
Complete Revascularization and One-Year Survival with Good Neurological Outcome in Patients Resuscitated from an Out-of-Hospital Cardiac Arrest

 ,
,  , ,
, ,  and
and 
Abstract
:1. Introduction
2. Material and Methods
2.1. Type of Study
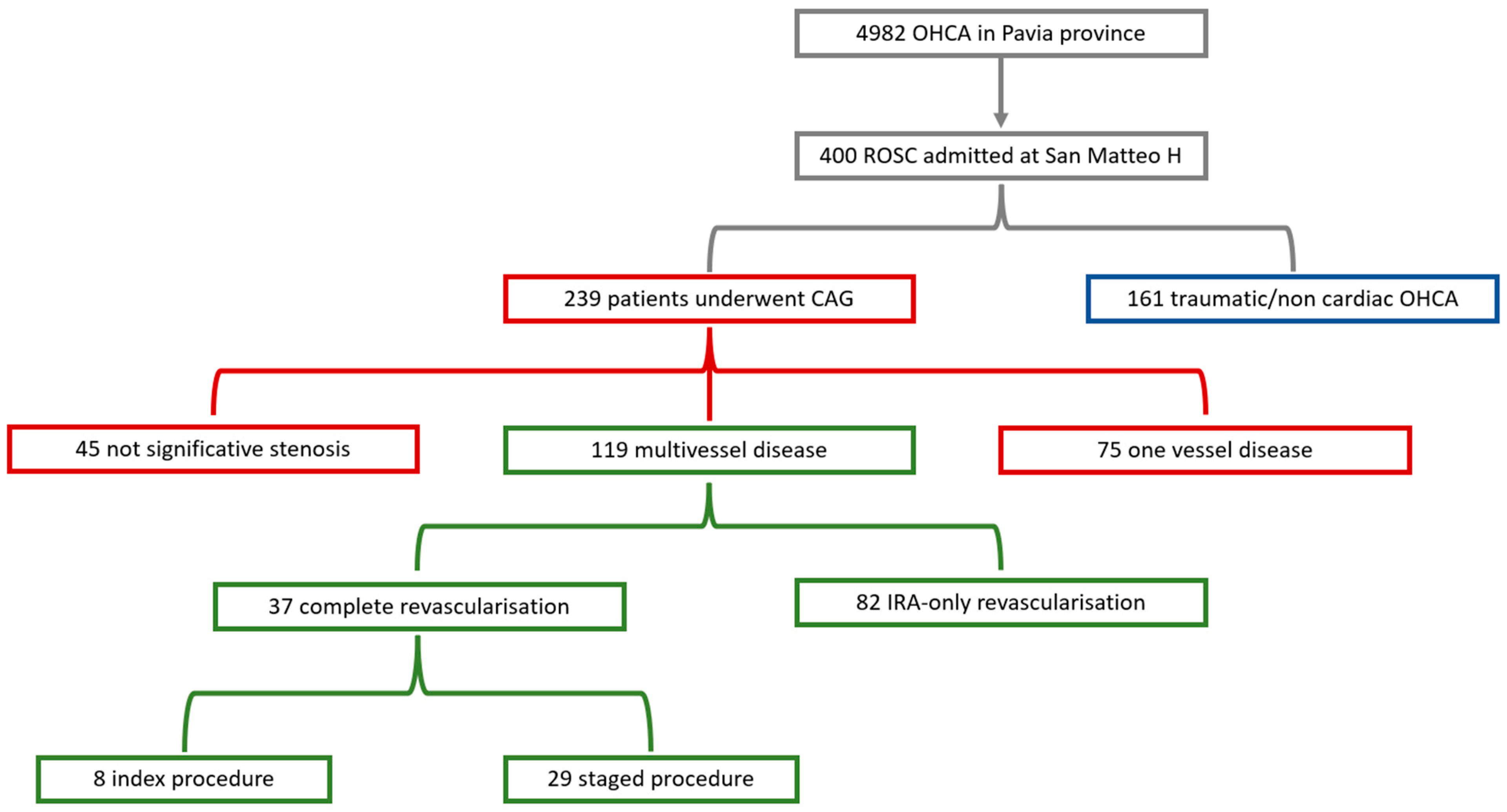
2.2. Patient Selection
2.3. Definitions
2.4. Study Endpoints
2.5. Data Management
2.6. Data Collection
2.7. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Complete Revascularization vs. IRA-Only Revascularization
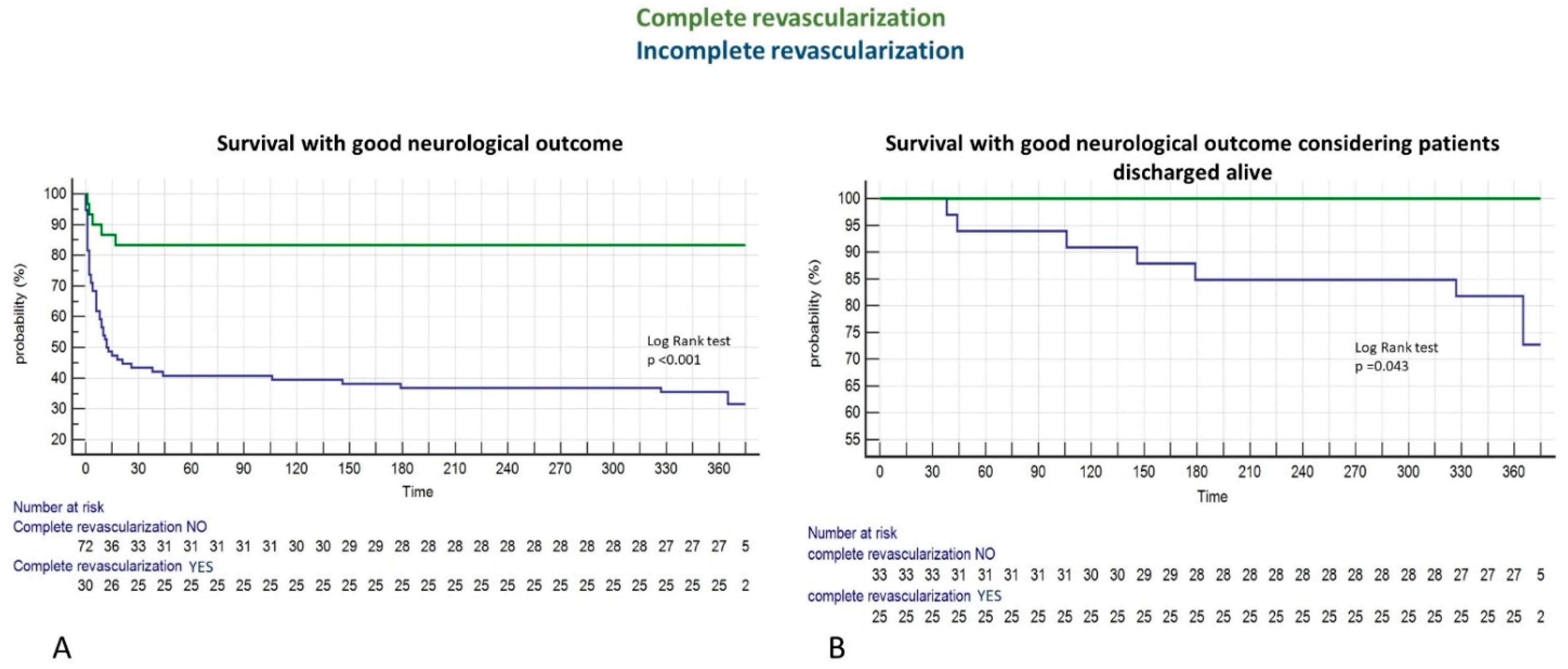
3.3. Primary and Secondary Endpoints: Complete Revascularization and One Year Survival with Good Neurological Outcome
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Atwood, C.; Eisenberg, M.S.; Herlitz, J.; Rea, T.D. Incidence of EMS-treated out-of-hospital cardiac arrest in Europe. Resuscitation 2005, 67, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Kiguchi, T.; Okubo, M.; Nishiyama, C.; Maconochie, I.; Ong, M.E.H.; Kern, K.B.; Wyckoff, M.H.; McNally, B.; Christensen, E.F.; Tjelmeland, I.; et al. Out-of-hospital cardiac arrest across the World: First report from the International Liaison Committee on Resuscitation (ILCOR). Resuscitation 2020, 152, 39–49. [Google Scholar] [CrossRef] [PubMed]
- Gräsner, J.T.; Wnent, J.; Herlitz, J.; Perkins, G.D.; Lefering, R.; Tjelmeland, I.; Koster, R.W.; Masterson, S.; Rossell-Ortiz, F.; Maurer, H.; et al. Survival after out-of-hospital cardiac arrest in Europe—Results of the EuReCa TWO study. Resuscitation 2020, 148, 218–226. [Google Scholar] [CrossRef] [PubMed]
- Gräsner, J.T.; Herlitz, J.; Tjelmeland, I.B.M.; Wnent, J.; Masterson, S.; Lilja, G.; Bein, B.; Böttiger, B.W.; Rosell-Ortiz, F.; Nolan, J.P.; et al. European Resuscitation Council Guidelines 2021: Epidemiology of cardiac arrest in Europe. Resuscitation 2021, 161, 61–79. [Google Scholar] [CrossRef] [PubMed]
- Myat, A.; Song, K.J.; Rea, T. Out-of-hospital cardiac arrest: Current concepts. Lancet 2018, 391, 970–979. [Google Scholar] [CrossRef]
