


Impact of COVID-19 Pandemic on Initiation of Immunosuppressive Treatment in Immune-Mediated Inflammatory Diseases in Austria: A Nationwide Retrospective Study
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants and Data Extraction
2.3. Objectives
2.4. Data Analysis
2.5. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
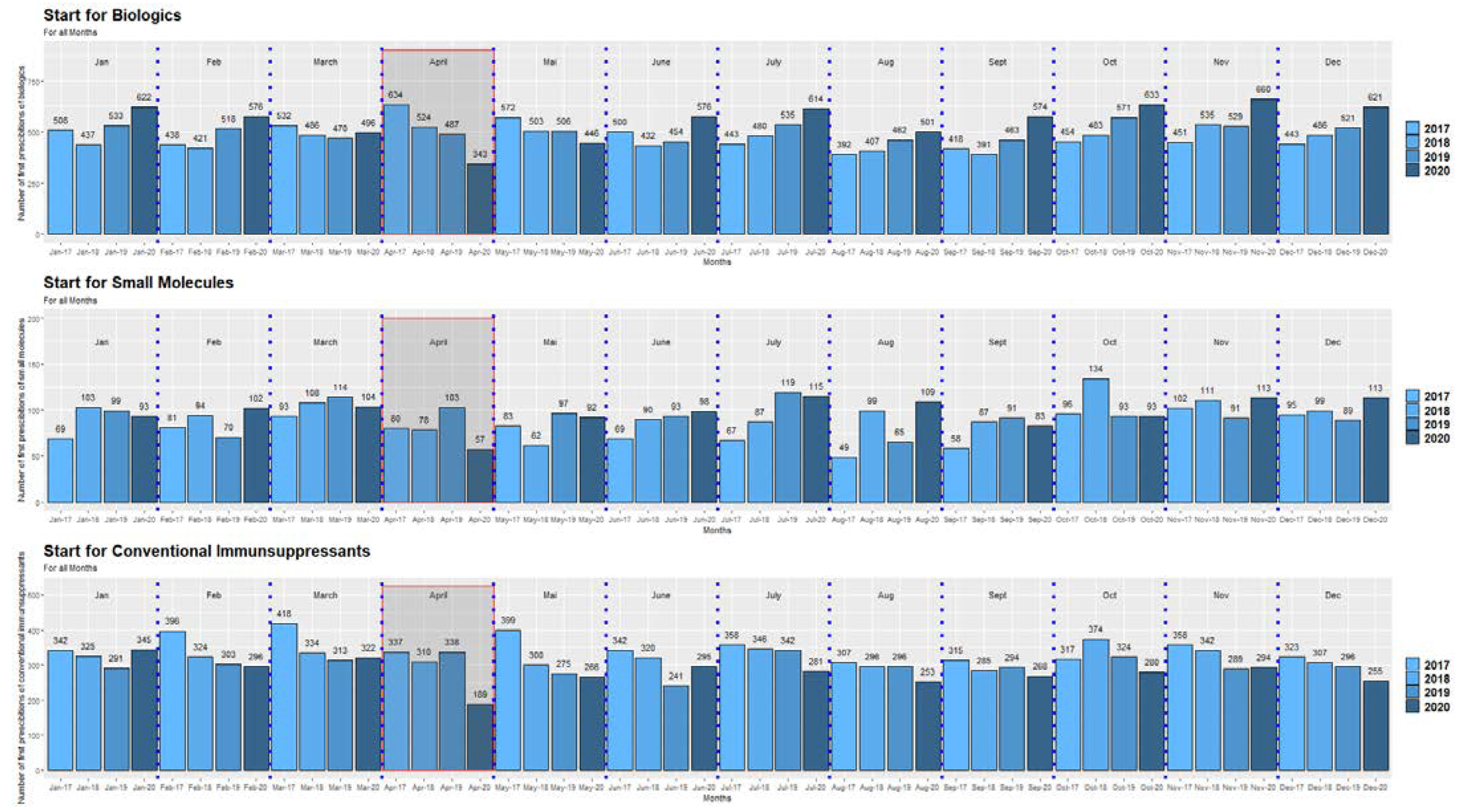
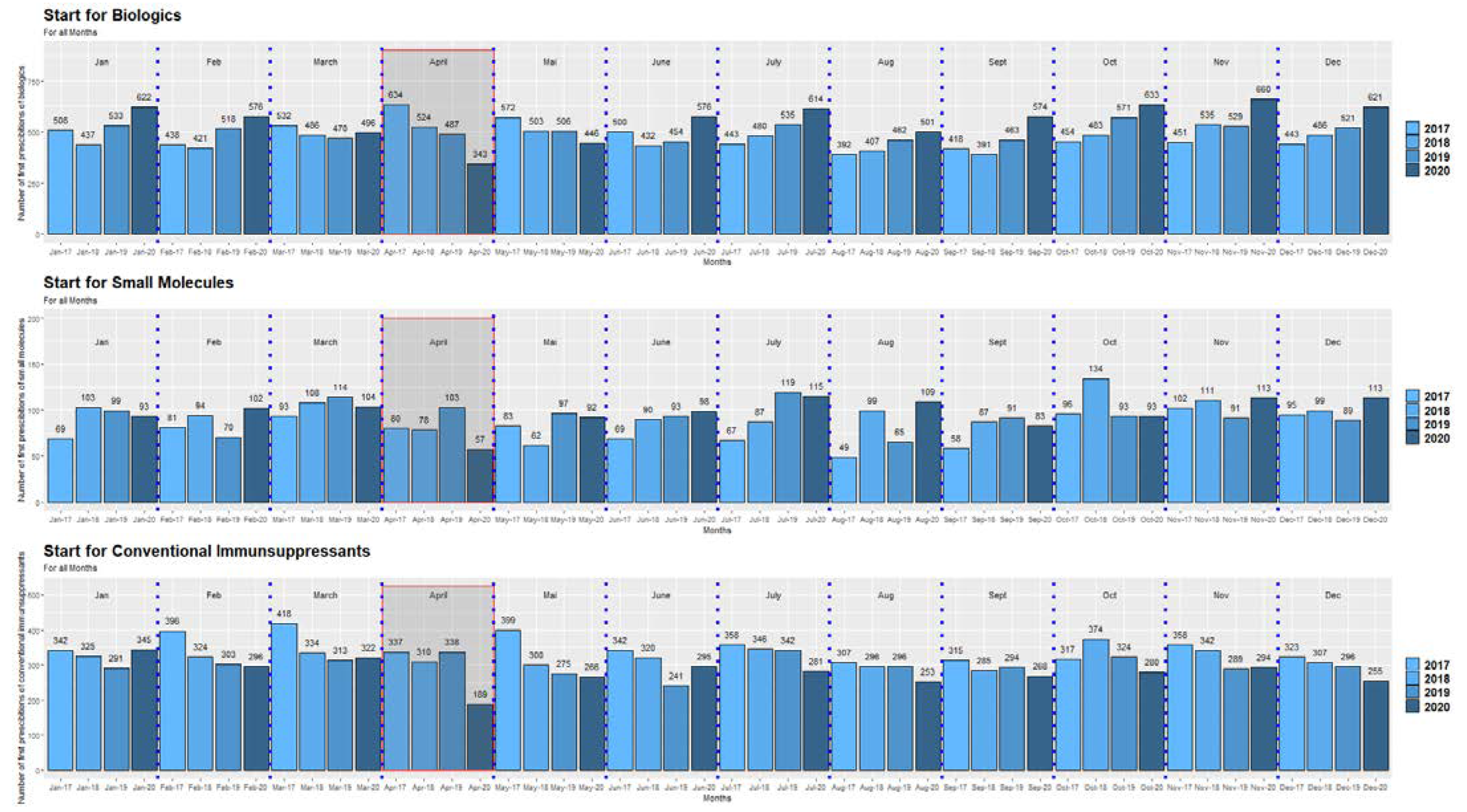
3.2. Impact of the COVID-19 Pandemic on the Initiation of Conventional Immunosuppressive and Advanced Targeted Therapies
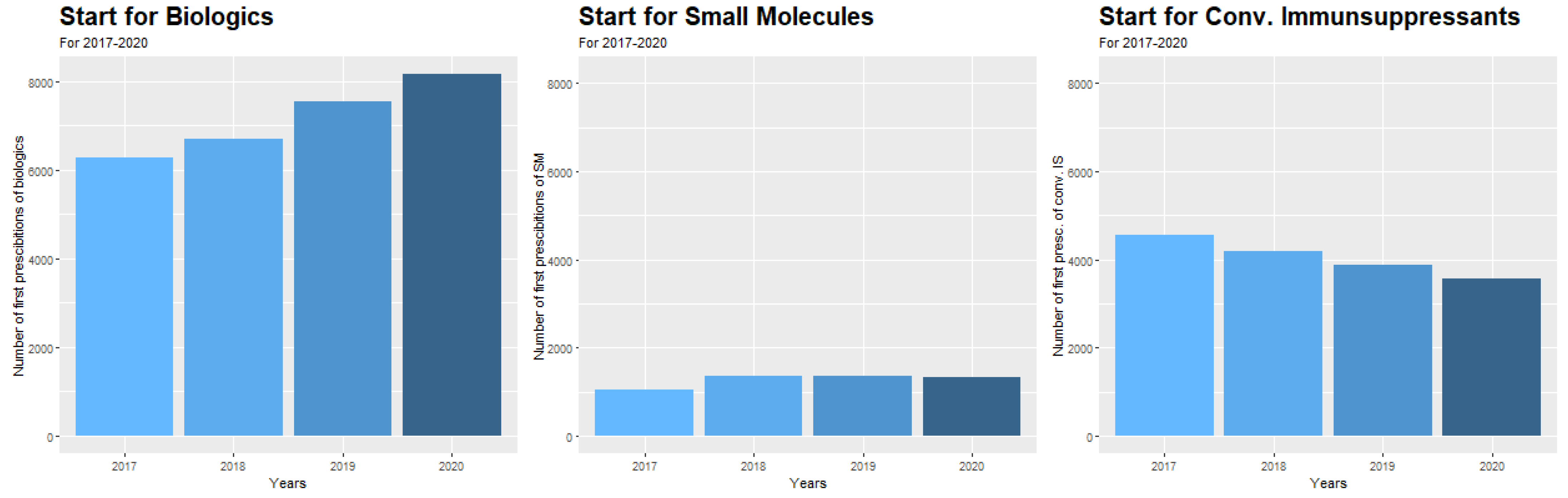
3.3. Changes in the Initiation of Therapies during the Observation Period Independent from COVID-19
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Conference Presentation
Abbreviations
| ADT | advanced targeted therapies |
| IMID | immune-mediated inflammatory diseases |
| IBD | inflammatory bowel diseases |
| RA | rheumatoid arthritis |
| PA | psoriatic arthritis |
| SM | small molecules |
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Lu, R.; Zhao, X.; Li, J.; Niu, P.; Yang, B.; Wu, H.; Wang, W.; Song, H.; Huang, B.; Zhu, N.; et al. Genomic characterization and epidemiology of 2019 novel coronavirus: Implications for virus origins and receptor binding. Lancet 2020, 395, 565–574. [Google Scholar] [CrossRef]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yabg, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. China Novel Coronavirus Investigating and Research Team. A novel coronavirus from patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Morens, D.M.; Daszak, P.; Taubenberger, J.K. Escaping Pandora’s box—Another novel coronavirus. N. Engl. J. Med. 2020, 382, 1293–1295. [Google Scholar] [CrossRef]
- Available online: https://coronavirus.jhu.edu/map.html (accessed on 31 July 2022).
