
Prognostic Significance of Organ-Specific Metastases in Patients with Metastatic Upper Tract Urothelial Carcinoma
 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Database and Patient Selection
2.2. Study Outcomes
2.3. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics
3.2. Metastatic Patterns
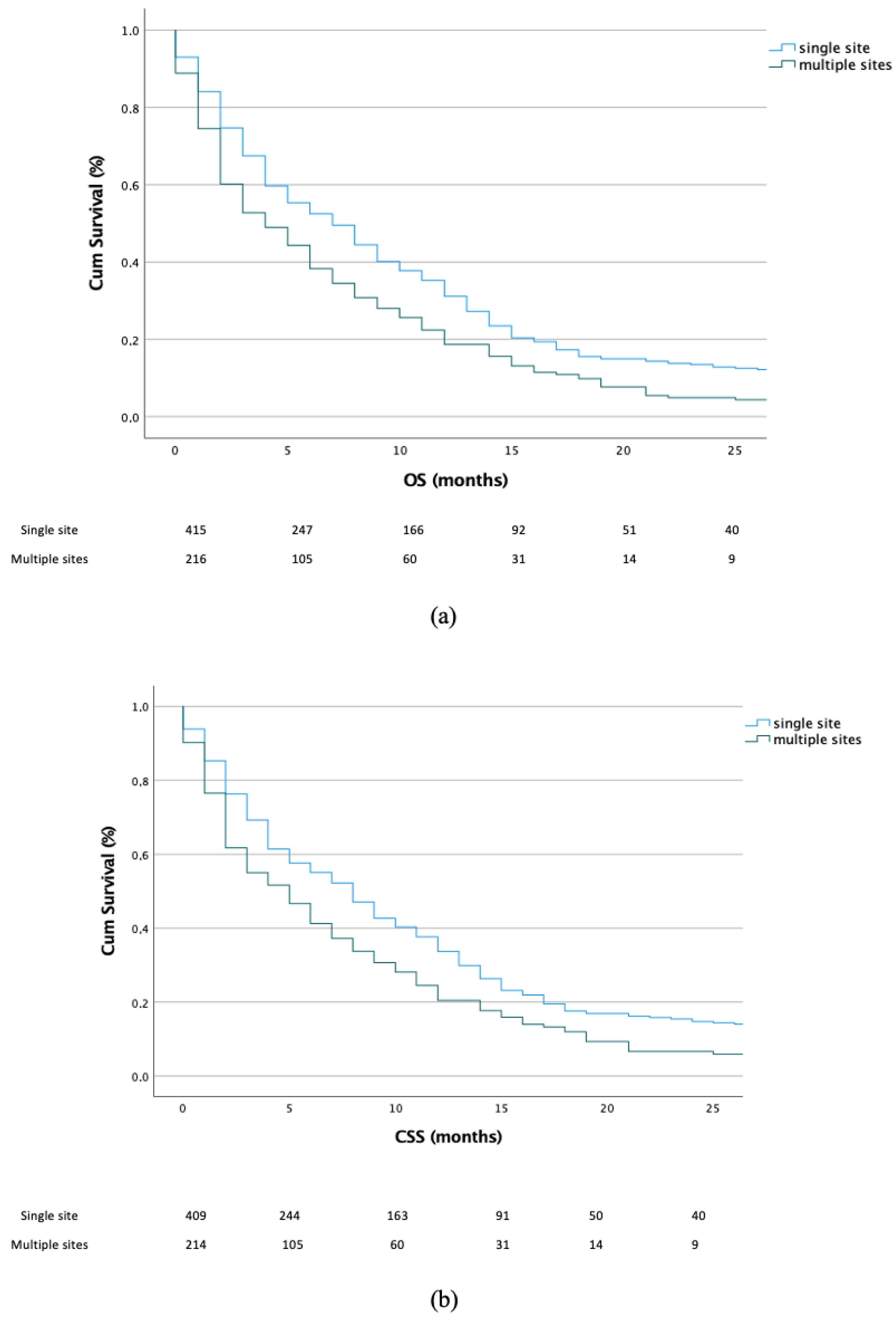
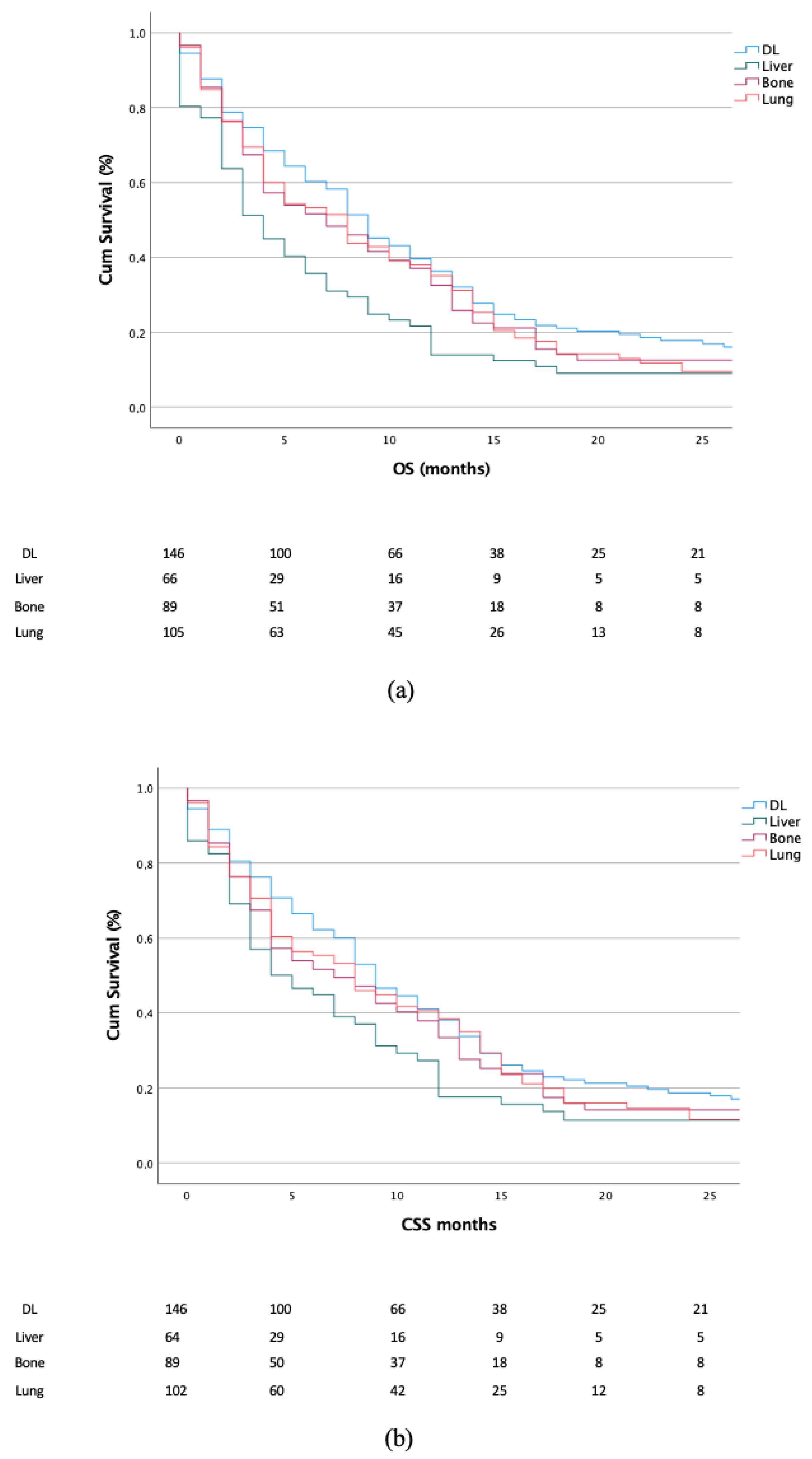
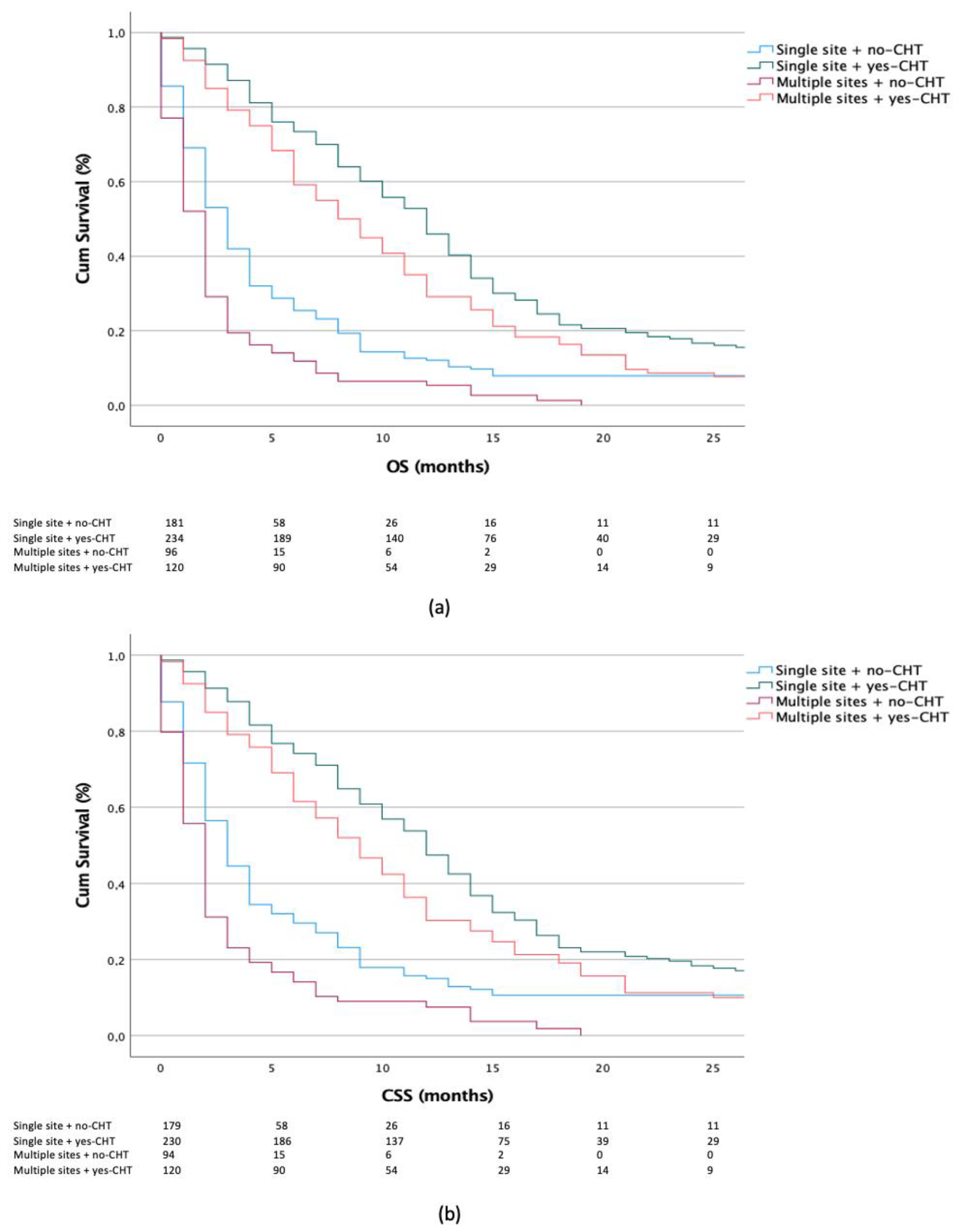
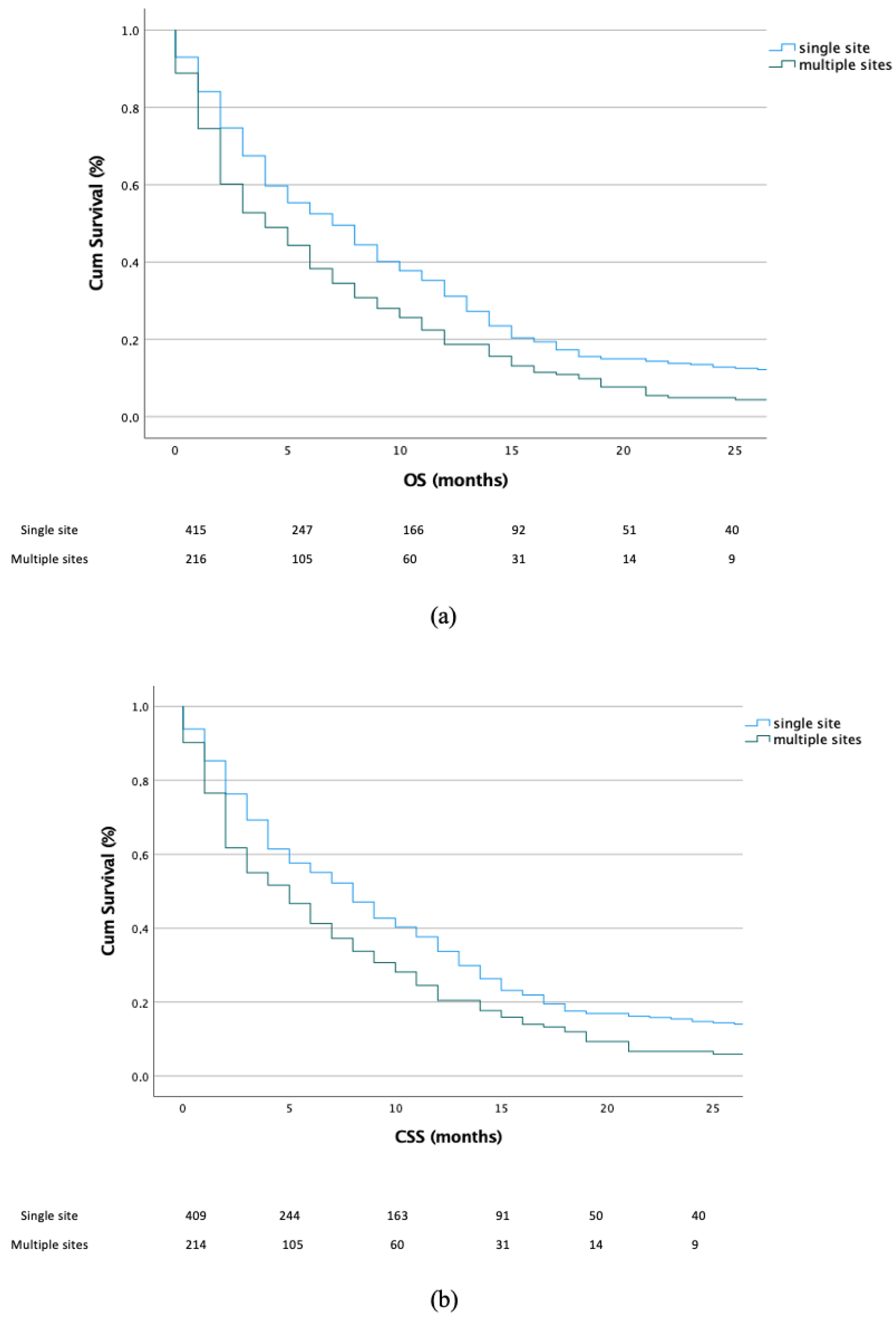
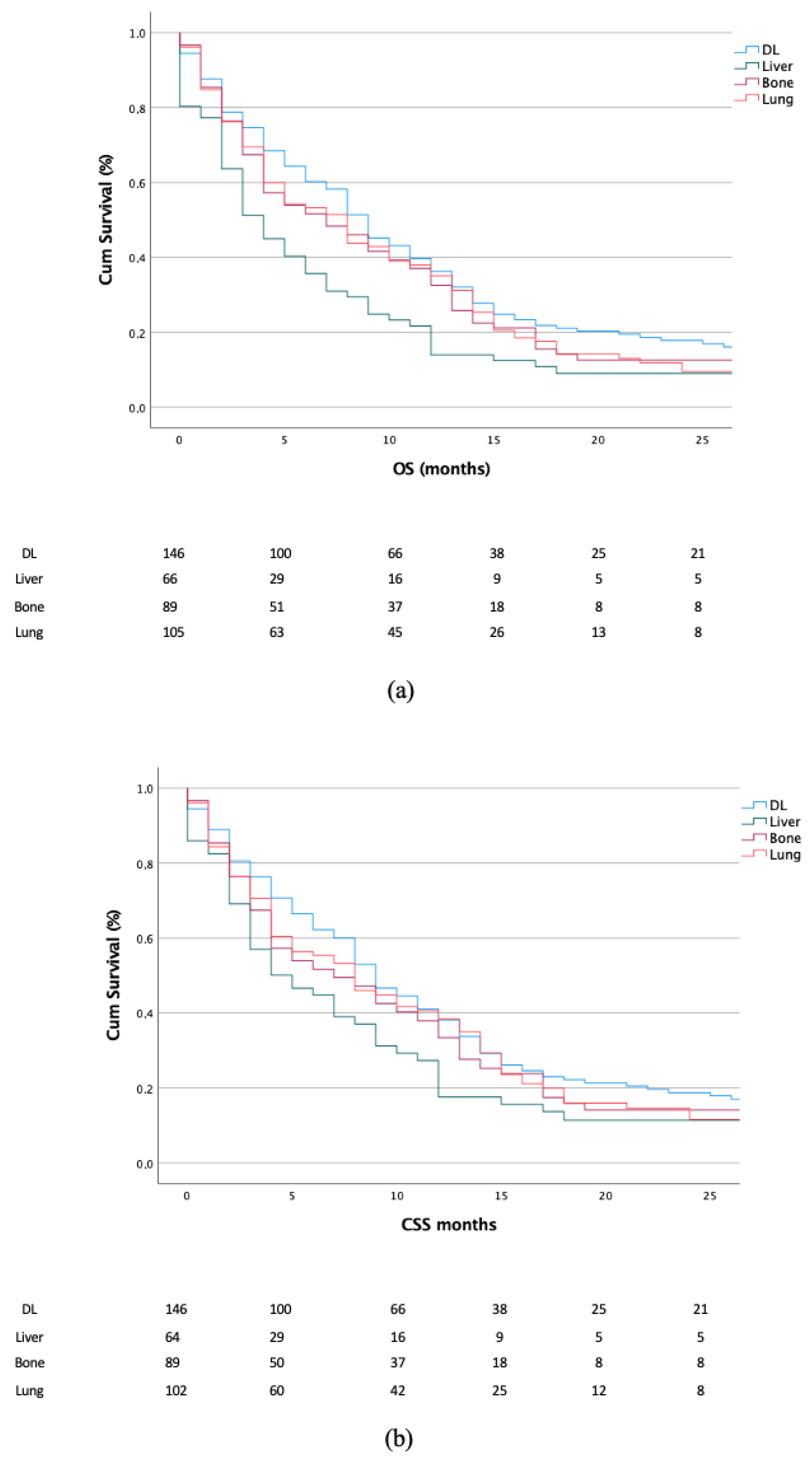
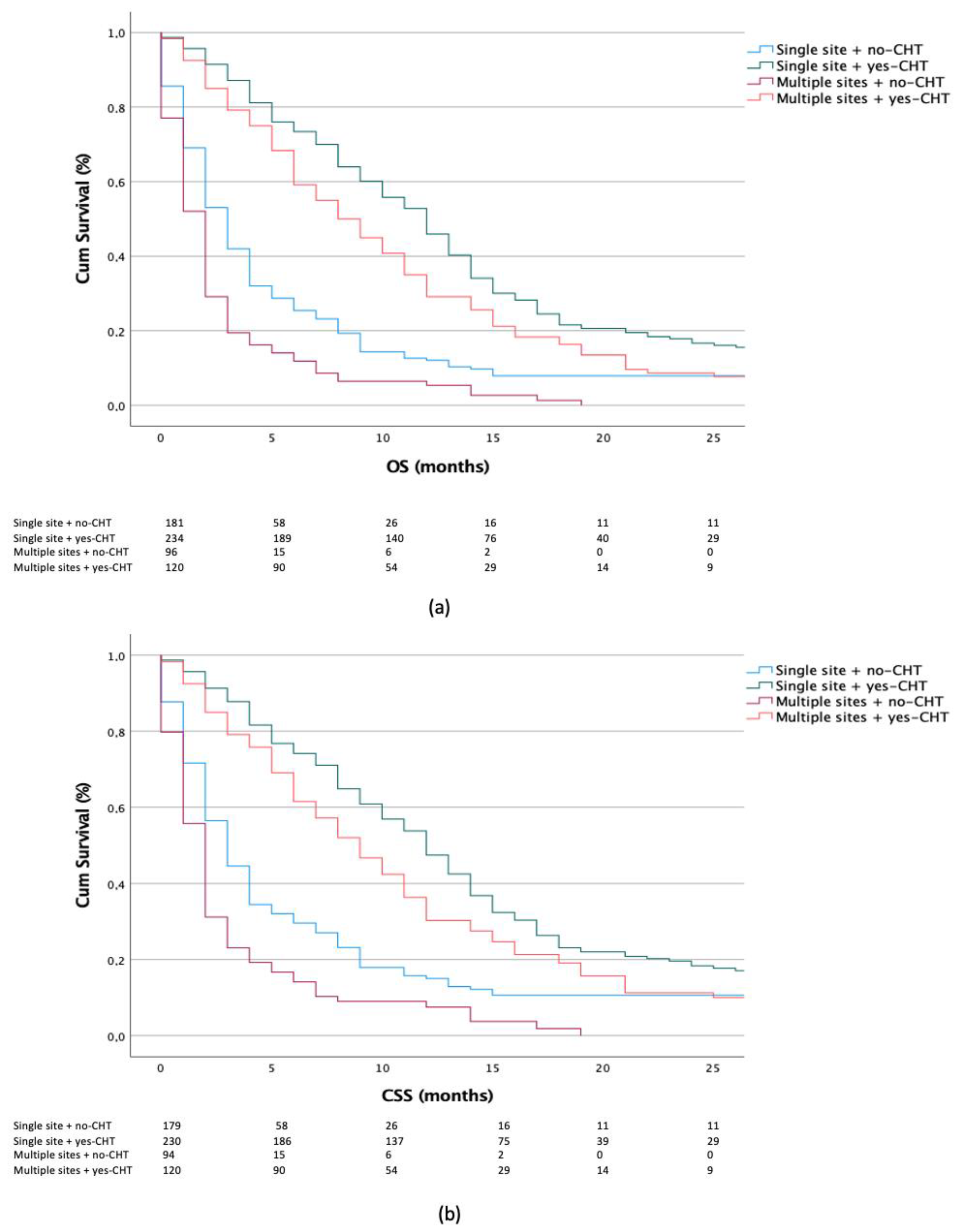
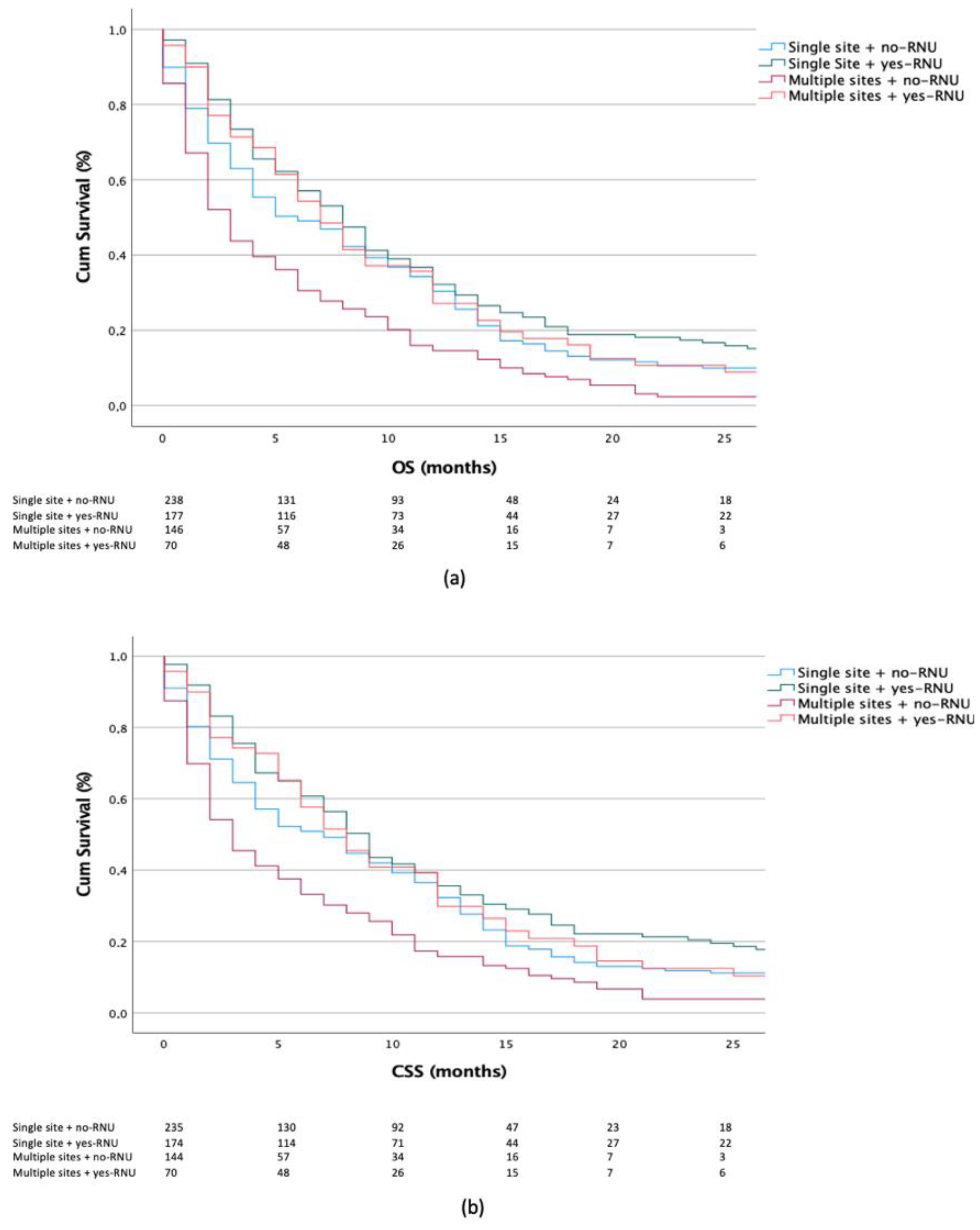
3.3. Impact of Metastatic Sites and Treatment Scheme on Survival Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer J Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Zhang, T.; Wu, J.; Wen, J.; Tao, D.; Wan, T.; Zhu, W. Prognosis and risk factors of patients with upper urinary tract urothelial carcinoma and postoperative recurrence of bladder cancer in central China. BMC Urol. 2019, 19, 24. [Google Scholar] [CrossRef] [PubMed]
- Raman, J.D.; Messer, J.; Sielatycki, J.A.; Hollenbeak, C.S. Incidence and survival of patients with carcinoma of the ureter and renal pelvis in the USA, 1973–2005. Br. J. Urol. Int. 2011, 107, 1059–1064. [Google Scholar] [CrossRef] [PubMed]
