March, L. Musculoskeletal health conditions represent a global threat to healthy aging: A report for the 2015 World Health Organization world report on ageing and health. Gerontologist 2016, 56, S243–S255. [Google Scholar] [CrossRef] [PubMed]
- Brinda, E.M.; Rajkumar, A.P.; Attermann, J.; Gerdtham, U.G.; Enemark, U.; Jacob, K.S. Health, social, and economic variables associated with depression among older people in low and middle income countries: World health organization study on global AGEing and adult health. Am. J. Geriatr. Psychiatry 2016, 24, 1196–1208. [Google Scholar] [CrossRef] [PubMed]
- Stenhagen, M.; Ekstrom, H.; Nordell, E.; Elmstahl, S. Falls in the general elderly population: A 3- and 6-year prospective study of risk factors using data from the longitudinal population study ‘Good ageing in Skane’. BMC Geriatr. 2013, 13, 81. [Google Scholar] [CrossRef]
- Callisaya, M.L.; Ayers, E.; Barzilai, N.; Ferrucci, L.; Guralnik, J.M.; Lipton, R.B.; Otahal, P.; Srikanth, V.K.; Verghese, J. Motoric Cognitive Risk Syndrome and Falls Risk: A Multi-Center Study. J. Alzheimers Dis. 2016, 53, 1043–1052. [Google Scholar] [CrossRef]
- Quach, L.; Galica, A.M.; Jones, R.N.; Procter-Gray, E.; Manor, B.; Hannan, M.T.; Lipsitz, L.A. The Nonlinear Relationship Between Gait Speed and Falls: The Maintenance of Balance, Independent Living, Intellect, and Zest in the Elderly of Boston Study. J. Am. Geriatr. Soc. 2011, 59, 1069–1073. [Google Scholar] [CrossRef]
- Muraki, S.; Akune, T.; Oka, H.; Ishimoto, Y.; Nagata, K.; Yoshida, M.; Tokimura, F.; Nakamura, K.; Kawaguchi, H.; Yoshimura, N. Physical performance, bone and joint diseases, and incidence of falls in Japanese men and women: A longitudinal cohort study. Osteoporos. Int. 2013, 24, 459–466. [Google Scholar] [CrossRef]
- Barry, V.W.; Caputo, J.L.; Kang, M. The joint association of fitness and fatness on cardiovascular disease mortality: A meta-analysis. Prog. Cardiovasc. Dis. 2018, 61, 136–141. [Google Scholar] [CrossRef]
- Heiland, E.G.; Welmer, A.K.; Wang, R.; Santoni, G.; Fratiglioni, L.; Qiu, C.X. Cardiovascular risk factors and the risk of disability in older adults: Variation by age and functional status. J. Am. Med. Dir. Assoc. 2018, 20, 208. [Google Scholar] [CrossRef]
- Lee, W.J.; Peng, L.N.; Chiou, S.T.; Chen, L.K. Physical health indicators improve prediction of cardiovascular and all-cause mortality among middle-aged and older people: A national population-based study. Sci. Rep. 2017, 7, 40427. [Google Scholar] [CrossRef]
- Birtwhistle, R.; Bell, N.R.; Thombs, B.D.; Grad, R.; Dickinson, J.A. Periodic preventive health visits: A more appropriate approach to delivering preventive services: From the Canadian Task Force on Preventive Health Care. Can. Fam. Physician 2017, 63, 824–826. [Google Scholar]
- Cavanaugh, E.J.; Richardson, J.; McCallum, C.A.; Wilhelm, M. The Predictive Validity of Physical Performance Measures in Determining Markers of Preclinical Disability in Community-Dwelling Middle-Aged and Older Adults: A Systematic Review. Phys. Ther. 2018, 98, 1010–1021. [Google Scholar] [CrossRef] [PubMed]
