
Lipid Peroxidation Levels in Saliva and Plasma of Patients Suffering from Periodontitis

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
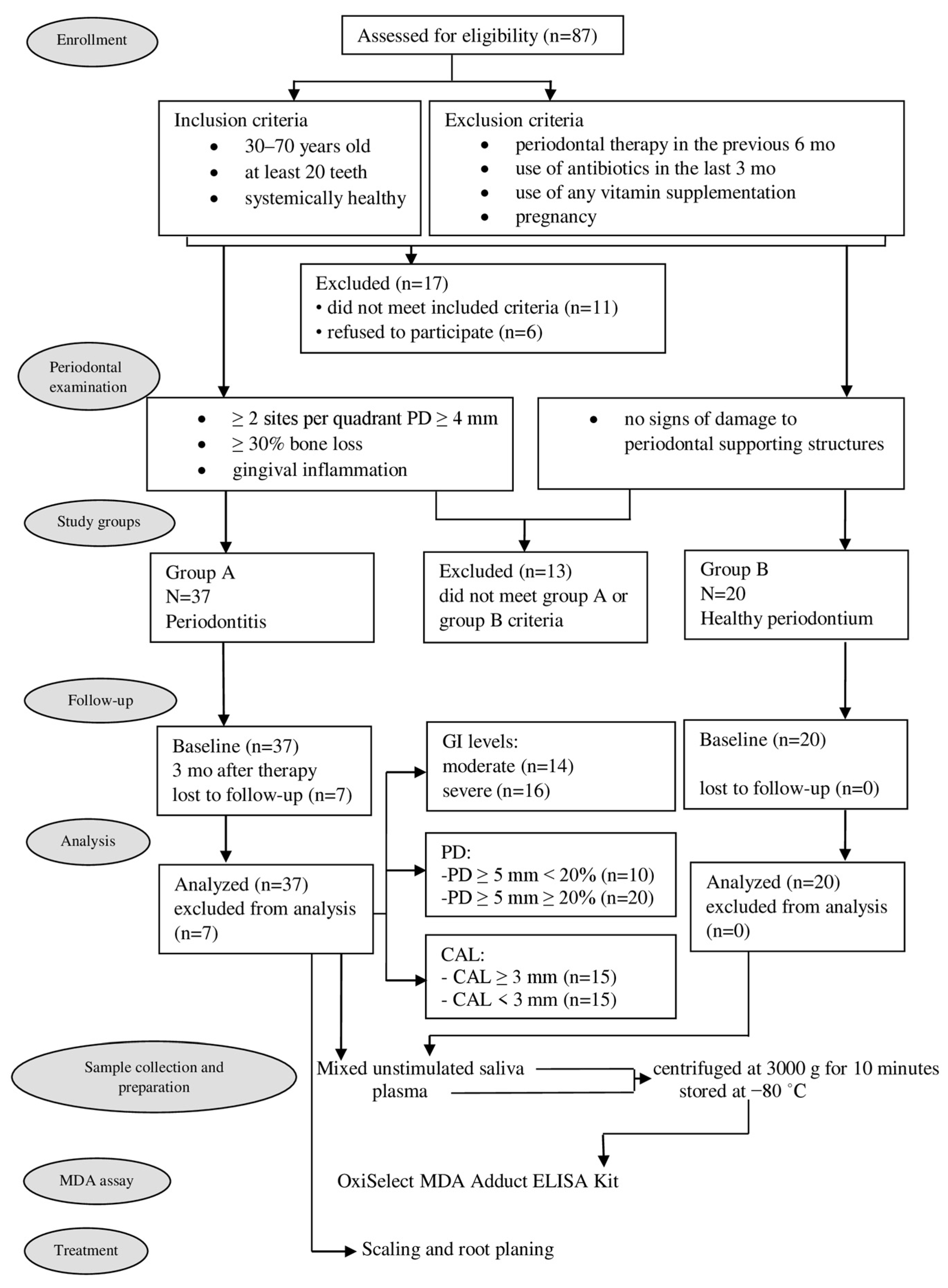
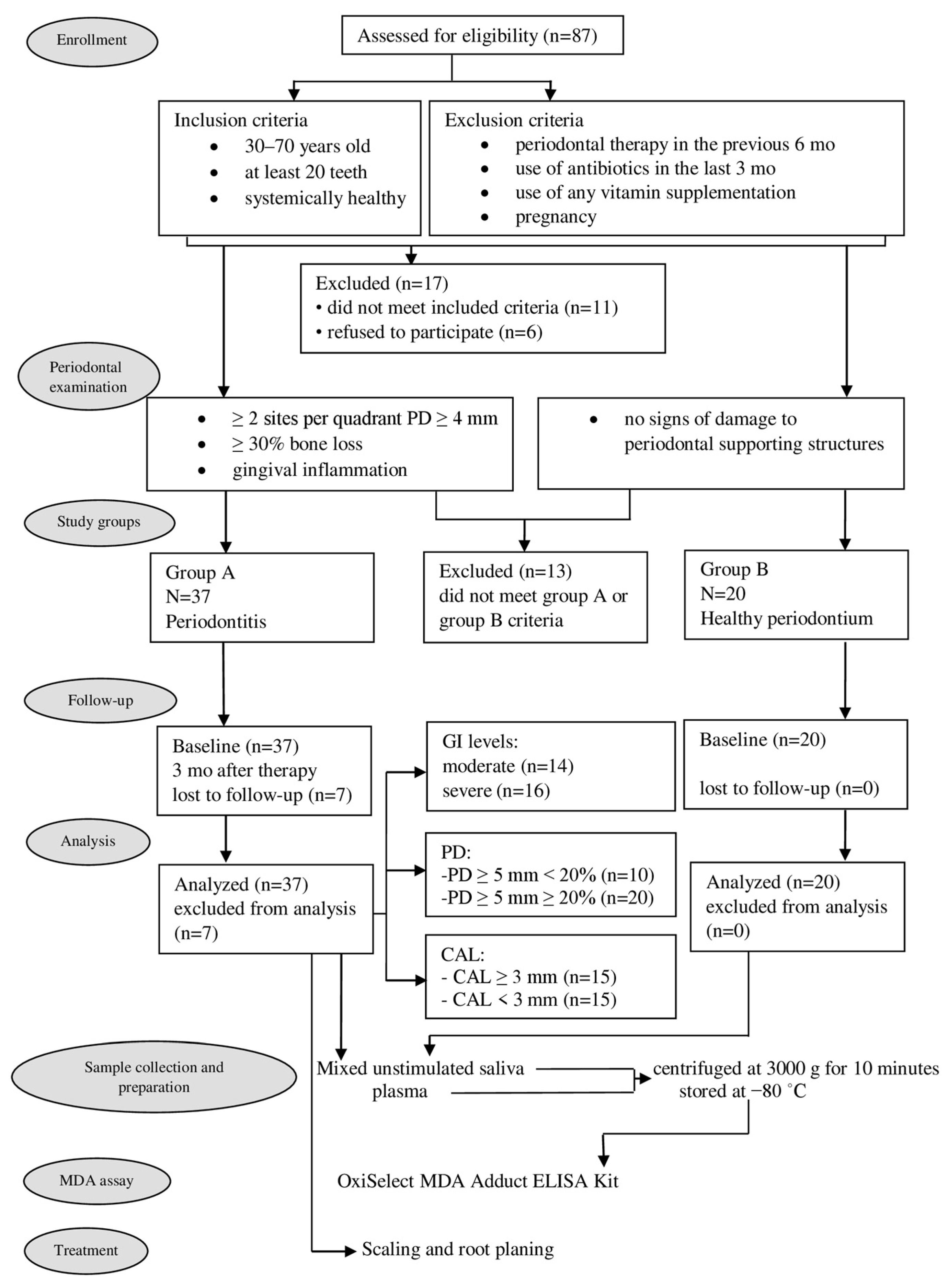
2.1. Subjects
2.2. Periodontal Examination
2.3. Study Groups
2.4. Sample Collection and Preparation
2.5. MDA Assay
2.6. Treatment
2.7. Follow-Up
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Peterson, P.E.; Ogawa, H. Strengthening the Prevention of Periodontal Disease: The WHO Approach. J. Periodontol. 2005, 76, 2187–2193. [Google Scholar] [CrossRef] [PubMed]
- Żukowski, P.; Maciejczyk, M.; Waszkiel, D. Sources of free radicals and oxidative stress in the oral cavity. Arch. Oral Biol. 2018, 92, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Andrukhov, O.; Rausch-Fan, X. Oxidative Stress and antioxidant system in periodontitis. Front. Physiol. 2017, 8, 910. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaschler, M.M.; Stockwell, B.R. Lipid peroxidation in cell death. Biochem. Biophys. Res. Commun. 2017, 482, 419–425. [Google Scholar] [CrossRef]
- Tsikas, D. Assessment of lipid peroxidation by measuring malondialdehyde (MDA) and relatives in biological samples: Analytical and biological challenges. Anal. Biochem. 2017, 524, 13–30. [Google Scholar] [CrossRef]
- Chole, R.H.; Patil, R.N.; Basak, A.; Palandurkar, K.; Bhowate, R. Estimation of serum malondialdehyde in oral cancer and precancer and its association with healthy individuals, gender, alcohol, and tobacco abuse. J. Cancer Res. Ther. 2010, 6, 487–491. [Google Scholar] [CrossRef]
- Rašić, S.; Rebić, D.; Hasić, S.; Rašić Šarac, M.D. Influence of malondialdehyde and matrix metalloproteinase-9 on progression of carotid atherosclerosis in chronic renal disease with cardiometabolic syndrome. Mediat. Inflamm. 2015, 2015, 614357. [Google Scholar] [CrossRef] [Green Version]
- Kaefer, M.; De Carvalho, J.A.; Piva, S.J.; da Silva, D.B.; Becker, A.M.; Sangoi, M.B.; Almeida, T.C.; Hermes, C.L.; Coelho, A.C.; Tonello, R.; et al. Plasma malondialdehyde levels and risk factors for the development of chronic complications in type 2 diabetic patients on insulin therapy. Clin. Lab. 2012, 58, 973–978. [Google Scholar] [CrossRef]
