
Association between Endometriosis, Irritable Bowel Syndrome and Eating Disorders: ENDONUT Pilot Study

 , , ,
, , ,
Abstract
1. Introduction
2. Method
2.1. Population
2.2. Data Collection
2.3. Statistical Analyses
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Serdar, E. Endometriosis. N. Engl. J. Med. 2009, 360, 268–279. [Google Scholar]
- Pugsley, Z.; Ballard, K. Management of endometriosis in general practice: The pathway to diagnosis. Br. J. Gen. Pract. 2007, 57, 470–476. [Google Scholar] [PubMed]
- Nnoaham, K.E.; Hummelshoj, L.; Webster, P.; d’Hooghe, T.; de Cicco Nardone, F.; de Cicco Nardone, C.; Jenkinson, C.; Kennedy, S.H.; Zondervan, K.T.; World Endometriosis Research Foundation Global Study of Women's Health consortium. Impact of endometriosis on quality of life and work productivity: A multicenter study accros ten countries. Fertil. Steril. 2011, 96, 366–373. [Google Scholar] [CrossRef] [PubMed]
- Škegro, B.; Bjedov, S.; Mikuš, M.; Mustač, F.; Lešin, J.; Matijević, V.; Ćorić, M.; Elveđi Gašparović, V.; Medić, F.; Sokol Karadjole, V. Endometriosis, Pain and Mental Health. Psychiatr. Danub. 2021, 33 (Suppl. 4), 632–636. [Google Scholar] [PubMed]
- Mikuš, M.; Matak, L.; Vujić, G.; Škegro, B.; Škegro, I.; Augustin, G.; Lagana, A.S.; Ćorić, M. The short form endometriosis health profile questionnaire (EHP-5): Psychometric validity assessment of a Croatian version. Arch. Gynecol. Obstet. 2022. [CrossRef]
- Viganò, D.; Zara, F.; Usai, P. Irritable bowel syndrome and endometriosis: New insights for old diseases. Dig. Liver Dis. 2018, 50, 213–219. [Google Scholar] [CrossRef]
- Saidi, K.; Sharma, S.; Ohlsson, B. A systematic review and meta-analysis of the associations between endometriosis and irritable bowel syndrome. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 246, 99–105. [Google Scholar] [CrossRef]
