

Sibling Influences on Trajectories of Maladaptive Behaviors in Autism

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.3. Measures
2.4. Statistical Analyses
3. Results
3.1. ABC Trajectory Models
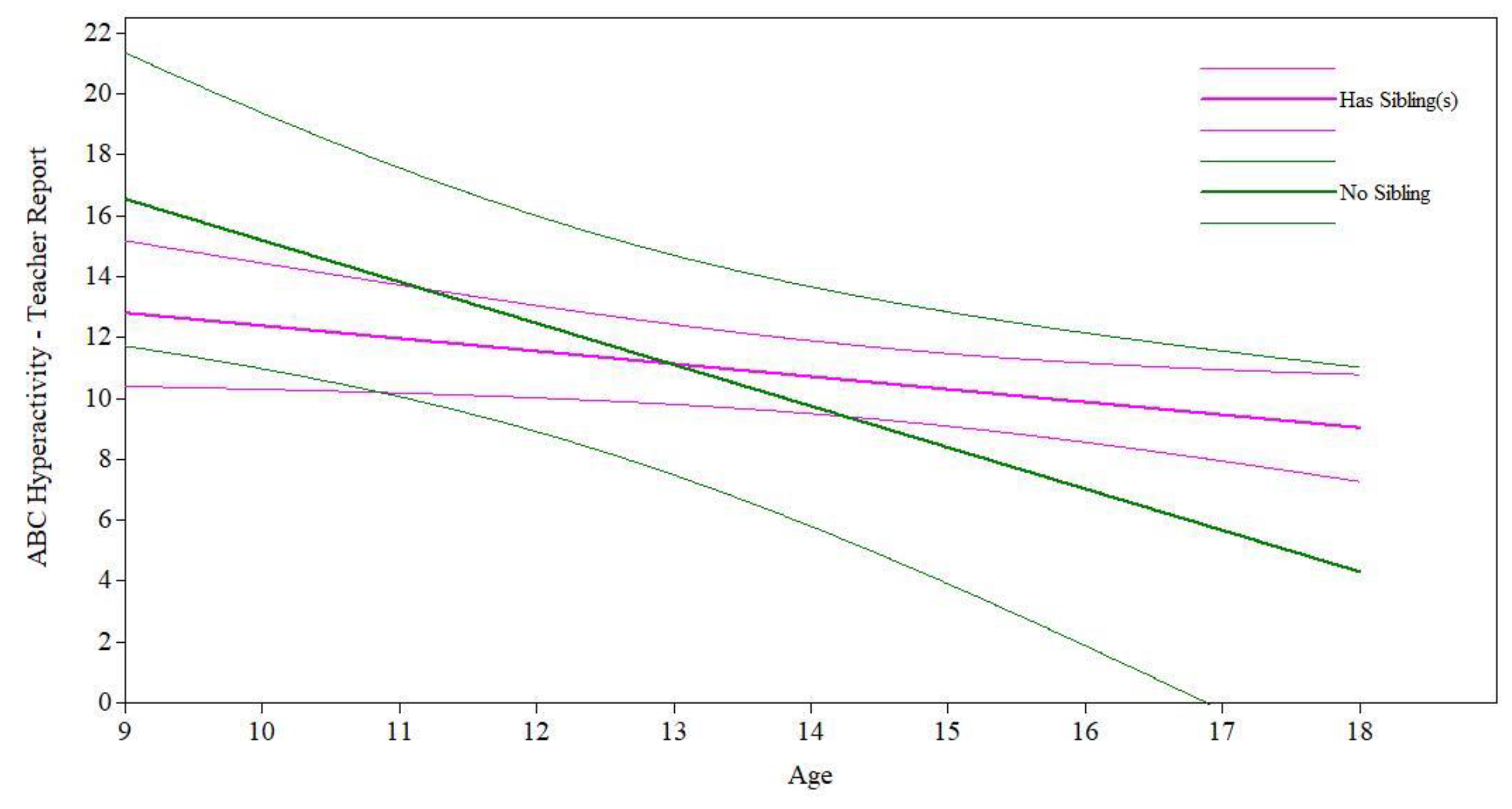
3.2. Presence of a Sibling Analyses
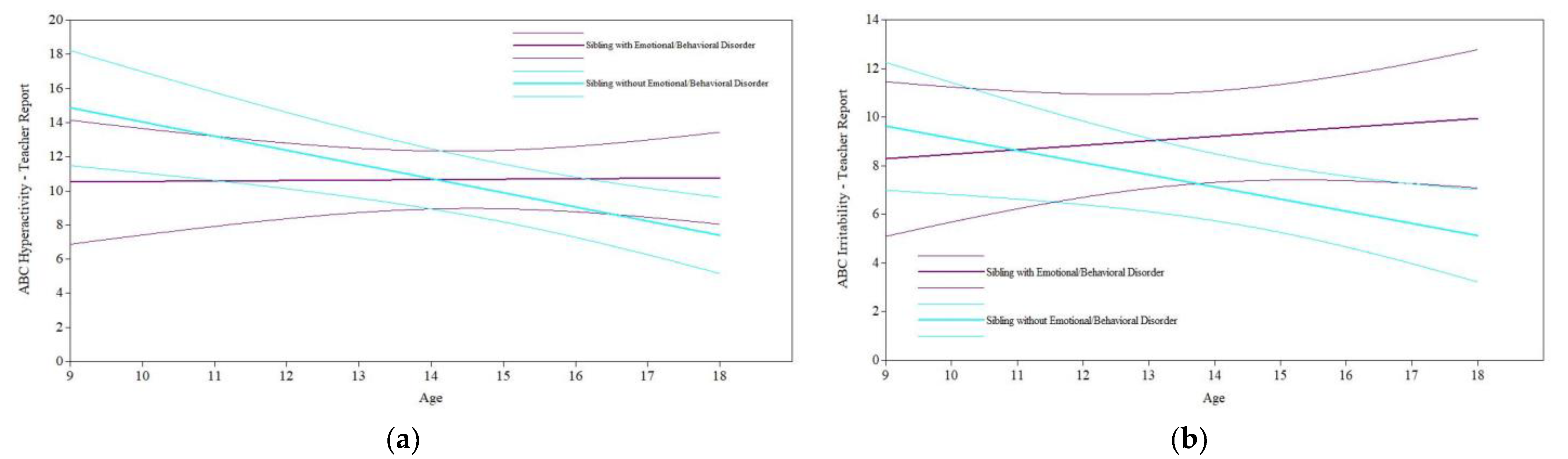
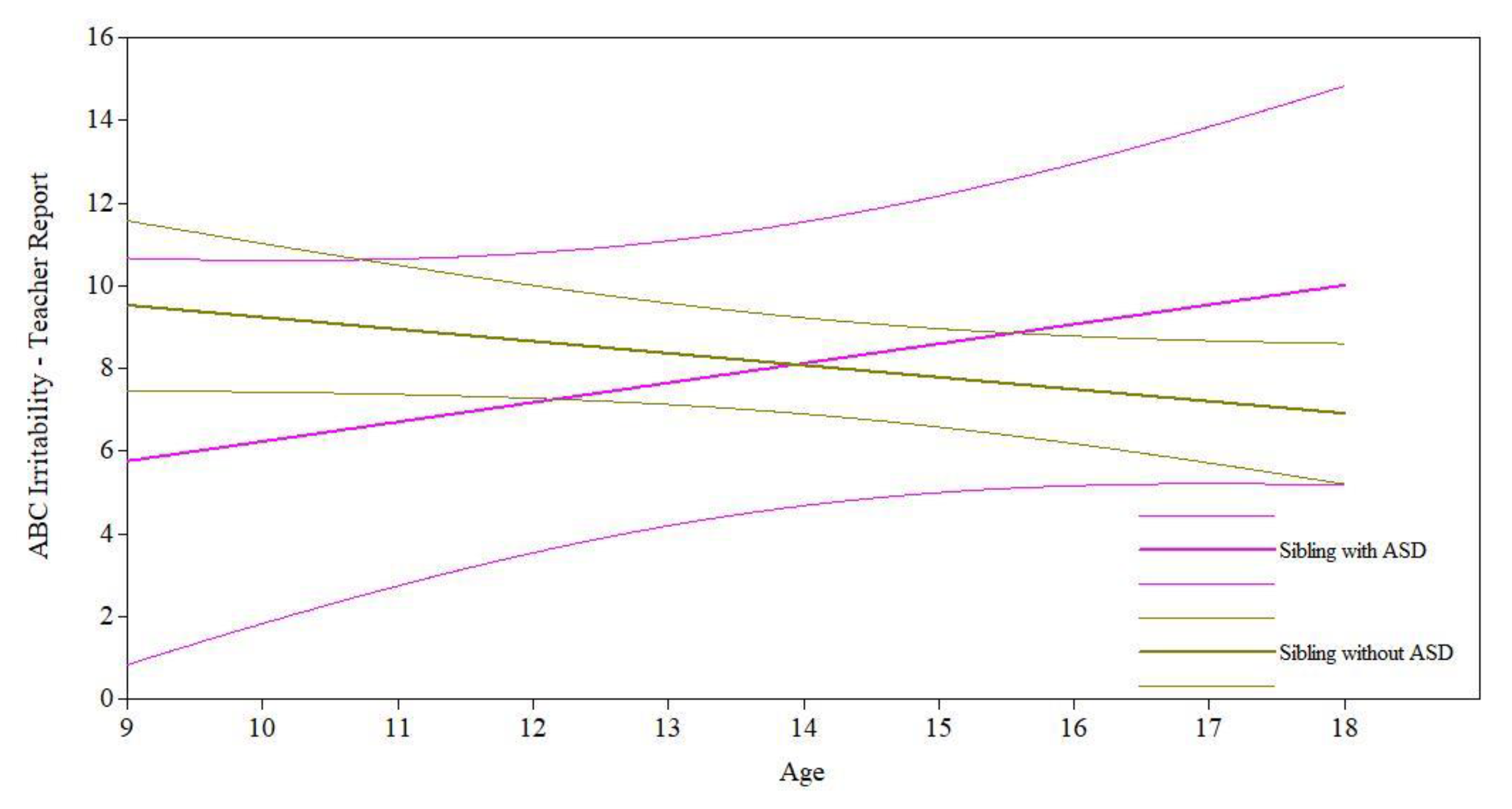
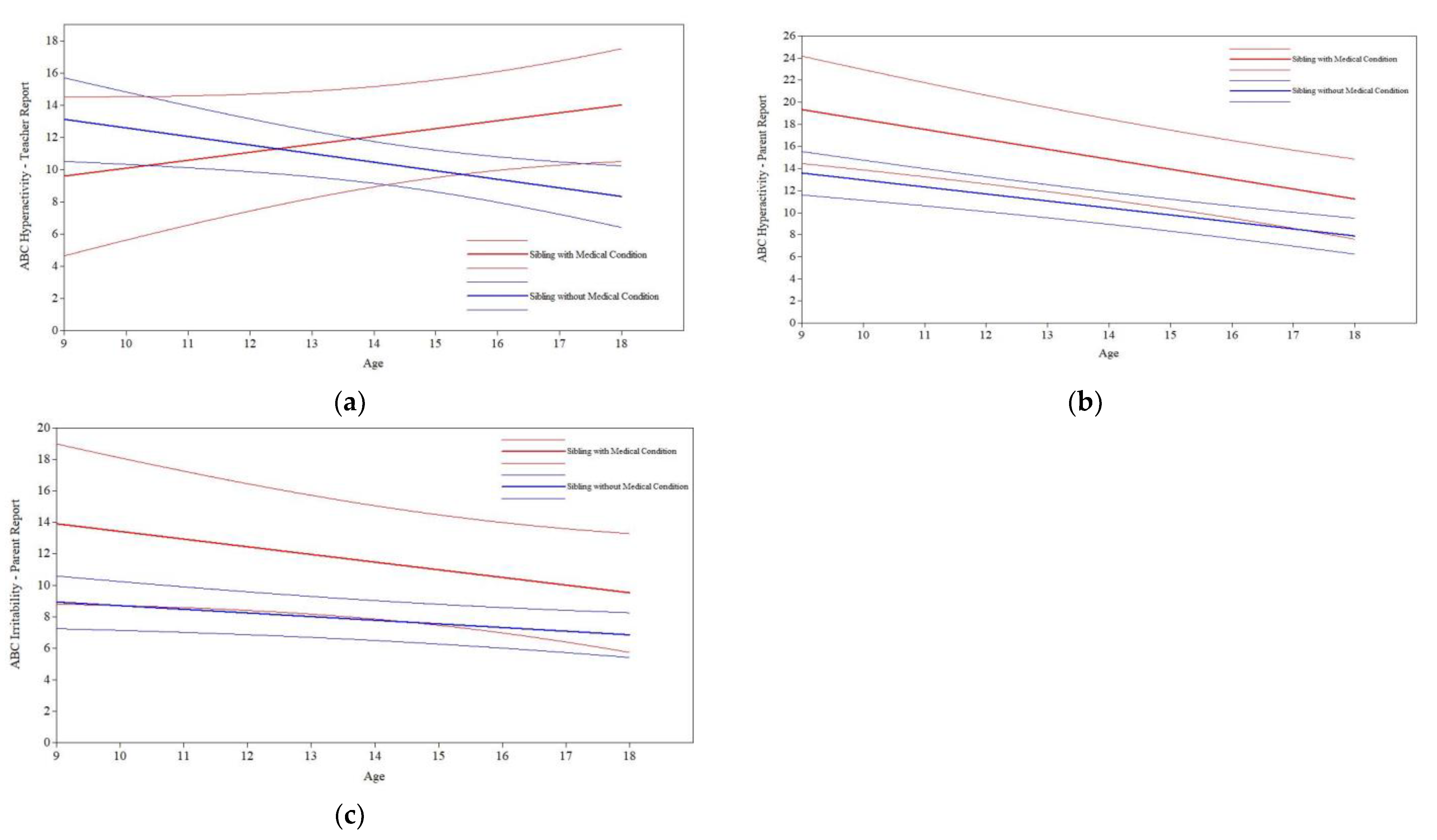
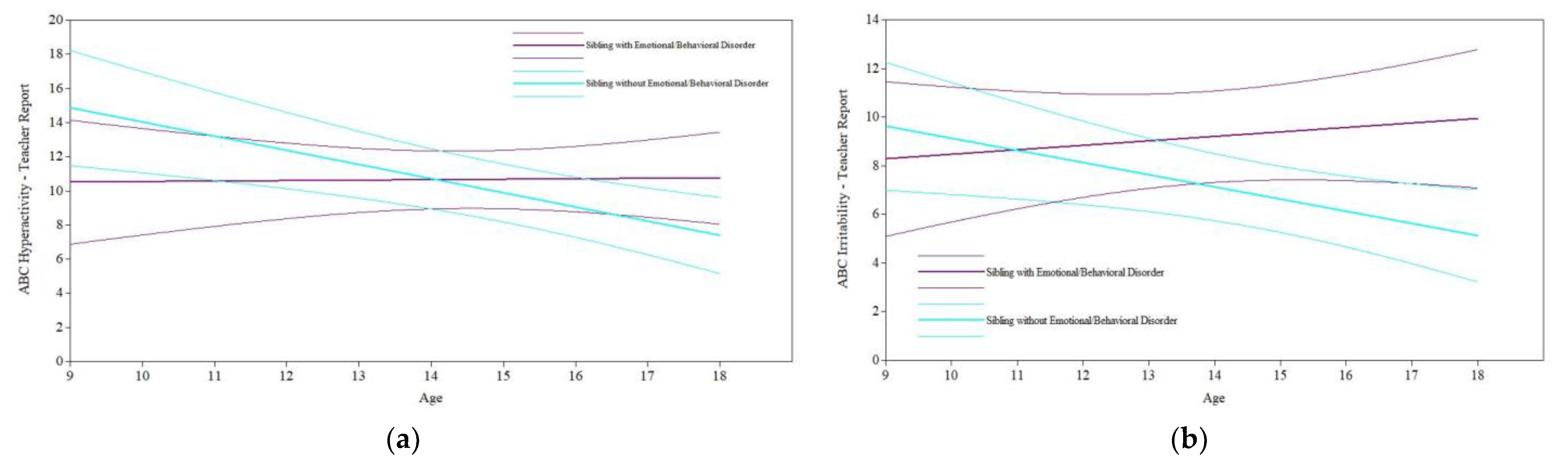
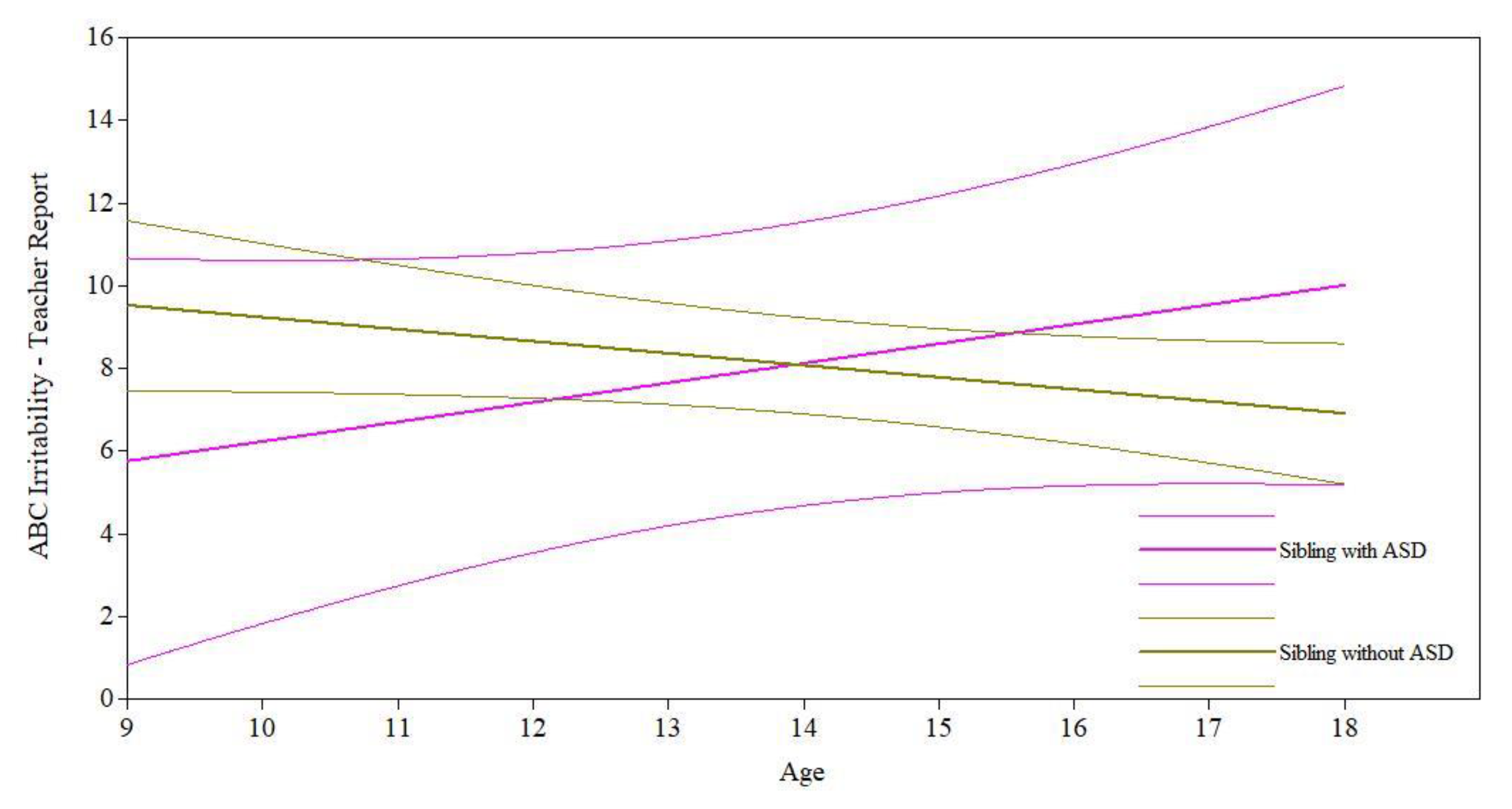
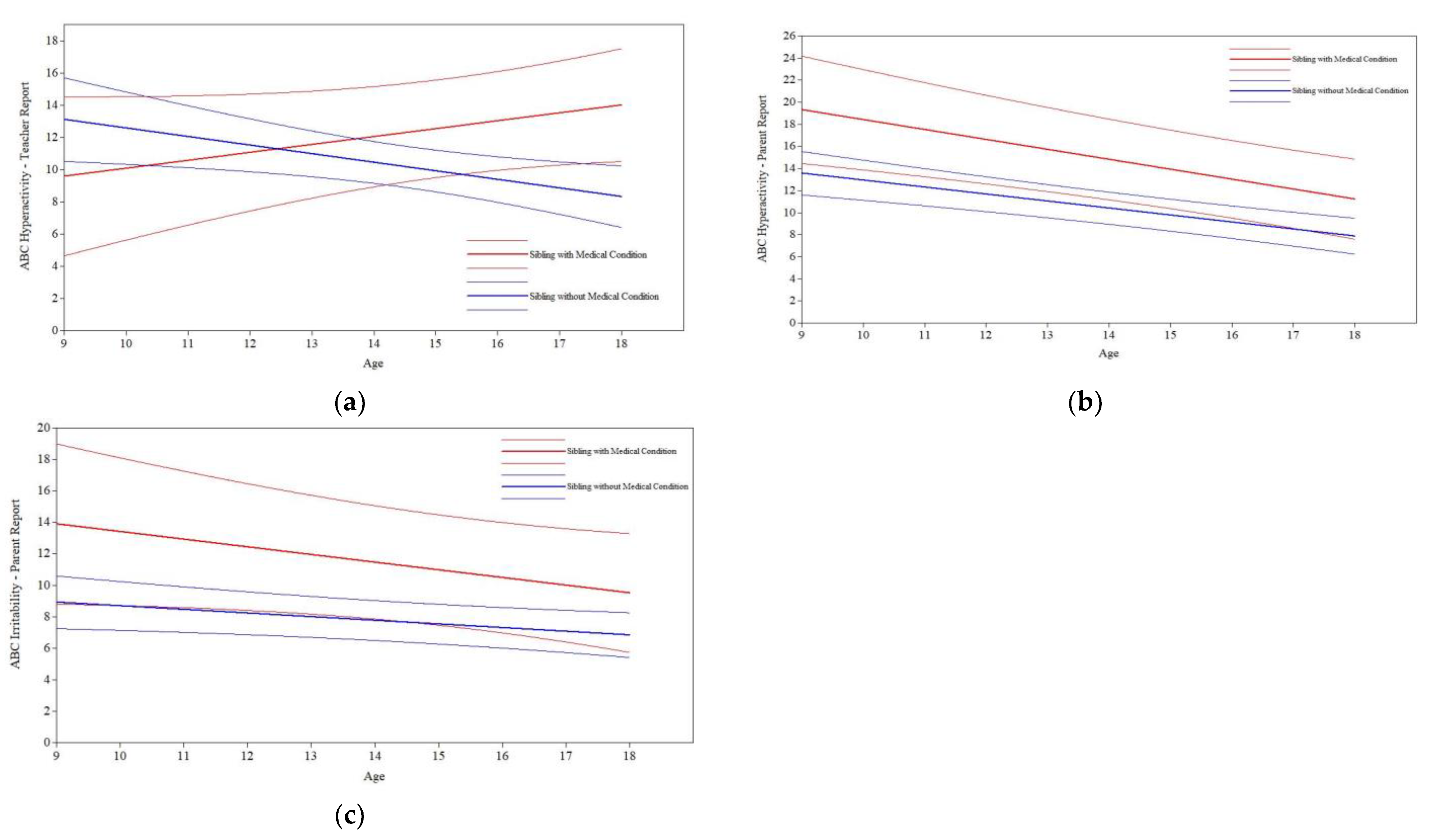
3.3. Sibling Diagnostic Predictors Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cicirelli, V. Sibling Relationships Across the Life Span; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2013; ISBN 978-1-4757-6509-0. [Google Scholar]
- Dunn, J. Siblings and Socialization. In Handbook of Socialization: Theory and Research; The Guilford Press: New York, NY, USA, 2007; pp. 309–327. ISBN 978-1-59385-332-7. [Google Scholar]
- Lamb, M.E.; Sutton-Smith, B.; Sutton-Smith, B.; Lamb, M.E. Sibling Relationships: Their Nature and Significance Across the Lifespan; Psychology Press: New York, NY, USA, 2014; ISBN 978-1-315-80278-7. [Google Scholar]
- Ferraioli, S.J.; Hansford, A.; Harris, S.L. Benefits of Including Siblings in the Treatment of Autism Spectrum Disorders. Cogn. Behav. Pract. 2012, 19, 413–422. [Google Scholar] [CrossRef]
- Knott, F.; Lewis, C.; Williams, T. Sibling Interaction of Children with Autism: Development Over 12 Months. J. Autism Dev. Disord. 2007, 37, 1987–1995. [Google Scholar] [CrossRef] [PubMed]
- Orsmond, G.I.; Seltzer, M.M. Siblings of Individuals with Autism Spectrum Disorders across the Life Course. Ment. Retard. Dev. Disabil. Res. Rev. 2007, 13, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Rosen, N.E.; McCauley, J.B.; Lord, C. Influence of Siblings on Adaptive Behavior Trajectories in Autism Spectrum Disorder. Autism 2022, 26, 135–145. [Google Scholar] [CrossRef] [PubMed]
- Ben-Itzchak, E.; Zukerman, G.; Zachor, D.A. Having Older Siblings Is Associated with Less Severe Social Communication Symptoms in Young Children with Autism Spectrum Disorder. J. Abnorm. Child. Psychol. 2016, 44, 1613–1620. [Google Scholar] [CrossRef]
- Ben-Itzchak, E.; Nachshon, N.; Zachor, D.A. Having Siblings Is Associated with Better Social Functioning in Autism Spectrum Disorder. J. Abnorm. Child. Psychol. 2019, 47, 921–931. [Google Scholar] [CrossRef]
