
Comparison of Clinical Outcomes after Non-ST-Segment and ST-Segment Elevation Myocardial Infarction in Diabetic and Nondiabetic Populations

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
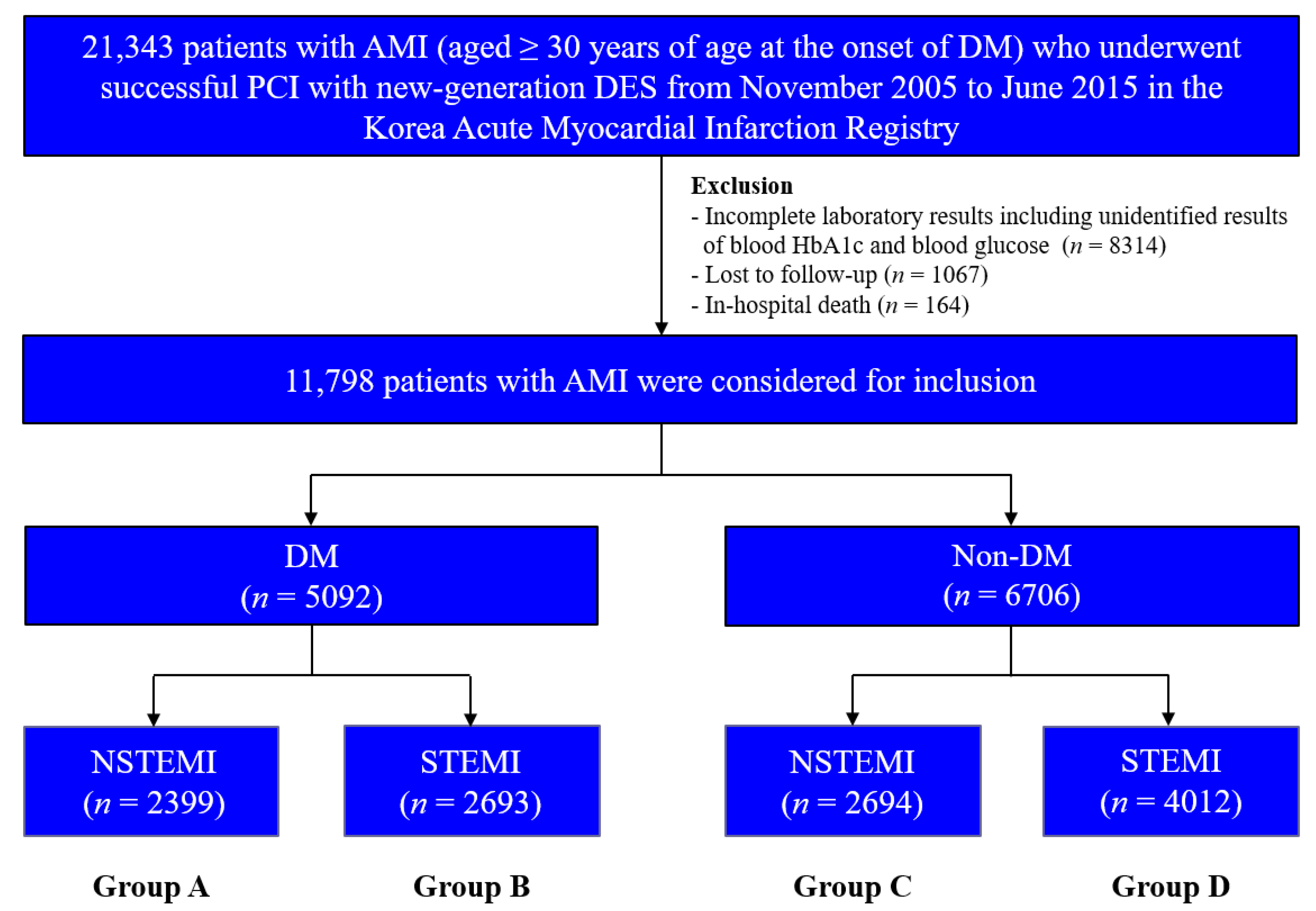
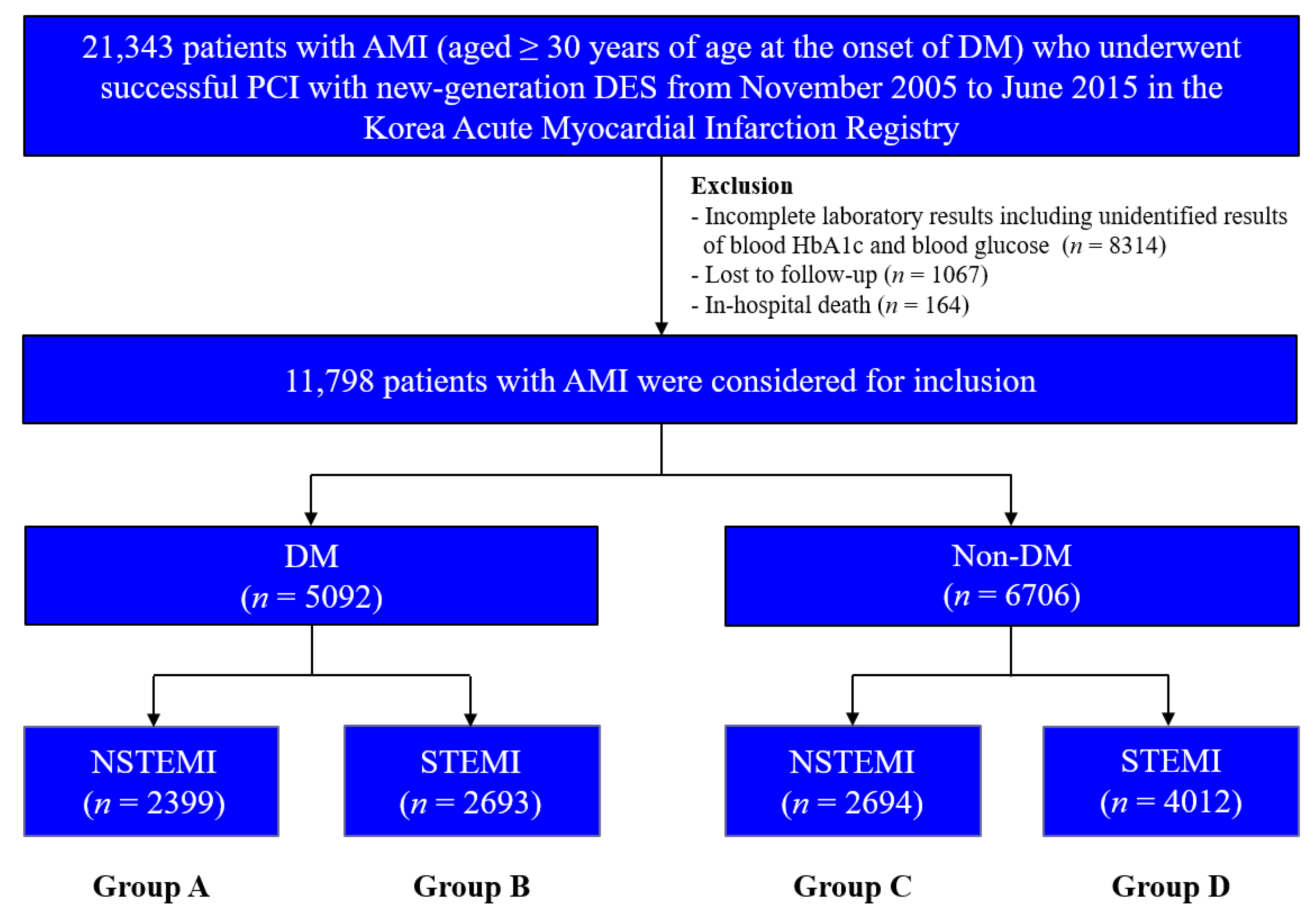
2.1. Study Population
2.2. Percutaneous Coronary Intervention and Medical Treatment
2.3. Study Definitions and Clinical Outcomes
2.4. Statistical Analyses
3. Results
3.1. Baseline Characteristics
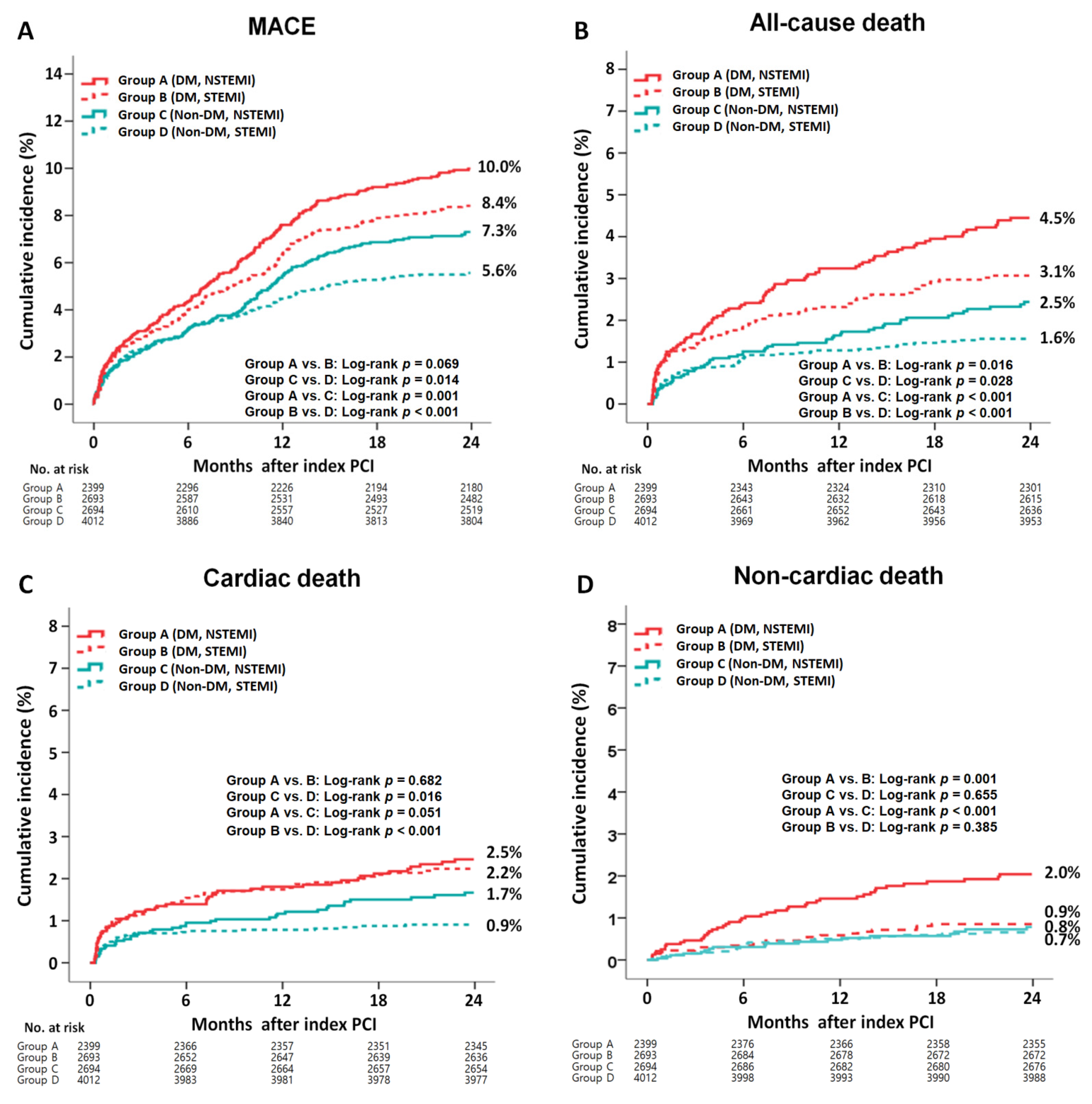
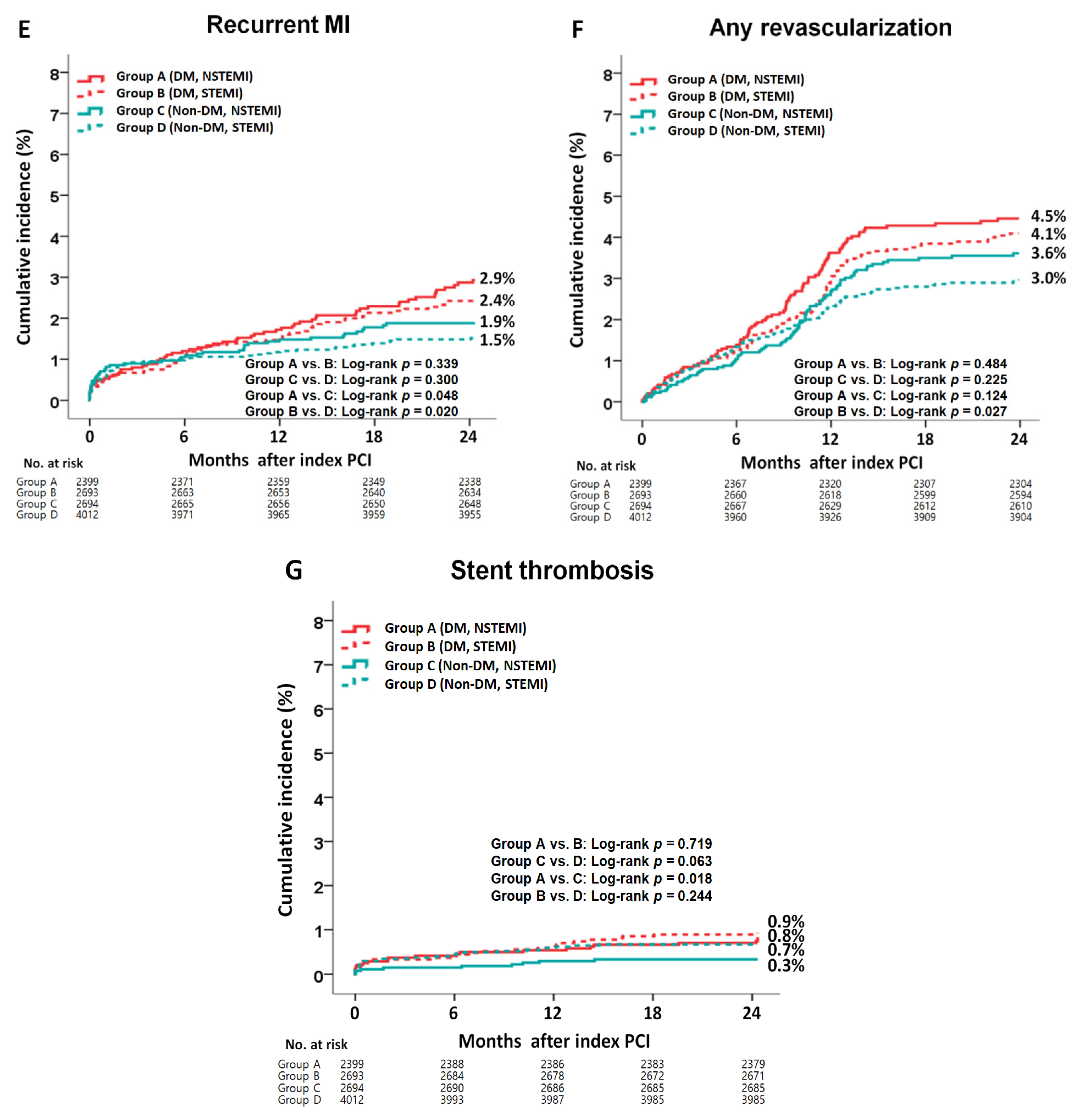
3.2. Clinical Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Milazzo, V.; Cosentino, N.; Genovese, S.; Campodonico, J.; Mazza, M.; de Metrio, M.; Marenzi, G. Diabetes Mellitus and Acute Myocardial Infarction: Impact on Short and Long-Term Mortality. Adv. Exp. Med. Biol. 2021, 1307, 153–169. [Google Scholar] [PubMed]
- Ertelt, K.; Brener, S.J.; Mehran, R.; Ben-Yehuda, O.; McAndrew, T.; Stone, G.W. Comparison of Outcomes and Prognosis of Patients With Versus Without Newly Diagnosed Diabetes Mellitus After Primary Percutaneous Coronary Intervention for ST-Elevation Myocardial Infarction (the HORIZONS-AMI Study). Am. J. Cardiol. 2017, 119, 1917–1923. [Google Scholar] [CrossRef] [PubMed]
- Libby, P. Mechanisms of acute coronary syndromes and their implications for therapy. N. Engl. J. Med. 2013, 368, 2004–2013. [Google Scholar] [CrossRef]
- Bassand, J.P.; Hamm, C.W.; Ardissino, D.; Boersma, E.; Budaj, A.; Fernández-Avilés, F.; Fox, K.A.; Hasdai, D.; Ohman, E.M.; Wallentin, L.; et al. Guidelines for the diagnosis and treatment of non-ST-segment elevation acute coronary syndromes. Eur. Heart J. 2007, 28, 1598–1660. [Google Scholar] [PubMed]
- Basalay, M.V.; Yellon, D.M.; Davidson, S.M. Targeting myocardial ischaemic injury in the absence of reperfusion. Basic Res. Cardiol. 2020, 115, 63. [Google Scholar] [CrossRef]
- Basir, M.B.; Schreiber, T.; Dixon, S.; Alaswad, K.; Patel, K.; Almany, S.; Khandelwal, A.; Hanson, I.; George, A.; Ashbrook, M.; et al. Feasibility of early mechanical circulatory support in acute myocardial infarction complicated by cardiogenic shock: The Detroit cardiogenic shock initiative. Catheter. Cardiovasc. Interv. 2018, 91, 454–461. [Google Scholar] [CrossRef]
- Puymirat, E.; Simon, T.; Cayla, G.; Cottin, Y.; Elbaz, M.; Coste, P.; Lemesle, G.; Motreff, P.; Popovic, B.; Khalife, K.; et al. Acute Myocardial Infarction: Changes in Patient Characteristics, Management, and 6-Month Outcomes Over a Period of 20 Years in the FAST-MI Program (French Registry of Acute ST-Elevation or Non-ST-Elevation Myocardial Infarction) 1995 to 2015. Circulation 2017, 136, 1908–1919. [Google Scholar] [CrossRef]
- Fox, C.S.; Muntner, P.; Chen, A.Y.; Alexander, K.P.; Roe, M.T.; Cannon, C.P.; Saucedo, J.F.; Kontos, M.C.; Wiviott, S.D. Use of evidence-based therapies in short-term outcomes of ST-segment elevation myocardial infarction and non-ST-segment elevation myocardial infarction in patients with chronic kidney disease: A report from the National Cardiovascular Data Acute Coronary Treatment and Intervention Outcomes Network registry. Circulation 2010, 121, 357–365. [Google Scholar]
- Goldberg, R.J.; Currie, K.; White, K.; Brieger, D.; Steg, P.G.; Goodman, S.G.; Dabbous, O.; Fox, K.A.; Gore, J.M. Six-month outcomes in a multinational registry of patients hospitalized with an acute coronary syndrome (the Global Registry of Acute Coronary Events [GRACE]). Am. J. Cardiol. 2004, 93, 288–293. [Google Scholar] [CrossRef]
- Chan, M.Y.; Sun, J.L.; Newby, L.K.; Shaw, L.K.; Lin, M.; Peterson, E.D.; Califf, R.M.; Kong, D.F.; Roe, M.T. Long-term mortality of patients undergoing cardiac catheterization for ST-elevation and non-ST-elevation myocardial infarction. Circulation 2009, 119, 3110–3117. [Google Scholar] [CrossRef]