- Nolan, J.P.; Sandroni, C.; Böttiger, B.W.; Cariou, A.; Cronberg, T.; Friberg, H.; Genbrugge, C.; Haywood, K.; Lilja, G.; Moulaert, V.R.M.; et al. European Resuscitation Council and European Society of Intensive Care Medicine guidelines 2021: Post-resuscitation care. Intensive Care Med. 2021, 47, 369–421. [Google Scholar] [CrossRef]
- Baldi, E.; Schnaubelt, S.; Caputo, M.L.; Klersy, C.; Clodi, C.; Bruno, J.; Compagnoni, S.; Benvenuti, C.; Domanovits, H.; Burkart, R.; et al. Association of Timing of Electrocardiogram Acquisition After Return of Spontaneous Circulation with Coronary Angiography Findings in Patients with Out-of-Hospital Cardiac Arrest. JAMA Netw. Open 2021, 4, e2032875. [Google Scholar] [CrossRef]
- Jentzer, J.C.; Scutella, M.; Pike, F.; Fitzgibbon, J.; Krehel, N.M.; Kowalski, L.; Callaway, C.W.; Rittenberger, J.C.; Reynolds, J.C.; Barsness, G.W.; et al. Early coronary angiography and percutaneous coronary intervention are associated with improved outcomes after out of hospital cardiac arrest. Resuscitation 2018, 123, 15–21. [Google Scholar] [CrossRef]
- Tranberg, T.; Lippert, F.K.; Christensen, E.F.; Stengaard, C.; Hjort, J.; Lassen, J.F.; Petersen, F.; Jensen, J.S.; Bäck, C.; Jensen, L.O.; et al. Distance to invasive heart centre, performance of acute coronary angiography, and angioplasty and associated outcome in out-of-hospital cardiac arrest: A nationwide study. Eur. Heart J. 2017, 38, 1645–1652. [Google Scholar] [CrossRef]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [CrossRef] [Green Version]
- Lemkes, J.S.; Janssens, G.N.; van der Hoeven, N.W.; Jewbali, L.S.; Dubois, E.A.; Meuwissen, M.; Rijpstra, T.A.; Bosker, H.A.; Blans, M.J.; Bleeker, G.B.; et al. Coronary Angiography after Cardiac Arrest without ST-Segment Elevation. N. Engl. J. Med. 2019, 380, 1397–1407. [Google Scholar] [CrossRef] [PubMed]
- Desch, S.; Freund, A.; Graf, T.; Fichtlscherer, S.; Haake, H.; Preusch, M.; Hammer, F.; Akin, I.; Christ, M.; Liebetrau, C.; et al. Immediate unselected coronary angiography versus delayed triage in survivors of out-of-hospital cardiac arrest without ST-segment elevation: Design and rationale of the TOMAHAWK trial. Am. Heart J. 2019, 209, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Anyfantakis, Z.A.; Baron, G.; Aubry, P.; Himbert, D.; Feldman, L.J.; Juliard, J.