- Van Kan, G.A.; Rolland, Y.; Andrieu, S.; Bauer, J.; Beauchet, O.; Bonnefoy, M.; Cesari, M.; Donini, L.M.; Gillette-Guyonnet, S.; Inzitari, M.; et al. Gait speed at usual pace as a predictor of adverse outcomes in community-dwelling older people an International Academy on Nutrition and Aging (IANA) Task Force. J. Nutr. Health Aging 2009, 13, 881–889. [Google Scholar] [CrossRef] [PubMed]
- Cooper, R.; Strand, B.H.; Hardy, R.; Patel, K.V.; Kuh, D. Physical capability in mid-life and survival over 13 years of follow-up: British birth cohort study. BMJ Clin. Res. Ed. 2014, 348, 2219. [Google Scholar] [CrossRef] [PubMed]
- Barry, V.W.; Baruth, M.; Beets, M.W.; Durstine, J.L.; Liu, J.; Blair, S.N. Fitness vs. fatness on all-cause mortality: A meta-analysis. Prog. Cardiovasc. Dis. 2014, 56, 382–390. [Google Scholar] [CrossRef] [PubMed]
- Cooper, R.; Kuh, D.; Hardy, R. Objectively measured physical capability levels and mortality: Systematic review and meta-analysis. BMJ 2010, 341, c4467. [Google Scholar] [CrossRef]
- Lee, D.-c.; Artero, E.G.; Sui, X.; Blair, S.N. Mortality trends in the general population: The importance of cardiorespiratory fitness. J. Psychopharmacol. 2010, 24, 27–35. [Google Scholar] [CrossRef] [PubMed]
- García-Hermoso, A.; Cavero-Redondo, I.; Ramírez-Vélez, R.; Ruiz, J.R.; Ortega, F.B.; Lee, D.-C.; Martínez-Vizcaíno, V. Muscular strength as a predictor of all-cause mortality in an apparently healthy population: A systematic review and meta-analysis of data from approximately 2 million men and women. Arch. Phys. Med. Rehabil. 2018, 99, 2100–2113.e5. [Google Scholar] [CrossRef]
- Volaklis, K.A.; Halle, M.; Meisinger, C. Muscular strength as a strong predictor of mortality: A narrative review. Eur. J. Intern. Med. 2015, 26, 303–310. [Google Scholar] [CrossRef]
- Goodway, J.D.; Ozmun, J.C.; Gallahue, D.L. Understanding Motor Development: Infants, Children, Adolescents, Adults; Jones & Bartlett Learning: Burlington, MA, USA, 2019. [Google Scholar]
- Bandy, W.D.; Sanders, B. Therapeutic Exercise: Techniques for Intervention; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2001. [Google Scholar]
- Quan, M.H.; Xun, P.C.; Chen, C.; Wen, J.; Wang, Y.Y.; Wang, R.; Chen, P.J.; He, K. Walking Pace and the Risk of Cognitive Decline and Dementia in Elderly Populations: A Meta-analysis of Prospective Cohort Studies. J. Gerontol. Ser. A-Biol. Sci. Med. Sci. 2017, 72, 266–270. [Google Scholar] [CrossRef]
- Peel, N.M.; Alapatt, L.J.; Jones, L.V.; Hubbard, R.E. The Association between Gait Speed and Cognitive Status in Community-Dwelling Older People: A Systematic Review and Meta-analysis. J. Gerontol. Ser. A-Biol. Sci. Med. Sci. 2019, 74, 943–948. [Google Scholar] [CrossRef]
- Grande, G.; Triolo, F.; Nuara, A.; Welmer, A.K.; Fratiglioni, L.; Vetrano, D.L. Measuring gait speed to better identify prodromal dementia. Exp. Gerontol. 2019, 124, 110625. [Google Scholar] [CrossRef]
- Wang, D.X.M.; Yao, J.; Zirek, Y.; Reijnierse, E.M.; Maier, A.B. Muscle mass, strength, and physical performance predicting activities of daily living: A meta-analysis. J. Cachexia Sarcopenia Muscle 2020, 11, 3–25. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Ruiz, J.R.; Castro-Piñero, J.; Artero, E.G.; Ortega, F.B.; Sjöström, M.; Suni, J.; Castillo, M.J. Predictive validity of health-related fitness in youth: A systematic review. Br. J. Sports Med. 2009, 43, 909–923. [Google Scholar] [CrossRef]