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.; Ou, C.; He, J.; Liu, L.; Shan, H.; Lei, C.; Hui, D.; et al. China Medical Treatment Expert Group for Covid-19. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Vygen-Bonnet, S.; Koch, J.; Bogdan, C.; Harder, T.; Heininger, U.; Kling, K.; Littmann, M.; Meerpohl, J.; Meyer, H.; Mertens, T.; et al. Beschluss und wissenschaftliche begründung der Ständigen Impfkommission (STIKO) für die COVID-19-Impfempfehlung. Epid. Bull. 2021, 2, 3–63. [Google Scholar]
- Mayerhöfer, T.; Klein, S.; Peer, A.; Perschinka, F.; Lehner, G.; Hasslacher, J.; Bellmann, R.; Gasteiger, L.; Mittermayr, M.; Exchertzhuber, S.; et al. Changes in characteristics and outcomes of critically ill COVID-19 patients in Tyrol (Austria) over 1 year. Wien. Klin. Wochenschr. 2021, 133, 1237–1247. [Google Scholar] [CrossRef]
- Gao, Y.; Ding, M.; Dong, X.; Zhang, J.; Azkur, A.; Azkur, D.; Gan, H.; Sun, Y.; Fu, W.; Li, W.; et al. Risk factors for severe and critically ill COVID-19 patients: A review. Allergy 2021, 76, 428–455. [Google Scholar] [CrossRef]
- Gomollón, F.; Dignass, A.; Annese, V.; Tilg, H.; Assche, G.; Lindsay, J.; Peyrin-Biroulet, L.; Cullen, G.; Daperno, M.; Kucharzik, T.; et al. 3rd European Evidence-based Consensus on the diagnosis and Management of Crohn’s Disease 2016: Part 1: Diagnosis and Medical Treatment. J. Crohn’s Colitis 2017, 11, 3–25. [Google Scholar] [CrossRef]
- Harbord, M.; Eliakim, R.; Bettenworth, D.; Karmiris, K.; Katsanos, K.; Kopylov, U.; Kucharzik, T.; Molnár, T.; Raine, T.; Sebastian, S.; et al. Third European Evidence-based Consensus on Diagnosis and Management of Ulcerative Colitis. Part 2: Current Management. J. Crohn’s Colitis 2017, 11, 769–784. [Google Scholar] [CrossRef]
- Aletaha, D.; Smolen, J.S. Diagnosis and management of rheumatoid arthritis: A review. JAMA 2018, 320, 1360–1372. [Google Scholar] [CrossRef] [PubMed]
- Ighani, A.; Partridge, A.; Shear, N.; Lynde, C.; Gulliver, W.; Sibbald, C.; Fleming, P. Comparison of management guidelines for moderate-to-severe plaque psoriasis: A review of phototherapy, systemic therapies, and biologic agents. J. Cutan. Med. Surg. 2019, 23, 204–221. [Google Scholar] [CrossRef] [PubMed]
- Verstockt, B.; Ferrante, M.; Vermeire, S.; Van Assche, G. New treatment options for inflammatory bowel diseases. J. Gastroenterol. 2018, 53, 585–590. [Google Scholar] [CrossRef] [PubMed]
- Kirchgesner, J.; Lemaitre, M.; Carrat, F.; Zureik, M.; Carbonnel, F.; Dray-Spira, R. Risk of serious and opportunistic infections associated with treatment of inflammatory bowel diseases. Gastroenterology 2018, 155, 337–346.e10. [Google Scholar] [CrossRef]
- Kirchgesner, J.; Deai, R.; Beaugerie, L.; Schneeweiss, S.; Kim, S. Risk of serious infections with vedolizumab versus tumor necrosis factor antagonists in patients with inflammatory bowel disease. Clin. Gastroenterol. Hepatol. 2022, 20, 314–324. [Google Scholar] [CrossRef]
- Restellini, S.; Pittet, V. Inflammatory Bowel Disease and COVID-19. ECCO Letter. Published 30 September 2020. Available online: https://ecco-ibd.eu/publications/ecco-news/item/inflammatory-bowel-disease-and-covid-19.html (accessed on 31 July 2022).
- Alunno, A.; Najm, A.; Machado, P.; Bertheussen, H.; Burmester, G.; Carubbi, F.; De Mraco, G.; Giacomelli, R.; Hermine, O.; Isaacs, J.; et al. EULAR points to consider on pathophysiology and use of Immunomodulatory therapies in COVID-19. Ann. Rheum. Dis. 2021, 80, 698–706. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Clinical Guidance for Adult Patients with Rheumatic Diseases, Developed by the ACR COVID-19 Clinical Guidance Task Force. Available online: https://www.rheumatology.org/Portals/0/Files/ACR-COVID-19-Clinical-Guidance-Summary-Patients-with-Rheumatic-Diseases.pdf (accessed on 31 July 2022).