- Almaeen, A.H.; Alduraywish, A.A.; Mobasher, M.A.; Almadhi, O.I.M.; Nafeh, H.N.; El-Metwally, T.H. Oxidative stress, immunological and cellular hypoxia biomarkers in hepatitis C treatment-naïve and cirrhotic patients. Arch. Med. Sci. 2021, 17, 368–375. [Google Scholar] [CrossRef]
- Rumopa, H.; Wagey, F.W.; Supaarman, E. Malondialdehyde levels in preeclampsia before and after delivery. Obstet. Ginekol. Indones. 2018, 6-3, 143–148. [Google Scholar] [CrossRef]
- Khalili, J.; Biloklytska, H.F. Salivary malondialdehyde levels in clinically healthy and periodontal diseased individuals. Oral Dis. 2008, 14, 754–760. [Google Scholar] [CrossRef] [PubMed]
- Dakovic, D. Malondialdehyde as an Indicator of Local Oxidative Cell Damage in Periodontitis Patients. Master’s Thesis, Military Medical Academy, Belgarde, Serbia, 2005. [Google Scholar]
- Canakci, C.F.; Cicek, Y.; Yildirim, A.; Sezer, U.; Canakci, A. Increased levels of 8-hydroxydeoxyguanosine and malondialdehyde and its relationship with antioxidant enzymes in saliva of periodontitis patients. Eur. J. Dent. 2009, 3, 100–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trivedi, S.; Lal, N.; Mahdi, A.A.; Mittal, M.; Singh, B.; Pandey, S. Evaluation of antioxidant enzymes activity and malondialdehyde levels in patients with chronic periodontitis and diabetes mellitus. J. Periodontol. 2014, 85, 713–720. [Google Scholar] [CrossRef]
- Skutnik- Radziszewska, A.; Zalewska, A. Salivary redox biomarkers in the course of caries and periodontal disease. Appl. Sci. 2020, 10, 6240. [Google Scholar] [CrossRef]
- Akalın, F.A.; Baltacιoğlu, E.; Alver, A.; Karabulut, E. Lipid peroxidation levels and total oxidant status in serum, saliva and gingival crevicular fluid in patients with chronic periodontitis. J. Clin. Periodontol. 2007, 34, 558–565. [Google Scholar] [CrossRef] [PubMed]
- Dhotre, P.S.; Suryaker, A.N.; Bhogade, R.B. Oxidative stress in periodontitis. Eur. J. Gen. Med. 2012, 9, 81–84. [Google Scholar] [CrossRef]
