
A Systematic Review on the Role of Repeat Transurethral Resection after Initial en Bloc Resection for Non-Muscle Invasive Bladder Cancer
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search and Study Selection
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction and Study Quality Assessment
2.4. Data Processing and Statistical Analysis
3. Results
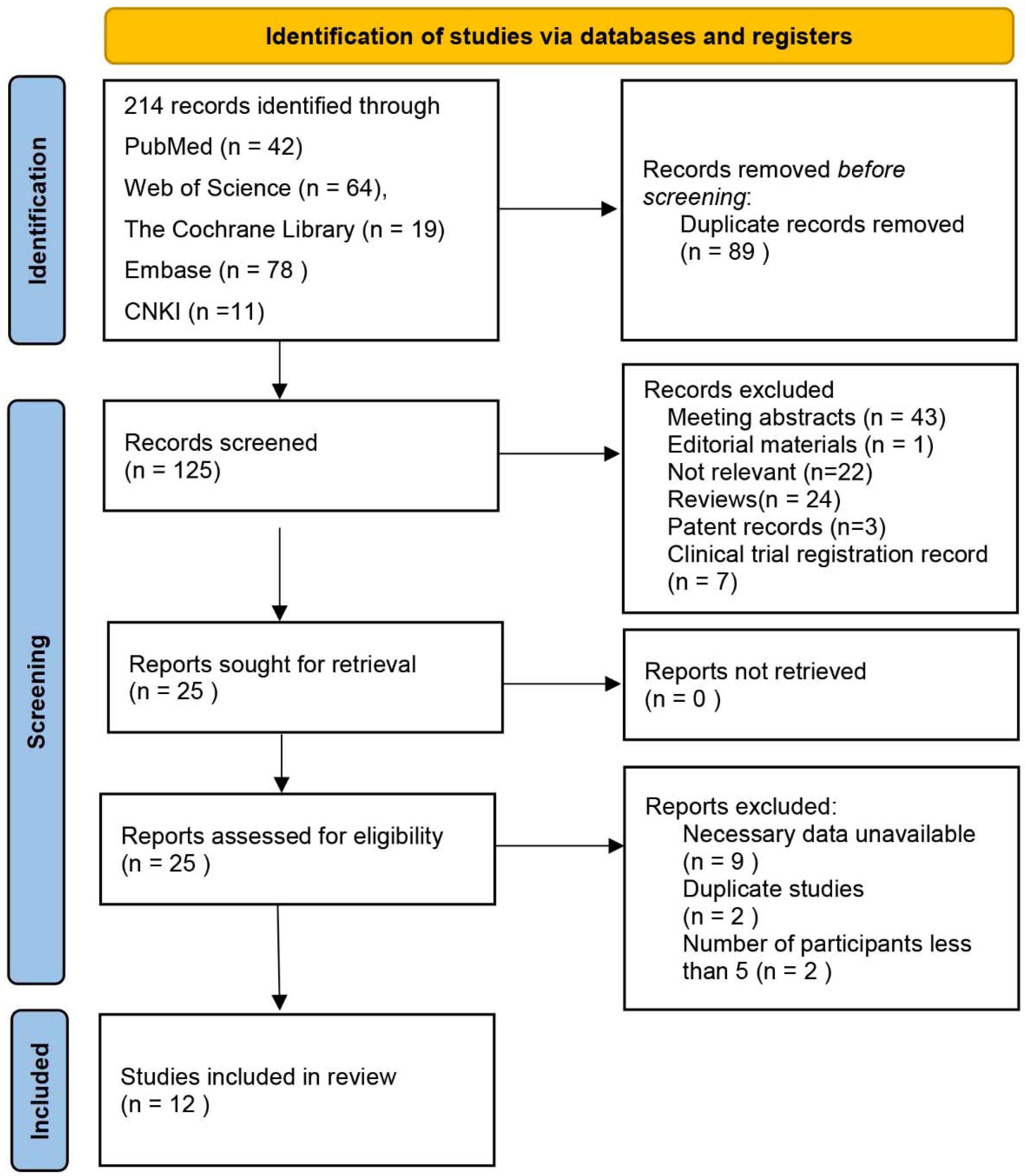
3.1. Literature Search and Study Selection
3.2. Systematic Reviews of Included Studies
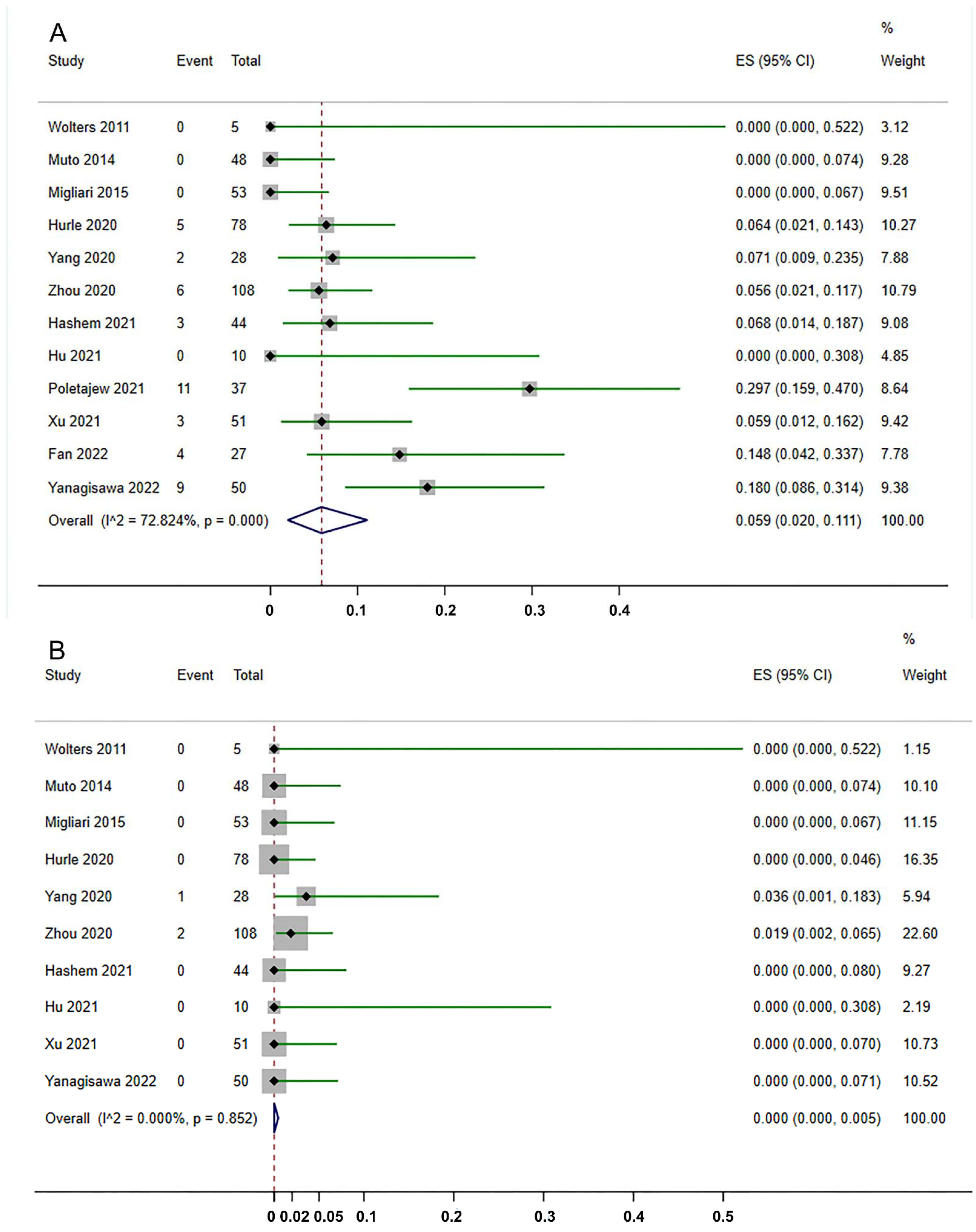
3.3. Residual Tumors and Upstage at reTURB after ERBT
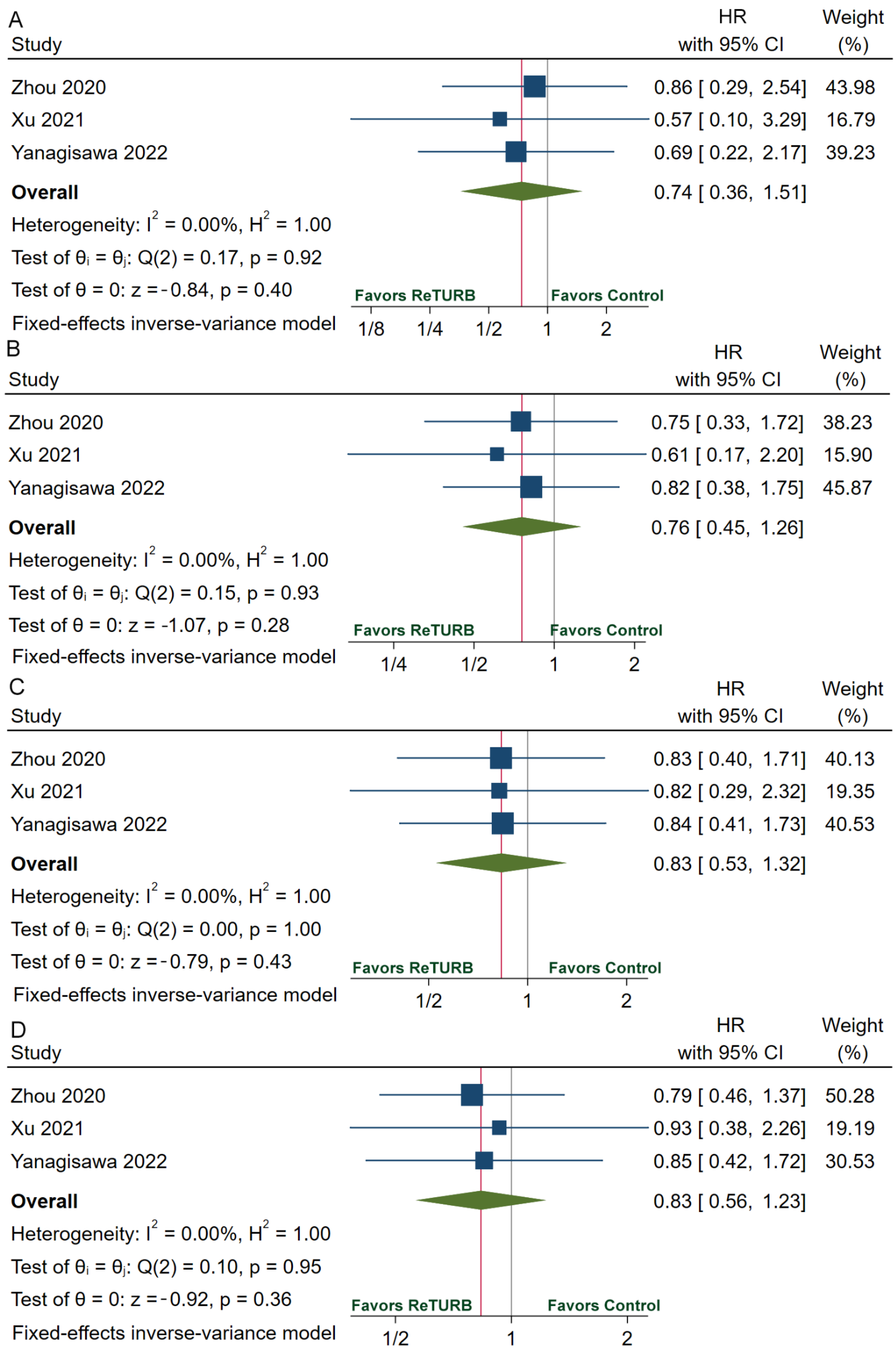
3.4. Recurrence and Progression
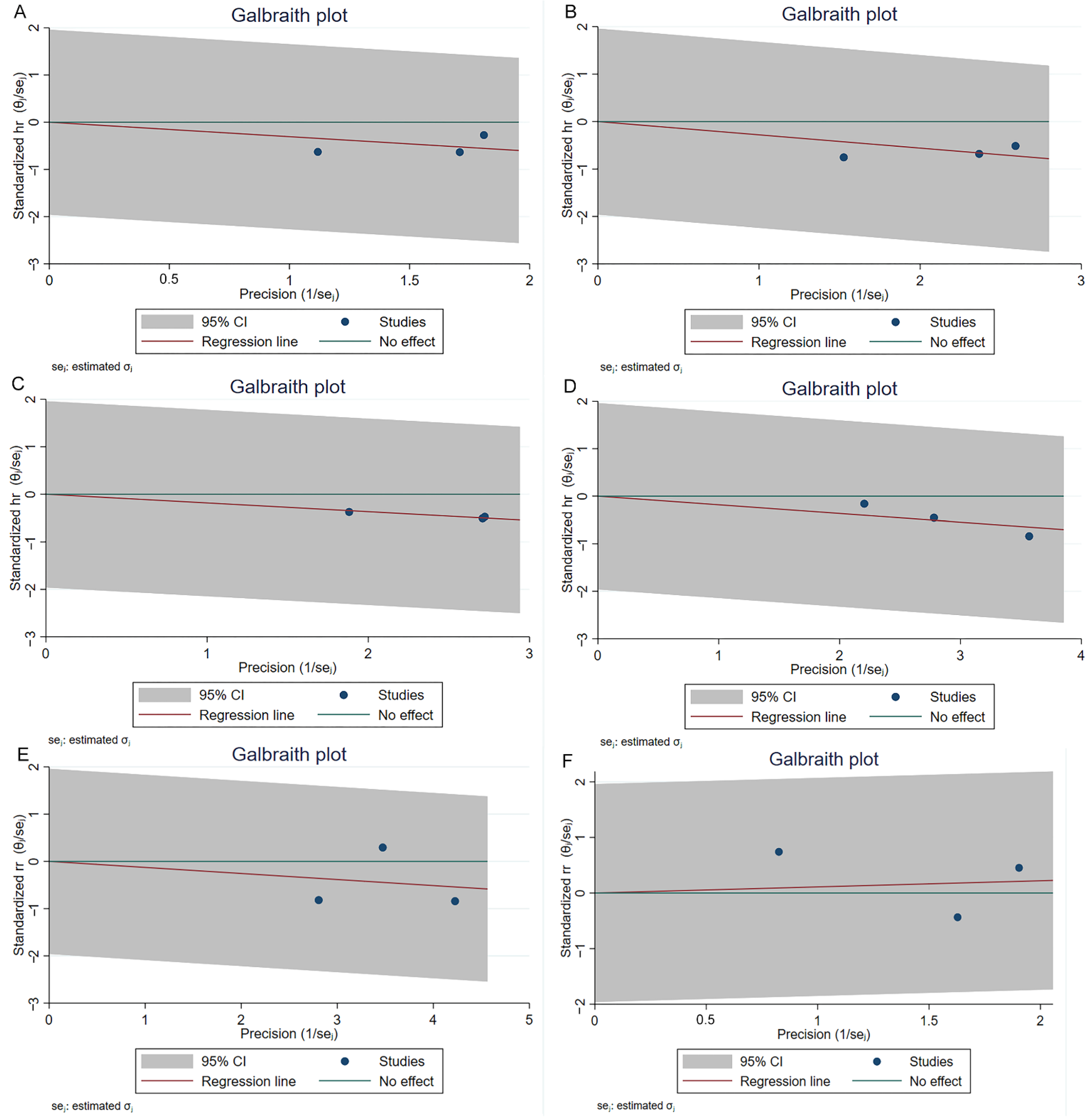
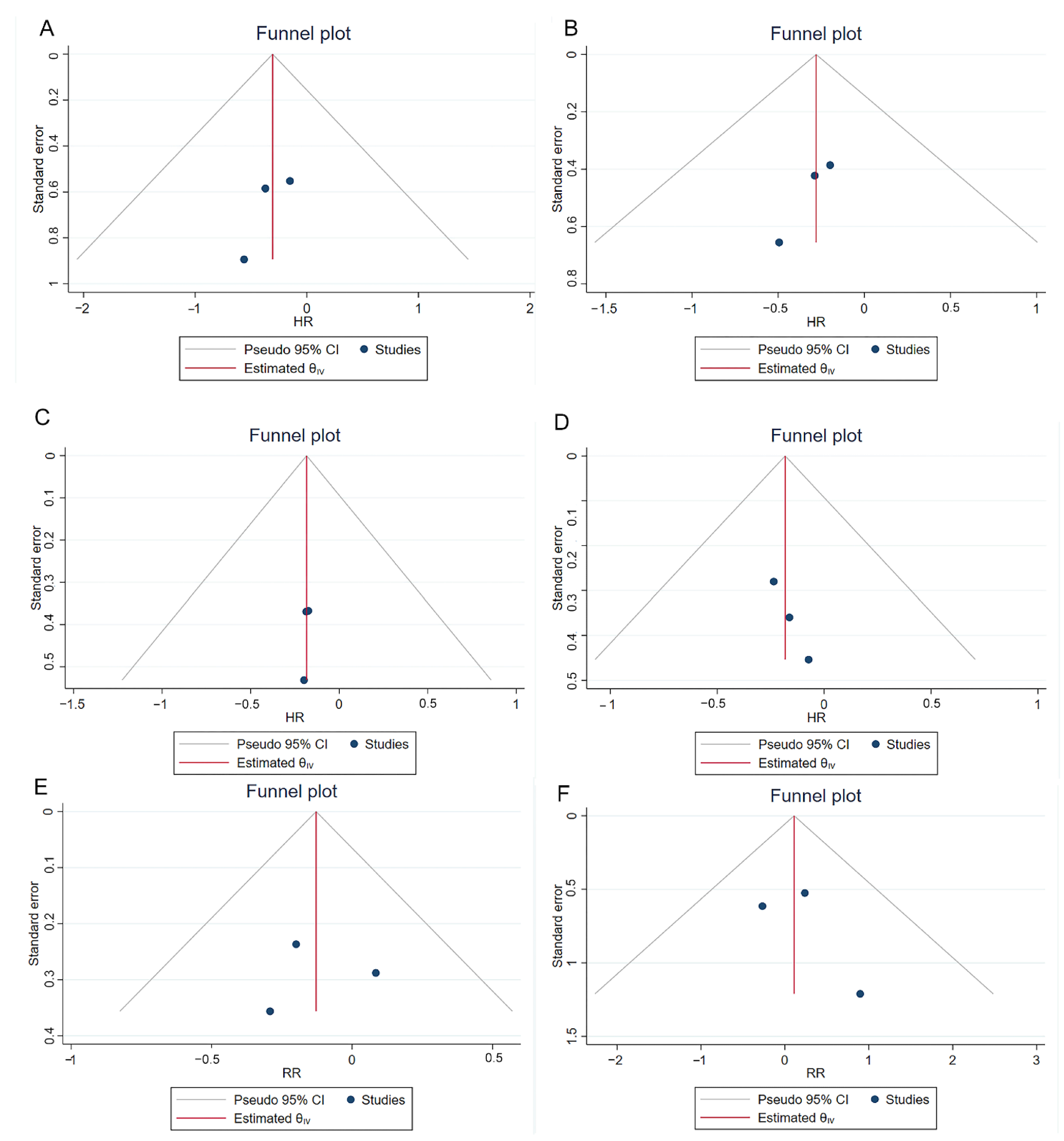
3.5. Risk of Bias Assessment, Heterogeneity, and Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Richters, A.; Aben, K.K.H.; Kiemeney, L. The global burden of urinary bladder cancer: An update. World J. Urol. 2020, 38, 1895–1904. [Google Scholar] [CrossRef] [PubMed]
- Safiri, S.; Kolahi, A.A.; Naghavi, M.; Global Burden of Disease Bladder Cancer Collaborators. Global, regional and national burden of bladder cancer and its attributable risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease study 2019. BMJ Glob. Health 2021, 6, e004128. [Google Scholar] [CrossRef] [PubMed]