- Moore, J.S.; Gibson, P.R.; Perry, R.E.; Burgell, R.E. Endometriosis in patients with irritable bowel syndrome: Specific symptomatic and demographic profile, and response to the low FODMAP diet. Aust. N. Z. J. Obstet. Gynecol. 2017, 57, 201–205. [Google Scholar] [CrossRef]
- Chiaffarino, F.; Cipriani, S.; Ricci, E.; Mauri, P.A.; Esposito, G.; Barretta, M.; Vercellini, P.; Parazzini, F. Endometriosis and irritable bowel syndrome: A systematic review and meta-analysis. Arch. Gynecol. Obstet. 2020, 303, 17–25. [Google Scholar] [CrossRef]
- Sood, R.; Law, G.R.; Ford, A.C. Diagnosis of IBS: Symptoms, symptom-based criteria, biomarkers or ‘psychomarkers’. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 683–691. [Google Scholar] [CrossRef]
- Sperber, A.; Dumitrascu, D.; Fukudo, S.; Gerson, C.; Ghoshal, U.C.; Gwee, K.A.; Hungin, A.P.; Kang, J.-Y.; Minhu, C.; Schmulson, M.; et al. The global prevalence of IBS in adults remains elusive due to the heterogeneity of studies: A Rome Foundation working team literature review. Gut 2016, 66, 1075–1082. [Google Scholar] [CrossRef] [PubMed]
- Chang, L. Updates to the Rome Criteria for Irritable Bowel Syndrome. Gastroenterol. Hepatol. 2017, 13, 304–306. [Google Scholar]
- Drossman, D.A. Functional Gastrointestinal Disorders: History, Pathophysiology, Clinical Features, and Rome IV. Gastroenterology 2016, 150, 1262–1279.e2. [Google Scholar] [CrossRef] [PubMed]
- Mari, A.; Hosadurg, D.; Martin, L.; Zarate-Lopez, N.; Passananti, V.; Emmanuel, A. Adherence with a low-FODMAP diet in irritable bowel syndrome: Are eating disorders the missing link? Eur. J. Gastroenterol. Hepatol. 2019, 31, 178–182. [Google Scholar] [CrossRef] [PubMed]
- Santonicola, A.; Gagliardi, M.; Guarino, M.P.L.; Siniscalchi, M.; Ciacci, C.; Iovino, P. Eating Disorders and Gastrointestinal Diseases. Nutrients 2019, 11, 3038. [Google Scholar] [CrossRef] [PubMed]