- Polonski, L.; Gasior, M.; Gierlotka, M.; Osadnik, T.; Kalarus, Z.; Trusz-Gluza, M.; Zembala, M.; Wilczek, K.; Lekston, A.; Zdrojewski, T.; et al. A comparison of ST elevation versus non-ST elevation myocardial infarction outcomes in a large registry database: Are non-ST myocardial infarctions associated with worse long-term prognoses? Int. J. Cardiol. 2011, 152, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Hao, Y.; Lu, Q.; Li, T.; Yang, G.; Hu, P.; Ma, A. Admission hyperglycemia and adverse outcomes in diabetic and non-diabetic patients with non-ST-elevation myocardial infarction undergoing percutaneous coronary intervention. BMC Cardiovasc. Disord. 2017, 17, 6. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Li, X.; Zhang, Y.; Zhang, L.; Wu, Q.; Bai, Z.; Si, J.; Zuo, X.; Shi, N.; Li, J.; et al. Impact of glycemic control status on patients with ST-segment elevation myocardial infarction undergoing percutaneous coronary intervention. BMC Cardiovasc. Disord. 2020, 20, 36. [Google Scholar] [CrossRef]
- Kim, Y.H.; Her, A.Y.; Jeong, M.H.; Kim, B.K.; Hong, S.J.; Kim, S.; Ahn, C.M.; Kim, J.S.; Ko, Y.G.; Choi, D.; et al. Effects of stent generation on clinical outcomes after acute myocardial infarction compared between prediabetes and diabetes patients. Sci. Rep. 2021, 11, 9364. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.A.; Cho, S.J.; Jeong, M.H.; Kim, Y.J.; Kim, C.J.; Cho, M.C.; Kim, H.S.; Ahn, Y.; Koh, G.; Lee, J.M.; et al. Hypoglycemia at admission in patients with acute myocardial infarction predicts a higher 30-day mortality in patients with poorly controlled type 2 diabetes than in well-controlled patients. Diabetes Care 2014, 37, 2366–2373. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Chae, S.C.; Oh, D.J.; Kim, H.S.; Kim, Y.J.; Ahn, Y.; Cho, M.C.; Kim, C.J.; Yoon, J.H.; Jeong, M.H.; et al. Multicenter Cohort Study of Acute Myocardial Infarction in Korea—Interim Analysis of the Korea Acute Myocardial Infarction Registry-National Institutes of Health Registry. Circ. J. 2016, 80, 1427–1436. [Google Scholar] [CrossRef] [PubMed]
- Grech, E.D. ABC of interventional cardiology: Percutaneous coronary intervention. II: The procedure. BMJ 2003, 326, 1137–1140. [Google Scholar] [CrossRef]
- Chen, K.Y.; Rha, S.W.; Li, Y.J.; Poddar, K.L.; Jin, Z.; Minami, Y.; Wang, L.; Kim, E.J.; Park, C.G.; Seo, H.S.; et al. Triple versus dual antiplatelet therapy in patients with acute ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention. Circulation 2009, 119, 3207–3214. [Google Scholar] [CrossRef]
- Lee, S.W.; Park, S.W.; Hong, M.K.; Kim, Y.H.; Lee, B.K.; Song, J.M.; Han, K.H.; Lee, C.W.; Kang, D.H.; Song, J.K.; et al. Triple versus dual antiplatelet therapy after coronary stenting: Impact on stent thrombosis. J. Am. Coll. Cariol. 2005, 46, 1833–1837. [Google Scholar] [CrossRef]
- American Diabetes Association. Standards of medical care in diabetes–2010. Diabetes Care 2010, 33 (Suppl. 1), S11–S61. [Google Scholar] [CrossRef]
- Amsterdam, E.A.; Wenger, N.K.; Brindis, R.G.; Casey, D.E., Jr.; Ganiats, T.G.; Holmes, D.R., Jr.; Jaffe, A.S.; Jneid, H.; Kelly, R.F.; Kontos, M.C.; et al. 2014 AHA/ACC Guideline for the Management of Patients with Non-ST-Elevation Acute Coronary Syndromes: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cariol. 2014, 64, e139–e228. [Google Scholar] [CrossRef] [Green Version]
- Roffi, M.; Patrono, C.; Collet, J.P.; Mueller, C.; Valgimigli, M.; Andreotti, F.; Bax, J.J.; Borger, M.A.; Brotons, C.; Chew, D.P.; et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2016, 37, 267–315. [Google Scholar] [PubMed]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [PubMed]
- O’Gara, P.T.; Kushner, F.G.; Ascheim, D.D.; Casey, D.E., Jr.; Chung, M.K.; de Lemos, J.A.; Ettinger, S.M.; Fang, J.C.; Fesmire, F.M.; Franklin, B.A.; et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation 2013, 127, e362–e425. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.M.; Rhee, T.M.; Hahn, J.Y.; Kim, H.K.; Park, J.; Hwang, D.; Choi, K.H.; Kim, J.; Park, T.K.; Yang, J.H.; et al. Multivessel Percutaneous Coronary Intervention in Patients With ST-Segment Elevation Myocardial Infarction With Cardiogenic Shock. J. Am. Coll. Cariol. 2018, 71, 844–856. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.H.; Her, A.Y.; Jeong, M.H.; Kim, B.K.; Lee, S.Y.; Hong, S.J.; Shin, D.H.; Kim, J.S.; Ko, Y.G.; Choi, D.; et al. Impact of renin-angiotensin system inhibitors on long-term clinical outcomes in patients with acute myocardial infarction treated with successful percutaneous coronary intervention with drug-eluting stents: Comparison between STEMI and NSTEMI. Atherosclerosis 2019, 280, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Vatcheva, K.P.; Lee, M.; McCormick, J.B.; Rahbar, M.H. Multicollinearity in Regression Analyses Conducted in Epidemiologic Studies. Epidemiology 2016, 6, e120. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H. Multicollinearity and misleading statistical results. Korean J. Anesthesiol. 2019, 72, 558–569. [Google Scholar] [CrossRef]