- Oweira, H.; Petrausch, U.; Helbling, D.; Schmidt, J.; Mannhart, M.; Mehrabi, A.; Schöb, O.; Giryes, A.; Decker, M.; Abdel-Rahman, O. Prognostic value of site-specific metastases in pancreatic adenocarcinoma: A Surveillance Epidemiology and End Results database analysis. World J. Gastroenterol. 2017, 23, 1872–1880. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.-G.; Li, H.; Tang, L.-Y.; Sun, J.-Y.; Zhang, W.-W.; Li, F.-Y.; Chen, Y.-X.; He, Z.-Y. The effect of distant metastases sites on survival in de novo stage-IV breast cancer: A SEER database analysis. Tumour Biol. J. Int. Soc. Oncodevelopmental. Biol. Med. 2017, 39, 1010428317705082. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Rahman, O. Clinical correlates and prognostic value of different metastatic sites in metastatic renal cell carcinoma. Future Oncol. 2017, 13, 1967–1980. [Google Scholar] [CrossRef] [PubMed]
- Shou, J.; Zhang, Q.; Zhang, D. The prognostic effect of metastasis patterns on overall survival in patients with distant metastatic bladder cancer: A SEER population-based analysis. World J. Urol. 2021, 39, 4151–4158. [Google Scholar] [CrossRef] [PubMed]