-M.; Ricard-Hibon, A.; Burnod, A.; Cokkinos, D.V.; Steg, P.G. Acute coronary angiographic findings in survivors of out-of-hospital cardiac arrest. Am. Heart J. 2009, 157, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Rosen, B.D.; Fernandes, V.; McClelland, R.L.; Carr, J.J.; Detrano, R.; Bluemke, D.A.; Lima, J.A. Relationship between Baseline Coronary Calcium Score and Demonstration of Coronary Artery Stenoses During Follow-Up. MESA (Multi-Ethnic Study of Atherosclerosis). JACC Cardiovasc. Imaging 2009, 2, 1175–1183. [Google Scholar] [CrossRef]
- Lipinski, M.; Do, D.; Morise, A.; Froelicher, V. What percent luminal stenosis should be used to define angiographic coronary artery disease for noninvasive test evaluation? Ann. Noninvasive Electrocardiol. 2002, 7, 98–105. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)-A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Perkins, G.D.; Jacobs, I.G.; Nadkarni, V.M.; Berg, R.A.; Bhanji, F.; Biarent, D.; Bossaert, L.L.; Brett, S.J.; Chamberlain, D.; De Caen, A.R.; et al. Cardiac arrest and cardiopulmonary resuscitation outcome reports: Update of the Utstein resuscitation registry templates for out-of-hospital cardiac arrest: A statement for healthcare professionals from a task force of the international liaison committee. Circulation 2015, 132, 1286–1300. [Google Scholar] [CrossRef]
- Baldi, E.; Compagnoni, S.; Buratti, S.; Primi, R.; Bendotti, S.; Currao, A.; Gentile, F.R.; Sechi, G.M.; Mare, C.; Bertona, R.; et al. Long-Term Outcome After Out-of-Hospital Cardiac Arrest: An Utstein-Based Analysis. Front. Cardiovasc. Med. 2021, 8, 764043. [Google Scholar] [CrossRef]
- Mehta, S.R.; Wood, D.A.; Storey, R.F.; Mehran, R.; Bainey, K.R.; Nguyen, H.; Meeks, B.; Di Pasquale, G.; López-Sendón, J.; Faxon, D.P.; et al. Complete Revascularization with Multivessel PCI for Myocardial Infarction. N. Engl. J. Med. 2019, 381, 1411–1421. [Google Scholar] [CrossRef] [Green Version]