- Kalantari, S.; Khalili, D.; Asgari, S.; Fahimfar, N.; Hadaegh, F.; Tohidi, M.; Azizi, F. Predictors of early adulthood hypertension during adolescence: A population-based cohort study. BMC Public Health 2017, 17, 915. [Google Scholar] [CrossRef]
- Montalescot, G.; Dallongeville, J.; van Belle, E.; Rouanet, S.; Baulac, C.; Degrandsart, A.; Vicaut, E. STEMI and NSTEMI: Are they so different? 1 year outcomes in acute myocardial infarction as defined by the ESC/ACC definition (the OPERA registry). Eur. Heart J. 2007, 28, 1409–1417. [Google Scholar] [CrossRef]
- Marfella, R.; Nappo, F.; de Angelis, L.; Paolisso, G.; Tagliamonte, M.R.; Giugliano, D. Hemodynamic effects of acute hyperglycemia in type 2 diabetic patients. Diabetes Care 2000, 23, 658–663. [Google Scholar] [CrossRef] [PubMed]
- Odegaard, A.O.; Jacobs, D.R., Jr.; Sanchez, O.A.; Goff, D.C., Jr.; Reiner, A.P.; Gross, M.D. Oxidative stress, inflammation, endothelial dysfunction and incidence of type 2 diabetes. Cardiovasc. Diabetol. 2016, 15, 51. [Google Scholar] [CrossRef]
- Okura, N.; Ogawa, H.; Katoh, J.; Yamauchi, T.; Hagiwara, N. Long-term prognosis of patients with acute myocardial infarction in the era of acute revascularization (from the Heart Institute of Japan Acute Myocardial Infarction [HIJAMI] registry). Int. J. Cardiol. 2012, 159, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Bundhun, P.K.; Li, N.; Chen, M.H. Adverse cardiovascular outcomes between insulin-treated and non-insulin treated diabetic patients after percutaneous coronary intervention: A systematic review and meta-analysis. Cardiovasc. Diabetol. 2015, 14, 135. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.H.; Her, A.Y.; Jeong, M.H.; Kim, B.K.; Hong, S.J.; Lee, S.J.; Ahn, C.M.; Kim, J.S.; Ko, Y.G.; Choi, D.; et al. Two-year outcomes between ST-elevation and non-ST-elevation myocardial infarction in patients with chronic kidney disease undergoing newer-generation drug-eluting stent implantation. Catheter. Cardiovasc. Interv. 2022, 99, 1022–1037. [Google Scholar] [CrossRef]
- Nikolsky, E.; Mehran, R.; Dangas, G.D.; Xu, K.; Parvataneni, R.; Witzenbichler, B.; Guagliumi, G.; Kornowski, R.; Généreux, P.; Brener, S.J.; et al. Cerebrovascular events after a primary percutaneous coronary intervention strategy for acute ST-segment-elevation myocardial infarction: Analysis from the HORIZONS-AMI Trial. Circ. Cardiovasc. Interv. 2015, 8, e002283. [Google Scholar] [CrossRef]
- Spencer, F.A.; Gore, J.M.; Yarzebski, J.; Lessard, D.; Jackson, E.A.; Goldberg, R.J. Trends (1986 to 1999) in the incidence and outcomes of in-hospital stroke complicating acute myocardial infarction (The Worcester Heart Attack Study). Am. J. Cardiol. 2003, 92, 383–388. [Google Scholar] [CrossRef]
- Jernberg, T.; Hasvold, P.; Henriksson, M.; Hjelm, H.; Thuresson, M.; Janzon, M. Cardiovascular risk in post-myocardial infarction patients: Nationwide real world data demonstrate the importance of a long-term perspective. Eur. Heart J. 2015, 36, 1163–1170. [Google Scholar] [CrossRef]
- Kim, Y.H.; Her, A.Y.; Jeong, M.H.; Kim, B.K.; Hong, S.J.; Kim, S.; Ahn, C.M.; Kim, J.S.; Ko, Y.G.; Choi, D.; et al. Effects of prediabetes on long-term clinical outcomes of patients with acute myocardial infarction who underwent PCI using new-generation drug-eluting stents. Diabetes Res. Clin. Pract. 2020, 160, 107994. [Google Scholar] [CrossRef]
- Jensen, L.O.; Maeng, M.; Thayssen, P.; Tilsted, H.H.; Terkelsen, C.J.; Kaltoft, A.; Lassen, J.F.; Hansen, K.N.; Ravkilde, J.; Christiansen, E.H.; et al. Influence of diabetes mellitus on clinical outcomes following primary percutaneous coronary intervention in patients with ST-segment elevation myocardial infarction. Am. J. Cardiol. 2012, 109, 629–635. [Google Scholar] [CrossRef] [PubMed]