- Dong, F.; Fu, H.; Shi, X.; Shen, Y.; Xu, T.; Gao, F.; Wang, X.; Zhong, S.; Ding, Q.; Shen, Z.; et al. How do organ-specific metastases affect prognosis and surgical treatment for patients with metastatic upper tract urothelial carcinoma: First evidence from population based data. Clin. Exp. Metastasis 2017, 34, 467–477. [Google Scholar] [CrossRef] [PubMed]
- Bellmunt, J.; von der Maase, H.; Mead, G.M.; Skoneczna, I.; De Santis, M.; Daugaard, G.; Boehle, A.; Chevreau, C.; Paz-Ares, L.; Laufman, L.R.; et al. Randomized phase III study comparing paclitaxel/cisplatin/gemcitabine and gemcitabine/cisplatin in patients with locally advanced or metastatic urothelial cancer without prior systemic therapy: EORTC Intergroup Study 30987. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2012, 30, 1107–1113. [Google Scholar] [CrossRef] [PubMed]
- Rink, M.; Ehdaie, B.; Cha, E.K.; Green, D.A.; Karakiewicz, P.I.; Babjuk, M.; Margulis, V.; Raman, J.D.; Svatek, R.S.; Fajkovic, H.; et al. Stage-specific impact of tumor location on oncologic outcomes in patients with upper and lower tract urothelial carcinoma following radical surgery. Eur. Urol. 2012, 62, 677–684. [Google Scholar] [CrossRef] [PubMed]
- Margulis, V.; Shariat, S.F.; Matin, S.F.; Kamat, A.M.; Zigeuner, R.; Kikuchi, E.; Lotan, Y.; Weizer, A.; Raman, J.; Wood, C.G.; et al. Outcomes of radical nephroureterectomy: A series from the Upper Tract Urothelial Carcinoma Collaboration. Cancer 2009, 115, 1224–1233. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.-K.; Wu, Z.-G.; Xiao, Y.-B.; Wang, Q.-Q.; Yu, D.-D.; Cai, J.; Zhou, C.-F. Prognostic Value of Site-Specific Metastases and Therapeutic Roles of Surgery and Chemotherapy for Patients with Metastatic Renal Pelvis Cancer: A SEER Based Study. Technol. Cancer Res. Treat. 2021, 20, 15330338211004914. [Google Scholar] [CrossRef] [PubMed]
- Palma, D.A.; Olson, R.; Harrow, S.; Gaede, S.; Louie, A.V.; Haasbeek, C.; Mulroy, L.; Lock, M.; Rodrigues, G.B.; Yaremko, B.P.; et al. Stereotactic Ablative Radiotherapy for the Comprehensive Treatment of Oligometastatic Cancers: Long-Term Results of the SABR-COMET Phase II Randomized Trial. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2020, 38, 2830–2838. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Li, S.; Chi, Z.; Cui, C.; Si, L.; Yan, X.; Mao, L.; Lian, B.; Tang, B.; Wang, X.; et al. Clinicopathological characteristics, prognosis, and chemosensitivity in patients with metastatic upper tract urothelial carcinoma. Urol. Oncol. 2021, 39, e1–e75. [Google Scholar] [CrossRef] [PubMed]
- Nazzani, S.; Preisser, F.; Mazzone, E.; Marchioni, M.; Bandini, M.; Tian, Z.; Mistretta, F.A.; Shariat, S.F.; Soulières, D.; Montanari, E.; et al. Survival Effect of Chemotherapy in Metastatic Upper Urinary Tract Urothelial Carcinoma. Clin. Genitourin. Cancer 2019, 17, e97–e103. [Google Scholar] [CrossRef] [PubMed]