- Matthews, N.L.; Goldberg, W.A.; Lukowski, A.F. Theory of Mind in Children with Autism Spectrum Disorder: Do Siblings Matter? Autism Res. 2013, 6, 443–453. [Google Scholar] [CrossRef]
- Matthews, N.L.; Goldberg, W.A. Theory of Mind in Children with and without Autism Spectrum Disorder: Associations with the Sibling Constellation. Autism 2018, 22, 311–321. [Google Scholar] [CrossRef]
- O’Brien, K.; Slaughter, V.; Peterson, C.C. Sibling Influences on Theory of Mind Development for Children with ASD. J. Child. Psychol. Psychiatry 2011, 52, 713–719. [Google Scholar] [CrossRef]
- Whiteman, S.D.; McHale, S.M.; Soli, A. Theoretical Perspectives on Sibling Relationships. J. Fam. Theory Rev. 2011, 3, 124–139. [Google Scholar] [CrossRef] [Green Version]
- Dunn, J. Sibling Influences on Childhood Development. J. Child. Psychol. Psychiatry 1988, 29, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Shattuck, P.T.; Seltzer, M.M.; Greenberg, J.S.; Orsmond, G.I.; Bolt, D.; Kring, S.; Lounds, J.; Lord, C. Change in Autism Symptoms and Maladaptive Behaviors in Adolescents and Adults with an Autism Spectrum Disorder. J. Autism Dev. Disord. 2007, 37, 1735–1747. [Google Scholar] [CrossRef] [PubMed]
- De Bildt, A.; Sytema, S.; Kraijer, D.; Sparrow, S.; Minderaa, R. Adaptive Functioning and Behaviour Problems in Relation to Level of Education in Children and Adolescents with Intellectual Disability. J. Intellect. Disabil. Res. 2005, 49, 672–681. [Google Scholar] [CrossRef] [PubMed]
- Baghdadli, A.; Pascal, C.; Grisi, S.; Aussilloux, C. Risk Factors for Self-Injurious Behaviours among 222 Young Children with Autistic Disorders. J. Intellect. Disabil. Res. 2003, 47, 622–627. [Google Scholar] [CrossRef] [PubMed]
- Holden, B.; Gitlesen, J.P. A Total Population Study of Challenging Behaviour in the County of Hedmark, Norway: Prevalence, and Risk Markers. Res. Dev. Disabil. 2006, 27, 456–465. [Google Scholar] [CrossRef]
- Matson, J.L.; Wilkins, J.; Macken, J. The Relationship of Challenging Behaviors to Severity and Symptoms of Autism Spectrum Disorders. J. Ment. Health Res. Intellect. Disabil. 2008, 2, 29–44. [Google Scholar] [CrossRef]
- Simonoff, E.; Pickles, A.; Charman, T.; Chandler, S.; Loucas, T.; Baird, G. Psychiatric Disorders in Children with Autism Spectrum Disorders: Prevalence, Comorbidity, and Associated Factors in a Population-Derived Sample. J. Am. Acad. Child. Adolesc. Psychiatry 2008, 47, 921–929. [Google Scholar] [CrossRef]
