
Alterations in Glomerular Filtration Rates Using Different Algorithms in the Korean Population Visiting Local Clinics and Hospitals


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Analytical Methods
2.3. Definitions
2.4. Statistical Analysis
2.5. Ethics
3. Results
3.1. Baseline Characteristics of Subjects
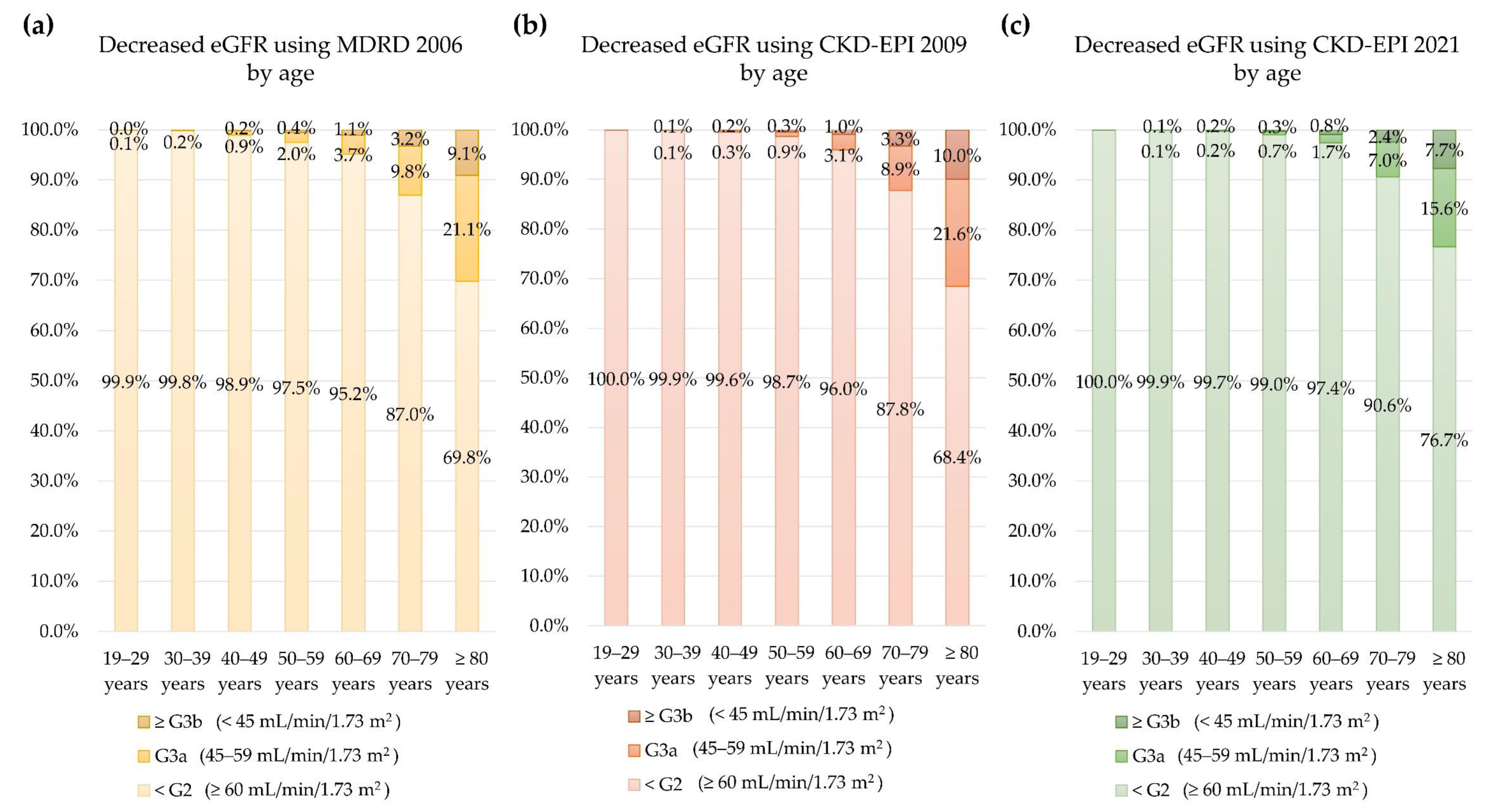
3.2. eGFR by Age
3.3. Overall Agreement among the Three Equations
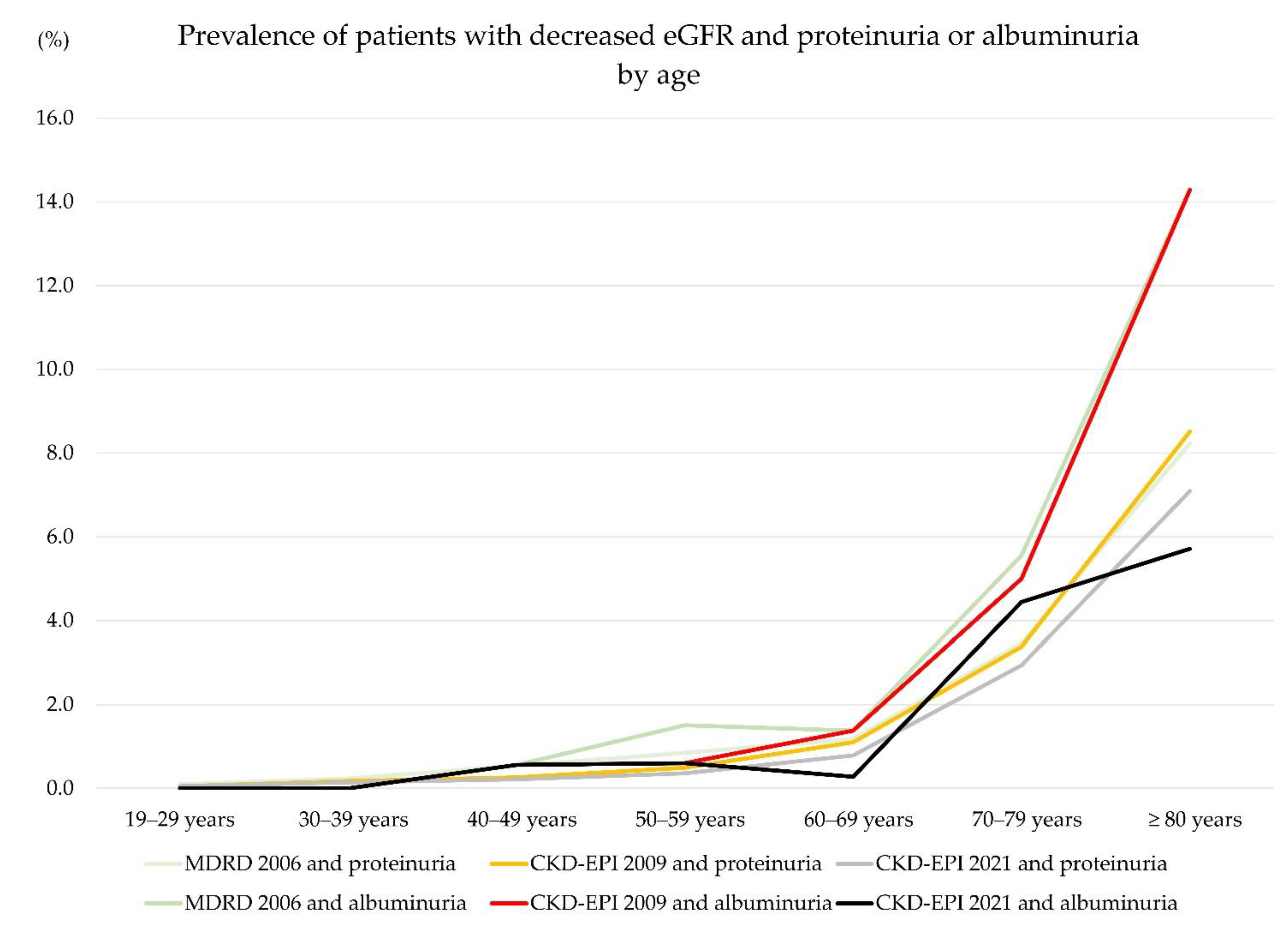
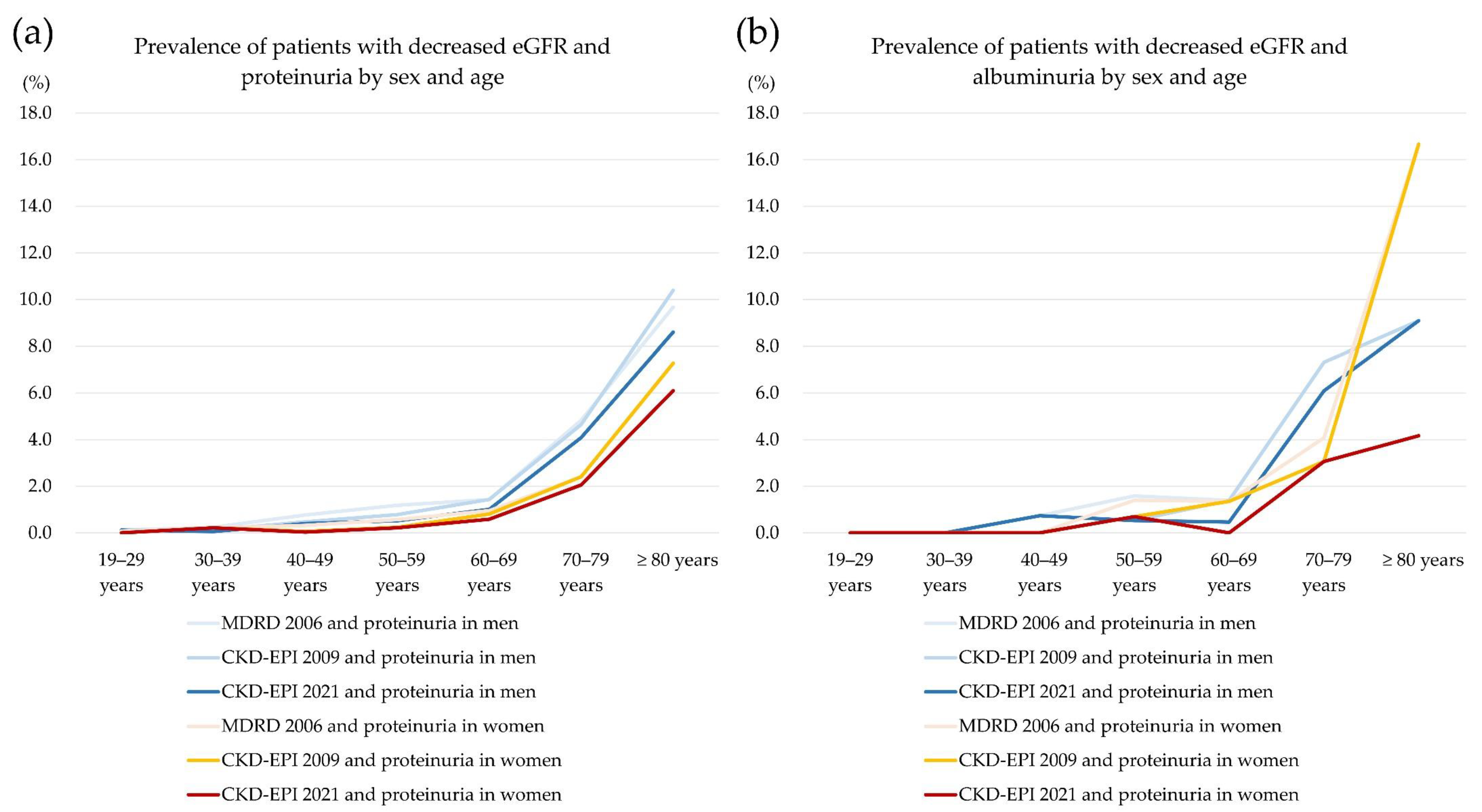
3.4. Decreased eGFR with Proteinuria or Albuminuria
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- KDIGO. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease; Kidney International Supplements; KDIGO: Brussels, Belgium, 2013; Volume 3, Available online: http://kdigo.org/home/guidelines/ckd-evaluation-management/ (accessed on 5 July 2022).
