
Tweenager Computer Visual Syndrome Due to Tablets and Laptops during the Postlockdown COVID-19 Pandemic and the Influence on the Binocular and Accommodative System


 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Aspects
2.2. Patients
2.3. Material and Measures
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Galindo-Romero, C.; Ruiz-Porras, A.; García-Ayuso, D.; Di Pierdomenico, J.; Sobrado-Calvo, P.; Valiente-Soriano, F.J. Computer vision syndrome in the spanish population during the COVID-19 lockdown. Optom. Vis. Sci. 2021, 98, 1255–1262. [Google Scholar] [CrossRef] [PubMed]
- Mohan, A.; Sen, P.; Shah, C.; Jain, E.; Jain, S. Prevalence and risk factor assessment of digital eye strain among children using online e-learning during the COVID-19 pandemic: Digital eye strain among kids (DESK study-1). Indian J. Ophthalmol. 2021, 69, 140–144. [Google Scholar] [CrossRef] [PubMed]
- Sheppard, A.L.; Wolffsohn, J.S. Digital eye strain: Prevalence, measurement and amelioration. BMJ Open Ophthalmol. 2018, 3, e000146. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Zhu, L.; Zheng, S.; Ji, Y.; Xiang, Y.; Lv, B.; Xiong, L.; Li, Z.; Yi, S.; Huang, H.; et al. Survey on the progression of myopia in children and adolescents in chongqing during COVID-19 pandemic. Front. Public Health 2021, 9, 646770. [Google Scholar] [CrossRef]
- American Optometric Association. Computer Vision Syndrome. Available online: https://www.aoa.org/healthy-eyes/eye-and-vision-conditions/computer-vision-syndrome?sso=y (accessed on 30 August 2022).
- Al Tawil, L.; Aldokhayel, S.; Zeitouni, L.; Qadoumi, T.; Hussein, S.; Ahamed, S.S. Prevalence of self-reported computer vision syndrome symptoms and its associated factors among university students. Eur. J. Ophthalmol. 2020, 30, 189–195. [Google Scholar] [CrossRef]
- Gupta, R.; Chauhan, L.; Varshney, A. Impact of e-schooling on digital eye strain in coronavirus disease era: A survey of 654 students. J. Curr. Ophthalmol. 2021, 33, 158–164. [Google Scholar] [CrossRef]
- Straker, L.; Maslen, B.; Burgess-Limerick, R.; Johnson, P.; Dennerlein, J. Evidence-based guidelines for the wise use of computers by children: Physical development guidelines. Ergonomics 2010, 53, 458–477. [Google Scholar] [CrossRef]
- Hu, L.; Yan, Z.; Ye, T.; Lu, F.; Xu, P.; Chen, H. Differences in children and adolescents’ ability of reporting two CVS-related visual problems. Ergonomics 2013, 56, 1546–1557. [Google Scholar] [CrossRef]