- Kim, J.A.; Szatmari, P.; Bryson, S.E.; Streiner, D.L.; Wilson, F.J. The Prevalence of Anxiety and Mood Problems among Children with Autism and Asperger Syndrome. Autism 2000, 4, 117–132. [Google Scholar] [CrossRef]
- Hansen, S.N.; Schendel, D.E.; Francis, R.W.; Windham, G.C.; Bresnahan, M.; Levine, S.Z.; Reichenberg, A.; Gissler, M.; Kodesh, A.; Bai, D.; et al. Recurrence Risk of Autism in Siblings and Cousins: A Multinational, Population-Based Study. J. Am. Acad. Child. Adolesc. Psychiatry 2019, 58, 866–875. [Google Scholar] [CrossRef]
- Ozonoff, S.; Young, G.S.; Carter, A.; Messinger, D.; Yirmiya, N.; Zwaigenbaum, L.; Bryson, S.; Carver, L.J.; Constantino, J.N.; Dobkins, K.; et al. Recurrence Risk for Autism Spectrum Disorders: A Baby Siblings Research Consortium Study. Pediatrics 2011, 128, e488–e495. [Google Scholar] [CrossRef] [Green Version]
- Maenner, M.J.; Shaw, K.A.; Bakian, A.V.; Bilder, D.A.; Durkin, M.S.; Esler, A.; Furnier, S.M.; Hallas, L.; Hall-Lande, J.; Hudson, A.; et al. Prevalence and Characteristics of Autism Spectrum Disorder Among Children Aged 8 Years—Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2018. MMWR Surveill. Summ. 2021, 70, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Charman, T.; Young, G.S.; Brian, J.; Carter, A.; Carver, L.J.; Chawarska, K.; Curtin, S.; Dobkins, K.; Elsabbagh, M.; Georgiades, S.; et al. Non-ASD Outcomes at 36 Months in Siblings at Familial Risk for Autism Spectrum Disorder (ASD): A Baby Siblings Research Consortium (BSRC) Study. Autism Res. 2017, 10, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Messinger, D.; Young, G.S.; Ozonoff, S.; Dobkins, K.; Carter, A.; Zwaigenbaum, L.; Landa, R.J.; Charman, T.; Stone, W.L.; Constantino, J.N.; et al. Beyond Autism: A Baby Siblings Research Consortium Study of High-Risk Children at Three Years of Age. J. Am. Acad. Child. Adolesc. Psychiatry 2013, 52, 300–308. [Google Scholar] [CrossRef] [PubMed]
- Meyer, K.A.; Ingersoll, B.; Hambrick, D.Z. Factors Influencing Adjustment in Siblings of Children with Autism Spectrum Disorders. Res. Autism Spectr. Disord. 2011, 5, 1413–1420. [Google Scholar] [CrossRef]
- Orsmond, G.I.; Seltzer, M.M. Adolescent Siblings of Individuals with an Autism Spectrum Disorder: Testing a Diathesis-Stress Model of Sibling Well-Being. J. Autism Dev. Disord. 2009, 39, 1053–1065. [Google Scholar] [CrossRef] [PubMed]