- Reed-Knight, B.; Squires, M.; Chitkara, D.K.; Van Tilburg, M.A.L. Adolescents with IBS report increased eating associated symptoms, changes in dietary composition, and altered eating behaviors: A pilot comparison study to healthy adolescents. Neurogastroenterol. Motil. 2016, 28, 1915–1920. [Google Scholar] [CrossRef]
- Battle, D.E. Diagnostic and Statistical Manual of Mental Disorders (DSM). Codas 2013, 25, 191–192. [Google Scholar]
- Sato, Y.; Fukudo, S. Gastrointestinal symptoms and disorders in patients with eating disorders. Clin. J. Gastroenterol. 2015, 8, 255–263. [Google Scholar] [CrossRef]
- Abraham, S.; Kellow, J.E. Do the digestive tract symptoms in eating disorder patients represent functional gastrointestinal disorders? BMC Gastroenterol. 2013, 13, 38. [Google Scholar] [CrossRef]
- DeJong, H.; Perkins, S.; Grover, M.; Schmidt, U. The prevalence of irritable bowel syndrome in outpatients with bulimia nervosa. Int. J. Eat. Disord. 2011, 44, 661–664. [Google Scholar] [CrossRef]
- Melchior, C.; Desprez, C.; Riachi, G.; Leroi, A.-M.; Déchelotte, P.; Achamrah, N.; Ducrotté, P.; Tavolacci, M.-P.; Gourcerol, G. Anxiety and Depression Profile Is Associated with Eating Disorders in Patients with Irritable Bowel Syndrome. Front. Psychiatry 2020, 10, 928. [Google Scholar] [CrossRef] [PubMed]
- Galmiche, M.; Déchelotte, P.; Lambert, G.; Tavolacci, M.P. Prevalence of eating disorders over the 2000–2018 period: A systematic literature review. Am. J. Clin. Nutr. 2019, 109, 1402–1413. [Google Scholar] [CrossRef] [PubMed]
- Luck, A.J.; MorganLuck, J.F.; Reid, F.; O’Brien, A.; Brunton, J.; Price, C.; Perry, L.; Lacey, J.H. The SCOFF questionnaire and clinical interview for eating disorders in general practice: Comparative study. BMJ 2002, 325, 755–756. [Google Scholar] [CrossRef]