- Wee, S.W.; Moon, N.J.; Lee, W.K.; Jeon, S. Ophthalmological factors influencing visual asthenopia as a result of viewing 3D displays. Br. J. Ophthalmol. 2012, 96, 1391–1394. [Google Scholar] [CrossRef]
- Cacho-Martínez, P.; García-Muñoz, Á.; Ruiz-Cantero, M.T. Is there any evidence for the validity of diagnostic criteria used for accommodative and nonstrabismic binocular dysfunctions? J. Optom. 2014, 7, 2–21. [Google Scholar] [CrossRef]
- Li, R.; Ying, B.; Qian, Y.; Chen, D.; Li, X.; Zhu, H.; Liu, H. Prevalence of self-reported symptoms of computer vision syndrome and associated risk factors among school students in China during the COVID-19 Pandemic. Ophthalmic Epidemiol. 2021, 29, 363–373. [Google Scholar] [CrossRef] [PubMed]
- Tarczy-Hornoch, K. Accommodative lag and refractive error in infants and toddlers. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2012, 16, 112–117. [Google Scholar] [CrossRef] [PubMed]
- González-Pérez, M.; Susi, R.; Antona, B.; Barrio, A.; González, E. The Computer-Vision Symptom Scale (CVSS17): Development and initial validation. Investig. Ophthalmol. Vis. Sci. 2014, 55, 4504–4511. [Google Scholar] [CrossRef] [PubMed]
- De-Hita-Cantalejo, C.; García-Pérez, Á.; Sánchez-González, J.M.; Capote-Puente, R.; Sánchez-González, M.C. Accommodative and binocular disorders in preteens with computer vision syndrome: A cross-sectional study. Ann. N. Y. Acad. Sci. 2021, 1492, 73–81. [Google Scholar] [CrossRef]
- Radner, W.; Benesch, T. Age-related course of visual acuity obtained with ETDRS 2000 charts in persons with healthy eyes. Graefe’s Arch. Clin. Exp. Ophthalmol. 2019, 257, 1295–1301. [Google Scholar] [CrossRef]
- León, A.; Estrada, J.M.; Rosenfield, M. Age and the amplitude of accommodation measured using dynamic retinoscopy. Ophthalmic Physiol. Opt. 2016, 36, 5–12. [Google Scholar] [CrossRef]
- Antona, B.; Sanchez, I.; Barrio, A.; Barra, F.; Gonzalez, E. Intra-examiner repeatability and agreement in accommodative response measurements. Ophthalmic Physiol. Opt. 2009, 29, 606–614. [Google Scholar] [CrossRef]
- Yothers, T.; Wick, B.; Morse, S.E. Clinical testing of accommodative facility: Part II. Development of an amplitude-scaled test. Optometry 2002, 73, 91–102. [Google Scholar]
- Scheiman, M.; Wick, B. Diagnosis and general treatment approach: Diagnostic testing. In Clinical Management of Binocular Vision: Heterophoric, Accommodative, and Eye Movement Disorders; Scheiman, M., Wick, B., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2008; pp. 3–49. ISBN 0781777844. [Google Scholar]