- Vassilakopoulou, M.; Rouge, T.D.L.M.; Colin, P.; Ouzzane, A.; Khayat, D.; Dimopoulos, M.; Papadimitriou, C.A.; Bamias, A.; Pignot, G.; Nouhaud, F.X.; et al. Outcomes after adjuvant chemotherapy in the treatment of high-risk urothelial carcinoma of the upper urinary tract (UUT-UC): Results from a large multicenter collaborative study. Cancer 2011, 117, 5500–5508. [Google Scholar] [CrossRef] [PubMed]
- Browne, B.M.; Stensland, K.D.; Moynihan, M.J.; Canes, D. An Analysis of Staging and Treatment Trends for Upper Tract Urothelial Carcinoma in the National Cancer Database. Clin. Genitourin. Cancer 2018, 16, e743–e750. [Google Scholar] [CrossRef] [PubMed]
- Seisen, T.; Jindal, T.; Karabon, P.; Sood, A.; Bellmunt, J.; Rouprêt, M.; Leow, J.J.; Vetterlein, M.; Sun, M.; Alanee, S.; et al. Efficacy of Systemic Chemotherapy Plus Radical Nephroureterectomy for Metastatic Upper Tract Urothelial Carcinoma. Eur. Urol. 2017, 71, 714–718. [Google Scholar] [CrossRef] [PubMed]
- Moschini, M.; Xylinas, E.; Zamboni, S.; Mattei, A.; Niegisch, G.; Yu, E.Y.; Bamias, A.; Agarwal, N.; Sridhar, S.S.; Sternberg, C.N.; et al. Efficacy of Surgery in the Primary Tumor Site for Metastatic Urothelial Cancer: Analysis of an International, Multicenter, Multidisciplinary Database. Eur. Urol. Oncol. 2020, 3, 94–101. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | No. | % |