- Dumas, J.E.; Wolf, L.C.; Fisman, S.N.; Culligan, A. Parenting Stress, Child Behavior Problems, and Dysphoria in Parents of Children with Autism, down Syndrome, Behavior Disorders, and Normal Development. Exceptionality 1991, 2, 97–110. [Google Scholar] [CrossRef]
- Sikora, D.; Moran, E.; Orlich, F.; Hall, T.A.; Kovacs, E.A.; Delahaye, J.; Clemons, T.E.; Kuhlthau, K. The Relationship between Family Functioning and Behavior Problems in Children with Autism Spectrum Disorders. Res. Autism Spectr. Disord. 2013, 7, 307–315. [Google Scholar] [CrossRef]
- Kirchhofer, S.M.; Orm, S.; Haukeland, Y.B.; Fredriksen, T.; Wakefield, C.E.; Fjermestad, K.W. A Systematic Review of Social Support for Siblings of Children with Neurodevelopmental Disorders. Res. Dev. Disabil. 2022, 126, 104234. [Google Scholar] [CrossRef]
- Rosen, N.E.; Schiltz, H.K.; Lord, C. Teacher- and Parent-Reported Trajectories of Challenging Behavior Among Individuals with Autism. medRxiv 2022. [Google Scholar] [CrossRef]
- Anderson, D.K.; Maye, M.P.; Lord, C. Changes in Maladaptive Behaviors from Midchildhood to Young Adulthood in Autism Spectrum Disorder. Am. J. Intellect. Dev. Disabil. 2011, 116, 381–397. [Google Scholar] [CrossRef] [Green Version]
- Stringer, D.; Kent, R.; Briskman, J.; Lukito, S.; Charman, T.; Baird, G.; Lord, C.; Pickles, A.; Simonoff, E. Trajectories of Emotional and Behavioral Problems from Childhood to Early Adult Life. Autism 2020, 24, 1011–1024. [Google Scholar] [CrossRef] [PubMed]
- Dickson, K.S.; Suhrheinrich, J.; Rieth, S.R.; Stahmer, A.C. Parent and Teacher Concordance of Child Outcomes for Youth with Autism Spectrum Disorder. J. Autism Dev. Disord. 2018, 48, 1423–1435. [Google Scholar] [CrossRef] [PubMed]
- De Los Reyes, A.; Kazdin, A.E. Informant Discrepancies in the Assessment of Childhood Psychopathology: A Critical Review, Theoretical Framework, and Recommendations for Further Study. Psychol. Bull. 2005, 131, 483. [Google Scholar] [CrossRef] [PubMed]
- Anderson, D.K.; Liang, J.W.; Lord, C. Predicting Young Adult Outcome among More and Less Cognitively Able Individuals with Autism Spectrum Disorders. J. Child. Psychol. Psychiatry 2014, 55, 485–494. [Google Scholar] [CrossRef] [PubMed]
- Lord, C.; Risi, S.; Lambrecht, L.; Cook, E.H.; Leventhal, B.L.; DiLavore, P.C.; Pickles, A.; Rutter, M. The Autism Diagnostic Observation Schedule-Generic: A Standard Measure of Social and Communication Deficits Associated with the Spectrum of Autism. J. Autism Dev. Disord. 2000, 30, 205–223. [Google Scholar] [CrossRef]