- Antona, B.; Gonzalez, E.; Barrio, A.; Barra, F.; Sanchez, I.; Cebrian, J.L. Strabometry precision: Intra-examiner repeatability and agreement in measuring the magnitude of the angle of latent binocular ocular deviations (heterophorias or latent strabismus). Binocul. Vis. Strabol. Q. 2011, 26, 91–104. [Google Scholar]
- Rosenfield, M. Computer vision syndrome: A review of ocular causes and potential treatments. Ophthalmic Physiol. Opt. 2011, 31, 502–515. [Google Scholar] [CrossRef]
- Blehm, C.; Vishnu, S.; Khattak, A.; Mitra, S.; Yee, R.W. Computer vision syndrome: A review. Surv. Ophthalmol. 2005, 50, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Loebis, R.; Subakti Zulkarnain, B.; Zahra, N. Correlation between the exposure time to mobile devices and the prevalence of evaporative dry eyes as one of the symptoms of computer vision syndrome among senior high school students in east Java, Indonesia. J. Basic Clin. Physiol. Pharmacol. 2021, 32, 541–545. [Google Scholar] [CrossRef]
- Sánchez-Valerio, M.D.R.; Mohamed-Noriega, K.; Zamora-Ginez, I.; Duarte, B.G.B.; Vallejo-Ruiz, V. Dry eye disease association with computer exposure time among subjects with computer vision syndrome. Clin. Ophthalmol. 2020, 14, 4311–4317. [Google Scholar] [CrossRef] [PubMed]
- Leng, T.S.; Saimon, R.; Rahman, M.; Safii, R.R.B.; Lianm, H.S.; John, N.; Thai, L.L.; Arsad, N. Factors predicting screen time related to physical and behavioural complaints in primary school children. Med. J. Malaysia 2020, 75, 649–654. [Google Scholar]
- Cankurtaran, F.; Menevşe, O.; Namli, A.; Kiziltoprak, H.S.; Altay, S.; Duran, M.; Demir, E.B.; Şahan, A.A.; Ekşi, C. The impact of digital game addiction on musculoskeletal system of secondary school children. Niger. J. Clin. Pract. 2022, 25, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Thorud, H.-M.S.; Mork, R.; Bjørset, C.O.; Gilson, S.J.; Hagen, L.A.; Langaas, T.; Pedersen, H.R.; Svarverud, E.; Vikesdal, G.H.; Baraas, R.C. Laboured reading and musculoskeletal pain in school children—the role of lifestyle behaviour and eye wear: A cross-sectional study. BMC Pediatr. 2022, 22, 416. [Google Scholar] [CrossRef]
- Ekemiri, K.; Ezinne, N.; Kamalodeen, K.; Pierre, K.; Lalla, B.; Amiebenomo, O.; van Staden, D.; Zeried, F.; Ekemiri, C.; Agho, K.E.; et al. Online e-learning during the COVID-19 lockdown in Trinidad and Tobago: Prevalence and associated factors with ocular complaints among schoolchildren aged 11–19 years. PeerJ 2022, 10, e13334. [Google Scholar] [CrossRef]
- Antona, B.; Barrio, A.R.; Gascó, A.; Pinar, A.; González-Pérez, M.; Puell, M.C. Symptoms associated with reading from a smartphone in conditions of light and dark. Appl. Ergon. 2018, 68, 12–17. [Google Scholar] [CrossRef]