- Shea, B.J.; Grimshaw, J.M.; Wells, G.A.; Boers, M.; Andersson, N.; Hamel, C.; Porter, A.C.; Tugwell, P.; Moher, D.; Bouter, L.M. Development of AMSTAR: A measurement tool to assess the methodological quality of systematic reviews. BMC Med. Res. Methodol. 2007, 7, 10. [Google Scholar] [CrossRef]
- Abu Samah, Z.; Singh, D.K.A.; Murukesu, R.R.; Shahar, S.; Nordin, N.A.M.; Omar, M.A.; Ai-Vyrn, C. Discriminative and Predictive Ability of Physical Performance Measures in Identifying Fall Risk among Older Adults. Sains Malays. 2018, 47, 2769–2776. [Google Scholar] [CrossRef]
- Brach, J.S.; Wert, D.; VanSwearingen, J.M.; Newman, A.B.; Studenski, S.A. Use of Stance Time Variability for Predicting Mobility Disability in Community-Dwelling Older Persons: A Prospective Study. J. Geriatr. Phys. Ther. 2012, 35, 112–117. [Google Scholar] [CrossRef] [PubMed]
- Sakurai, R.; Suzuki, H.; Ogawa, S.; Kawai, H.; Yoshida, H.; Hirano, H.; Ihara, K.; Obuchi, S.; Fujiwara, Y. Fear of falling, but not gait impairment, predicts subjective memory complaints in cognitively intact older adults. Geriatr. Gerontol. Int. 2017, 17, 1125–1131. [Google Scholar] [CrossRef] [PubMed]
- Dargent-Molina, P.; Schott, A.M.; Hans, D.; Favier, F.; Grandjean, H.; Baudoin, C.; Meunier, P.J.; Breart, G.; Grp, E.S. Separate and combined value of bone mass and gait speed measurements in screening for hip fracture risk: Results from the EPIDOS study. Osteoporos. Int. 1999, 9, 188–192. [Google Scholar] [CrossRef] [PubMed]
- Doi, T.; Hirata, S.; Ono, R.; Tsutsumimoto, K.; Misu, S.; Ando, H. The harmonic ratio of trunk acceleration predicts falling among older people: Results of a 1-year prospective study. J. Neuroeng. Rehabil. 2013, 10, 7. [Google Scholar] [CrossRef] [PubMed]
- Kang, L.; Han, P.P.; Wang, J.Z.; Ma, Y.X.; Jia, L.Y.; Fu, L.Y.; Yu, H.R.; Chen, X.Y.; Niu, K.J.; Guo, Q. Timed Up and Go Test can predict recurrent falls: A longitudinal study of the community-dwelling elderly in China. Clin. Interv. Aging 2017, 12, 2009–2016. [Google Scholar] [CrossRef] [PubMed]
- Kauppi, M.; Stenholm, S.; Impivaara, O.; Maki, J.; Heliovaara, M.; Jula, A. Fall-related risk factors and heel quantitative ultrasound in the assessment of hip fracture risk: A 10-year follow-up of a nationally representative adult population sample. Osteoporos. Int. 2014, 25, 1685–1695. [Google Scholar] [CrossRef]
- Laukkanen, P.; Leskinen, E.; Kauppinen, M.; Sakari-Rantala, R.; Heikkinen, E. Health and functional capacity as predictors of community dwelling among elderly people. J. Clin. Epidemiol. 2000, 53, 257–265. [Google Scholar] [CrossRef]
- Makizako, H.; Shimada, H.; Doi, T.; Tsutsumimoto, K.; Lee, S.; Hotta, R.; Nakakubo, S.; Harada, K.; Lee, S.; Bae, S.; et al. Cognitive Functioning and Walking Speed in Older Adults as Predictors of Limitations in Self-Reported Instrumental Activity of Daily Living: Prospective Findings from the Obu Study of Health Promotion for the Elderly. Int. J. Environ. Res. Public Health 2015, 12, 3002–3013. [Google Scholar] [CrossRef] [PubMed]
- Abe, T.; Kitamura, A.; Taniguchi, Y.; Amano, H.; Seino, S.; Yokoyama, Y.; Nishi, M.; Narita, M.; Ikeuchi, T.; Fujiwara, Y.; et al. Pathway from gait speed to incidence of disability and mortality in older adults: A mediating role of physical activity. Maturitas 2019, 123, 32–36. [Google Scholar] [CrossRef]