- Iglesias, J.F.; Heg, D.; Roffi, M.; Tüller, D.; Lanz, J.; Rigamonti, F.; Muller, O.; Moarof, I.; Cook, S.; Weilenmann, D.; et al. Five-Year Outcomes in Patients With Diabetes Mellitus Treated With Biodegradable Polymer Sirolimus-Eluting Stents Versus Durable Polymer Everolimus-Eluting Stents. J. Am. Heart Assoc. 2019, 8, e013607. [Google Scholar] [CrossRef]
- Kim, Y.H.; Her, A.Y.; Jeong, M.H.; Kim, B.K.; Hong, S.J.; Kim, S.; Ahn, C.M.; Kim, J.S.; Ko, Y.G.; Choi, D.; et al. Comparison of two-year clinical outcomes according to glycemic status and renal function in patients with acute myocardial infarction following implantation of new-generation drug-eluting stents. J. Diabetes Complicat. 2021, 35, 108019. [Google Scholar] [CrossRef] [PubMed]
- Hassan, S.; Ali, M.N.; Ghafoor, B. Evolutionary perspective of drug eluting stents: From thick polymer to polymer free approach. J. Cardiothorac. Surg. 2022, 17, 65. [Google Scholar] [CrossRef]
- Roe, M.T.; Parsons, L.S.; Pollack, C.V., Jr.; Canto, J.G.; Barron, H.V.; Every, N.R.; Rogers, W.J.; Peterson, E.D. Quality of care by classification of myocardial infarction: Treatment patterns for ST-segment elevation vs non-ST-segment elevation myocardial infarction. Arch. Intern. Med. 2005, 165, 1630–1636. [Google Scholar] [CrossRef] [PubMed]
- McKee, A.; Al-Khazaali, A.; Albert, S.G. Glucagon-like Peptide-1 Receptor Agonists versus Sodium-Glucose Cotransporter Inhibitors for Treatment of T2DM. J. Endocr. Soc. 2020, 4, bvaa037. [Google Scholar] [CrossRef] [PubMed]
- Htoo, P.T.; Buse, J.; Cavender, M.; Wang, T.; Pate, V.; Edwards, J.; Stürmer, T. Cardiovascular Effectiveness of Sodium-Glucose Cotransporter 2 Inhibitors and Glucagon-Like Peptide-1 Receptor Agonists in Older Patients in Routine Clinical Care With or Without History of Atherosclerotic Cardiovascular Diseases or Heart Failure. J. Am. Heart Assoc. 2022, 11, e022376. [Google Scholar] [CrossRef]
- Das, S.R.; Everett, B.M.; Birtcher, K.K.; Brown, J.M.; Januzzi, J.L., Jr.; Kalyani, R.R.; Kosiborod, M.; Magwire, M.; Morris, P.B.; Neumiller, J.J.; et al. 2020 Expert Consensus Decision Pathway on Novel Therapies for Cardiovascular Risk Reduction in Patients With Type 2 Diabetes: A Report of the American College of Cardiology Solution Set Oversight Committee. J. Am. Coll. Cardiol. 2020, 76, 1117–1145. [Google Scholar] [CrossRef]
- Asrih, M.; Gariani, K. Impact of SGLT Inhibitors on Multiple Organ Defects in Diabetes. Curr. Diabetes Rev. 2020, 16, 411–418. [Google Scholar] [CrossRef]
- Harding, J.L.; Wander, P.L.; Zhang, X.; Li, X.; Karuranga, S.; Chen, H.; Sun, H.; Xie, Y.; Oram, R.A.; Magliano, D.J.; et al. The Incidence of Adult-Onset Type 1 Diabetes: A Systematic Review From 32 Countries and Regions. Diabetes Care 2022, 45, 994–1006. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variables | Overall (n = 11,798) | DM (n = 5092) | Non-DM (n = 6706) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| NSTEMI (n = 5093) | STEMI (n = 6705) | p Value | NSTEMI (n = 2399) | STEMI (n = 2693) | p Value | NSTEMI (n = 2694) | STEMI (n = 4012) | p Value | |
| Male, n (%) | 3626 (71.2) | 5184 (77.3) | <0.001 | 1585 (66.1) | 1996 (74.1) | <0.001 | 2041 (75.8) | 3188 (79.5) | 0.001 |
| Age, years | 64.4 ± 12.0 | 62.1 ± 12.5 | <0.001 | 65.5 ± 11.3 | 63.0 ± 11.9 | <0.001 | 63.5 ± 12.6 | 61.4 ± 13.0 | <0.001 |
| LVEF, % | 54.1 ± 11.1 | 50.7 ± 11.0 | <0.001 | 52.6 ± 11.9 | 50.0 ± 11.1 | <0.001 | 55.4 ± 10.2 | 51.2 ± 10.8 | <0.001 |
| BMI, kg/m2 | 24.1 ± 3.2 | 24.2 ± 3.1 | 0.076 | 24.3 ± 3.1 | 24.5 ± 3.1 | 0.017 | 24.0 ± 3.2 | 24.0 ± 3.1 | 0.404 |
| SBP, mmHg | 134.8 ± 26.6 | 127.7 ± 27.9 | <0.001 | 134.5 ± 26.8 | 128.1 ± 28.6 | <0.001 | 135.0 ± 26.5 | 127.5 ± 27.5 | <0.001 |
| DBP, mmHg | 80.7 ± 15.2 | 78.4 ± 16.8 | <0.001 | 79.8 ± 15.1 | 77.8 ± 17.0 | <0.001 | 81.5 ± 15.7 | 78.7 ± 16.7 | <0.001 |
| Cardiogenic shock, n (%) | 113 (2.2) | 395 (5.9) | <0.010 | 61 (2.5) | 176 (6.5) | <0.001 | 52 (1.9) | 219 (5.5) | <0.001 |