- Lord, C.; Rutter, M.; DiLavore, P.; Risi, S.; Gotham, K.; Bishop, S. Autism Diagnostic Observation Schedule–2nd Edition (ADOS-2); Western Psychological Services: Torrance, CA, USA, 2012. [Google Scholar]
- Gotham, K.; Pickles, A.; Lord, C. Standardizing ADOS Scores for a Measure of Severity in Autism Spectrum Disorders. J. Autism Dev. Disord. 2009, 39, 693–705. [Google Scholar] [CrossRef]
- Wechsler, D. The Wechsler Abbreviated Scale for Intelligence; The Psychological Corporation: San Antonio, TX, USA, 1999. [Google Scholar]
- Wechsler, D. Weschler Intelligence Scale for Children: Third Edition Manual, 3rd ed.; The Psychological Corporation: San Antonio, TX, USA, 1991. [Google Scholar]
- Elliot, C.D. The Nature and Structure of Children’s Abilities: Evidence From the Differential Ability Scales. J. Psychoeduc. Assess. 1990, 8, 376–390. [Google Scholar] [CrossRef]
- Elliott, C.D. Differential Ability Scales, 2nd ed.; Harcourt Assessment: San Antonio, TX, USA, 2007. [Google Scholar]
- Aman, M.G.; Singh, N.N.; Stewart, A.W.; Field, C.J. The Aberrant Behavior Checklist: A Behavior Rating Scale for the Assessment of Treatment Effects. Am. J. Ment. Defic. 1985, 89, 485–491. [Google Scholar]
- Fok, M.; Bal, V.H. Differences in Profiles of Emotional Behavioral Problems across Instruments in Verbal versus Minimally Verbal Children with Autism Spectrum Disorder. Autism Res. 2019, 12, 1367–1375. [Google Scholar] [CrossRef]
- Aman, M.G.; Richmond, G.; Stewart, A.W.; Bell, J.C.; Kissel, R.C. The Aberrant Behavior Checklist: Factor Structure and the Effect of Subject Variables in American and New Zealand Facilities. Am. J. Ment. Defic. 1987, 91, 570–578. [Google Scholar]
- Rojahn, J.; Helsel, W.J. The Aberrant Behavior Checklist with Children and Adolescents with Dual Diagnosis. J. Autism Dev. Disord. 1991, 21, 17–28. [Google Scholar] [CrossRef] [PubMed]
- Brinkley, J.; Nations, L.; Abramson, R.K.; Hall, A.; Wright, H.H.; Gabriels, R.; Gilbert, J.R.; Pericak-Vance, M.A.; Cuccaro, M.L. Factor Analysis of the Aberrant Behavior Checklist in Individuals with Autism Spectrum Disorders. J. Autism Dev. Disord. 2007, 37, 1949–1959. [Google Scholar] [CrossRef]
- Kaat, A.J.; Lecavalier, L.; Aman, M.G. Validity of the Aberrant Behavior Checklist in Children with Autism Spectrum Disorder. J. Autism Dev. Disord. 2014, 44, 1103–1116. [Google Scholar] [CrossRef]