- Lopes, N.H.; Paulitsch, F.d.S.; Gois, A.F.; Pereira, A.C.; Stolf, N.A.; Dallan, L.O.; Ramires, J.A.; Hueb, W.A. Impact of number of vessels disease on outcome of patients with stable coronary artery disease: 5-year follow-up of the Medical, Angioplasty, and bypass Surgery Study (MASS). Eur. J. Cardio-Thorac. Surg. 2008, 33, 349–354. [Google Scholar] [CrossRef] [PubMed]
- Blackledge, H.M.; Squire, B. Improving long-term outcomes following coronary artery bypass graft or percutaneous coronary revascularisation: Results from a large, population-based cohort with first intervention 1995–2004. Heart 2009, 95, 304–311. [Google Scholar] [CrossRef] [PubMed]
- Wald, D.S.; Morris, J.K.; Wald, N.J.; Chase, A.J.; Edwards, R.J.; Hughes, L.O.; Berry, C.; Oldroyd, K.G. Randomized Trial of Preventive Angioplasty in Myocardial Infarction. N. Engl. J. Med. 2013, 369, 1115–1123. [Google Scholar] [CrossRef] [PubMed]
- Gershlick, A.H.; Khan, J.N.; Kelly, D.J.; Greenwood, J.P.; Sasikaran, T.; Curzen, N.; Blackman, D.J.; Dalby, M.; Fairbrother, K.L.; Banya, W.; et al. Randomized trial of complete versus lesion-only revascularization in patients undergoing primary percutaneous coronary intervention for stemi and multivessel disease: The CvLPRIT trial. J. Am. Coll. Cardiol. 2015, 65, 963–972. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.T.; Tsai, M.S.; Huang, C.H.; Sung, C.W.; Chuang, P.Y.; Wang, C.H.; Wu, Y.W.; Chang, W.T.; Chen, W.J. Multivessel versus Culprit-Only Revascularization Strategies in Cardiac Arrest Survivors. Acta Cardiol. Sin. 2022, 38, 175–186. [Google Scholar] [CrossRef]
- Kim, Y.J.; Park, D.W.; Kim, Y.H.; Choi, M.; Kim, S.J.; Lee, G.T.; Lee, D.H.; Lee, B.K.; Oh, J.S.; Oh, S.H.; et al. Immediate complete revascularization showed better outcome in out-of-hospital cardiac arrest survivors with left main or triple-vessel coronary diseases. Sci. Rep. 2022, 12, 4354. [Google Scholar] [CrossRef]
- Buratti, S.; Crimi, G.; Somaschini, A.; Cornara, S.; Camporotondo, R.; Cosentino, N.; Moltrasio, M.; Rubino, M.; De Metrio, M.; Marana, I.; et al. A preprocedural risk score predicts acute kidney injury following primary percutaneous coronary intervention. Catheter. Cardiovasc. Interv. 2021, 98, 197–205. [Google Scholar] [CrossRef]