- Babjuk, M.; Burger, M.; Capoun, O.; Cohen, D.; Comperat, E.M.; Dominguez Escrig, J.L.; Gontero, P.; Liedberg, F.; Masson-Lecomte, A.; Mostafid, A.H.; et al. European Association of Urology Guidelines on Non-muscle-invasive Bladder Cancer (Ta, T1, and Carcinoma in Situ). Eur. Urol. 2022, 81, 75–94. [Google Scholar] [CrossRef] [PubMed]
- Kramer, M.W.; Altieri, V.; Hurle, R.; Lusuardi, L.; Merseburger, A.S.; Rassweiler, J.; Struck, J.P.; Herrmann, T.R.W. Current Evidence of Transurethral En-bloc Resection of Nonmuscle Invasive Bladder Cancer. Eur. Urol. Focus 2017, 3, 567–576. [Google Scholar] [CrossRef]
- Ukai, R.; Kawashita, E.; Ikeda, H. A new technique for transurethral resection of superficial bladder tumor in 1 piece. J. Urol. 2000, 163, 878–879. [Google Scholar] [CrossRef]
- Yanagisawa, T.; Mori, K.; Motlagh, R.S.; Kawada, T.; Mostafaei, H.; Quhal, F.; Laukhtina, E.; Rajwa, P.; Aydh, A.; Konig, F.; et al. En Bloc Resection for Bladder Tumors: An Updated Systematic Review and Meta-Analysis of Its Differential Effect on Safety, Recurrence and Histopathology. J. Urol. 2022, 207, 754–768. [Google Scholar] [CrossRef]
- Symeonidis, E.N.; Lo, K.L.; Chui, K.L.; Vakalopoulos, I.; Sountoulides, P. En bloc resection of bladder tumors: Challenges and unmet needs in 2022. Future Oncol. 2022, 18, 2545–2558. [Google Scholar] [CrossRef]
- Teoh, J.Y.; MacLennan, S.; Chan, V.W.; Miki, J.; Lee, H.Y.; Chiong, E.; Lee, L.S.; Wei, Y.; Yuan, Y.; Yu, C.P.; et al. An International Collaborative Consensus Statement on En Bloc Resection of Bladder Tumour Incorporating Two Systematic Reviews, a Two-round Delphi Survey, and a Consensus Meeting. Eur. Urol. 2020, 78, 546–569. [Google Scholar] [CrossRef]