- Mowatt, L.; Gordon, C.; Santosh, A.B.R.; Jones, T. Computer vision syndrome and ergonomic practices among undergraduate university students. Int. J. Clin. Pract. 2018, 72, e13035. [Google Scholar] [CrossRef]
- Mehra, D.; Galor, A. Digital screen use and dry eye: A review. Asia-Pacific J. Ophthalmol. 2020, 9, 491–497. [Google Scholar] [CrossRef]
- Golebiowski, B.; Long, J.; Harrison, K.; Lee, A.; Chidi-Egboka, N.; Asper, L. Smartphone use and effects on tear film, blinking and binocular vision. Curr. Eye Res. 2020, 45, 428–434. [Google Scholar] [CrossRef] [PubMed]
- Bade, A.; Boas, M.; Gallaway, M.; Mitchell, G.L.; Scheiman, M.; Kulp, M.T.; Cotter, S.A.; Rouse, M. Relationship between clinical signs and symptoms of convergence insufficiency. Optom. Vis. Sci. 2013, 90, 988–995. [Google Scholar] [CrossRef] [PubMed]
- Costa Lança, C.; Rowe, F.J. Variability of fusion vergence measurements in heterophoria. Strabismus 2016, 24, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Cacho-Martínez, P.; García-Muñoz, Á.; Ruiz-Cantero, M.T. Diagnostic validity of clinical signs associated with a large exophoria at near. J. Ophthalmol. 2013, 2013, 549435. [Google Scholar] [CrossRef] [PubMed]
- Lim, Z.; Seenyen, L.; Quah, B.L. Characteristics of divergence excess type intermittent exotropia in Asian children. J. AAPOS 2011, 15, 468–472. [Google Scholar] [CrossRef]
- Fu, T.; Wang, J.; Levin, M.; Su, Q.; Li, D.; Li, J. Fusional vergence detected by prism bar and synoptophore in chinese childhood intermittent exotropia. J. Ophthalmol. 2015, 2015, 987048. [Google Scholar] [CrossRef]
- Rowe, F.J. Fusional vergence measures and their significance in clinical assessment. Strabismus 2010, 18, 48–57. [Google Scholar] [CrossRef]
- Roper-Hall, G. The influence of the vergence system on strabismus diagnosis and management. Strabismus 2009, 17, 3–8. [Google Scholar] [CrossRef]
- Cacho-Martínez, P.; García-Muñoz, Á.; Ruiz-Cantero, M.T. Do we really know the prevalence of accomodative and nonstrabismic binocular dysfunctions? J. Optom. 2010, 3, 185–197. [Google Scholar] [CrossRef]
- Iqbal, M.; Said, O.; Ibrahim, O.; Soliman, A. Visual sequelae of computer vision syndrome: A cross-sectional case-control study. J. Ophthalmol. 2021, 2021, 6630286. [Google Scholar] [CrossRef]