|---|---|---|
| Age (years) | ||
| <65 | 176 | 27.8 |
| ≥65 | 457 | 72.2 |
| Gender | ||
| Female | 267 | 42 |
| Male | 366 | 57.8 |
| (T)NM | ||
| X | 151 | 23.8 |
| 0–2 | 160 | 25.3 |
| 3–4 | 322 | 50.9 |
| T(N)M | ||
| 0 | 202 | 31.9 |
| >1 | 431 | 68.1 |
| Grade | ||
| Low | 159 | 25.1 |
| High | 474 | 74.9 |
| Race | ||
| White | 529 | 83.6 |
| Black | 38 | 6.0 |
| Other | 66 | 10.4 |
| Radiation | ||
| No | 54 | 8.5 |
| Yes | 122 | 19.3 |
| Unknown | 457 | 72.2 |
| Radical nephroureterectomy | ||
| No | 386 | 61.0 |
| Yes | 247 | 39.0 |
| Chemotherapy | ||
| No | 195 | 30.8 |
| Yes | 354 | 55.9 |
| Unknown | 84 | 13.3 |
| Primary site | ||
| Renal pelvis | 427 | 67.5 |
| Ureter | 166 | 26.2 |
| Ureteric orifice | 40 | 6.3 |
| Number of metastatic sites | ||
| Single organ site | 417 | 65.9 |
| Multiple organ sites | 216 | 34.1 |
| Factors | Median OS (Months) HR (95% CI) | p-Value | Median CSS (Months) HR (95% CI) | p-Value |
|---|---|---|---|---|
| Age (years) | ||||
| <65 | Reference | |||
| ≥65 | 1.196 (0.903–1.584) | 0.213 | 1.167 (0.871–1.564) | 0.301 |
| Gender | ||||
| Female | Reference | |||