- Norris, M.; Aman, M.G.; Mazurek, M.O.; Scherr, J.F.; Butter, E.M. Psychometric Characteristics of the Aberrant Behavior Checklist in a Well-Defined Sample of Youth with Autism Spectrum Disorder. Res. Autism Spectr. Disord. 2019, 62, 1–9. [Google Scholar] [CrossRef]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide-Eighth Edition; Muthén and Muthén: Los Angeles, CA, USA, 1998–2017. [Google Scholar]
- Finch, W.H.; Bolin, J.E. Multilevel Modeling Using Mplus; Chapman and Hall/CRC: Boca Raton, FL, USA, 2017; ISBN 1-315-16588-0. [Google Scholar]
- Luke, D.A. Multilevel Modeling; Sage Publications: Thousand Oaks, CA, USA, 2020; Volume 143, ISBN 1-5443-1030-5. [Google Scholar]
- Woodman, A.C.; Smith, L.E.; Greenberg, J.S.; Mailick, M.R. Change in Autism Symptoms and Maladaptive Behaviors in Adolescence and Adulthood: The Role of Positive Family Processes. J. Autism Dev. Disord. 2015, 45, 111–126. [Google Scholar] [CrossRef] [PubMed]
- Brown, W.H.; Odom, S.L. Strategies and Tactics for Promoting Generalization and Maintenance of Young Children’s Social Behavior. Res. Dev. Disabil. 1994, 15, 99–118. [Google Scholar] [CrossRef]
- Carr, E.G.; Darcy, M. Setting Generality of Peer Modeling in Children with Autism. J. Autism Dev. Disord. 1990, 20, 45–59. [Google Scholar] [CrossRef]
- Jahr, E.; Eldevik, S.; Eikeseth, S. Teaching Children with Autism to Initiate and Sustain Cooperative Play. Res. Dev. Disabil. 2000, 21, 151–169. [Google Scholar] [CrossRef]
- Bauminger, N.; Solomon, M.; Rogers, S.J. Externalizing and Internalizing Behaviors in ASD. Autism Res. 2010, 3, 101–112. [Google Scholar] [CrossRef]
- Cibralic, S.; Kohlhoff, J.; Wallace, N.; McMahon, C.; Eapen, V. A Systematic Review of Emotion Regulation in Children with Autism Spectrum Disorder. Res. Autism Spectr. Disord. 2019, 68, 101422. [Google Scholar] [CrossRef]
- Greenlee, J.L.; Stelter, C.R.; Piro-Gambetti, B.; Hartley, S.L. Trajectories of Dysregulation in Children with Autism Spectrum Disorder. J. Clin. Child. Adolesc. Psychol. 2021, 50, 858–873. [Google Scholar] [CrossRef] [PubMed]
- Kochanska, G.; Coy, K.C.; Murray, K.T. The Development of Self-Regulation in the First Four Years of Life. Child. Dev. 2001, 72, 1091–1111. [Google Scholar] [CrossRef] [PubMed]