- Garcia, F.D.; Grigioni, S.; Allais, E.; Houy-Durand, E.; Thibaut, F.; Déchelotte, P. Detection of eating disorders in patient: Validity and reliability of the French version of the SCOFF questionnaire. Clin. Nutr. 2011, 30, 178–181. [Google Scholar] [CrossRef] [PubMed]
- Kleiman, S.C.; Watson, H.J.; Bulik-Sullivan, E.C.; Huh, E.Y.; Tarantino, L.M.; Bulik, C.M.; Carroll, I.M. The intestinal microbiota in acute anorexia nervosa and during renourishment: Relationship to depression, anxiety, and eating disorders psychopathology. Psychosom. Med. 2015, 77, 969–981. [Google Scholar] [CrossRef]
- Manson, L.B. Feeding systems and the gut microbiome: Gut-brain interactions with relevance to psychiatric conditions. Psychosomatics 2017, 58, 574–580. [Google Scholar] [CrossRef]
- Perkins, S.; Keville, S.; Schmidt, U.; Chalder, T. Eating disorders and irritable bowel syndrome: Is there a link? J. Psychosom. Res. 2005, 59, 57–64. [Google Scholar] [CrossRef]
- Kleiman, S.C.; Glenny, E.M.; Bulik-Sullivan, E.C.; Huh, E.Y.; Tsilimigras, M.C.B.; Fodor, A.A.; Bulik, C.; Carroll, I.M. Daily Changes in Composition and Diversity of the Intestinal Microbiota in Patients with Anorexia Nervosa: A Cases Series. Eur. Eat. Disord. Rev. 2017, 25, 423–427. [Google Scholar] [CrossRef]
- Morita, C.; Tsuji, H.; Hata, T.; Gondo, M.; Takakura, S.; Kawai, K.; Yoshihara, K.; Ogata, K.; Nomoto, K.; Miyazaki, K.; et al. Gut Dysbiosis in Patients with Anorexia Nervosa. PLoS ONE 2015, 10, e0145274. [Google Scholar] [CrossRef]
- Borgo, F.; Riva, A.; Benetti, A.; Casiraghi, M.C.; Bertelli, S.; Garbossa, S.; Anselmetti, S.; Scarone, S.; Pontiroli, A.E.; Morace, G.; et al. Microbiota in anorexia nervosa: The triangle between bacterial species, metabolites and psychological tests. PLoS ONE 2017, 12, e0179739. [Google Scholar] [CrossRef]