- Cherian, D.A.; Peter, T.; Narayanan, A.; Madhavan, S.S.; Achammada, S.; Vynat, G.P. Malondialdehyde as a marker of oxidative stress in periodontitis patients. J. Pharm. Bioallied Sci. 2019, 11 (Suppl. S2), 297–300. [Google Scholar] [CrossRef] [PubMed]
- Sobaniec, H.; Sobaniec-Lotowska, M.E. Morphological examinations of hard tissues of periodontium and evaluation of selected processes of lipid peroxidation in blood serum of rats in the course of experimental periodontitis. Med. Sci. Monit. 2000, 6, 875–881. [Google Scholar] [PubMed]
- Cesaratto, L.; Vascotto, C.; Calligaris, S.; Tell, G. The importance of redox state in liver damage. Ann. Hepatol. 2004, 3, 86–92. [Google Scholar] [CrossRef]
- Ekuni, D.; Tomofuji, T.; Tamaki, N.; Sanbe, T.; Azuma, T.; Yamanaka, R.; Yamamoto, T.; Watanabe, T. Mechanical stimulation of gingiva reduces plasma 8-OHdG level in rat periodontitis. Arch. Oral Biol. 2008, 53, 324–329. [Google Scholar] [CrossRef]
- Tomofuji, T.; Sanbe, T.; Ekuni, D.; Azuma, T.; Irie, K.; Maruyama, T.; Tamaki, N.; Yamamoto, T. Oxidative damage of rat liver induced by ligature-induced periodontitis and chronic ethanol consumption. Arch. Oral Biol. 2008, 53, 1113–1118. [Google Scholar] [CrossRef] [PubMed]
- Albano, E. Oxidative mechanisms in the pathogenesis of alcoholic liver disease. Mol. Asp. Med. 2008, 29, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Ekuni, D.; Tomofuji, T.; Sanbe, T.; Irie, K.; Azuma, T.; Maruyama, T.; Tamaki, N.; Murakami, J.; Kokeguchi, S.; Yamamoto, T. Periodontitis-induced lipid peroxidation in rat descending aorta is involvedin initiation of atherosclerosis. J. Periodontal Res. 2009, 44, 434–442. [Google Scholar] [CrossRef] [PubMed]
- Silness, J.; Löe, H. Periodontal disease in pregnancy (II). Correlation between oral hygiene and periodontal condition. Acta Odontol. Scand. 1964, 22, 121–135. [Google Scholar] [CrossRef]
- Löe, H.; Silness, P. Periodontal disease in pregnancy I. Prevalence and severity. Acta Odontol. Scand. 1963, 21, 533–551. [Google Scholar] [CrossRef]