- Adachi, T.; Kamiya, K.; Kono, Y.; Iwatsu, K.; Shimizu, Y.; Honda, I.; Yamada, S. Estimation of reduced walking speed using simple measurements of physical and psychophysiological function in community-dwelling elderly people: A cross-sectional and longitudinal study. Aging Clin. Exp. Res. 2019, 31, 59–66. [Google Scholar] [CrossRef]
- Blain, H.; Carriere, I.; Sourial, N.; Berard, C.; Favier, F.; Colvez, A.; Bergman, H. Balance and walking speed predict subsequent 8-year mortality independently of current and intermediate events in well-functioning women aged 75 years and older. J. Nutr. Health Aging 2010, 14, 595–600. [Google Scholar] [CrossRef] [PubMed]
- Briggs, R.; Carey, D.; Claffey, P.; McNicholas, T.; Donoghue, O.; Kennelly, S.P.; Kenny, R.A. Do Differences in Spatiotemporal Gait Parameters Predict the Risk of Developing Depression in Later Life? J. Am. Geriatr. Soc. 2019, 67, 1050–1056. [Google Scholar] [CrossRef]
- Buracchio, T.; Dodge, H.H.; Howieson, D.; Wasserman, D.; Kaye, J. The Trajectory of Gait Speed Preceding Mild Cognitive Impairment. Arch. Neurol. 2010, 67, 980–986. [Google Scholar] [CrossRef]
- Camargo, E.C.; Weinstein, G.; Beiser, A.S.; Tan, Z.S.; DeCarli, C.; Kelly-Hayes, M.; Kase, C.; Murabito, J.M.; Seshadri, S. Association of Physical Function with Clinical and Subclinical Brain Disease: The Framingham Offspring Study. J. Alzheimer’s Dis. 2016, 53, 1597–1608. [Google Scholar] [CrossRef]
- Deshpande, N.; Metter, E.J.; Guralnik, J.; Bandinelli, S.; Ferrucci, L. Predicting 3-Year Incident Mobility Disability in Middle-Aged and Older Adults Using Physical Performance Tests. Arch. Phys. Med. Rehabil. 2013, 94, 994–997. [Google Scholar] [CrossRef]
- Doi, T.; Nakakubo, S.; Tsutsumimoto, K.; Kim, M.J.; Kurita, S.; Ishii, H.; Shimada, H. Spatio-temporal gait variables predicted incident disability. J. Neuroeng. Rehabil. 2020, 17, 11. [Google Scholar] [CrossRef]
- Elbaz, A.; Sabia, S.; Brunner, E.; Shipley, M.; Marmot, M.; Kivimaki, M.; Singh-Manoux, A. Association of walking speed in late midlife with mortality: Results from the Whitehall II cohort study. Age 2013, 35, 943–952. [Google Scholar] [CrossRef] [PubMed]
- Georgiopoulou, V.V.; Kalogeropoulos, A.P.; Chowdhury, R.; Binongo, J.N.G.; Bibbins-Domingo, K.; Rodondi, N.; Simonsick, E.M.; Harris, T.; Newman, A.B.; Kritchevsky, S.B.; et al. Exercise Capacity, Heart Failure Risk, and Mortality in Older Adults: The Health ABC Study. Am. J. Prev. Med. 2016, 52, 144–153. [Google Scholar] [CrossRef]
- Hoogendijk, E.O.; Rijnhart, J.J.M.; Skoog, J.; Robitaille, A.; van den Hout, A.; Ferrucci, L.; Huisman, M.; Skoog, I.; Piccinin, A.M.; Hofer, S.M.; et al. Gait speed as predictor of transition into cognitive impairment: Findings from three longitudinal studies on aging. Exp. Gerontol. 2020, 129, 110783. [Google Scholar] [CrossRef] [PubMed]
- Idland, G.; Pettersen, R.; Avlund, K.; Bergland, A. Physical performance as long-term predictor of onset of activities of daily living (ADL) disability: A 9-year longitudinal study among community-dwelling older women. Arch. Gerontol. Geriatr. 2013, 56, 501–506. [Google Scholar] [CrossRef] [PubMed]