- Bulik, C.M.; Flatt, R.; Abbaspour, A.; Carroll, I. Reconceptualizing anorexia nervosa. Psychiatry Clin. Neurosci. 2019, 73, 518–525. [Google Scholar] [CrossRef] [PubMed]
- Lam, Y.Y.; Maguire, S.; Palacios, T.; Caterson, I.D. Are the Gut Bacteria Telling Us to Eat or Not to Eat? Reviewing the Role of Gut Microbiota in the Etiology, Disease Progression and Treatment of Eating Disorders. Nutrients 2017, 9, 602. [Google Scholar] [CrossRef] [PubMed]
- Breton, J.; Tennoune, N.; Lucas, N.; Francois, M.; Legrand, R.; Jacquemot, J.; Goichon, A.; Guérin, C.; Peltier, J.; Pestel-Caron, M.; et al. Gut Commensal E. coli Proteins Activate Host Satiety Pathways following Nutrient-Induced Bacterial Growth. Cell Metab. 2015, 23, 324–334. [Google Scholar] [CrossRef] [PubMed]
- Achamrah, N.; Nobis, S.; Breton, J.; Jésus, P.; Belmonte, L.; Maurer, B.; Legrand, R.; Bôle-Feysot, C.; Rego, J.C.D.; Goichon, A.; et al. Maintaining physical activity during refeeding improves body composition, intestinal hyperpermeability and behavior in anorectic mice. Sci. Rep. 2016, 6, 21887. [Google Scholar] [CrossRef]
- Monteleone, P.; Carratù, R.; Cartenì, M.; Generoso, M.; Lamberti, M.; De Magistris, L.; Brambilla, F.; Colurcio, B.; Secondulfo, M.; Maj, M. Intestinal permeability is decreased in anorexia nervosa. Mol. Psychiatry 2003, 9, 76–80. [Google Scholar] [CrossRef]
- Jésus, P.; Ouelaa, W.; François, M.; Riachy, L.; Guérin, C.; Aziz, M.; Rego, J.-C.D.; Déchelotte, P.; Fetissov, S.O.; Coëffier, M. Alteration of intestinal barrier function during activity-based anorexia in mice. Clin. Nutr. 2014, 33, 1046–1053. [Google Scholar] [CrossRef]
- Jiang, I.; Yong, P.; Allaire, C.; Bedaiwy, M. Intricate Connections between the Microbiota and Endometriosis. Int. J. Mol. Sci. 2021, 22, 5644. [Google Scholar] [CrossRef]