- Saxer, U.P.; Mühlemann, H.R. Motivation und Aufklarung. Schweiz. Mon. Für Zahnmed. 1975, 85, 905–919. [Google Scholar]
- Predin, T.; Djuric, M.; Nikolic, N.; Mirnic, J.; Gusic, I.; Petrovic, D.J.; Milasin, J. Clinical and microbiological effects of quadrant versus full-mouth root planing—A randomized study. J. Dent. Sci. 2014, 9, 400–406. [Google Scholar] [CrossRef] [Green Version]
- Mirnic, J.; Djuric, M.; Predin, T.; Gusic, I.; Petrovic, D.; Andjelkovic, A.; Bajkin, B. Impact of the level of metabolic control on the non-surgical periodontal therapy outcomes in diabetes mellitus type 2 patients: Clinical effects. Srp. Arh. Celok. Lek. 2013, 141, 738–743. [Google Scholar] [CrossRef]
- Veljović, T.; Đurić, M.; Gušić, I.; Mirnić, J.; Čakić, S.; Maletin, A.; Brkić, S. The Influence of Periodontal Disease Treatment on 8-Hydroxy-Deoxyguanosine Concentrations in Saliva and Plasma of Chronic Periodontitis Patients. Acta Clin. Croat. 2020, 59, 615–622. [Google Scholar] [CrossRef]
- Armitage, G.C. Development of a classification system for periodontal diseases and conditions. Ann. Periodontol. 1999, 4, 1–6. [Google Scholar] [CrossRef]
- Tsai, C.C.; Chen, H.S.; Chen, S.L.; Ho, Y.P.; Ho, K.Y.; Wu, Y.M.; Hung, C.C. Lipid peroxidation: A possible role in the progression of the chronic periodontitis. J. Periodontal Res. 2005, 40, 378–384. [Google Scholar] [CrossRef] [PubMed]
- Takane, M.; Sugano, N.; Ezawa, T.; Uchiyama, T.; Ito, K. A marker of oxidative stress in saliva: Association with periodontally-involved teeth of a hopeless prognosis. J. Oral Sci. 2005, 47, 53–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takane, M.; Sugano, N.; Iwasaki, H.; Iwano, Y.; Shimizu, N.; Ito, K. New biomarker evidence of oxidative DNA damage in whole saliva from clinically healthy and periodontally diseased individuals. J. Periodontol. 2002, 73, 551–554. [Google Scholar] [CrossRef] [PubMed]
- Önder, C.; Kurgan, S.; Altıngöz, M.; Bağış, N.; Uyanık, M.; Serdar, M.A.; Kantarcı, A.; Günhan, M. Impact of non-surgical periodontal therapy on saliva and serum levels of markers of oxidative stress. Clin. Oral Investig. 2017, 2, 1961–1969. [Google Scholar] [CrossRef]