- Olson, S.L.; Ip, K.I.; Gonzalez, R.; Beyers-Carlson, E.E.A.; Volling, B.L. Development of Externalizing Symptoms across the Toddler Period: The Critical Role of Older Siblings. J. Fam. Psychol. 2020, 34, 165–174. [Google Scholar] [CrossRef]
- Hastings, R.P. Behavioral Adjustment of Siblings of Children with Autism Engaged in Applied Behavior Analysis Early Intervention Programs: The Moderating Role of Social Support. J. Autism Dev. Disord. 2003, 33, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Ross, P.; Cuskelly, M. Adjustment, Sibling Problems and Coping Strategies of Brothers and Sisters of Children with Autistic Spectrum Disorder. J. Intellect. Dev. Disabil. 2006, 31, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Verté, S.; Roeyers, H.; Buysse, A. Behavioural Problems, Social Competence and Self-Concept in Siblings of Children with Autism. Child. Care Health Dev. 2003, 29, 193–205. [Google Scholar] [CrossRef] [PubMed]
- Hall, H.R.; Graff, J.C. Maladaptive Behaviors of Children with Autism: Parent Support, Stress, and Coping. Issues Compr. Pediatr. Nurs. 2012, 35, 194–214. [Google Scholar] [CrossRef]
- Smith, L.E.; Greenberg, J.S.; Seltzer, M.M.; Hong, J. Symptoms and Behavior Problems of Adolescents and Adults With Autism: Effects of Mother–Child Relationship Quality, Warmth, and Praise. Am. J. Ment. Retard. 2008, 113, 387–402. [Google Scholar] [CrossRef]
- Ganjiwale, D.; Ganjiwale, J.; Sharma, B.; Mishra, B. Quality of Life and Coping Strategies of Caregivers of Children with Physical and Mental Disabilities. J. Fam. Med. Prim. Care 2016, 5, 343–348. [Google Scholar] [CrossRef]
- Gupta, V.B. Comparison of Parenting Stress in Different Developmental Disabilities. J. Dev. Phys. Disabil. 2007, 19, 417–425. [Google Scholar] [CrossRef]
- Greene, R.W.; Beszterczey, S.K.; Katzenstein, T.; Park, K.; Goring, J. Are Students with ADHD More Stressful to Teach?: Patterns of Teacher Stress in an Elementary School Sample. J. Emot. Behav. Disord. 2002, 10, 79–89. [Google Scholar] [CrossRef]
- Lecavalier, L.; Leone, S.; Wiltz, J. The Impact of Behaviour Problems on Caregiver Stress in Young People with Autism Spectrum Disorders. J. Intellect. Disabil. Res. 2006, 50, 172–183. [Google Scholar] [CrossRef] [PubMed]
- Cicirelli, V.G. Sibling Influence Throughout the Lifespan. In Sibling Relationships; Psychology Press: London, UK, 1982; ISBN 978-1-315-80278-7. [Google Scholar]
- El-Ghoroury, N.H.; Romanczyk, R.G. Play Interactions of Family Members Towards Children with Autism. J. Autism Dev. Disord. 1999, 29, 249–258. [Google Scholar] [CrossRef]