- Jung, H.W.; Jang, I.Y.; Lee, C.K.; Yu, S.S.; Hwang, J.K.; Jeon, C.; Lee, Y.S.; Lee, E. Usual gait speed is associated with frailty status, institutionalization, and mortality in community-dwelling rural older adults: A longitudinal analysis of the Aging Study of Pyeongchang Rural Area. Clin. Interv. Aging 2018, 13, 1079–1089. [Google Scholar] [CrossRef] [PubMed]
- Looker, A.C. Dysmobility syndrome and mortality risk in US men and women age 50 years and older. Osteoporos. Int. 2015, 26, 93–102. [Google Scholar] [CrossRef]
- Luukinen, H.; Koski, K.; Laippala, P.; Kivela, S.L. Predictors for recurrent falls among the home-dwelling elderly. Scand. J. Prim. Health Care 1995, 13, 294–299. [Google Scholar] [CrossRef]
- Makizako, H.; Furuna, T.; Yoshida, H.; Shimada, H.; Satoh, K.; Akanuma, T.; Ihira, H.; Suzuki, T. Usual Walking Speed Predicts Decline of Functional Capacity among Community-Dwelling Older Japanese Women: A 4-year Longitudinal Study. J. Phys. Ther. Sci. 2010, 22, 405–412. [Google Scholar] [CrossRef]
- Nakamoto, M.; Otsuka, R.; Yuki, A.; Nishita, Y.; Tange, C.; Tomida, M.; Kato, Y.; Ando, F.; Shimokata, H.; Suzuki, T. Higher gait speed and smaller sway area decrease the risk for decline in higher-level functional capacity among middle-aged and elderly women. Arch. Gerontol. Geriatr. 2015, 61, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Niiranen, T.J.; Enserro, D.M.; Larson, M.G.; Vasan, R.S. Multisystem Trajectories over the Adult Life Course and Relations to Cardiovascular Disease and Death. J. Gerontol. Ser. A-Biol. Sci. Med. Sci. 2019, 74, 1778–1785. [Google Scholar] [CrossRef] [PubMed]
- Nofuji, Y.; Shinkai, S.; Taniguchi, Y.; Amano, H.; Nishi, M.; Murayama, H.; Fujiwara, Y.; Suzuki, T. Associations of Walking Speed, Grip Strength, and Standing Balance With Total and Cause-Specific Mortality in a General Population of Japanese Elders. J. Am. Med. Dir. Assoc. 2016, 17, 184.e1–184.e7. [Google Scholar] [CrossRef] [PubMed]
- Ojagbemi, A.; D’Este, C.; Verdes, E.; Chatterji, S.; Gureje, O. Gait speed and cognitive decline over 2 years in the Ibadan study of aging. Gait Posture 2015, 41, 736–740. [Google Scholar] [CrossRef] [PubMed]
- Osuka, Y.; Kim, H.; Watanabe, Y.; Taniguchi, Y.; Kojima, N.; Seino, S.; Kawai, H.; Sakurai, R.; Inagaki, H.; Awata, S. A combined stepping and visual tracking task predicts cognitive decline in older adults better than gait or visual tracking tasks alone: A prospective study. Aging Clin. Exp. Res. 2020, 33, 1865–1873. [Google Scholar] [CrossRef]
- Rosso, A.L.; Metti, A.L.; Faulkner, K.; Brach, J.S.; Studenski, S.A.; Redfern, M.; Rosano, C. Associations of Usual Pace and Complex Task Gait Speeds With Incident Mobility Disability. J. Am. Geriatr. Soc. 2019, 67, 2072–2076. [Google Scholar] [CrossRef]
- Sabia, S.; Dumurgier, J.; Tavernier, B.; Head, J.; Tzourio, C.; Elbaz, A. Change in Fast Walking Speed Preceding Death: Results From a Prospective Longitudinal Cohort Study. J. Gerontol. Ser. A-Biol. Sci. Med. Sci. 2014, 69, 354–362. [Google Scholar] [CrossRef]
- Sanders, J.B.; Bremmer, M.A.; Deeg, D.J.H.; Beekman, A.T.F. Do Depressive Symptoms and Gait Speed Impairment Predict Each Other’s Incidence? A 16-Year Prospective Study in the Community. J. Am. Geriatr. Soc. 2012, 60, 1673–1680. [Google Scholar] [CrossRef]