- Delanaye, P.; Jager, K.J.; Bökenkamp, A.; Christensson, A.; Dubourg, L.; Eriksen, B.O.; Gaillard, F.; Gambaro, G.; van der Giet, M.; Glassock, R.J.; et al. CKD: A Call for an Age-Adapted Definition. J. Am. Soc. Nephrol. 2019, 30, 1785–1805. [Google Scholar] [CrossRef]
- Korean Academy of Medical Sciences; Korea Disease Control and Prevention Agency. Evidence-Based Guideline for Chronic Kidney Disease in Primary Care; 2022. Available online: https://ksn.or.kr/bbs/?code=g_guideline (accessed on 5 July 2022).
- Inker, L.A.; Astor, B.C.; Fox, C.H.; Isakova, T.; Lash, J.P.; Peralta, C.A.; Kurella Tamura, M.; Feldman, H.I. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for the evaluation and management of CKD. Am. J. Kidney Dis. 2014, 63, 713–735. [Google Scholar] [CrossRef] [PubMed]
- Inker, L.A.; Eneanya, N.D.; Coresh, J.; Tighiouart, H.; Wang, D.; Sang, Y.; Crews, D.C.; Doria, A.; Estrella, M.M.; Froissart, M.; et al. New Creatinine- and Cystatin C-Based Equations to Estimate GFR without Race. N. Engl. J. Med. 2021, 385, 1737–1749. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Coresh, J.; Greene, T.; Stevens, L.A.; Zhang, Y.L.; Hendriksen, S.; Kusek, J.W.; Van Lente, F. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann. Intern. Med. 2006, 145, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Buchkremer, F.; Segerer, S. The 2009 and 2021 CKD-EPI Equations: A Graphical Analysis of the Effect of Refitting GFR Estimating Equations Without a Race Coefficient. Kidney Med. 2022, 4, 100448. [Google Scholar] [CrossRef] [PubMed]
- Oh, K.H.; Kang, M.; Kang, E.; Ryu, H.; Han, S.H.; Yoo, T.H.; Kim, S.W.; Chae, D.W.; Lee, K.B.; Park, S.K.; et al. The KNOW-CKD Study: What we have learned about chronic kidney diseases. Kidney Res. Clin. Pract. 2020, 39, 121–135. [Google Scholar] [CrossRef] [PubMed]
- Oh, K.; Kim, Y.; Kweon, S.; Kim, S.; Yun, S.; Park, S.; Lee, Y.K.; Kim, Y.; Park, O.; Jeong, E.K. Korea National Health and Nutrition Examination Survey, 20th anniversary: Accomplishments and future directions. Epidemiol. Health 2021, 43, e2021025. [Google Scholar] [CrossRef] [PubMed]
- Iversen, E.; Bengaard, A.K.; Andersen, A.; Kallemose, T.; Damgaard, M.; Hornum, M.; Feldt-Rasmussen, B.; Andersen, O.; Houlind, M.B. Performance of the Cockcroft-Gault, Modification of Diet in Renal Disease, and new Chronic Kidney Disease Epidemiology Collaboration equations without race in older acute medical patients. Kidney Int. 2022, 101, 1087–1088. [Google Scholar] [CrossRef] [PubMed]
- Hornum, M.; Houlind, M.B.; Iversen, E.; Porrini, E.; Luis-Lima, S.; Oturai, P.; Iversen, M.; Bredahl, P.; Carlsen, J.; Møller, C.H.; et al. Estimating Renal Function Following Lung Transplantation. J. Clin. Med. 2022, 11, 1496. [Google Scholar] [CrossRef] [PubMed]