- Lee, J.W.; Cho, H.G.; Moon, B.Y.; Kim, S.Y.; Yu, D.S. Effects of prolonged continuous computer gaming on physical and ocular symptoms and binocular vision functions in young healthy individuals. PeerJ 2019, 7, e7050. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Zhang, W.H.; Dai, S.Z.; Peng, H.Y.; Wang, L.Y. Binocular vision and abnormal head posture in children when watching television. Int. J. Ophthalmol. 2016, 9, 746–749. [Google Scholar] [CrossRef] [PubMed]
- Zetterberg, C.; Forsman, M.; Richter, H.O. Neck/shoulder discomfort due to visually demanding experimental near work is influenced by previous neck pain, task duration, astigmatism, internal eye discomfort and accommodation. PLoS ONE 2017, 12, e0182439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porcar, E.; Montalt, J.C.; Pons, Á.M.; España-Gregori, E. Symptomatic accommodative and binocular dysfunctions from the use of flat-panel displays. Int. J. Ophthalmol. 2018, 11, 501–505. [Google Scholar] [CrossRef]


{kind=link}
| Variables (Units) | Low-Demand Digital Devices (n = 59) | High-Demand Digital Devices (n = 49) | p Value |
|---|---|---|---|
| Male (%) Female (%) | 16 (27.1) 43 (72.9) | 24 (49.0) 25 (51.0) | 0.05 |
| Caucasian (%) Asian (%) | 57 (96.6) 2 (3.4) | 46 (93.8) 3 (6.2) | 0.85 |
| Age (years) | 10.80 ± 0.76 (10 to 12) | 11.02 ± 0.47 (10 to 12) | <0.01 |
| Item Questionnaire 1 (Score Points) | 2.44 ± 1.02 (1 to 3) | 3.41 ± 0.70 (2 to 4) | <0.01 |
| Item Questionnaire 2 (Score Points) | 2.59 ± 0.81 (2 to 4) | 3.02 ± 0.75 (2 to 4) | <0.01 |
| Item Questionnaire 3 (Score Points) | 2.32 ± 0.53 (2 to 4) | 2.69 ± 0.87 (1 to 4) | <0.01 |
| Item Questionnaire 4 (Score Points) | 2.42 ± 0.59 (1 to 3) | 3.16 ± 0.74 (1 to 4) | <0.01 |
| Item Questionnaire 5 (Score Points) | 1.83 ± 0.74 (1 to 3) | 3.43 ± 0.67 (2 to 4) | <0.01 |
| Item Questionnaire 6 (Score Points) | 2.37 ± 0.82 (1 to 4) | 3.16 ± 0.74 (2 to 4) | <0.01 |
| Item Questionnaire 7 (Score Points) | 3.02 ± 0.82 (1 to 4) | 3.35 ± 0.77 (2 to 4) | 0.03 |
| Item Questionnaire 8 (Score Points) | 2.36 ± 0.66 (1 to 3) | 3.61 ± 0.53 (2 to 4) | <0.01 |
| Item Questionnaire 9 (Score Points) | 3.32 ± 0.95 (1 to 4) | 3.59 ± 0.61 (1 to 4) | 0.26 |
| Item Questionnaire 10 (Score Points) | 3.39 ± 0.96 (1 to 4) | 3.78 ± 0.51 (2 to 4) | 0.02 |
| Item Questionnaire 11 (Score Points) | 3.69 ± 0.67 (1 to 4) | 3.73 ± 0.56 (1 to 4) | 0.97 |
| Item Questionnaire 12 (Score Points) | 3.34 ± 0.95 (1 to 4) | 3.71 ± 0.50 (2 to 4) | 0.05 |
| Item Questionnaire 13 (Score Points) | 2.25 ± 0.95 (1 to 4) | 3.33 ± 0.77 (1 to 4) | <0.01 |
| Item Questionnaire 14 (Score Points) | 2.17± 1.10 (1 to 4) | 3.53 ± 0.61 (2 to 4) | <0.01 |