- Sanders, J.B.; Bremmer, M.A.; Comijs, H.C.; van de Ven, P.M.; Deeg, D.J.H.; Beekman, A.T.F. Gait Speed and Processing Speed as Clinical Markers for Geriatric Health Outcomes. Am. J. Geriatr. Psychiatry 2016, 25, 374–385. [Google Scholar] [CrossRef] [PubMed]
- Stijntjes, M.; Aartsen, M.J.; Taekema, D.G.; Gussekloo, J.; Huisman, M.; Meskers, C.G.M.; de Craen, A.J.M.; Maier, A.B. Temporal Relationship Between Cognitive and Physical Performance in Middle-Aged to Oldest Old People. J. Gerontol. Ser. A-Biol. Sci. Med. Sci. 2017, 72, 662–668. [Google Scholar] [CrossRef]
- Tian, Q.; Resnick, S.M.; Studenski, S.A.; Ferrucci, L. Lap Time Variability From a 400-m Walk Is Associated with Future Mild Cognitive Impairment and Alzheimer’s Disease. J. Am. Med. Dir. Assoc. 2019, 20, 1535–1539.e3. [Google Scholar] [CrossRef]
- Veronese, N.; Solmi, M.; Maggi, S.; Noale, M.; Sergi, G.; Manzato, E.; Prina, A.M.; Fornaro, M.; Carvalho, A.F.; Stubbs, B. Frailty and incident depression in community-dwelling older people: Results from the ELSA study. Int. J. Geriatr. Psychiatry 2017, 32, E141–E149. [Google Scholar] [CrossRef]
- Veronese, N.; Stubbs, B.; Trevisan, C.; Bolzetta, F.; De Rui, M.; Solmi, M.; Sartori, L.; Musacchio, E.; Zambon, S.; Perissinotto, E.; et al. Poor Physical Performance Predicts Future Onset of Depression in Elderly People: Progetto Veneto Anziani Longitudinal Study. Phys. Ther. 2017, 97, 659–668. [Google Scholar] [CrossRef] [PubMed]
- Ward, R.E.; Beauchamp, M.K.; Latham, N.K.; Leveille, S.G.; Percac-Lima, S.; Kurlinski, L.; Ni, P.S.; Goldstein, R.; Jette, A.M.; Bean, J.F. Neuromuscular Impairments Contributing to Persistently Poor and Declining Lower-Extremity Mobility Among Older Adults: New Findings Informing Geriatric Rehabilitation. Arch. Phys. Med. Rehabil. 2016, 97, 1316–1322. [Google Scholar] [CrossRef]
- Wihlborg, A.; Englund, M.; Akesson, K.; Gerdhem, P. Fracture predictive ability of physical performance tests and history of falls in elderly women: A 10-year prospective study. Osteoporos. Int. 2015, 26, 2101–2109. [Google Scholar] [CrossRef] [PubMed]
- Zucchelli, A.; Vetrano, D.L.; Grande, G.; Calderon-Larranaga, A.; Fratiglioni, L.; Marengoni, A.; Rizzuto, D. Comparing the prognostic value of geriatric health indicators: A population-based study. BMC Med. 2019, 17, 185. [Google Scholar] [CrossRef] [PubMed]
- Pajala, S.; Era, P.; Koskenvuo, M.; Kaprio, J.; Tormakangas, T.; Rantanen, T. Force platform balance measures as predictors of indoor and outdoor falls in community-dwelling women aged 63-76 years. J. Gerontol. Ser. A-Biol. Sci. Med. Sci. 2008, 63, 171–178. [Google Scholar] [CrossRef]
- Austin, N.; Devine, A.; Dick, I.; Prince, R.; Bruce, D. Fear of falling in older women: A longitudinal study of incidence, persistence, and predictors. J. Am. Geriatr. Soc. 2007, 55, 1598–1603. [Google Scholar] [CrossRef]
- Ersoy, Y.; MacWalter, R.S.; Durmus, B.; Altay, Z.E.; Baysal, O. Predictive Effects of Different Clinical Balance Measures and the Fear of Falling on Falls in Postmenopausal Women Aged 50 Years and Over. Gerontology 2009, 55, 660–665. [Google Scholar] [CrossRef]
- Frames, C.W.; Soangra, R.; Lockhart, T.E.; Lach, J.; Ha, D.S.; Roberto, K.A.; Lieberman, A. Dynamical Properties of Postural Control in Obese Community-Dwelling Older Adults. Sensors 2018, 18, 1692. [Google Scholar] [CrossRef]