- Lin, S.; Lau, L.; Chanchlani, L.; Kennedy, N.; Ng, S. Recent advances in clinical practice: Management of inflammatory bowel disease during the COVID-19 pandemic. Gut 2022, 71, 1426–1439. [Google Scholar] [CrossRef] [PubMed]
- Scaldaferri, F.; Pugliese, D.; Privitera, G.; Onali, S.; Lopetuso, L.; Rizzati, G.; Settanni, C.; Pizzoferrato, M.; Schiavoni, E.; Turchini, L.; et al. Impact of COVID-19 pandemic on the daily management of biotechnological therapy in inflammatory bowel disease patients: Reorganisational response in a high-volume Italian inflammatory bowel disease centre. United Eur. Gastroenterol. J. 2020, 8, 775–781. [Google Scholar] [CrossRef]
- Saibeni, S.; Scucchi, L.; Dragoni, G.; Bezzio, C.; Miranda, A.; Ribaldone, D.; Bertani, A.; Bossa, F.; Allocca, M.; Buda, D.; et al. Activities related to inflammatory bowel disease management during and after the coronavirus disease 2019 lockdown in Italy: How to maintain standards of care. United Eur. Gastroenterol. J. 2020, 8, 1228–1235. [Google Scholar] [CrossRef]
- Allocca, M.; Fiorino, G.; Furfaro, F.; Gilardi, D.; Radice, S.; D’Amico, F.; Zilli, A.; Danese, S. Maintaining the Quality Standards of Care for Inflammatory Bowel Disease Patients during the COVID-19 pandemic. Clin. Gastroenterol. Hepatol. 2020, 18, 1882–1883. [Google Scholar] [CrossRef]
- Shintaro, A.; Shadi, H.; Dejan, M.; Sakuraba, A. Prevalence and Clinical outcomes of COVID-19 in patients with autoimmune diseases: A systematic review and meta-analysis. Ann. Rheum. Dis. 2021, 80, 384–391. [Google Scholar]
- Ungaro, C.; Brenner, E.; Gearry, R.; Kaplan, G.; Kissous-Hung, M.; Lewis, J.; Ng, S.; Rahier, J.; Reinisch, W.; Steinwurz, F.; et al. Effect of IBD medications on COVID-19 outcomes: Results from an international registry. Gut 2021, 70, 725–732. [Google Scholar] [CrossRef] [PubMed]
- Bachiller-Corral, J.; Boteanu, A.; Garcia-Villanueva, M.; Puente, C.; Revenga, M.; Diaz-Miguel, M.; Rodriguez-Garcia, A.; Morell-Hita, J.; Valero, M.; Larena, C.; et al. Risk of severe COVID-19 infection in patients with inflammatory rheumatic diseases. J. Rheutmatol. 2021, 48, 1098–1102. [Google Scholar] [CrossRef] [PubMed]
- Dejaco, C.; Alunno, A.; Bijlsma, J.; Boonen, A.; Combe, B.; Finckh, A.; Machado, P.; Padjen, I.; Sivera, F.; Stamm, T.; et al. Influence of COVID-19 pandemic on decisions for the management of people with inflammatory rheumatic and musculoskeletal diseases: A survey among EULAR countries. Ann. Rheum. Dis. 2020, 80, 518–526. [Google Scholar] [CrossRef]
- Ansarin, K.; Taghizadieh, A.; Safiri, S.; Mahdavi, A.; Ranjbar, S.; Teymouri, S.; Maleki, M.; Khabbazi, A. COVID-19 outcomes in patients with systemic autoimmune diseases treated with immunomodulatory drugs. Ann. Rheum. Dis. Online ahead of print. 2020. [Google Scholar] [CrossRef]
- Emmi, G.; Bettiol, A.; Mattioli, I.; Silvestri, E.; Di Scala, G.; Urban, M.; Vaglio, A.; Prisco, D. SARS-CoV-2 infection among patients with systemic autoimmune diseases. Autoimmun. Rev. 2020, 19, 102575. [Google Scholar] [CrossRef]
- Fredi, M.; Cavazzana, I.; Moschetti, L.; Andreoli, L.; Franceschini, F. COVID-19 in patients with rheumatic diseases in northern Italy: A single-centre observa- tional and case-control study. Lancet Rheumatol. 2020, 2, e549–e556. [Google Scholar] [CrossRef]