- Warad, S.B.; Pattanashetti, J.; Kalburgi, N.; Koregol, A.; Rao, S. Estimation of salivary malondialdehyde levels in smokeless tobacco chewers with chronic periodontitis-A cross sectional clinico biochemical study. Odovtos-Int. J. Dental. Sci. 2021, 23, 137–146. [Google Scholar] [CrossRef]
- Gutteridge, J.M.C. Lipid peroxidation and antioxidants as biomarkers of tissue damage. Clin. Chem. 1995, 41, 1819–1828. [Google Scholar] [CrossRef]
- Aziz, A.S.; Kalekar, M.G.; Benjamin, T.; Suryakar, A.N.; Prakashan, M.M.; Bijle, M.N.A. Effect of nonsurgical periodontal therapy on some oxidative stress markers in patients with chronic periodontitis: A biochemical study. World J. Dent. 2013, 4, 17–23. [Google Scholar] [CrossRef]
- Wei, D.; Zhang, X.L.; Wang, Y.Z.; Yang, C.X.; Chen, G. Lipid peroxidation levels, total oxidant status and superoxide dismutase in serum, saliva and gingival crevicular fluid inchronic periodontitis patients before and after periodontal therapy. Aust. Dent. J. 2010, 55, 70–78. [Google Scholar] [CrossRef]
- Tripathi, V.; Singh, S.T.; Sharma, V.; Verma, A.; Singh, C.D.; Gill, J.S. Assessment of lipid peroxidation levels and total antioxidant status in chronic and aggressive periodontitis patients: An in vivo study. J. Contemp. Dent. Pract. 2018, 19, 287–291. [Google Scholar] [CrossRef]
- Bastos, A.S.; Graves, D.T.; de Melo Loureiro, A.P.; Júnior, C.R.; Abdalla, D.S.P.; Faulin, T.E.S.; Câmara, N.O.; Andriankaja, O.M.; Orrico, S.R.P. Lipid peroxidation is associated with the severity of periodontal disease and local inflammatory markers in patients with type 2 diabetes. J. Clin. Endocr. Metab. 2012, 97, 1353–1362. [Google Scholar] [CrossRef] [Green Version]