- Maki, B.E.; Holliday, P.J.; Topper, A.K. A prospective study of postural balance and risk of falling in an ambulatory and independent elderly population. J. Gerontol. 1994, 49, M72–M84. [Google Scholar] [CrossRef]
- Muir, S.W.; Berg, K.; Chesworth, B.M.; Klar, N.; Speechley, M. Modifiable Risk Factors Identify People Who Transition from Non-fallers to Fallers in Community-Dwelling Older Adults: A Prospective Study. Physiother. Can. 2010, 62, 358–367. [Google Scholar] [CrossRef]
- Mulasso, A.; Roppolo, M.; Gobbens, R.J.; Rabaglietti, E. Mobility, balance and frailty in community-dwelling older adults: At is the best 1-year predictor of falls? Geriatr. Gerontol. Int. 2017, 17, 1463–1469. [Google Scholar] [CrossRef] [PubMed]
- Swanenburg, J.; de Bruin, E.D.; Uebelhart, D.; Mulder, T. Falls prediction in elderly people: A 1-year prospective study. Gait Posture 2010, 31, 317–321. [Google Scholar] [CrossRef]
- Breton, E.; Beloin, F.; Fortin, C.; Martin, A.; Ouellet, M.E.; Payette, H.; Levasseur, M. Gender-specific associations between functional autonomy and physical capacities in independent older adults: Results from the NuAge study. Arch. Gerontol. Geriatr. 2014, 58, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Bullain, S.S.; Corrada, M.M.; Perry, S.M.; Kawas, C.H. Sound Body Sound Mind? Physical Performance and the Risk of Dementia in the Oldest-Old: The 90+Study. J. Am. Geriatr. Soc. 2016, 64, 1408–1415. [Google Scholar] [CrossRef]
- Kwan, M.M.; Lin, S.I.; Close, J.C.; Lord, S.R. Depressive symptoms in addition to visual impairment, reduced strength and poor balance predict falls in older Taiwanese people. Age Ageing 2012, 41, 606–612. [Google Scholar] [CrossRef][Green Version]
- Nitz, J.C.; Stock, L.; Khan, A. Health-related predictors of falls and fractures in women over 40. Osteoporos. Int. 2013, 24, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Vellas, B.J.; Wayne, S.J.; Romero, L.; Baumgartner, R.N.; Rubenstein, L.Z.; Garry, P.J. One-leg balance is an important predictor of injurious falls in older persons. J. Am. Geriatr. Soc. 1997, 45, 735–738. [Google Scholar] [CrossRef]
- Clemson, L.; Kendig, H.; Mackenzie, L.; Browning, C. Predictors of Injurious Falls and Fear of Falling Differ: An 11-Year Longitudinal Study of Incident Events in Older People. J. Aging Health 2015, 27, 239–256. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.C.; Best, J.R.; Bryan, S.; Li, L.C.; Hsu, C.L.; Gomez, C.; Vertes, K.; Liu-Ambrose, T. Mobility Is a Key Predictor of Change in Well-Being Among Older Adults Who Experience Falls: Evidence From the Vancouver Falls Prevention Clinic Cohort. Arch. Phys. Med. Rehabil. 2015, 96, 1634–1640. [Google Scholar] [CrossRef] [PubMed]
- Asai, T.; Oshima, K.; Fukumoto, Y.; Yonezawa, Y.; Matsuo, A.; Misu, S. Does dual-tasking provide additional value in timed “up and go” test for predicting the occurrence of falls? A longitudinal observation study by age group (young-older or old-older adults). Aging Clin. Exp. Res. 2020, 33, 77–84. [Google Scholar] [CrossRef]
- Doi, T.; Tsutsumimoto, K.; Nakakubo, S.; Kim, M.J.; Kurita, S.; Hotta, R.; Shimada, H. Physical Performance Predictors for Incident Dementia Among Japanese Community-Dwelling Older Adults. Phys. Ther. 2019, 99, 1132–1140. [Google Scholar] [CrossRef]