- Powles, T.; Bellmunt, J.; Comperat, E.; De Santis, M.; Huddart, R.; Loriot, Y.; Necchi, A.; Valderrama, B.P.; Ravaud, A.; Shariat, S.F.; et al. Bladder cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 2022, 33, 244–258. [Google Scholar] [CrossRef]
- Chang, S.S.; Boorjian, S.A.; Chou, R.; Clark, P.E.; Daneshmand, S.; Konety, B.R.; Pruthi, R.; Quale, D.Z.; Ritch, C.R.; Seigne, J.D.; et al. Diagnosis and Treatment of Non-Muscle Invasive Bladder Cancer: AUA/SUO Guideline. J. Urol. 2016, 196, 1021–1029. [Google Scholar] [CrossRef]
- Monteiro, L.L.; Witjes, J.A.; Agarwal, P.K.; Anderson, C.B.; Bivalacqua, T.J.; Bochner, B.H.; Boormans, J.L.; Chang, S.S.; Dominguez-Escrig, J.L.; McKiernan, J.M.; et al. ICUD-SIU International Consultation on Bladder Cancer 2017: Management of non-muscle invasive bladder cancer. World J. Urol. 2019, 37, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Bhindi, B.; Kool, R.; Kulkarni, G.S.; Siemens, D.R.; Aprikian, A.G.; Breau, R.H.; Brimo, F.; Fairey, A.; French, C.; Hanna, N.; et al. Canadian Urological Association guideline on the management of non-muscle-invasive bladder cancer—Abridged version. Can. Urol. Assoc. J. 2021, 15, 230–239. [Google Scholar] [PubMed]