- Chadchan, S.B.; Popli, P.; Ambati, C.R.; Tycksen, E.; Han, S.J.; Bulun, S.E.; Putluri, N.; Biest, S.W.; Kommagani, R. Gut microbiota–derived short-chain fatty acids protect against the progression of endometriosis. Life Sci. Alliance 2021, 4, e202101224. [Google Scholar] [CrossRef]
- Lee, Y.; Kim, Y.-K. Understanding the Connection between the Gut–Brain Axis and Stress/Anxiety Disorders. Curr. Psychiatry Rep. 2021, 23, 22. [Google Scholar] [CrossRef]
- Chadchan, S.B.; Singh, V.; Kommagani, R. Female reproductive dysfunctions and the gut microbiota. J. Mol. Endocrinol. 2022, 69, R81–R94. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | No (%) |
|---|---|
| Age (years) | (18–49) (34) 6.804 (1) |
| Presence of digestive endometriosis | 44 (48.4) (2) |
| Endometriosis-related digestive surgery | 44 (44) |
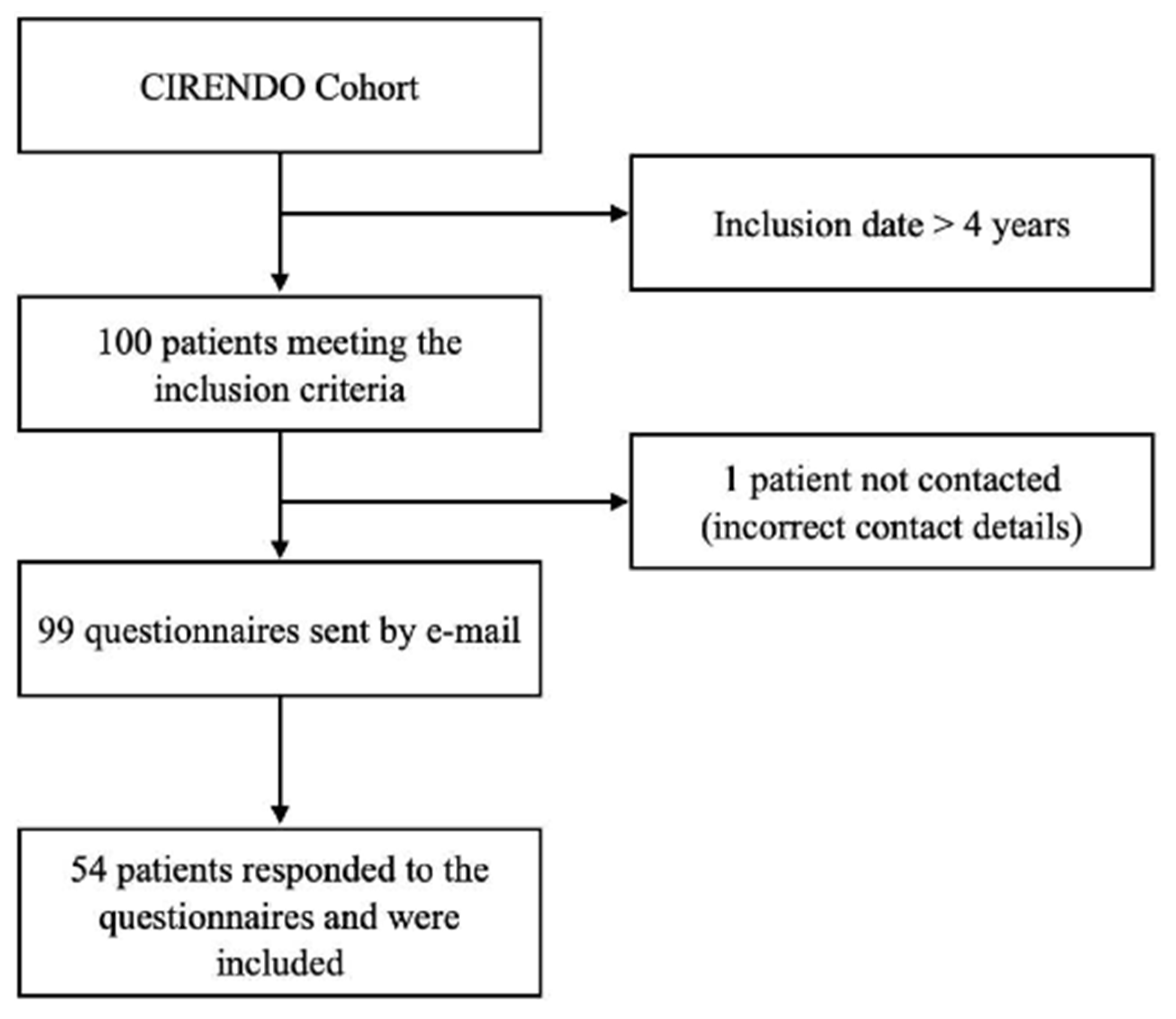
| Response to the questionnaires | 54 (54) |
| Variables | No (%) |
|---|---|
| Age (years) | (18–49) (34.5) 7.427 (1) |
| BMI (kg/m2) | (16.87–34.56) (24.85) 4.099 (1) |
| Age at diagnosis of endometriosis (years) | (17–47) (31) 7.836 (1) |
| Presence of digestive endometriosis | 25 (50) (2) |
| Endometriosis-related digestive surgery | 26 (48.1) |
| History of IBS | 10 (18.5) |
| History of ED | 3 (5.6) |
| History of anxiety and depressive disorders | 5 (9.3) |
| Delay in diagnosis of endometriosis > 6 years | 38 (70.4) |
| Regular abdominal pain | 35 (64.8) |
| Pain not related to the menstrual cycle | 24/35 (68.6) |
| Regular use of analgesics | 15 (27.8) |
| Regular use of anxiolytics | 6 (11.1) |
| Ongoing hormone treatment for endometriosis | 33 (61.1) |
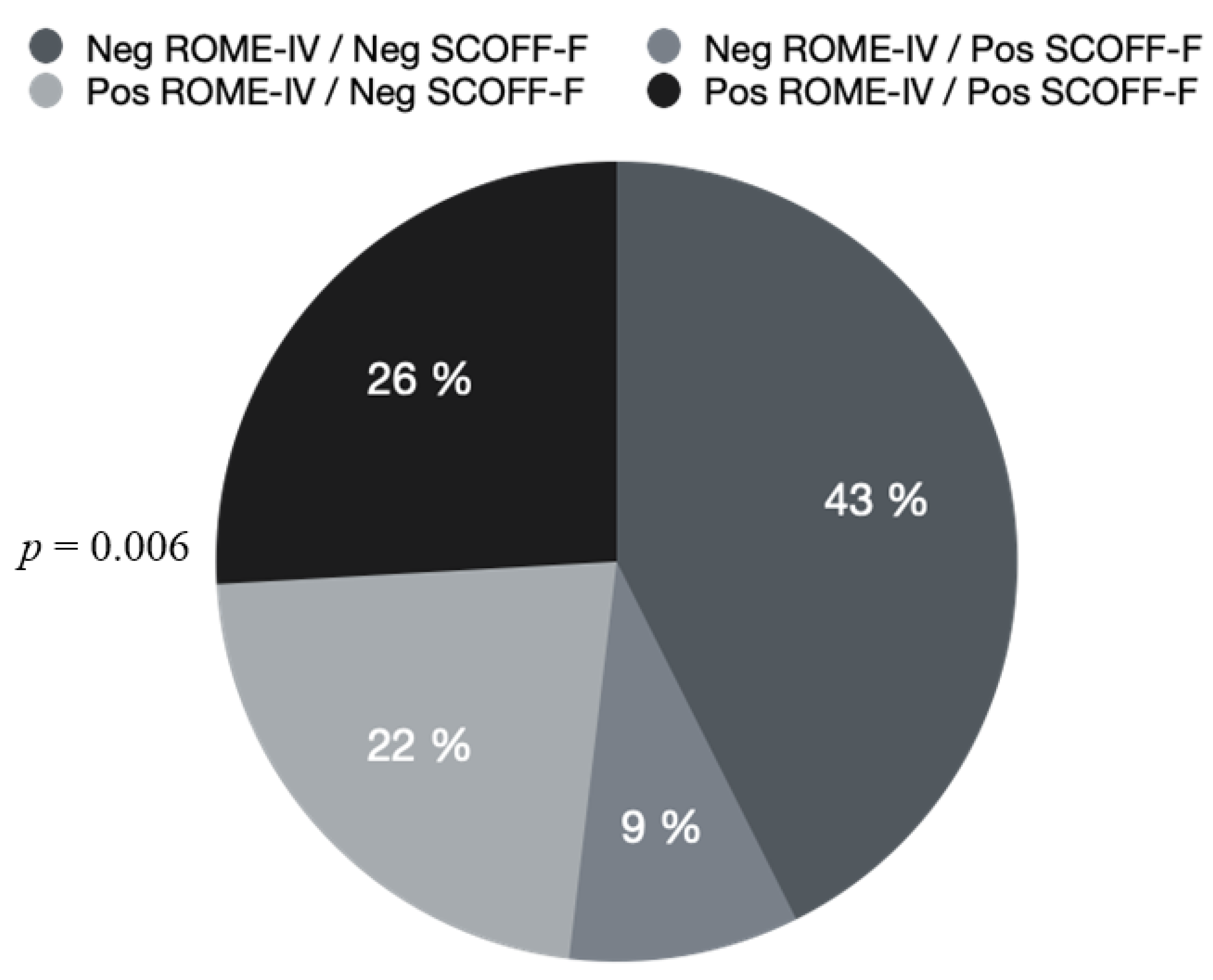
| Positive SCOFF-F | 19 (35.2) |
| Positive EAT-26 | 10 (18.5) |
| Positive ROME-IV | 26 (48.1) |
| Positive HAD-Anxiety | 33 (61.1) |
| Positive HAD-Depression | 18 (33.3) |
| Positive HAD-Anxiety and Depression | 12 (22.2) |
| Negative ROME-IV No (%) | Positive ROME-IV No (%) | p Value (<0.05 *) | |