- Donoghue, O.; Feeney, J.; O’Leary, N.; Kenny, R.A. Baseline Mobility is Not Associated with Decline in Cognitive Function in Healthy Community-Dwelling Older Adults: Findings From The Irish Longitudinal Study on Ageing (TILDA). Am. J. Geriatr. Psychiatry 2017, 26, 438–448. [Google Scholar] [CrossRef]
- Savva, G.M.; Donoghue, O.A.; Horgan, F.; O’Regan, C.; Cronin, H.; Kenny, R.A. Using Timed Up-and-Go to Identify Frail Members of the Older Population. J. Gerontol. Ser. A-Biol. Sci. Med. Sci. 2013, 68, 441–446. [Google Scholar] [CrossRef]
- Schroll, M.; Avlund, K.; Davidsen, M. Predictors of five-year functional ability in a longitudinal survey of men and women aged 75 to 80. The 1914-population in Glostrup, Denmark. Aging-Clin. Exp. Res. 1997, 9, 143–152. [Google Scholar] [CrossRef] [PubMed]
- Bravell, M.E.; Finkel, D.; Aslan, A.D.; Reynolds, C.A.; Hallgren, J.; Pedersen, N.L. Motor functioning differentially predicts mortality in men and women. Arch. Gerontol. Geriatr. 2017, 72, 6–11. [Google Scholar] [CrossRef] [PubMed]
- van Tulder, M.W.; Ostelo, R.; Vlaeyen, J.W.; Linton, S.J.; Morley, S.J.; Assendelft, W.J. Behavioral treatment for chronic low back pain: A systematic review within the framework of the Cochrane Back Review Group. Spine 2000, 25, 2688–2699. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [PubMed]
- Coll-Risco, I.; Acosta-Manzano, P.; Borges-Cosic, M.; Camiletti-Moiron, D.; Aranda, P.; Soriano-Maldonado, A.; Aparicio, V.A. Body Composition Changes Following a Concurrent Exercise Intervention in Perimenopausal Women: The FLAMENCO Project Randomized Controlled Trial. J. Clin. Med. 2019, 8, 1678. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W. Reference values for the timed up and go test: A descriptive meta-analysis. J. Geriatr. Phys. Ther. 2006, 29, 64–68. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marín-Jiménez, N.; Cruz-León, C.; Perez-Bey, A.; Conde-Caveda, J.; Grao-Cruces, A.; Aparicio, V.A.; Castro-Piñero, J.; Cuenca-García, M. Predictive Validity of Motor Fitness and Flexibility Tests in Adults and Older Adults: A Systematic Review. J. Clin. Med. 2022, 11, 328. https://doi.org/10.3390/jcm11020328
Marín-Jiménez N, Cruz-León C, Perez-Bey A, Conde-Caveda J, Grao-Cruces A, Aparicio VA, Castro-Piñero J, Cuenca-García M. Predictive Validity of Motor Fitness and Flexibility Tests in Adults and Older Adults: A Systematic Review. Journal of Clinical Medicine. 2022; 11(2):328. https://doi.org/10.3390/jcm11020328
Chicago/Turabian StyleMarín-Jiménez, Nuria, Carolina Cruz-León, Alejandro Perez-Bey, Julio Conde-Caveda, Alberto Grao-Cruces, Virginia A. Aparicio, José Castro-Piñero, and Magdalena Cuenca-García. 2022. "Predictive Validity of Motor Fitness and Flexibility Tests in Adults and Older Adults: A Systematic Review" Journal of Clinical Medicine 11, no. 2: 328. https://doi.org/10.3390/jcm11020328
APA StyleMarín-Jiménez, N., Cruz-León, C., Perez-Bey, A., Conde-Caveda, J., Grao-Cruces, A., Aparicio, V. A., Castro-Piñero, J., & Cuenca-García, M. (2022). Predictive Validity of Motor Fitness and Flexibility Tests in Adults and Older Adults: A Systematic Review. Journal of Clinical Medicine, 11(2), 328. https://doi.org/10.3390/jcm11020328