- NCC Networks Inc. NCCN Clinical Practice Guidelines in Oncology: Bladder Cancer (Version 2 2022). Available online: https://www.nccn.org/professionals/physician_gls/pdf/bladder.pdf (accessed on 30 June 2022).
- Huang, J.; Xu, C.; Zhang, X. Chinese Urological Association guidelines on the diagnosis and treatment of bladder cancer. In Chinese Guidelines on Urological and Andrological Disease, 2019th ed.; Huang, J., Ed.; China Science Publishing & Media Ltd.: Beijing, China, 2020; pp. 27–84. [Google Scholar]
- NICE Guideline: Bladder Cancer: Diagnosis and Management. Available online: https://www.nice.org.uk/guidance/ng2 (accessed on 1 July 2022).
- Kim, L.H.C.; Patel, M.I. Transurethral resection of bladder tumour (TURBT). Transl. Androl. Urol. 2020, 9, 3056–3072. [Google Scholar] [CrossRef]
- Divrik, R.T.; Sahin, A.F.; Yildirim, U.; Altok, M.; Zorlu, F. Impact of routine second transurethral resection on the long-term outcome of patients with newly diagnosed pT1 urothelial carcinoma with respect to recurrence, progression rate, and disease-specific survival: A prospective randomised clinical trial. Eur. Urol. 2010, 58, 185–190. [Google Scholar] [CrossRef]
- Sfakianos, J.P.; Kim, P.H.; Hakimi, A.A.; Herr, H.W. The effect of restaging transurethral resection on recurrence and progression rates in patients with nonmuscle invasive bladder cancer treated with intravesical bacillus Calmette-Guerin. J. Urol. 2014, 191, 341–345. [Google Scholar]