- Ambati, M.; Rani, K.R.; Reddy, P.V.; Suryaprasanna, J.; Dasari, R.; Gireddy, H. Evaluation of oxidative stress in chronic periodontitis patients following systemic antioxidant supplementation: A clinical and biochemical study. J. Nat. Sci. Biol. Med. 2017, 8, 99–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naresh, K.C.; Subramaniam, M.R.; Prashanth, R.S.; Ranganath, V.; Abhilasha, S.P.; Anu, A.J. Salivary antioxidant enzymes and lipid peroxidation product malondialdehyde and sialic acid levels among smokers and non-smokers with chronic periodontitis—A clinico-biochemical study. J. Fam. Med. Prim. Care 2019, 8, 2960–2964. [Google Scholar] [CrossRef]
- Guentsch, A.; Preshaw, P.M.; Bremer, S.S.; Klinger, G.; Glockmann, E.; Sigusch, B.W. Lipid peroxidation and antioxidant activity in saliva of periodontitis patients: Effect of smoking and periodontal treatment. Clin. Oral Investig. 2008, 12, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Garg, N.; Singh, R.; Dixit, J.; Jain, A.; Tewari, V. Levels of lipid peroxides and antioxidants in smokers and nonsmokers. J. Periodontal Res. 2006, 41, 405–410. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group A (n = 30) | Group B (n = 20) | p-Value | |
|---|---|---|---|
| Gender, n (%) Male Female | 10 (33.3%) 20 (66.7%) | 9 (45%) 11 (55%) | 0.553 |
| Age in years (mean ± SD) | 48.70 ± 9.68 | 46.25 ± 9.25 | 0.472 |
| Number of teeth (mean ± SD) | 22.54 ± 2.14 | 25.34 ± 3.94 | 0.487 |
| Smoking, n (%) Yes No | 10 (33.3%) 20 (66.7%) | 7 (35%) 13 (65%) | 1.000 |
| Group A Baseline | Group A Three Months after Therapy | Group B | |
|---|---|---|---|
| PI | 1.40 ± 0.43 (0.83−1.97) | 0.35 ± 0.22 (0.08−1.12) a | 0.32 ± 0.28 (0.04−1.01) b |
| GI | 1.79 ± 0.64 (1.08−2.79) | 0.25 ± 0.33 (0.02−1.31) a | 0.19 ± 0.37 (0.00−0.50) b |
| PBI | 1.57 ± 0.81 (0.64−3.47) | 0.71 ± 0.43 (0.08−1.73) a | 0.28 ± 0.39 (0.00−1.78) b,c |
| PD (mm) | 3.14 ± 0.56 (2.87−4.42) | 2.59 ± 0.45 (1.95−3.81) a | 1.45 ± 0.18 (1.13−1.71) b,c |
| CAL (mm) | 2.70 ± 1.03 (1.76−5.50) | 2.19 ± 0.81 (0.59−4.08) a | 0.43 ± 0.56 (0.00−1.09) b,c |
| MDA-saliva (pmol/μL) | 2.99 ± 1.21 (1.11−4.80) | 2.14 ± 0.95 (1.11−4.80) a | 1.33 ± 0.92 (0.23−3.70) b,c |
| MDA-plasma (pmol/μL) | 0.50 ± 0.13 (0.29−0.70) | 0.47 ± 0.11 (0.29−0.70) | 0.40 ± 0.13 (0.13−0.62) b |
| GI Moderate (n = 14) | GI Severe (n = 16) | |