| Item Questionnaire 15 (Score Points) | 1.59 ± 0.91 (0 to 4) | 3.80 ± 0.40 (3 to 4) | <0.01 |
| Item Questionnaire 16 (Score Points) | 1.63 ± 0.96 (1 to 4) | 3.65 ± 0.59 (2 to 4) | <0.01 |
| Item Questionnaire 17 (Score Points) | 2.53 ± 1.08 (1 to 4) | 3.10 ± 0.77 (1 to 4) | <0.01 |
| Item Questionnaire 18 (Score Points) | 2.53± 0.93 (1 to 4) | 3.06 ± 0.74 (2 to 4) | <0.01 |
| Item Questionnaire 19 (Score Points) | 1.93 ± 1.08 (1 to 4) | 1.45 ± 0.73 (1 to 4) | 0.01 |
| Mean Computer Vision Syndrome (Score Points) | 2.52 ± 0.11 (2.42 to 3.05) | 3.12 ± 0.28 (2.47 to 3.68) | <0.01 |
| (2.42 to 3.05) | |||
| Computer Visual Syndrome Survey is shown in Supplementary Document S1 | |||
| Variables (Units) | Low-Demand Digital Devices (n = 59) | High-Demand Digital Devices (n = 49) | p Value |
|---|---|---|---|
| Visual Acuity (Decimal Scale) | |||
| Right Eye | 1.11 ± 0.15 (0.80 to 1.25) | 0.64 ± 0.07 (0.60 to 0.90) | <0.01 |
| Left Eye | 1.11 ± 0.14 (0.80 to 1.25) | 0.65 ± 0.06 (0.60 to 0.90) | <0.01 |
| Both Eyes | 1.22 ± 0.07 (1.00 to 1.25) | 0.62 ± 0.05 (0.60 to 0.90) | <0.01 |
| Accommodation Amplitude | |||
| Right Eye (centimeters) | 9.63 ± 2.81 (6.00 to 25.00) | 9.05 ± 2.21 (5.00 to 14.00) | 0.46 |
| Right Eye (diopters) | 11.00 ± 2.44 (4.00 to 16.67) | 11.77 ± 3.15 (7.14 to 20.00) | 0.46 |
| Left Eye (centimeters) | 9.88 ± 2.87 (6.00 to 23.50) | 9.01 ± 2.16 (6.00 to 15.00) | 0.23 |
| Left Eye (diopters) | 10.76 ± 2.42 (4.26 to 16.67) | 11.76 ± 2.92 (6.67 to 16.67) | 0.23 |
| Both Eyes (centimeters) | 9.61 ± 2.58 (4.00 to 19.50) | 9.37 ± 3.03 (5.00 to 20.00) | 0.62 |
| Both Eyes (diopters) | 11.14 ± 3.36 (5.13 to 25.00) | 11.66 ± 3.54 (5.00 to 20.00) | 0.62 |
| Accommodative Posture and Facility | |||
| Both Eyes Posture (centimeters) | 44.56 ± 6.79 (31.00 to 80.00) | 48.79 ± 12.98 (30.00 to 100.00) | 0.20 |
| Both Eyes Posture (diopters) | 0.21 ± 0.31 (−0.73 to 1.25) | 0.35 ± 0.40 (−0.83 to 1.50) | 0.20 |
| Both Eyes Facility (cycles per minute) | 8.50 ± 3.33 (2.00 to 15.00) | 9.53 ± 5.19 (0.00 to 21.00) | 0.11 |
| Variables (Units) | Low-Demand Digital Devices (n = 59) | High-Demand Digital Devices (n = 49) | p Value |
|---|---|---|---|
| Phoria (negative exophoria and positive endophoria) Near Point of Convergence (NPC) | |||
| Near Phoria (Δ, prism diopter) | −1.53 ± 2.07 (−12.00 to 0.00) | −5.78 ± 8.62 (−25.00 to +12.00) | <0.01 |
| Distance Phoria (Δ, prism diopter) | −0.24 ± 2.10 (−16.00 to +2.00) | −1.94 ± 4.48 (−16.00 to +8.00) | <0.01 |
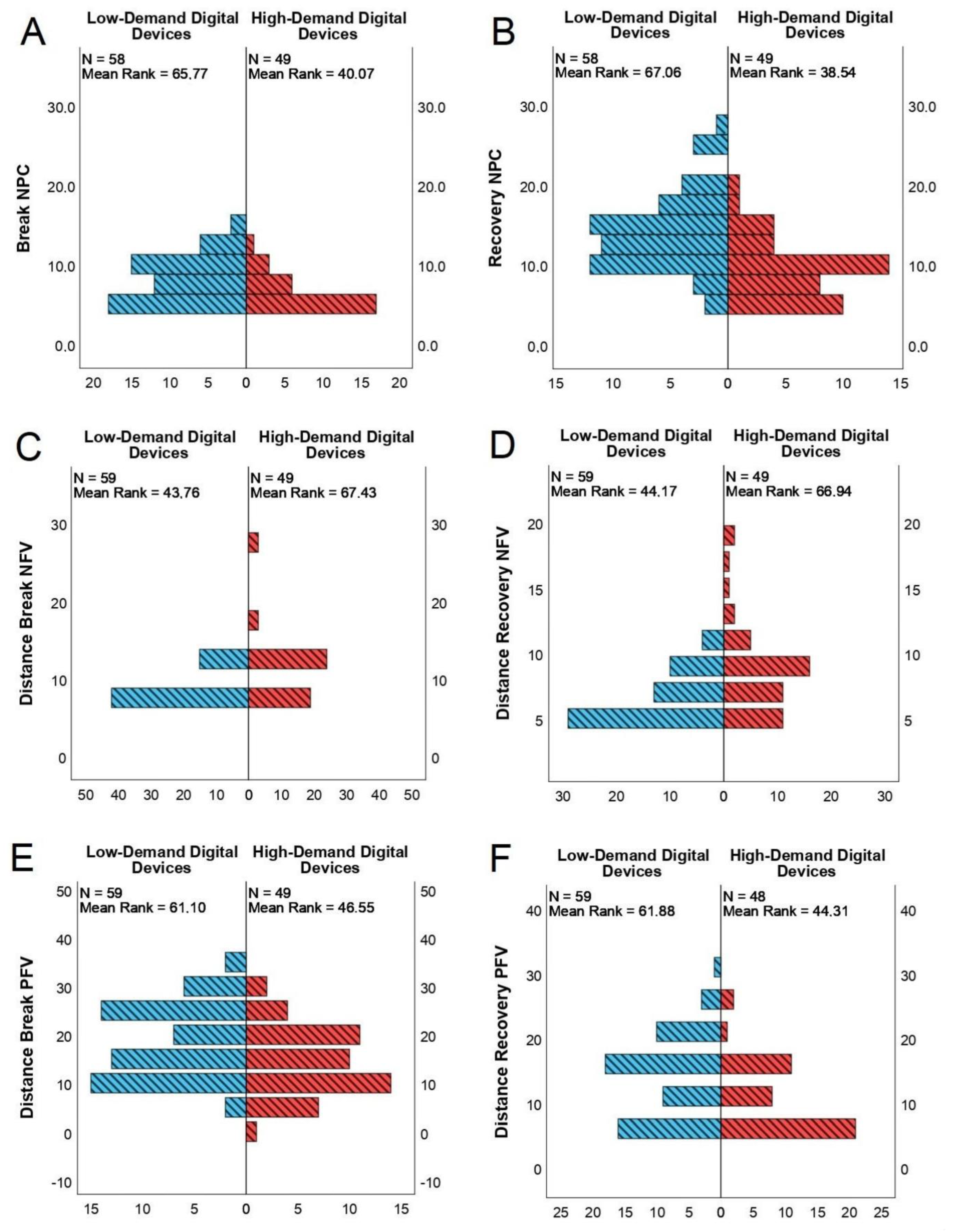
| Break NPC (centimeter) | 7.31 ± 3.57 (0.00 to 15.00) | 4.35 ± 3.05 (0.00 to 12.50) | <0.01 |