- Rubio-Briones, J.; Algaba, F.; Gallardo, E.; Marcos-Rodriguez, J.A.; Climent, M.A.; on Behalf of the Sogug Multidisciplinary Working Group. Recent Advances in the Management of Patients with Non-Muscle-Invasive Bladder Cancer Using a Multidisciplinary Approach: Practical Recommendations from the Spanish Oncology Genitourinary (SOGUG) Working Group. Cancers 2021, 13, 4762. [Google Scholar] [CrossRef]
- Del Giudice, F.; Flammia, R.S.; Chung, B.I.; Moschini, M.; Pradere, B.; Mari, A.; Soria, F.; Albisinni, S.; Krajewski, W.; Szydelko, T.; et al. Compared Efficacy of Adjuvant Intravesical BCG-TICE vs. BCG-RIVM for High-Risk Non-Muscle Invasive Bladder Cancer (NMIBC): A Propensity Score Matched Analysis. Cancers 2022, 14, 887. [Google Scholar] [CrossRef]
- Del Giudice, F.; Busetto, G.M.; Gross, M.S.; Maggi, M.; Sciarra, A.; Salciccia, S.; Ferro, M.; Sperduti, I.; Flammia, S.; Canale, V.; et al. Efficacy of three BCG strains (Connaught, TICE and RIVM) with or without secondary resection (re-TUR) for intermediate/high-risk non-muscle-invasive bladder cancers: Results from a retrospective single-institution cohort analysis. J. Cancer Res. Clin. Oncol. 2021, 147, 3073–3080. [Google Scholar] [CrossRef]
- Lee, L.J.; Kwon, C.S.; Forsythe, A.; Mamolo, C.M.; Masters, E.T.; Jacobs, I.A. Humanistic and Economic Burden of Non-Muscle Invasive Bladder Cancer: Results of Two Systematic Literature Reviews. Clin. Outcomes Res. 2020, 12, 693–709. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 1 June 2022).