- Delanaye, P.; Masson, I.; Maillard, N.; Pottel, H.; Mariat, C. The New 2021 CKD-EPI Equation Without Race in a European Cohort of Renal Transplanted Patients. Transplantation 2022. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Hundemer, G.L.; White, C.A.; Norman, P.A.; Knoll, G.A.; Tangri, N.; Sood, M.M.; Hiremath, S.; Burns, K.D.; McCudden, C.; Akbari, A. Performance of the 2021 Race-Free CKD-EPI Creatinine- and Cystatin C-Based Estimated GFR Equations Among Kidney Transplant Recipients. Am. J. Kidney Dis. 2022. [Google Scholar] [CrossRef] [PubMed]
- Silva, V.T.C.E.; Gil-Jr, L.A.; Inker, L.; Caires, R.; Costalonga, E.; Coura-Filho, G.; Esteves-Diz, M.D.P.; Castro, G.; Mathew, P.; Levey, A.; et al. Performance of the 2021 CKD-EPI equations without a race coefficient in a multi-racial population of adults with solid tumors: A prospective cross-sectional study. J. Clin. Oncol. 2022, 40 (Suppl. 16), 12064. [Google Scholar] [CrossRef]
- Wang, Y.; Levey, A.S.; Inker, L.A.; Jessani, S.; Bux, R.; Samad, Z.; Yaqub, S.; Karger, A.B.; Allen, J.C.; Jafar, T.H. Performance of Serum β2-Microglobulin- and β-Trace Protein-Based Panel Markers and 2021 Creatinine- and Cystatin-Based GFR Estimating Equations in Pakistan. Kidney Med. 2022, 4, 100444. [Google Scholar] [CrossRef]
- Oh, S.W.; Kim, S.; Na, K.Y.; Kim, K.W.; Chae, D.W.; Chin, H.J. Glomerular Filtration Rate and Proteinuria: Association with Mortality and Renal Progression in a Prospective Cohort of a Community-Based Elderly Population. PLoS ONE 2014, 9, e94120. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Data |
|---|---|
| Age, year (Mean, SD) | 50.1 (15.0) |
| Age group (n, %) | |
| 19–29 years | 46,882 (10.6) |
| 30–39 years | 73,217 (16.5) |
| 40–49 years | 105,633 (23.9) |
| 50–59 years | 92,879 (21.0) |
| 60–69 years | 76,935 (17.4) |
| 70–79 years | 37,313 (8.4) |
| ≥ 80 years | 9707 (2.2%) |
| SEX (n, %) | |
| Men | 205,236 (46.4) |
| Women | 237,330 (53.6) |
| Follow-up number (Mean, SD) | 1.1 (0.40) |
| Serum creatinine (mg/dL, Mean, SD) | 0.8 (0.33) |
| eGFR using MDRD 2006 (mL/min/1.73 m2, Mean, SD) | 92.2 (19.8) |
| eGFR using CKD-EPI 2009 (mL/min/1.73 m2, Mean, SD) | 97.1 (17.5) |
| eGFR using CKD-EPI 2021 (mL/min/1.73 m2, Mean, SD) | 100.8 (17.1) |
| Decreased eGFR (<60 mL/min/1.73 m2) | |
| Based on MDRD 2006 (n, %) | 15,208 (3.4%) |
| Based on CKD-EPI 2009 (n, %) | 12,482 (2.8%) |
| Based on CKD-EPI 2021 (n, %) | 9076 (2.1%) |
| Urine dipstick reagent strip protein test performed (n, %) | 26,608 (6.0%) |
| Urine albumin-creatinine ratio test performed (n,%) | 1151 (0.3%) |
| Both dipstick and albumin-creatinine ratio test performed (n, %) | 319 (0.1%) |
| Agreement of Three Categories of eGFR; ≤G2, G3a, and ≥G3b) | n (%) |
|---|---|