- Symons, R.; Pontone, G.; Schwitter, J.; Francone, M.; Iglesias, J.F.; Barison, A.; Zalewski, J.; de Luca, L.; Degrauwe, S.; Claus, P.; et al. Long-Term Incremental Prognostic Value of Cardiovascular Magnetic Resonance After ST-Segment Elevation Myocardial Infarction: A Study of the Collaborative Registry on CMR in STEMI. JACC Cardiovasc. Imaging 2018, 11, 813–825. [Google Scholar] [CrossRef]
- Thiele, H.; Akin, I.; Sandri, M.; De Waha-Thiele, S.; Meyer-Saraei, R.; Fuernau, G.; Eitel, I.; Nordbeck, P.; Geisler, T.; Landmesser, U.; et al. One-Year Outcomes after PCI Strategies in Cardiogenic Shock. N. Engl. J. Med. 2018, 379, 1699–1710. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Patients Who UnderwentCAG (n = 239) | Patients with Multivessel Disease (n = 119) | |
|---|---|---|
| Age (years) | 63.7 ± 12.4 | 66.8 ± 12 |
| Sex (%) | ||
| Male | 191 (79.9) | 98 (82.4) |
| Female | 48 (20.1) | 21 (17.6) |
| BMI (kg/m2) | 25.7 (24.1–27.8) | 26 (24–28) |
| Hypertension (%) | 174 (72.8) | 90 (81.1) |
| Diabetes (%) | 38 (15.9) | 19 (17.3) |
| Smoker (%) | 29 (12.1) | 35 (31) |
| Hypercholesterolemia (%) | 123 (51.5) | 67 (60.4) |
| Previous myocardial revascularization (%) | ||
| Previous PCI | 13 (5.4) | 9 (7.5) |
| Previous CABG | 31 (13.1) | 18 (15.1) |
| Previous PCI + CABG | 2 (0.8) | 1 (0.8) |
| Rhythm at presentation (%) | ||
| Shockable | 201 (84.1) | 100 (84) |
| Not shockable | 38 (15.9) | 19 (16) |
| First rhythm detected (%) | ||
| VF | 181 (75.7) | 88 (74) |
| Pulseless VT | 3 (1.3) | 3 (2.5) |
| PEA | 22 (9.2) | 13 (10.9) |
| Asystole | 12 (5.0) | 5 (4.2) |
| AED shockable | 17 (7.1) | 9 (7.6) |
| AED not shockable | 4 (1.7) | 1 (0.8) |
| ECG diagnostic for STEMI (%) | 162 (67.9) | 75 (74.3) |
| HR (bpm) | 99 ± 29 | 101 ± 30.3 |
| Median CA duration (min) | 24 (13.6–41.9) | 23 (13–42) |
| Time from CA to CAG (days) | 0.8 ± 3.4 | 0.7 ± 2.4 |
| LVEF (%) | 37 (30–45) | 40 (30–45) |
| Pharmacological haemodynamic support (%) | 80 (33.5) | 37 (33) |
| IABP (%) | 14 (5.9) | 7 (6.4) |
| ECMO (%) | 26 (10.9) | 9 (8.2) |
| IABP + ECMO (%) | 9 (3.7) | 6 (5.5) |
| Serum Creatinine on admission (mg/dL) | 1.04 (0.9–1.3) | 1.03 (0.9–1.3) |