- Liu, M.; Gao, Y.; Zhang, Y.; Shi, S.; Chen, Y.; Tian, J. The association between severe or dead COVID-19 and autoimmune diseases: A systematic review and meta-analysis. J. Infect. 2020, 81, e93–e95. [Google Scholar] [CrossRef]
- Macaluso, F.S.; Orlando, A. COVID-19 in patients with inflamma- tory bowel disease: A systematic review of clinical data. Digest. Liver Dis. 2020, 52, 1222–1227. [Google Scholar] [CrossRef]
- D’Silva, K.M.; Serling-Boyd, N.; Wallwork, R.; Hsu, T.; Fu, X.; Gravallese, E.; Choi, H.; Sparks, J.; Wallace, Z. Clinical characteristics and outcomes of patients with coronavirus disease 2019 (COVID-19) and rheumatic disease: A comparative cohort study from a US hot spot. Ann. Rheum. Dis. 2020, 79, 1156–1162. [Google Scholar] [CrossRef]
- Gianfrancesco, M.; Hyrich, K.L.; Al-Adely, S.; Carmona, L.; Danila, M.; Gossec, L.; Izadi, Z.; Jacobsohn, L.; Katz, P.; Lawson-Tovey, S.; et al. Characteristics associated with hospitalisation for COVID-19 in people with rheumatic disease: Data from the COVID-19 Global Rheuma- tology Alliance physician-reported registry. Ann. Rheum. Dis. 2020, 79, 859–866. [Google Scholar] [CrossRef]
- Pablos, J.L.; Galindo, M.; Carmona, L.; Lledó, A.; Retuerto, M.; Blanco, R.; Gonzalez-Gay, M.; Martinez-Lopez, D.; Castrejón, I.; Alvaro-Gracia, J.; et al. Clinical outcomes of hospitalised patients with COVID-19 and chronic inflammatory and autoimmune rheumatic diseases: A multicentric matched cohort study. Ann. Rheum. Dis. 2020, 79, 1544–1549. [Google Scholar] [CrossRef] [PubMed]
- Bower, H.; Frisell, T.; Giuseppe, D.; Delcoigne, B.; Alenius, G.M.; Baecklund, E.; Chatzidionysiou, K.; Feltelius, N.; Forsblad-d’Elia, H.; Kastbom, A.; et al. Effects oft he COVID-19 pandemic on patients with inflammatory joint diseases in Sweden: From infection severity to impact on care provision. RMD Open 2021, 7, e001987. [Google Scholar] [CrossRef]
- Ungaro, R.C.; Brenner, E.; Agrawal, M.; Zhang, X.; Kappelman, M.; Colombel, J.F. Impact of medications on COVID-19 outcomes in inflammatory bowel disease: Analysis of more than 6000 patients from an international registry. Gastroenterology 2022, 162, 316–319. [Google Scholar] [CrossRef]
- Kridin, K.; Schonmann, Y.; Bitan, D.; Damiani, G.; Peretz, A.; Weinstein, O.; Cohen, A. Coronavirus disease 2019 (COVID-19)-associated hospitalization and mortality in patitnets with psoriasis: A population-based study. Am. J. Clin. Dermatol. 2021, 22, 709–718. [Google Scholar] [CrossRef] [PubMed]
- Izadi, Z.; Brenner, E.; Mahil, S.; Dand, N.; Yiu, Z.; Yates, M.; Ungaro, R.; Zhang, X.; Agrawal, M.; Colombel, J.F. Association between tumor necrosis factor inhibitors and the risk of hopitalisation or death among patients with immune-mediated inflammatory disesase and COVID-19. JAMA Netw. Open 2021, 4, e2129639. [Google Scholar] [CrossRef] [PubMed]
- Regierer, A.C.; Hasseli, R.; Schäfer, M.; Hoyer, B.; Krause, A.; Lorenz, H.M.; Pfeil, A.; Richter, J.; Schmeiser, T.; Schulze-Koops, H.; et al. TNFi is associated with positive outcome, but JAKi and rituximab are associated with negative outcomes of SARS-CoV-2 infection in patients with RMD. RMD Open 2021, 7, e001896. [Google Scholar] [CrossRef]