| MDRD 2006 eGFR = CKD-EPI 2009 eGFR | 439,101 (99.2%) |
| MDRD 2006 eGFR > CKD-EPI 2009 eGFR | 325 (0.1%) |
| MDRD 2006 eGFR < CKD-EPI 2009 eGFR | 3140 (0.7%) |
| MDRD 2006 eGFR = CKD-EPI 2021 eGFR | 435,600 (98.4%) |
| MDRD 2006 eGFR > CKD-EPI 2021 eGFR | 0 (0.0%) |
| MDRD 2006 eGFR < CKD-EPI 2021 eGFR | 6966 (1.6%) |
| CKD-EPI 2009 eGFR = CKD-EPI 2021 eGFR | 438,415 (99.1%) |
| CKD-EPI 2009 eGFR > CKD-EPI 2021 eGFR | 0 (0.0%) |
| CKD-EPI 2009 eGFR < CKD-EPI 2021 eGFR | 4151 (0.9%) |
| eGFR Grade | Urine Dipstick Protein Tests (n = 29,838) | Urine Albumin-Creatinine Ratio Tests (n = 1550) | ||||
|---|---|---|---|---|---|---|
| Negative or Trace | ≥1+ | A1 (<30 mg/g Cr) | A2 (30–300 mg/g Cr) | A3 (>300 mg/g Cr) | ||
| Total | 24,372 (91.6%) | 2236 (8.4%) | 917 (79.7%) | 277 (19.7%) | 7 (0.6%) | |
| MDRD 2006 eGFR | ≤G2 (≥60 mL/min/1.73 m2) | 23,636 (96.8%) | 1932 (86.4%) | 863 (94.1%) | 202 (89.0%) | 6 (85.7%) |
| G3a (45–59 mL/min/1.73 m2) | 640 (2.6%) | 188 (8.4%) | 43 (4.7%) | 20 (8.8%) | 0 (0.0%) | |
| ≥G3b (<45 mL/min/1.73 m2) | 129 (0.5%) | 116 (5.2%) | 11 (1.2%) | 5 (2.2%) | 1 (14.3%) | |
| CKD-EPI 2009 eGFR | ≤G2 (≥60 mL/min/1.73 m2) | 23,755 (97.5%) | 1980 (88.6%) | 874 (95.3%) | 206 (90.7%) | 6 (85.7%) |
| G3a (45–59 mL/min/1.73 m2) | 497 (2.0%) | 140 (6.3%) | 33 (3.6%) | 16 (7.0%) | 0 (0.0%) | |
| ≥G3b (<45 mL/min/1.73 m2) | 120 (0.5%) | 116 (5.2%) | 10 (1.1%) | 5 (2.2%) | 1 (14.3%) | |
| CKD-EPI 2021 eGFR | ≤G2 (≥60 mL/min/1.73 m2) | 23,939 (98.2%) | 2030 (90.8%) | 888 (96.8%) | 214 (94.3%) | 6 (85.7%) |
| G3a (45–59 mL/min/1.73 m2) | 355 (1.5%) | 111 (5.0%) | 23 (2.5%) | 10 (4.4%) | 0 (0.0%) | |
| ≥G3b (<45 mL/min/1.73 m2) | 78 (0.3%) | 95 (4.2%) | 6 (0.7%) | 3 (1.3%) | 1 (14.3%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, R.; Lee, S.G.; Lee, E.H. Alterations in Glomerular Filtration Rates Using Different Algorithms in the Korean Population Visiting Local Clinics and Hospitals. J. Clin. Med. 2022, 11, 5339. https://doi.org/10.3390/jcm11185339
Choi R, Lee SG, Lee EH. Alterations in Glomerular Filtration Rates Using Different Algorithms in the Korean Population Visiting Local Clinics and Hospitals. Journal of Clinical Medicine. 2022; 11(18):5339. https://doi.org/10.3390/jcm11185339
Chicago/Turabian StyleChoi, Rihwa, Sang Gon Lee, and Eun Hee Lee. 2022. "Alterations in Glomerular Filtration Rates Using Different Algorithms in the Korean Population Visiting Local Clinics and Hospitals" Journal of Clinical Medicine 11, no. 18: 5339. https://doi.org/10.3390/jcm11185339
APA StyleChoi, R., Lee, S. G., & Lee, E. H. (2022). Alterations in Glomerular Filtration Rates Using Different Algorithms in the Korean Population Visiting Local Clinics and Hospitals. Journal of Clinical Medicine, 11(18), 5339. https://doi.org/10.3390/jcm11185339