- McCauley, J.B.; Pickles, A.; Huerta, M.; Lord, C. Defining Positive Outcomes in More and Less Cognitively Able Autistic Adults. Autism Res. 2020, 13, 1548–1560. [Google Scholar] [CrossRef] [PubMed]
- Orsmond, G.I.; Seltzer, M.M. Brothers and Sisters of Adults With Mental Retardation: Gendered Nature of the Sibling Relationship. Am. J. Ment. Retard. 2000, 105, 486–508. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hyperactivity | Irritability | Social Withdrawal | |
|---|---|---|---|
| Teacher Report | VIQ, ADOS-CSS, Reporter Consistency | VIQ, ADOS-CSS | VIQ, ADOS-CSS |
| Parent Report | VIQ | VIQ | VIQ, ADOS-CSS |
| Hyperactivity | Irritability | Social Withdrawal | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Teacher | Parent | Teacher | Parent | Teacher | Parent | |||||||
| Predictors | B on Intercept | B on Slope | B on Intercept | B on Slope | B on Intercept | B on Slope | B on Intercept | B on Slope | B on Intercept | B on Slope | B on Intercept | B on Slope |
| Presence of a Sibling | −3.75 | 0.94 ^ | −0.08 | 0.00 | −1.01 | 0.37 | 0.15 | 0.23 | −1.58 | 0.25 | −3.03 | 0.32 |
| Sibling Dx: Emotional/Behavioral Disorder | −4.34 | 0.86 * | 0.12 | −0.05 | −1.34 | 0.68 ^ | 1.01 | 0.04 | −0.86 | 0.30 | −0.26 | −0.10 |
| Sibling Dx: ASD | −3.80 | 0.62 | −0.26 | 0.01 | −3.77 | 0.76 ^ | 0.69 | 0.09 | 0.96 | −0.17 | −1.30 | −0.21 |
| Sibling Dx: Medical Condition | −3.52 | 1.02 * | 5.74 * | −0.27 | 0.68 | 0.32 | 4.98 ^ | −0.26 | −2.01 | 0.56 | 0.80 | 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rosen, N.E.; Schiltz, H.K.; Lord, C. Sibling Influences on Trajectories of Maladaptive Behaviors in Autism. J. Clin. Med. 2022, 11, 5349. https://doi.org/10.3390/jcm11185349
Rosen NE, Schiltz HK, Lord C. Sibling Influences on Trajectories of Maladaptive Behaviors in Autism. Journal of Clinical Medicine. 2022; 11(18):5349. https://doi.org/10.3390/jcm11185349
Chicago/Turabian StyleRosen, Nicole E., Hillary K. Schiltz, and Catherine Lord. 2022. "Sibling Influences on Trajectories of Maladaptive Behaviors in Autism" Journal of Clinical Medicine 11, no. 18: 5349. https://doi.org/10.3390/jcm11185349
APA StyleRosen, N. E., Schiltz, H. K., & Lord, C. (2022). Sibling Influences on Trajectories of Maladaptive Behaviors in Autism. Journal of Clinical Medicine, 11(18), 5349. https://doi.org/10.3390/jcm11185349