|---|---|---|
| PI—baseline | 1.08 ± 0.27 | 1.76 ± 0.11 a |
| PI—3 mo after therapy | 0.31 ± 0.10 b | 0.67 ± 0.35 b |
| GI—baseline | 1.37 ± 0.26 | 2.28 ± 0.21 a |
| GI—3 mo after therapy | 0.41 ± 0.20 b | 0.68 ± 0.52 b |
| PBI—baseline | 1.89 ± 0.39 | 2.01 ± 0.77 a |
| PBI—3 mo after therapy | 0.56 ± 0.27 b | 0.88 ± 0.53 b |
| PD (mm)—baseline | 2.88 ± 0.40 | 3.30 ± 0.57 a |
| PD (mm)—3 mo after therapy | 2.40 ± 0.31 b | 2.81 ± 0.49 b |
| CAL (mm)—baseline | 2.48 ± 0.78 | 2.96 ± 1.32 |
| CAL (mm)—3 mo after therapy | 1.69 ± 0.73 b | 1.91 ± 1.03 b |
| MDA-saliva (pmol/μL)—baseline | 2.42 ± 1.10 | 3.62 ± 1.22 a |
| MDA-saliva (pmol/μL)—3 mo after therapy | 1.83 ± 0.73 b | 2.50 ± 1.07 b |
| MDA-plasma (pmol/μL)—baseline | 0.45 ± 0.12 | 0.55 ± 0.13 a |
| MDA-plasma (pmol/μL)—3 mo after therapy | 0.43 ± 0.12 | 0.51 ± 0.09 |
| PD ≥ 5 mm < 20% (n = 10) | PD ≥ 5 mm ≥ 20% (n = 20) | |
|---|---|---|
| PI—baseline | 1.24 ± 0.32 | 1.49 ± 0.43 |
| PI—3 mo after therapy | 0.37 ± 0.23 b | 0.54 ± 0.33 b |
| GI—baseline | 1.55 ± 0.54 | 1.93 ± 0.45 |
| GI—3 mo after therapy | 0.48 ± 0.34 b | 0.59 ± 0.44 b |
| PBI—baseline | 1.41 ± 0.74 | 1.67 ± 0.71 |
| PBI—3 mo after therapy | 0.59 ± 0.40 b | 0.78 ± 0.45 b |
| PD (mm)—baseline | 2.58 ± 0.21 | 3.46 ± 0.41 a |
| PD (mm)—3 mo after therapy | 2.21 ± 0.21 b | 2.81 ± 0.40 b |
| CAL (mm)—baseline | 2.22 ± 0.91 | 2.99 ± 1.01 a |
| CAL (mm)—3 mo after therapy | 1.45 ± 0.75 b | 1.98 ± 0.90 b |
| MDA-saliva (pmol/μL)—baseline | 2.62 ± 1.11 | 3.21 ± 1.23 |
| MDA-saliva (pmol/μL)—3 mo after therapy | 2.09 ± 0.88 b | 2.15 ± 1.03 b |
| MDA-plasma (pmol/μL)—baseline | 0.44 ± 0.12 | 0.53 ± 0.12 |
| MDA-plasma (pmol/μL)—3 mo after therapy | 0.42 ± 0.12 | 0.45 ± 0.11 b |
| CAL < 3 mm (n = 15) | CAL ≥ 3 mm (n = 15) | |
|---|---|---|
| PI—baseline | 1.22 ± 0.37 | 1.58 ± 0.36 a |
| PI—3 mo after therapy | 0.43 ± 0.28 b | 0.53 ± 0.33 b |
| GI—baseline | 1.65 ± 0.50 | 1,94 ± 0.43 |
| GI—3 mo after therapy | 0.49 ± 0.34 b | 0.60 ± 0.46 b |
| PBI—baseline | 1.38 ± 0.78 | 1.77 ± 0.62 |
| PBI—3 mo after therapy | 0.53 ± 0.33 b | 0.88 ± 0.46 b |