- Magro, F.; Rahier, J.-F.; Abreu, C.; MacMahon, E.; Hart, A.; Van der Woude, C.; Gordon, H.; Adamina, M.; Viget, N.; Vavricka, S.; et al. Inflammatory Bowel Disease Management During the COVID-19 Outbreak: The Ten Do’s and Don’ts from the ECCO-COVID Taskforce. J. Crohn’s Colitis 2020, 14 (Suppl. S3), S798–S806. [Google Scholar] [CrossRef]
- Morris, E.; Goldacre, R.; Spata, E.; Mafham, M.; Finan, P.; Shelton, J.; Richards, M.; Spencer, K.; Emberson, J.; Hollings, S.; et al. Impact of the COVID-19 pandemic on the detection and management of colorectal cancer in England: A population-based study. Lancet Gastroenterol. Hepatol. 2021, 6, 199–208. [Google Scholar] [CrossRef]
- Groen, M.; Derks, M.; Kuijpers, C.; Nagtegaal, I.; Hoentjen, F. Reduction in Inflammatory Bowel Disease Healthcare during the Coronavirus Disease 2019 Pandemic: A nationwide retrospective cohort study. Gastroenterology 2021, 160, 935–937. [Google Scholar] [CrossRef]
- Mendelsohn, A.; Nam, Y.; Marshall, J.; McDermott, C.; Kochar, B.; Kappelman, M.; Brown, J.; Lockhart, C. Utilization patterns and characteristics of users of biologic anti-inflammatory agents in a large, US commercially insured population. Pharmacol. Res. Perspect. 2021, 9, e00708. [Google Scholar] [CrossRef]
- Han, J.; Lee, J.; Han, K.; Seo, H.; Bang, C.; Park, Y.; Lee, J.; Park, Y. Epidemiology and medication trends in patients with Psoriasis: A nationwide population-based Cohort Study from Korea. Acta Derm. Venereol. 2018, 98, 396–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sánchez-Piedra, C.; Sueiro-Delgado, D.; García-González, J.; Ros-Vilamajo, I.; Prior-Español, A.; Moreno-Ramos, M.; Garcia-Magallon, B.; Calvo-Gutiérrez, J.; Perez-Vera, Y.; Martín-Domenech, R.; et al. Changes in the use patterns of bDMARDs in patients with rheumatic diseases over the past 13 years. Sci. Rep. 2021, 11, 15051. [Google Scholar] [CrossRef] [PubMed]
- Alulis, S.; Vadstrup, K.; Borsi, A.; Nielsen, A.; Jørgensen, T.; Qvist, N.; Munkholm, P. Treatment patterns for biologics in ulcerative colitis and Crohn’s disease: A Danish nationwide register study from 2003 to 2015. Scand. J. Gastroenterol. 2020, 55, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Torres, J.; Bonovas, S.; Doherty, G.; Kucharzik, T.; Gisbert, J.; Raine, T.; Adamina, M.; Armuzzi, A.; Bachmann, O.; Bager, P.; et al. on behalf of the European Crohn’s and Colitis Organisation [ECCO], ECCO Guidelines on Therapeutics in Crohn’s Disease: Medical Treatment. J. Crohn’s Colitis 2020, 14, 4–22. [Google Scholar] [CrossRef]
- Raine, T.; Bonovas, S.; Burisch, J.; Kucharzik, T.; Adamina, M.; Annese, V.; Bachmann, O.; Bettenworth, D.; Chaparro, M.; Czuber-Dochan, W.; et al. ECCO Guidelines on Therapeutics in Ulcerative Colitis: Medical Treatment. J. Crohn’s Colitis 2022, 16, 2–17. [Google Scholar] [CrossRef]
- Alunno, A.; Najm, A.; Machado, P.M.; Bertheussen, H.; Burmester, G.R.; Carubbi, F.; De Marco, G.; Giacomelli, R.; Hermine, O.; Isaacs, J.; et al. 2021 update of the EULAR points to consider on the use of immunomodulatory therapies in COVID-19. Ann. Rheum. Dis. 2022, 81, 34–40. [Google Scholar] [CrossRef]
- Menter, A.; Strober, B.E.; Kaplan, D.H.; Kivelevitch, D.; Prater, E.; Stoff, B.; Armstrong, A.; Connor, C.; Cordoro, K.; Davis, D.; et al. Joint AAD-NPF guidelines of care for the management and treatment of psoriasis with biologics. J. Am. Acad Dermatol. 2019, 80, 1029–1072. [Google Scholar] [CrossRef]