- Knoll, T.; Omar, M.I.; Maclennan, S.; Hernandez, V.; Canfield, S.; Yuan, Y.; Bruins, M.; Marconi, L.; Van Poppel, H.; N’Dow, J.; et al. Key Steps in Conducting Systematic Reviews for Underpinning Clinical Practice Guidelines: Methodology of the European Association of Urology. Eur. Urol. 2018, 73, 290–300. [Google Scholar] [CrossRef] [Green Version]
- Tierney, J.F.; Stewart, L.A.; Ghersi, D.; Burdett, S.; Sydes, M.R. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials 2007, 8, 16. [Google Scholar] [CrossRef]
- Wolters, M.; Kramer, M.W.; Becker, J.U.; Christgen, M.; Nagele, U.; Imkamp, F.; Burchardt, M.; Merseburger, A.S.; Kuczyk, M.A.; Bach, T.; et al. Tm:YAG laser en bloc mucosectomy for accurate staging of primary bladder cancer: Early experience. World J. Urol. 2011, 29, 429–432. [Google Scholar] [CrossRef]
- Muto, G.; Collura, D.; Giacobbe, A.; D’Urso, L.; Muto, G.L.; Demarchi, A.; Coverlizza, S.; Castelli, E. Thulium:yttrium-aluminum-garnet laser for en bloc resection of bladder cancer: Clinical and histopathologic advantages. Urology 2014, 83, 851–855. [Google Scholar] [CrossRef]
- Migliari, R.; Buffardi, A.; Ghabin, H. Thulium laser endoscopic en bloc enucleation of nonmuscle-invasive bladder cancer. J. Endourol. 2015, 29, 1258–1262. [Google Scholar] [CrossRef]
- Hurle, R.; Casale, P.; Lazzeri, M.; Paciotti, M.; Saita, A.; Colombo, P.; Morenghi, E.; Oswald, D.; Colleselli, D.; Mitterberger, M.; et al. En bloc re-resection of high-risk NMIBC after en bloc resection: Results of a multicenter observational study. World J. Urol. 2020, 38, 703–708. [Google Scholar] [CrossRef]
- Yang, Y.; Liu, C.; Yang, X.; Wang, D. Transurethral en bloc resection with monopolar current for non-muscle invasive bladder cancer based on TNM system. Transl. Cancer Res. 2020, 9, 2210–2219. [Google Scholar] [CrossRef]
- Zhou, W.; Wang, W.; Wu, W.; Yan, T.; Du, G.; Liu, H. Can a second resection be avoided after initial thulium laser endoscopic en bloc resection for non-muscle invasive bladder cancer? A retrospective single-center study of 251 patients. BMC Urol. 2020, 20, 30. [Google Scholar] [CrossRef]
- Hashem, A.; Mosbah, A.; El-Tabey, N.A.; Laymon, M.; Ibrahiem, E.-H.; Abd Elhamid, M.; Elshal, A.M. Holmium Laser En-bloc Resection Versus Conventional Transurethral Resection of Bladder Tumors for Treatment of Non-muscle-invasive Bladder Cancer: A Randomized Clinical Trial. Eur. Urol. Focus 2021, 7, 1035–1043. [Google Scholar] [CrossRef]
- Hu, H.; Li, B.; Liu, Z.; Meng, X.; Li, C.; Li, F.; Hu, J.; Chen, Y.; Li, Z.; Wang, S. The individual surgical protocol of transurethral en bloc resection of bladder tumor based on VI-RADS and preliminary experience. Chin. J. Urol. 2021, 42, 180–184. [Google Scholar]
- Poletajew, S.; Krajewski, W.; Stelmach, P.; Adamowicz, J.; Nowak, L.; Moschini, M.; Zapala, P.; Drewa, T.; Paradysz, A.; Radziszewski, P.; et al. En-bloc resection of urinary bladder tumour—A prospective controlled multicentre observational study. Videosurg. Other Miniinvasive Tech. 2021, 16, 145–150. [Google Scholar] [CrossRef]
- Xu, S.; Cao, P.; Wang, K.; Wu, T.; Hu, X.; Chen, H.; Xu, L.; Gu, J.; Wu, S.; Zhu, L.; et al. Clinical Outcomes of Reresection in Patients with High-Risk Nonmuscle-Invasive Bladder Cancer Treated with en Bloc Transurethral Resection: A Retrospective Study with a 1-Year Follow-Up. J. Endourol. 2021, 35, 1801–1807. [Google Scholar] [CrossRef]
- Fan, J.; Zhang, X.; Fan, J.; Li, L.; He, D.; Wu, K. Risk Stratification for the Rate and Location of Residual Bladder Tumor for the Decision of Re-Transurethral Resection of Bladder Tumor. Front. Oncol. 2022, 12, 788568. [Google Scholar] [CrossRef]
- Yanagisawa, T.; Sato, S.; Hayashida, Y.; Okada, Y.; Iwatani, K.; Matsukawa, A.; Kimura, T.; Takahashi, H.; Egawa, S.; Shariat, S.F.; et al. Do we need repeat transurethral resection after en bloc resection for pathological T1 bladder cancer? BJU Int. 2022. [Google Scholar] [CrossRef]
- Cumberbatch, M.G.K.; Foerster, B.; Catto, J.W.F.; Kamat, A.M.; Kassouf, W.; Jubber, I.; Shariat, S.F.; Sylvester, R.J.; Gontero, P. Repeat Transurethral Resection in Non-muscle-invasive Bladder Cancer: A Systematic Review. Eur. Urol. 2018, 73, 925–933. [Google Scholar] [CrossRef]