| PD (mm)—baseline | 3.05 ± 0.61 | 3.23 ± 0.50 |
| PD (mm)—3 mo after therapy | 2.42 ± 0.31 b | 2.75 ± 0.52 b |
| CAL (mm)—baseline | 1.99 ± 0.72 | 3.42 ± 0.77 a |
| CAL (mm)—3 mo after therapy | 1.35 ± 0.69 b | 2.23 ± 0.83 b |
| MDA-saliva (pmol/μL)—baseline | 2.80 ± 0.91 | 3.18 ± 1.45 |
| MDA-saliva (pmol/μL)—3 mo after therapy | 2.09 ± 0.74 b | 2.18 ± 1.15 b |
| MDA-plasma (pmol/μL)—baseline | 0.46 ± 0.13 | 0.54 ± 0.13 |
| MDA-plasma (pmol/μL)—3 mo after therapy | 0.44 ± 0.08 | 0.49 ± 0.14 |
| Parameter | MDA-Plasma | MDA-Saliva | ||
|---|---|---|---|---|
| Variable | Statistics | p-Value | Statistics | p-Value |
| Group | 2.593 a | 0.013 | 5.226 a | <0.001 |
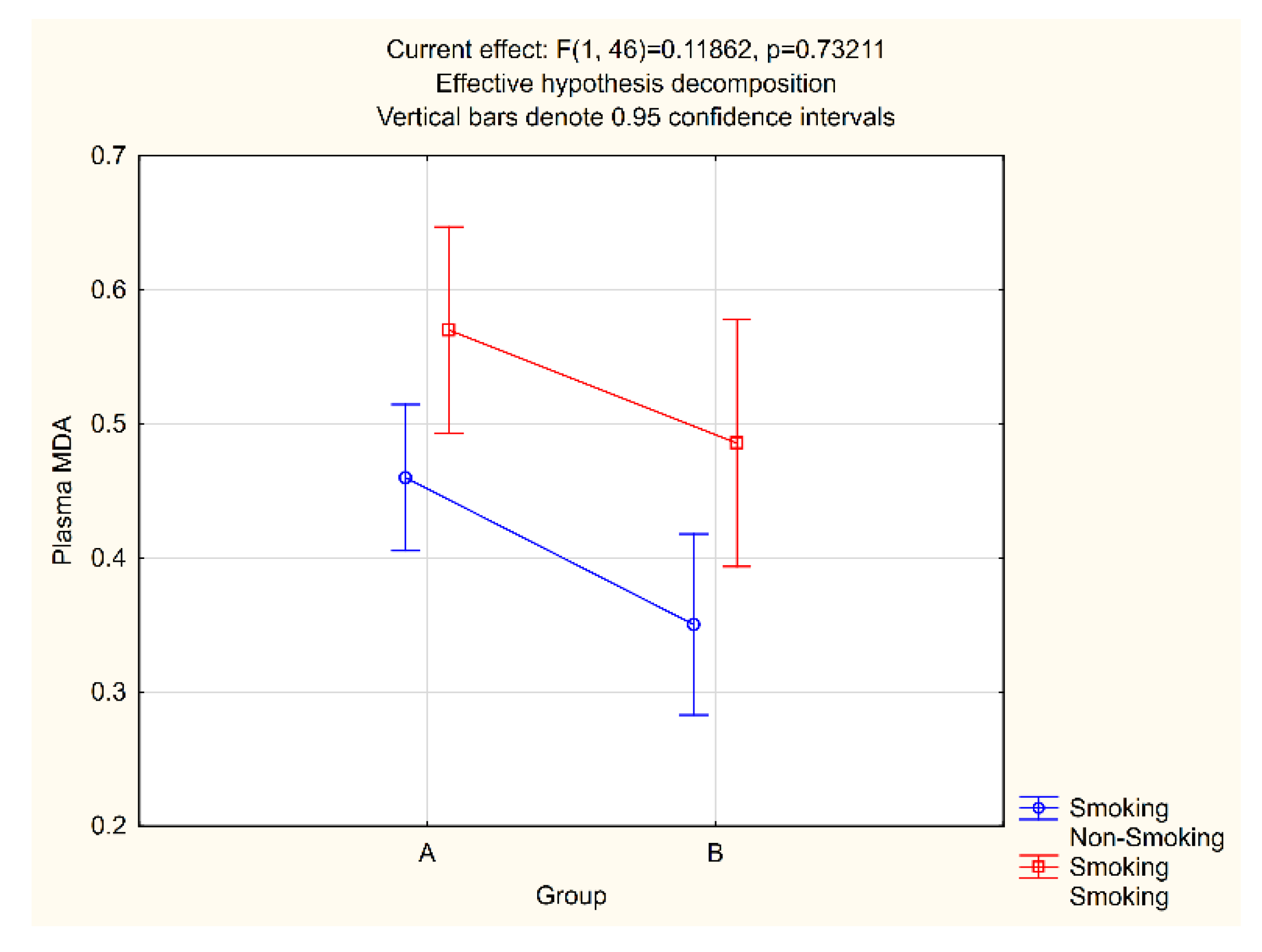
| Smoking | −3.077 a | 0.003 | −4.543 a | <0.001 |
| Gender | 0.073 a | 0.942 | −1.249 a | 0.218 |
| Age | 0.155 b | 0.283 | 0.014 b | 0.926 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Veljovic, T.; Djuric, M.; Mirnic, J.; Gusic, I.; Maletin, A.; Ramic, B.; Neskovic, I.; Vukoje, K.; Brkic, S. Lipid Peroxidation Levels in Saliva and Plasma of Patients Suffering from Periodontitis. J. Clin. Med. 2022, 11, 3617. https://doi.org/10.3390/jcm11133617
Veljovic T, Djuric M, Mirnic J, Gusic I, Maletin A, Ramic B, Neskovic I, Vukoje K, Brkic S. Lipid Peroxidation Levels in Saliva and Plasma of Patients Suffering from Periodontitis. Journal of Clinical Medicine. 2022; 11(13):3617. https://doi.org/10.3390/jcm11133617
Chicago/Turabian StyleVeljovic, Tanja, Milanko Djuric, Jelena Mirnic, Ivana Gusic, Aleksandra Maletin, Bojana Ramic, Isidora Neskovic, Karolina Vukoje, and Snezana Brkic. 2022. "Lipid Peroxidation Levels in Saliva and Plasma of Patients Suffering from Periodontitis" Journal of Clinical Medicine 11, no. 13: 3617. https://doi.org/10.3390/jcm11133617
APA StyleVeljovic, T., Djuric, M., Mirnic, J., Gusic, I., Maletin, A., Ramic, B., Neskovic, I., Vukoje, K., & Brkic, S. (2022). Lipid Peroxidation Levels in Saliva and Plasma of Patients Suffering from Periodontitis. Journal of Clinical Medicine, 11(13), 3617. https://doi.org/10.3390/jcm11133617