|---|---|---|---|
| Positive EAT-26 No (%) | 3 (5.6) | 7 (13) | p = 0.169 |
| Negative EAT-26 No (%) | 25 (46.3) | 19 (35.2) | |
| Presence of digestive endometriosis No (%) (1) | 15 (30) (1) | 10 (20) (1) | p = 0.258 |
| Absence of digestive endometriosis No (%) (1) | 11 (22) (1) | 14 (28) (1) | |
| Endometriosis-related digestive surgery No (%) | 14 (25.9) | 12 (22.2) | p = 0.777 |
| Absence of endometriosis-related digestive surgery No (%) | 14 (25.9) | 14 (25.9) | |
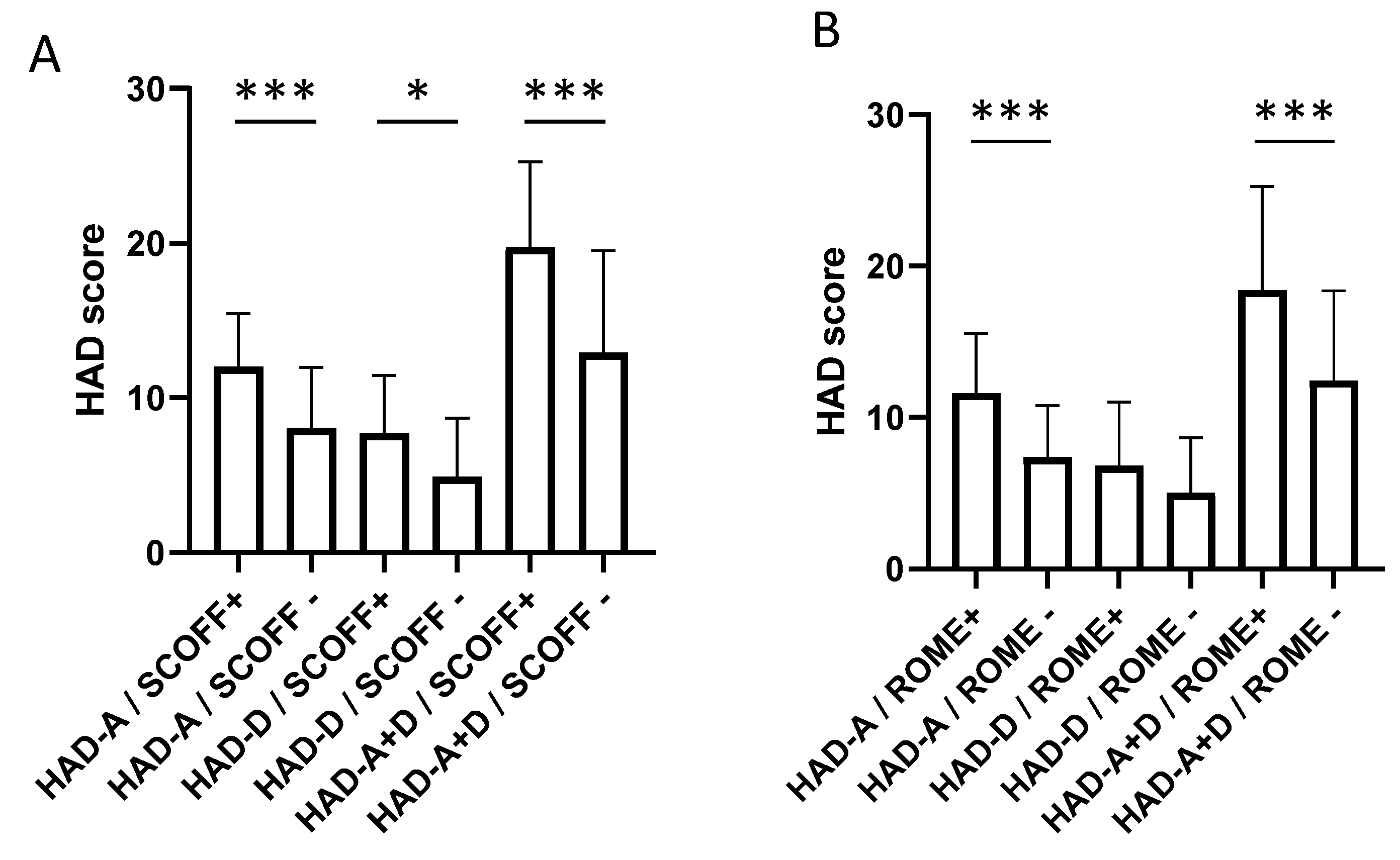
| Positive HAD-Anxiety No (%) | 11 (20.4) | 22 (40.7) | p = 0.001 * |
| Negative HAD-Anxiety No (%) | 17 (31.5) | 4 (7.4) | |
| Positive HAD-Depression No (%) | 8 (14.8) | 10 (18.5) | p = 0.441 |
| Negative HAD-Depression No (%) | 20 (37) | 16 (29.6) | |
| Both positive HAD-Anxiety and Depression No (%) | 2 (3.7) | 10 (18.5) | p = 0.008 * |
| HAD-Anxiety and Depression both non-positive No (%) | 26 (48.1) | 16 (29.6) |
| Negative SCOFF-F No (%) | Positive SCOFF-F No (%) | p Value (<0.05 *) | |
|---|---|---|---|
| Presence of digestive endometriosis No (%) (2) | 18 (36) (2) | 7 (14) (2) | p = 0.239 |
| Absence of digestive endometriosisNo (%) (2) | 14 (28) (2) | 11 (22) (2) | |
| Endometriosis-related digestive surgeryNo (%) | 19 (35.2) | 7 (13) | p = 0.221 |
| Absence of endometriosis-related digestive surgeryNo (%) | 16 (29.6) | 12 (22.2) | |
| Positive HAD-AnxietyNo (%) | 17 (31.5) | 16 (29.6) | p = 0.018 * |
| Negative HAD-AnxietyNo (%) | 18 (33.3) | 3 (5.5) | |
| Positive HAD-DepressionNo (%) | 10 (18.5) | 8 (14.8) | p = 0.314 |
| Negative HAD-Depression No (%) | 25 (46.3) | 11 (20.4) | |
| Both positive HAD-Anxiety and DepressionNo (%) | 5 (9.3) | 7 (13) | p = 0.057 |
| HAD-Anxiety and Depression both non-positiveNo (%) | 30 (55.6) | 12 (22.2) | |
| Francis score 0-199 No (%) (1) | 5 (19.2) (1) | 3 (11.5) (1) | p = 0.508 |