| Killip class I/II, n (%) | 4440 (87.2) | 5613 (83.7) | <0.001 | 2013 (83.9) | 2211 (82.1) | 0.087 | 2427 (90.1) | 3402 (84.8) | <0.001 |
| CPR on admission, n (%) | 122 (2.4) | 374 (5.6) | <0.001 | 60 (2.5) | 128 (4.8) | <0.001 | 62 (2.3) | 246 (6.1) | <0.001 |
| Hypertension, n (%) | 2779 (54.6) | 3120 (46.5) | <0.001 | 1540 (64.2) | 1532 (56.9) | <0.001 | 1239 (46.0) | 1588 (39.6) | <0.001 |
| Dyslipidemia, n (%) | 661 (13.0) | 736 (11.0) | 0.001 | 375 (15.6) | 356 (13.2) | 0.014 | 286 (10.6) | 380 (9.5) | 0.134 |
| Previous MI, n (%) | 234 (4.6) | 196 (2.9) | <0.001 | 149 (6.2) | 98 (3.6) | <0.001 | 85 (3.2) | 98 (2.4) | 0.079 |
| Previous PCI, n (%) | 386 (7.6) | 297 (4.4) | <0.001 | 239 (10.0) | 154 (5.7) | <0.001 | 147 (5.5) | 143 (3.6) | <0.001 |
| Previous CABG, n (%) | 31 (0.6) | 20 (0.3) | 0.015 | 25 (1.0) | 14 (0.5) | 0.036 | 6 (0.2) | 6 (0.1) | 0.561 |
| Previous HF, n (%) | 72 (1.4) | 55 (0.8) | 0.002 | 50 (2.1) | 28 (1.0) | 0.003 | 22 (0.8) | 27 (0.7) | 0.498 |
| Previous CVA, n (%) | 387 (7.6) | 326 (4.9) | <0.001 | 224 (9.3) | 168 (6.2) | <0.001 | 163 (6.1) | 158 (3.9) | <0.001 |
| Current smokers, n (%) | 1922 (37.7) | 3194 (47.6) | <0.001 | 803 (33.5) | 1182 (43.9) | <0.001 | 1119 (41.5) | 2012 (50.1) | <0.001 |
| Peak CK-MB, mg/dL | 23 (7.0–82.9) | 124.0 (34.6–268.5) | <0.001 | 18.3 (6.0–63.4) | 102.4 (26.9–236.2) | <0.001 | 29.5 (8.7–103.1) | 140.5 (39.6–290.8) | <0.001 |
| Peak Troponin-I, ng/mL | 11.0 (2.2–47.8) | 46.8 (16.0–61.2) | <0.001 | 8.7 (1.7–42.0) | 48.1 (18.5–67.8) | <0.001 | 12.7 (2.6–47.8) | 47.8 (12.7–52.1) | <0.001 |
| Blood glucose, mg/dL | 171.2 ± 88.6 | 184.6 ± 83.3 | <0.001 | 216.5 ± 103.1 | 234.3 ± 95.9 | <0.001 | 130.6 ± 43.4 | 150.8 ± 50.8 | <0.001 |
| Hemoglobin A1c, % | 6.64 ± 2.08 | 6.57 ± 2.22 | 0.074 | 7.72 ± 2.60 | 7.90 ± 3.00 | 0.022 | 5.67 ± 0.45 | 5.67 ± 0.45 | 0.800 |
| NT-ProBNP, pg/mL | 658.0 (160.0–2740.5) | 265.0 (59.0–1443.0) | <0.001 | 1325.5 (301.0–5417.0) | 453.5 (89.0–2621.8) | <0.001 | 484.0 (130.5–1857.5) | 225.0 (53.0–1195.0) | <0.001 |
| Hs-CRP, mg/dL | 10.1 ± 46.8 | 9.4 ± 37.9 | 0.427 | 10.7 ± 43.9 | 11.3 ± 43.1 | 0.596 | 9.5 ± 49.2 | 8.2 ± 33.9 | 0.210 |
| Serum creatinine, mg/dL | 1.17 ± 1.70 | 1.06 ± 1.20 | <0.001 | 1.34 ± 2.21 | 1.10 ± 0.86 | <0.001 | 1.03 ± 1.06 | 1.03 ± 1.39 | 0.822 |
| eGFR, mL/min/1.73 m2 | 88.3 ± 45.3 | 87.3 ± 37.2 | 0.215 | 83.1 ± 46.0 | 85.3 ± 41.3 | 0.074 | 92.8 ± 44.1 | 88.6 ± 34.1 | <0.001 |
| Total cholesterol, mg/dL | 181.8 ± 46.3 | 184.0 ± 43.7 | 0.013 | 177.3 ± 49.8 | 180.5 ± 45.8 | 0.015 | 186.0 ± 42.4 | 186.3 ± 42.1 | 0.795 |
| Triglyceride, mg/L | 136.3 ± 117.5 | 137.9 ± 109.8 | 0.445 | 150.2 ± 136.2 | 151.0 ± 124.0 | 0.814 | 123.9 ± 96.3 | 129.0 ± 98.2 | 0.032 |
| HDL cholesterol, mg/L | 43.0 ± 14.1 | 43.3 ± 15.4 | 0.291 | 41.6 ± 13.5 | 42.0 ± 14.4 | 0.359 | 44.2 ± 14.4 | 44.1 ± 16.0 | 0.869 |
| LDL cholesterol, mg/L | 114.7 ± 41.7 | 115.9 ± 39.5 | 0.096 | 109.3 ± 38.8 | 111.8 ± 37.2 | 0.018 | 119.5 ± 43.6 | 118.7 ± 40.8 | 0.467 |
| Diabetes management | |||||||||
| Diet, n (%) | 166 (3.3) | 244 (3.6) | 0.287 | 166 (6.9) | 244 (9.0) | 0.005 | |||
| Oral agent, n (%) | 1492 (29.3) | 1681 (25.1) | <0.001 | 1492 (62.2) | 1681 (62.4) | 0.885 | |||
| Insulin, n (%) | 160 (3.1) | 128 (1.9) | <0.001 | 160 (6.7) | 128 (4.8) | 0.003 | |||
| Untreated, n (%) | 581 (11.4) | 640 (9.5) | 0.001 | 581 (24.2) | 640 (23.8) | 0.718 | |||
| Discharge medications | |||||||||
| Aspirin, n (%) | 4940 (97.2) | 6484 (96.7) | 0.370 | 2326 (97.0) | 2596 (96.4) | 0.268 | 2614 (97.0) | 3888 (96.9) | 0.777 |
| Clopidogrel, n (%) | 4325 (84.9) | 5780 (86.2) | 0.049 | 2115 (88.2) | 2335 (86.7) | 0.118 | 2210 (82.0) | 3445 (85.9) | <0.001 |
| Ticagrelor, n (%) | 484 (9.5) | 607 (9.1) | 0.403 | 183 (7.6) | 219 (8.1) | 0.532 | 301 (11.2) | 388 (9.7) | 0.047 |
| Prasugrel, n (%) | 236 (4.6) | 366 (5.5) | 0.047 | 101 (4.2) | 139 (5.2) | 0.112 | 135 (4.4) | 227 (5.7) | 0.270 |
| Cilostazol, n (%) | 887 (17.4) | 1242 (18.5) | 0.122 | 462 (19.3) | 538 (20.0) | 0.525 | 425 (15.8) | 704 (17.5) | 0.058 |
| ACEIs, n (%) | 2581 (50.7) | 3849 (57.4) | <0.001 | 1133 (47.2) | 1455 (54.0) | <0.001 | 1448 (53.7) | 2394 (59.7) | <0.001 |