- Soria, F.; Marra, G.; D’Andrea, D.; Gontero, P.; Shariat, S.F. The rational and benefits of the second look transurethral resection of the bladder for T1 high grade bladder cancer. Transl. Androl. Urol. 2019, 8, 46–53. [Google Scholar] [CrossRef]
- Soria, F.; Giordano, A.; Gontero, P. Transurethral resection of bladder tumor and the need for re-transurethral resection of bladder tumor: Time to change our practice? Curr. Opin. Urol. 2020, 30, 370–376. [Google Scholar] [CrossRef]
- Creta, M.; Celentano, G.; Califano, G.; La Rocca, R.; Longo, N. En-bloc Laser Resection of Bladder Tumors: Where Are We Now? J. Clin. Med. 2022, 11, 3463. [Google Scholar] [CrossRef]
- Croghan, S.M.; Compton, N.; Manecksha, R.P.; Cullen, I.M.; Daly, P.J. En bloc transurethral resection of bladder tumors: A review of current techniques. Can. Urol. Assoc. J. 2022, 16, E287–E293. [Google Scholar] [CrossRef]
- Lin, L.; Guo, X.; Ma, Y.; Zhu, J.; Li, X. Does repeat transurethral resection of bladder tumor influence the diagnosis and prognosis of T1 bladder cancer? A systematic review and meta-analysis. Eur. J. Surg. Oncol. 2022. [Google Scholar] [CrossRef]
- Wong, V.K.; Ganeshan, D.; Jensen, C.T.; Devine, C.E. Imaging and Management of Bladder Cancer. Cancers 2021, 13, 1396. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Guidelines Body | Version | Recommendation on Suitable reTURB Candidates | Recommendation Strength | ReTURB Period after the Initial Resection |
|---|---|---|---|---|
| European Association of Urology | 2022 | 1. Incomplete initial TURB, or in case of doubt about the completeness of a TURB; 2. If there is no detrusor muscle in the specimen after initial resection, except for Ta LG/G1 tumors and primary CIS; 3. T1 tumors. | Strong | 2–6 weeks |
| National Comprehensive Cancer Network (NCCN) | Version 2.2022 | 1. Visually incomplete resection or high-volume tumor 2. TaHG, particularly if large, and/or no muscle in the specimen 3. T1 tumors | 2A * | 2–6 weeks |
| European Society for Medical Oncology (ESMO) | 2021 | 1. The initial TURB was incomplete. 2. If no detrusor muscle exists in the specimen on the initial resection, except for Ta LG and CIS. 3. In all pT1 tumors and all HG tumors, except for patients with primary CIS | Strong | 4–6 weeks |
| Canadian Urological Association | 2021 | 1. Incomplete initial TURB 2. TaHG tumors (e.g., large and/or multiple tumors) 3. T1 tumors | 1. Strong 2. Weak 3. Strong | within 6 weeks |
| American Urological Association & Society of Urological Oncology | 2020 | 1. Incomplete initial TURB 2. TaHG tumors 3. T1 tumors | 1. Strong 2. Moderate 3. Strong | within 6 weeks |
| Chinese Urological Association | 2019 | 1. Incomplete initial TURB 2. No muscle in specimen except for Ta LG/Gl and primary CIS 3. T1 tumors. | Moderate | 2–6 weeks |
| SIU & International Consultation on Bladder Cancer (ICUD) 2017 | 2017 | 1. Incomplete initial resection 2. TaHG tumors, particularly for patients with large or multifocal tumors 3. T1 disease | 1. B ** 2. C ** 3. B ** | within 6 weeks |
| National Institute for Clinical Excellence (NICE) | 2015 | 1. All high-risk non-muscle invasive bladder cancer | 1. Low | within 6 weeks |
| First Author & Year | Country | Study Type | Study Period | Re TURB Time | Participants | Groups | Patient Number | Male/ Female | Age Mean ± SD (Range) /Median (IQR) | Stage Ta/T1/Tis | Grade LG/HG | Residual Tumor (%) | Up Stage (%) | Recurrence (%) | RFS | Progression | PFS |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Zhou 2020 [32] | China | RC | June 2012–June 2018 | Within 2–6 weeks | Primary T1 and HG/G3 tumors, excluding primary CIS. | ReTURB | 108 | 86/22 | 66.12 ± 1.52 | 60/48/0 | 25/83 | 6 (5.6) | 2 (1.85) | 23 (21.3) | 1 year: 92.6 2 year: 88.4 * 3 year: 84.3 5 year: 68.0 * | 4 (3.7) | 1 year: 98.1 3 year: 96.3 |
| Control | 143 | 111/32 | 68.59 ± 1.36 | 87/56/0 | 49/94 | 11 (7.69) | 2 (1.40) | 39 (27.2) | 1 year: 90.2 2 year: 84.2 * 3 year: 80.4 5 year: 54.1 * | 7 (4.9) | 1 year: 97.9 3 year: 95.1 | ||||||