| Francis score 200-399 No (%) (1) | 6 (23.1) (1) | 10 (38.5) (1) | |
| Francis score ≥ 400No (%) (1) | 1 (3.8) (1) | 1 (3.8) (1) |
| Absence of Response to the Questionnaires No (%) | Response to the Questionnaires No (%) | p Value (<0.05 *) | |
|---|---|---|---|
| Presence of digestive endometriosis No (%) (1) | 22 (24.2) (1) | 25 (27.5) (1) | p = 0.728 |
| Absence of digestive endometriosis No (%) (1) | 19 (20.9) (1) | 25 (27.5) (1) | |
| Endometriosis-related digestive surgeryNo (%) | 18 (18) | 26 (26) | p = 0.365 |
| Absence of endometriosis-related digestive surgery No (%) | 28 (28) | 28 (28) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aupetit, A.; Grigioni, S.; Roman, H.; Coëffier, M.; Bréant, A.; Hennetier, C.; Achamrah, N. Association between Endometriosis, Irritable Bowel Syndrome and Eating Disorders: ENDONUT Pilot Study. J. Clin. Med. 2022, 11, 5773. https://doi.org/10.3390/jcm11195773
Aupetit A, Grigioni S, Roman H, Coëffier M, Bréant A, Hennetier C, Achamrah N. Association between Endometriosis, Irritable Bowel Syndrome and Eating Disorders: ENDONUT Pilot Study. Journal of Clinical Medicine. 2022; 11(19):5773. https://doi.org/10.3390/jcm11195773
Chicago/Turabian StyleAupetit, Alexandra, Sébastien Grigioni, Horace Roman, Moïse Coëffier, Amélie Bréant, Clotilde Hennetier, and Najate Achamrah. 2022. "Association between Endometriosis, Irritable Bowel Syndrome and Eating Disorders: ENDONUT Pilot Study" Journal of Clinical Medicine 11, no. 19: 5773. https://doi.org/10.3390/jcm11195773
APA StyleAupetit, A., Grigioni, S., Roman, H., Coëffier, M., Bréant, A., Hennetier, C., & Achamrah, N. (2022). Association between Endometriosis, Irritable Bowel Syndrome and Eating Disorders: ENDONUT Pilot Study. Journal of Clinical Medicine, 11(19), 5773. https://doi.org/10.3390/jcm11195773