| Recovery NPC (centimeter) | 13.01 ± 5.91 (0.00 to 27.00) | 8.20 ± 4.52 (0.00 to 19.00) | <0.01 |
| Negative Fusional Vergences (NFVs) | |||
| Near Break NFV (Δ, prism diopter) | 11.02 ± 2.81 (4.00 to 16.00) | 11.76 ± 5.98 (2.00 to 35.00) | 0.90 |
| Near Recovery NFV (Δ, prism diopter) | 8.14 ± 2.62 (2.00 to 14.00) | 8.10 ± 4.84 (1.00 to 20.00) | 0.35 |
| Distance Break NFV (Δ, prism diopter) | 7.83 ± 2.47 (2.00 to 14.00) | 10.96 ± 4.73 (6.00 to 25.00) | <0.01 |
| Distance Recovery NFV (Δ, prism diopter) | 5.41 ± 2.10 (1.00 to 10.00) | 7.71 ± 3.44 (4.00 to 18.00) | <0.01 |
| Positive Fusional Vergences (PFVs) | |||
| Near Break PFV (Δ, prism diopter) | 14.29 ± 6.45 (2.00 to 30.00) | 14.96 ± 7.57 (0.00 to 30.00) | 0.65 |
| Near Recovery PFV (Δ, prism diopter) | 10.76 ± 5.63 (1.00 to 25.00) | 10.70 ± 5.01 (1.00 to 20.00) | 0.80 |
| Distance Break PFV (Δ, prism diopter) | 18.22 ± 8.09 (4.00 to 35.00) | 14.08 ± 6.95 (0.00 to 30.00) | <0.01 |
| Distance Recovery PFV (Δ, prism diopter) | 13.31 ± 6.37 (2.00 to 30.00) | 9.73 ± 5.66 (1.00 to 25.00) | <0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De-Hita-Cantalejo, C.; Sánchez-González, J.-M.; Silva-Viguera, C.; Sánchez-González, M.C. Tweenager Computer Visual Syndrome Due to Tablets and Laptops during the Postlockdown COVID-19 Pandemic and the Influence on the Binocular and Accommodative System. J. Clin. Med. 2022, 11, 5317. https://doi.org/10.3390/jcm11185317
De-Hita-Cantalejo C, Sánchez-González J-M, Silva-Viguera C, Sánchez-González MC. Tweenager Computer Visual Syndrome Due to Tablets and Laptops during the Postlockdown COVID-19 Pandemic and the Influence on the Binocular and Accommodative System. Journal of Clinical Medicine. 2022; 11(18):5317. https://doi.org/10.3390/jcm11185317
Chicago/Turabian StyleDe-Hita-Cantalejo, Concepción, José-María Sánchez-González, Carmen Silva-Viguera, and María Carmen Sánchez-González. 2022. "Tweenager Computer Visual Syndrome Due to Tablets and Laptops during the Postlockdown COVID-19 Pandemic and the Influence on the Binocular and Accommodative System" Journal of Clinical Medicine 11, no. 18: 5317. https://doi.org/10.3390/jcm11185317
APA StyleDe-Hita-Cantalejo, C., Sánchez-González, J.-M., Silva-Viguera, C., & Sánchez-González, M. C. (2022). Tweenager Computer Visual Syndrome Due to Tablets and Laptops during the Postlockdown COVID-19 Pandemic and the Influence on the Binocular and Accommodative System. Journal of Clinical Medicine, 11(18), 5317. https://doi.org/10.3390/jcm11185317