| ARBs, n (%) | 1558 (30.6) | 1576 (23.5) | <0.001 | 828 (34.5) | 712 (26.4) | <0.001 | 730 (27.1) | 864 (21.5) | <0.001 |
| BBs, n (%) | 4219 (82.8) | 5641 (84.1) | 0.061 | 2007 (83.7) | 2266 (84.1) | 0.639 | 2212 (82.1) | 3375 (84.1) | 0.030 |
| CCBs, n (%) | 501 (9.8) | 243 (3.6) | <0.001 | 265 (11.0) | 115 (4.3) | <0.001 | 236 (8.8) | 128 (3.2) | <0.001 |
| Lipid lowering agents, n (%) | 4427 (86.9) | 5746 (85.7) | 0.056 | 2038 (85.0) | 2262 (84.0) | 0.347 | 2389 (88.7) | 3484 (86.8) | 0.025 |
| Year of index MI | <0.001 | <0.001 | <0.001 | ||||||
| Before 2013 | 2959 (58.1) | 4372 (65.2) | 1480 (61.7) | 1834 (68.1) | 1479 (54.9) | 2538 (63.3) | |||
| After 2013 | 2134 (41.9) | 2333 (34.8) | 919 (38.3) | 859 (31.9) | 1215 (45.1) | 1474 (36.7) | |||
| IRA | |||||||||
| Left main, n (%) | 127 (2.5) | 75 (1.1) | <0.001 | 66 (2.8) | 31(1.2) | <0.001 | 61 (2.3) | 44 (1.1) | <0.001 |
| LAD, n (%) | 2178 (42.8) | 3548 (52.9) | <0.001 | 1006 (41.9) | 1343 (49.9) | <0.001 | 1172 (43.5) | 2205 (55.0) | <0.001 |
| LCx, n (%) | 1364 (26.8) | 592 (8.8) | <0.001 | 625 (26.1) | 233 (8.7) | <0.001 | 739 (27.4) | 359 (8.9) | <0.001 |
| RCA, n (%) | 1424 (28.0) | 2490 (37.1) | <0.001 | 702 (29.3) | 1086 (40.3) | <0.001 | 722 (26.8) | 1404 (35.0) | <0.001 |
| Treated vessel | |||||||||
| Left main, n (%) | 214 (4.2) | 115 (1.7) | <0.001 | 105 (4.4) | 44 (1.6) | <0.001 | 109 (4.0) | 71 (1.8) | <0.001 |
| LAD, n (%) | 2888 (56.7) | 4035 (60.2) | <0.001 | 1378 (57.4) | 1582 (58.7) | 0.346 | 1510 (56.1) | 2453 (61.1) | <0.001 |
| LCx, n (%) | 2016 (39.6) | 1076 (16.0) | <0.001 | 957 (39.9) | 454 (16.9) | <0.001 | 1059 (39.3) | 622 (15.5) | <0.001 |
| RCA, n (%) | 1868 (36.7) | 2824 (42.1) | <0.001 | 937 (39.1) | 1236 (45.9) | <0.001 | 931 (34.6) | 1588 (39.6) | <0.001 |
| ACC/AHA lesion type | |||||||||
| Type B1, n (%) | 703 (13.8) | 857 (12.8) | 0.105 | 327 (13.6) | 327 (12.1) | 0.113 | 376 (14.0) | 530 (13.2) | 0.381 |
| Type B2, n (%) | 1797 (35.3) | 2031 (30.3) | <0.001 | 835 (34.8) | 825 (30.6) | 0.002 | 962 (35.7) | 1206 (30.1) | <0.001 |
| Type C, n (%) | 2124 (41.7) | 3139 (46.8) | <0.001 | 1025 (42.7) | 1280 (47.5) | 0.001 | 1099 (40.8) | 1859 (46.3) | <0.001 |
| Extent of CAD | |||||||||
| 1-vessel, n (%) | 2208 (43.4) | 3551 (53.0) | <0.001 | 910 (37.9) | 1267 (47.0) | <0.001 | 1298 (48.2) | 2284 (56.9) | <0.001 |
| 2-vessel, n (%) | 1724 (33.9) | 2010 (30.0) | <0.001 | 848 (35.3) | 845 (31.4) | 0.003 | 876 (32.6) | 1165 (29.0) | 0.002 |
| ≥3-vessel, n (%) | 1161 (22.8) | 1144 (17.1) | <0.001 | 641 (26.7) | 581 (21.6) | <0.001 | 520 (19.3) | 563 (14.0) | <0.001 |
| Pre-PCI TIMI 0/1, n (%) | 2047 (40.2) | 4781 (71.3) | <0.001 | 903 (37.6) | 1884 (70.0) | <0.001 | 1144 (42.5) | 2897 (72.2) | <0.001 |
| PCI within 24 h, n (%) | 4396 (86.3) | 6477 (96.6) | <0.001 | 2040 (85.0) | 2599 (96.5) | <0.001 | 2356 (87.5) | 3878 (96.7) | <0.001 |
| GP IIb/IIIa inhibitor, n (%) | 480 (9.4) | 1458 (21.7) | <0.001 | 202 (8.4) | 527 (19.6) | <0.001 | 278 (10.3) | 931 (23.2) | <0.001 |
| Transradial approach, n (%) | 1833 (36.0) | 1218 (18.2) | <0.001 | 815 (34.0) | 493 (18.3) | <0.001 | 1018 (37.8) | 725 (18.1) | <0.001 |
| IVUS, n (%) | 1241 (24.4) | 1352 (20.2) | <0.001 | 539 (22.5) | 542 (20.1) | 0.041 | 702 (26.1) | 810 (20.2) | <0.001 |
| OCT, n (%) | 67 (1.3) | 22 (0.3) | <0.001 | 26 (1.1) | 10 (0.4) | 0.004 | 41 (1.5) | 12 (0.3) | <0.001 |
| FFR, n (%) | 75 (1.5) | 61 (0.9) | 0.448 | 38 (1.6) | 24 (0.9) | 0.029 | 37 (1.4) | 37 (0.9) | 0.095 |
| Types of DES a | |||||||||
| ZES, n (%) | 1647 (32.3) | 2372 (35.4) | 0.206 | 789 (32.9) | 976 (36.2) | 0.012 | 858 (31.8) | 1396 (34.8) | 0.012 |
| EES, n (%) | 2710 (53.2) | 3374 (50.3) | 0.193 | 1289 (53.7) | 1336 (49.6) | 0.003 | 1421 (52.7) | 2038 (50.8) | 0.117 |
| BES, n (%) | 783 (15.4) | 873 (13.0) | 0.078 | 335 (14.0) | 330 (12.3) | 0.071 | 448 (16.6) | 543 (13.5) | <0.001 |
| Others, n (%) | 124 (2.4) | 190 (2.8) | 0.710 | 72 (3.0) | 89 (3.3) | 0.575 | 52 (1.9) | 101 (2.5) | 0.133 |
| Stent diameter, mm | 3.18 ± 0.42 | 3.07 ± 0.42 | <0.001 | 3.15 ± 0.42 | 3.04 ± 0.41 | <0.001 | 3.19 ± 0.41 | 3.09 ± 0.42 | <0.001 |