| Male | 0.900 (0.705–1.148) | 0.394 | 0.946 (0.732–1.221) | 0.946 |
| Tumor location | ||||
| Renal pelvis | Reference | |||
| Ureter | 0.782 (0.592–1.034) | 0.085 | 0.715 (0.530–0.965) | 0.028 |
| Ureter orifice | 1.044 (0.656–1.662) | 0.855 | 1.023 (0.630–1.662) | 0.926 |
| (T)NM | ||||
| 1–2 | Reference | |||
| 3–4 | 1.16 (0.869–1.553) | 0.312 | 0.946 (0.732–1.221) | 0.668 |
| T(N)M | ||||
| 0 | Reference | |||
| ≥1 | 0.962 (0.733–1.262) | 0.777 | 1.003 (0.753–1.337) | 0.983 |
| Number of organ metastasis | ||||
| Single organ site | Reference | |||
| Multiple organ sites | 1.425 (1.159–1.753) | <0.001 | 1.417 (1.141–1.760) | 0.002 |
| Radical nephroureterectomy | ||||
| No | Reference | |||
| Yes | 0.675 (0.514–0.886) | 0.005 | 0.671 (0.505–0.891) | 0.006 |
| Distant metastasis | ||||
| Lymph node | Reference | |||
| Liver | 1.732 (1.234–2.430) | 0.001 | 1.531 (1.062–2.207) | 0.022 |
| Bone | 1.188 (0.849–1.663) | 0.315 | 1.219 (0.863–1.721) | 0.261 |
| Lung | 1.179 (0.861–1.615) | 0.304 | 1.138 (0.817–1.585) | 0.444 |
| Chemotherapy | ||||
| No | Reference | |||
| Yes | 0.405 (0.313–0.523) | <0.001 | 0.435 (0.333–0.570) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tufano, A.; Cordua, N.; Nardone, V.; Ranavolo, R.; Flammia, R.S.; D’Antonio, F.; Borea, F.; Anceschi, U.; Leonardo, C.; Morrione, A.; et