| Xu 2021 [36] | China | RC | June 2015–June 2019 | Within 6 weeks | Primary T1/TaHG tumors, Tumor number ≤ 4 Diameter ≤ 4 cm | ReTURB | 51 | 41/10 | 67.4 ± 9.5 | 16/35/0 | 13/38 | 3 (5.88) | 0 (0) | 10 (19.6) | 1 year: 92.2 2 year: 87.6 * 3 year: 81.1 * 5 year: 71.5 * | 2 (3.9) | NA |
| Control | 64 | 53/11 | 66.8 ± 9.0 | 15/49/0 | 10/54 | 2 (3.13) | 0 (0) | 18 (28.1) | 1 year: 90.6 2 year: 81.1 * 3 year: 66.4 * 5 year: 63.1 * | 1 (1.5) | NA | ||||||
| Yanagisawa 2022 [38] | Japan | RC | April 2013–February 2021 | Within 2–6 weeks | T1 Tumors | ReTURB | 50 | 33/17 | 74 (70.25–78) | 0/50/0 | 0/50 | 9 (18.0) | 0 (0) | 18 (36.0) | 1 year: 66.5 * 2 year: 55.1 3 year: 54.9 * 5 year: 54.9 * | 7 (14.0) | 1 year: 95.7 * 3 year: 80.6 5 year: 64.5 * |
| Control | 56 | 43/13 | 76 (69–82.25) | 0/56/0 | 0/56 | NA | NA | 18 (32.1) | 1 year: 71.3 * 2 year: 59.9 3 year: 59.9 * 5 year: 54.0 * | 6 (10.7) | 1 year: 95.7 * 3 year: 82.6 5 year: 82.6 * | ||||||
| Wolters 2011 [27] | Germany | CS | June 2010–October 2010 | Within 6 weeks | Solitary papillary lesions, treatment-naive, on the lower bladder wall and trigonum | ReTURB | 5 | 4/1 | 57 (57–80) | 2/3/0 | G1 1 G2 1 G3 3 | NA | NA | NA | NA | NA | NA |
| Muto 2014 [28] | Italy | PCS | April 2011–September 2012 | Within 30–90 days | Naïve NMIBC | ReTURB | 48 | NA | NA | 31/17/0 | 31/17/0 | 0 (0) | 0 (0) | 7 (14.6) | 1.5 year: 85.4 | 0 (0) | NA |
| Migliari 2015 [29] | Italy | PC | February 2012–September 2013 | Within 90 days | Single papillary bladder tumor, diameter ≥ 1 cm | ReTURB | 53 | NA | NA | 30/23/0 | 30/23 | 0 (0) | 0 (0) | 12 (22.6) | 1.5 year: Ta 90.0 T1 76.0 | 0 (0) | NA |
| Hurle 2020 [30] | Italy | RCS | September 2011–April 2017 | Within 40 days | First diagnosis or a primary recurrence of High-risk NMIBC, a single tumor of ≤3 cm and ≤4 lesions | ReTURB | 78 | 51/27 | 68 ± 9 | 17/57/4 | G3 72 | 5 (6.41) | 0 (0) | 11 (14.1) | 1 year: 93.4 * 2 year: 92.0 * 3 year: 85.0 * 5 year: 85.0 * | 1 (1.3) | NA |
| Yang 2020 [31] | China | PC | October 2015–June 2017 | Within 2–6 weeks | Primary, HG and/or T1 tumor; diameter between 1.0 to 3.0 cm | ReTURB | 28 | NA | NA | NA | NA | 2 (7.14) | 1 (3.57) | NA | NA | NA | NA |
| Hashem 2021 [33] | Egypt | RCT | September 2015–September 2018 | 4 weeks after the primary resection | NMIBC | ReTURB | 44 | NA | NA | 2/42 | 28/16 | 3 (6.82) | 0 (0) | 7 (15.9) | 1 year: 92.6 * 2 year: 80.0 * 3 year: 80.0 * | NA | NA |
| Hu 2021 [34] | China | RCS | January 2019–October 2019 | 4–6 weeks | Primary T1 or TaHG | ReTURB | 10 | NA | NA | NA | NA | 0 (0) | 0 (0) | NA | NA | NA | NA |
| Poletajew 2021 [35] | Poland | PC | NA | Within 2–6 weeks | 1–4 cm in diameter. | ReTURB | 37 | NA | NA | NA | NA | 11 (29.73) | NA | NA | NA | NA | NA |
| Fan 2022 [37] | China | RCS | 2013– 2019 | Within 6 weeks | NA | ReTURB | 27 | NA | NA | NA | NA | 4 (14.81) | NA | NA | NA | NA | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, H.; Zhou, M.; Yang, B.; Zhou, S.; Liu, Z.; Zhang, J. A Systematic Review on the Role of Repeat Transurethral Resection after Initial en Bloc Resection for Non-Muscle Invasive Bladder Cancer. J. Clin. Med. 2022, 11, 5049. https://doi.org/10.3390/jcm11175049
Hu H, Zhou M, Yang B, Zhou S, Liu Z, Zhang J. A Systematic Review on the Role of Repeat Transurethral Resection after Initial en Bloc Resection for Non-Muscle Invasive Bladder Cancer. Journal of Clinical Medicine. 2022; 11(17):5049. https://doi.org/10.3390/jcm11175049
Chicago/Turabian StyleHu, Henglong, Mengqi Zhou, Binrui Yang, Shiwei Zhou, Zheng Liu, and Jiaqiao Zhang. 2022. "A Systematic Review on the Role of Repeat Transurethral Resection after Initial en Bloc Resection for Non-Muscle Invasive Bladder Cancer" Journal of Clinical Medicine 11, no. 17: 5049. https://doi.org/10.3390/jcm11175049
APA StyleHu, H., Zhou, M., Yang, B., Zhou, S., Liu, Z., & Zhang, J. (2022). A Systematic Review on the Role of Repeat Transurethral Resection after Initial en Bloc Resection for Non-Muscle Invasive Bladder Cancer. Journal of Clinical Medicine, 11(17), 5049. https://doi.org/10.3390/jcm11175049