- Alatab, S.; Sepanlou, S.; Ikuta, K.; Vahedi, H.; Bisignano, C.; Safiri, S.; Sadeghi, A.; Nixon, M.; Abdoli, A.; Abolhassani, H.; et al. on behalf of the GBD 2017 Inflammatory Bowel Disease Collaborators. The global, regional, and national burden of inflammatory bowel disease in 195 countries and territories, 1990–2017: A systematic analysis for the global burden of disease study 2017. Lancet Gastroenterol. Hepatol. 2020, 5, 17–30. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Biologics | TNF-Alpha Inhibitors | Adalimumab, Certolizumab Pegol, Etanercept, Golimumab, Infliximab |
|---|---|---|
| Anti C5 | eculizumab | |
| IL-1 inhibitors | anakinra, canakinumab | |
| IL-4 inhibitors | dupilumab | |
| IL-6 inhibitors | sarilumab, tocilizumab | |
| IL-17 Inhibitors | brodalumab, ixekizumab, secukinumab | |
| IL-23 inhibitors | guselkumab, risankizumab, tildrakizumab | |
| IL12/23 inhibitor | ustekinumab | |
| Anti-BAFF | belimumab | |
| B-cell depletion | rituximab | |
| integrin α4β7 inhibitor | vedolizumab | |
| Co-Stimulation inhibitor | abatacept | |
| Small molecules | PDE4 inhibitors | apremilast |
| JAK-inhibitors | baricitinib, tofacitinib, upadacitinib | |
| Conventional immunosuppressive medications | azathioprine, cyclosporine, leflunomide, mycophenolate mofetil, methotrexate | |
| Others | sulfalazine, mesalazine |
| Diagnosis | n (%) |
|---|---|
| Crohn’s disease; n (%) | 3488 (37.8) |
| Ulcerative colitis; n (%) | 2805 (30.4) |
| Rheumatoid arthritis; n (%) | 1543 (16.7) |
| Plaque psoriasis; n (%) | 629 (6.8) |
| Ankylosing spondylitis; n (%) | 259 (2.8) |
| Hidradenitis suppurativa; n (%) | 179 (1.9) |
| Childhood arthritis; n (%) | 151 (1.6) |
| Uveitis; n (%) | 112 (1.2) |
| Psoriatic arthritis; n (%) | 35 (0.4) |
| Behçet–Krankheit; n (%) | 33 (0.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kutschera, M.; Ritschl, V.; Reichardt, B.; Stamm, T.; Kiener, H.; Maier, H.; Reinisch, W.; Benka, B.; Novacek, G. Impact of COVID-19 Pandemic on Initiation of Immunosuppressive Treatment in Immune-Mediated Inflammatory Diseases in Austria: A Nationwide Retrospective Study. J. Clin. Med. 2022, 11, 5308. https://doi.org/10.3390/jcm11185308
Kutschera M, Ritschl V, Reichardt B, Stamm T, Kiener H, Maier H, Reinisch W, Benka B, Novacek G. Impact of COVID-19 Pandemic on Initiation of Immunosuppressive Treatment in Immune-Mediated Inflammatory Diseases in Austria: A Nationwide Retrospective Study. Journal of Clinical Medicine. 2022; 11(18):5308. https://doi.org/10.3390/jcm11185308
Chicago/Turabian StyleKutschera, Maximilian, Valentin Ritschl, Berthold Reichardt, Tanja Stamm, Hans Kiener, Harald Maier, Walter Reinisch, Bernhard Benka, and Gottfried Novacek. 2022. "Impact of COVID-19 Pandemic on Initiation of Immunosuppressive Treatment in Immune-Mediated Inflammatory Diseases in Austria: A Nationwide Retrospective Study" Journal of Clinical Medicine 11, no. 18: 5308. https://doi.org/10.3390/jcm11185308
APA StyleKutschera, M., Ritschl, V., Reichardt, B., Stamm, T., Kiener, H., Maier, H., Reinisch, W., Benka, B., & Novacek, G. (2022). Impact of COVID-19 Pandemic on Initiation of Immunosuppressive Treatment in Immune-Mediated Inflammatory Diseases in Austria: A Nationwide Retrospective Study. Journal of Clinical Medicine, 11(18), 5308. https://doi.org/10.3390/jcm11185308