al. Prognostic Significance of Organ-Specific Metastases in Patients with Metastatic Upper Tract Urothelial Carcinoma. J. Clin. Med. 2022, 11, 5310. https://doi.org/10.3390/jcm11185310
Tufano A, Cordua N, Nardone V, Ranavolo R, Flammia RS, D’Antonio F, Borea F, Anceschi U, Leonardo C, Morrione A, et al. Prognostic Significance of Organ-Specific Metastases in Patients with Metastatic Upper Tract Urothelial Carcinoma. Journal of Clinical Medicine. 2022; 11(18):5310. https://doi.org/10.3390/jcm11185310
Chicago/Turabian StyleTufano, Antonio, Nadia Cordua, Valerio Nardone, Raffaele Ranavolo, Rocco Simone Flammia, Federica D’Antonio, Federica Borea, Umberto Anceschi, Costantino Leonardo, Andrea Morrione, and et al. 2022. "Prognostic Significance of Organ-Specific Metastases in Patients with Metastatic Upper Tract Urothelial Carcinoma" Journal of Clinical Medicine 11, no. 18: 5310. https://doi.org/10.3390/jcm11185310
APA StyleTufano, A., Cordua, N., Nardone, V., Ranavolo, R., Flammia, R. S., D’Antonio, F., Borea, F., Anceschi, U., Leonardo, C., Morrione, A., & Giordano, A. (2022). Prognostic Significance of Organ-Specific Metastases in Patients with Metastatic Upper Tract Urothelial Carcinoma. Journal of Clinical Medicine, 11(18), 5310. https://doi.org/10.3390/jcm11185310