| Stent length, mm | 27.8 ± 12.8 | 26.7 ± 10.2 | 0.019 | 28.0 ± 12.9 | 27.0 ± 10.5 | 0.002 | 27.6 ± 12.6 | 26.5 ± 10.0 | <0.001 |
| Number of stents | 1.61 ± 0.89 | 1.40 ± 0.70 | <0.001 | 1.67 ± 0.90 | 1.44 ± 0.74 | <0.001 | 1.56 ± 0.88 | 1.40 ± 0.66 | <0.001 |
| Outcomes | DM (n = 5092) | Log-Rank | Unadjusted | Multivariable-Adjusted a | Propensity Score-Adjusted | ||||
|---|---|---|---|---|---|---|---|---|---|
| NSTEMI (n = 2399) | STEMI (n = 2693) | HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | ||
| MACE | 219 (10.0) | 211 (8.4) | 0.069 | 1.192 (0.986–1.440) | 0.069 | 1.098 (0.875–1.314) | 0.401 | 1.074 (0.850–1.358) | 0.548 |
| All-cause death | 98 (4.5) | 78 (3.1) | 0.016 | 1.436 (1.067–1.934) | 0.017 | 1.275 (0.914–1.684) | 0.121 | 1.334 (0.926–1.922) | 0.102 |
| Cardiac death | 54 (2.5) | 57 (2.2) | 0.682 | 1.081 (0.745–1.568) | 0.682 | 1.068 (0.695–1.580) | 0.756 | 1.078 (0.720–1.690) | 0.732 |
| Non-cardiac death | 44 (2.0) | 21 (0.9) | 0.001 | 2.403 (1.429–4.041) | 0.001 | 2.200 (1.231–3.813) | 0.007 | 2.484 (1.326–4.651) | 0.004 |
| Recurrent MI | 61 (2.9) | 59 (2.4) | 0.339 | 1.191 (0.832–1.703) | 0.339 | 1.102 (0.764–1.612) | 0.580 | 1.104 (0.751–1.720) | 0.660 |
| Any repeat revascularization | 95 (4.5) | 99 (4.1) | 0.484 | 1.106 (0.835–1.465) | 0.484 | 1.021 (0.612–1.312) | 0.901 | 1.186 (0.839–1.675) | 0.334 |
| ST (definite or probable) | 20 (0.8) | 25 (0.9) | 0.719 | 0.898 (0.499–1.616) | 0.719 | 0.901 (0.512–1.702) | 0.745 | 0.946 (0.485–1.968) | 0.882 |
| Outcomes | Non-DM (n = 6706) | Log-Rank | Unadjusted | Multivariable-Adjusted a | Propensity score-Adjusted | ||||
| NSTEMI (n = 2694) | STEMI (n = 4012) | HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | ||
| MACE | 175 (7.3) | 208 (5.6) | 0.014 | 1.287 (1.052–1.574) | 0.014 | 1.384 (1.120–1.694) | 0.002 | 1.543 (1.211–1.965) | <0.001 |
| All-cause death | 58 (2.5) | 59 (1.6) | 0.028 | 1.497 (1.042–2.151) | 0.029 | 2.054 (1.399–3.031) | <0.001 | 2.172 (1.423–3.276) | <0.001 |
| Cardiac death | 40 (1.7) | 35 (0.9) | 0.016 | 1.734 (1.102–2.730) | 0.017 | 2.688 (1.698–4.331) | <0.001 | 2.882 (1.679–4.967) | <0.001 |
| Non-cardiac death | 18 (0.8) | 24 (0.7) | 0.655 | 1.150 (0.624–2.118) | 0.655 | 1.215 (0.575–2.182) | 0.598 | 1.250 (0.641–2.557) | 0.539 |
| Recurrent MI | 46 (1.9) | 57 (1.5) | 0.300 | 1.227 (0.832–1.810) | 0.301 | 1.194 (0.772–1.751) | 0.511 | 1.380 (0.865–2.201) | 0.177 |
| Any repeat revascularization | 84 (3.6) | 108 (3.0) | 0.225 | 1.193 (0.897–1.586) | 0.226 | 1.184 (0.788–1.532) | 0.278 | 1.299 (0.920–1.835) | 0.137 |
| ST (definite or probable) | 9 (0.3) | 27 (0.7) | 0.063 | 0.495 (0.233–1.053) | 0.068 | 0.623 (0.302–1.178) | 0.184 | 0.513 (0.252–1.245) | 0.140 |
| Outcomes | Overall (n = 11,798) | Log-Rank | Unadjusted | Multivariable-Adjusted a | Propensity score-Adjusted | ||||
| NSTEMI (n = 5093) | STEMI (n = 6705) | HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | ||
| MACE | 394 (8.6) | 419 (6.7) | 0.001 | 1.269 (1.106–1.456) | 0.001 | 1.214 (1.034–1.315) | 0.006 | 1.298 (1.097–1.535) | 0.002 |
| All-cause death | 156 (3.4) | 137 (2.2) | <0.001 | 1.529 (1.216–1.924) | <0.001 | 1.521 (1.208–1.994) | <0.001 | 1.653 (1.252–2.183) | <0.001 |
| Cardiac death | 94 (2.0) | 92 (1.4) | 0.032 | 1.369 (1.027–1.824) | 0.032 | 1.367 (1.009–1.684) | 0.041 | 1.499 (1.060–2.120) | 0.022 |
| Non-cardiac death | 62 (1.4) | 45 (0.7) | 0.001 | 1.859 (1.266–2.729) | 0.002 | 1.745 (1.207–2.596) | 0.005 | 1.977 (1.239–3.155) | 0.004 |
| Recurrent MI | 107 (2.4) | 116 (1.9) | 0.102 | 1.245 (0.957–1.619) | 0.103 | 1.214 (0.902–1.563) | 0.372 | 1.247 (0.905–1.719) | 0.177 |
| Any repeat revascularization | 179 (4.0) | 207 (3.4) | 0.123 | 1.170 (0.958–1.429) | 0.123 | 1.060 (0.682–1.297) | 0.521 | 1.068 (0.837–1.324) | 0.597 |
| ST (definite or probable) | 29 (0.6) | 52 (0.8) | 0.179 | 0.733 (0.466–1.155) | 0.181 | 0.746 (0.502–1.273) | 0.382 | 0.754 (0.433–1.313) | 0.319 |
| Outcomes | NSTEMI (n = 5093) | Log-Rank | Unadjusted | Multivariable-Adjusted a | |||
|---|---|---|---|---|---|---|---|
| DM (n = 2399) | Non-DM (n = 2694) | HR (95% CI) | p | HR (95% CI) | p | ||
| MACE | 219 (10.0) | 175 (7.3) | 0.001 | 1.391 (1.140–1.696) | 0.001 | 1.326 (1.080–1.629) | 0.007 |
| All-cause death | 98 (4.5) | 58 (2.5) | <0.001 | 1.873 (1.354–2.592) | <0.001 | 1.701 (1.215–2.382) | 0.002 |
| Cardiac death | 54 (2.5) | 40 (1.7) | 0.051 | 1.498 (0.995–2.255) | 0.053 | 1.325 (0.866–2.027) | 0.195 |
| Non-cardiac death | 44 (2.0) | 18 (0.8) | <0.001 | 2.706 (1.564–4.683) | <0.001 | 2.549 (1.450–4.480) | 0.001 |
| Recurrent MI | 61 (2.9) | 46 (1.9) | 0.048 | 1.469 (1.002–2.154) | 0.049 | 1.469 (0.990–2.180) | 0.056 |
| Any repeat revascularization | 95 (4.5) | 84 (3.6) | 0.124 | 1.259 (0.938–1.688) | 0.125 | 1.223 (0.904–1.654) | 0.191 |
| ST (definite or probable) | 20 (0.8) | 9 (0.3) | 0.018 | 2.501 (1.139–5.492) | 0.022 | 2.272 (1.010–5.023) | 0.048 |
| Outcomes | STEMI (n = 6705) | Log-rank | Unadjusted | Multivariable-Adjusted a | |||
| DM (n = 2693) | Non-DM (n = 4012) | HR (95% CI) | p | HR (95% CI) | p | ||
| MACE | 211 (8.4) | 208 (5.6) | <0.001 | 1.507 (1.244–1.825) | <0.001 | 1.481 (1.218–1.801) | <0.001 |
| All-cause death | 78 (3.1) | 59 (1.6) | <0.001 | 1.961 (1.399–2.751) | <0.001 | 1.869 (1.322–2.643) | <0.001 |
| Cardiac death | 57 (2.2) | 35 (0.9) | <0.001 | 2.419 (1.588–3.684) | <0.001 | 2.248 (1.462–3.458) | <0.001 |
| Non-cardiac death | 21 (0.9) | 24 (0.7) | 0.385 | 1.296 (0.721–2.327) | 0.386 | 1.307 (0.716–2.384) | 0.383 |
| Recurrent MI | 59 (2.4) | 57 (1.5) | 0.020 | 1.535 (1.067–2.209) | 0.021 | 1.537 (1.060–2.228) | 0.023 |
| Any repeat revascularization | 99 (4.1) | 108 (3.0) | 0.027 | 1.360 (1.035–1.786) | 0.027 | 1.374 (1.041–1.816) | 0.024 |
| ST (definite or probable) | 25 (0.9) | 27 (0.7) | 0.244 | 1.380 (0.801–2.377) | 0.246 | 1.381 (0.792–2.224) | 0.315 |
| Outcomes | Overall (n = 11,798) | Log-rank | Unadjusted | Multivariable-Adjusted a | |||
| DM (n = 5092) | Non-DM (n = 6706) | HR (95% CI) | p | HR (95% CI) | p | ||
| MACE | 430 (9.1) | 383 (6.2) | <0.001 | 1.473 (1.283–1.690) | <0.001 | 1.434 (1.245–1.652) | <0.001 |
| All-cause death | 176 (3.7) | 117 (1.9) | <0.001 | 1.969 (1.558–2.488) | <0.001 | 1.866 (1.467–2.374) | <0.001 |
| Cardiac death | 111 (2.3) | 75 (1.2) | <0.001 | 1.939 (1.447–2.599) | <0.001 | 1.818 (1.345–2.457) | <0.001 |
| Non-cardiac death | 65 (1.4) | 42 (0.7) | <0.001 | 2.022 (1.372–2.981) | <0.001 | 1.957 (1.313–2.916) | 0.001 |
| Recurrent MI | 120 (2.7) | 103 (1.7) | 0.002 | 1.524 (1.171–1.983) | 0.002 | 1.527 (1.166–2.000) | 0.002 |
| Any repeat revascularization | 194 (4.0) | 192 (3.4) | 0.006 | 1.324 (1.085–1.617) | 0.006 | 1.314 (1.071–1.611) | 0.009 |
| ST (definite or probable) | 45 (0.9) | 36 (0.5) | 0.024 | 1.648 (1.063–2.554) | 0.026 | 1.521 (1.027–2.351) | 0.037 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.H.; Her, A.-Y.; Rha, S.-W.; Choi, C.U.; Choi, B.G.; Kim, J.B.; Park, S.; Kang, D.O.; Park, J.Y.; Park, S.-H.; et al. Comparison of Clinical Outcomes after Non-ST-Segment and ST-Segment Elevation Myocardial Infarction in Diabetic and Nondiabetic Populations. J. Clin. Med. 2022, 11, 5079. https://doi.org/10.3390/jcm11175079
Kim YH, Her A-Y, Rha S-W, Choi CU, Choi BG, Kim JB, Park S, Kang DO, Park JY, Park S-H, et al. Comparison of Clinical Outcomes after Non-ST-Segment and ST-Segment Elevation Myocardial Infarction in Diabetic and Nondiabetic Populations. Journal of Clinical Medicine. 2022; 11(17):5079. https://doi.org/10.3390/jcm11175079
Chicago/Turabian StyleKim, Yong Hoon, Ae-Young Her, Seung-Woon Rha, Cheol Ung Choi, Byoung Geol Choi, Ji Bak Kim, Soohyung Park, Dong Oh Kang, Ji Young Park, Sang-Ho Park, and et al. 2022. "Comparison of Clinical Outcomes after Non-ST-Segment and ST-Segment Elevation Myocardial Infarction in Diabetic and Nondiabetic Populations" Journal of Clinical Medicine 11, no. 17: 5079. https://doi.org/10.3390/jcm11175079
APA StyleKim, Y. H., Her, A.-Y., Rha, S.-W., Choi, C. U., Choi, B. G., Kim, J. B., Park, S., Kang, D. O., Park, J. Y., Park, S.-H., & Jeong, M. H. (2022). Comparison of Clinical Outcomes after Non-ST-Segment and ST-Segment Elevation Myocardial Infarction in Diabetic and Nondiabetic Populations. Journal of Clinical Medicine, 11(17), 5079. https://doi.org/10.3390/jcm11175079