| hs-TNI on admission (ng/L) | 695 (517–1126) | 913 (245.8–4455.5) |
| hs-TNI peak value (ng/L) | 51,194 (7853–102,181) | 52,611 (9662–106,017) |
| CK on admission (U/L) | 231 (132–534) | 263 (133–541) |
| CK peak value (U/L) | 1947 (735–5154) | 2106 (985–4013) |
| Hb on admission (g/dL) | 13.4 ± 1.8 | 13.7 ± 1.9 |
| Survival at discharge (%) | 157 (66) | 72 (60.5) |
| Characteristic | Complete Revascularization (CR) (n = 37) | IRA-Only Revascularization (n = 82) | p Value |
|---|---|---|---|
| Age (years) | 62.0 ± 11.6 | 69.0 ± 12.1 | 0.16 |
| Sex | |||
| Male | 33 (89%) | 65 (79%) | 0.19 |
| Female | 4 (11%) | 17 (21%) | |
| BMI (kg/m2) | 26.1 (24.2–29.3) | 25.4 (24.2–27.8) | 0.35 |
| Hypertension | 26 (70%) | 70 (86%) | 0.04 |
| Diabetes | 2 (5.4%) | 19 (23%) | 0.02 |
| Smoker | 13 (35%) | 24 (29%) | 0.63 |
| Hypercholesterolemia | 25 (67%) | 34 (56%) | 0.27 |
| Previous myocardial revascularization | 6 (16%) | 22 (27%) | 0.27 |
| Rhythm at presentation | |||
| Shockable | 35 (95%) | 65 (79%) | 0.035 |
| Not shockable | 2 (5%) | 17 (21%) | |
| First rhythm detected | 0.23 | ||
| VF | 29 (78.4%) | 59 (71.9%) | |
| Pulseless VT | 1 (2.7%) | 2 (2.5%) | |
| PEA | 2 (5.4%) | 11 (13.4%) | |
| Asystole | 0 (0%) | 5 (6.1%) | |
| DAE shockable | 5 (13.5%) | 4 (4.9%) | |
| DAE not shockable | 0 (0%) | 1 (1.2%) | |
| ECG diagnostic for STEMI | 30 (81%) | 58 (70%) | 0.23 |
| HR (bpm) | 100 ± 34 | 100 ± 28 | 0.95 |
| Median CA duration (min) | 18.3 (4.0–32.7) | 27.3 (14.0–42.3) | 0.05 |
| Time from CA to CAG (days) | 0.5 ± 1.7 | 0.8 ± 2.6 | 0.21 |
| Time from CA to CR | 5 (2.5–10.3) | ||
| LVEF (%) | 40 (37–45) | 40 (25–50) | 0.46 |
| Pharmacological haemodynamic support | 8 (22%) | 32 (39%) | 0.09 |
| LV mechanical assistance | 6 (16.2%) | 17 (20.1%) | 0.09 |
| IABP | 2 (5%) | 5 (6.1%) | |
| ECMO | 0 | 10 (12%) | |
| IABP + ECMO | 4 (10%) | 2 (2.4%) | |
| Number of vessels involved | 0.45 | ||
| Two-vessel disease | 22 (59.5%) | 47 (56.1%) | |
| Three-vessel disease | 15 (40.5%) | 36 (43.9%) | |
| Chronic total occlusion | 9 (24.3%) | 41 (50.0%) | 0.009 |
| Serum Creatinine on admission (mg/dL) | 0.98 (0.83–1.05) | 1.1 (0.9–1.4) | 0.019 |
| TNI on admission (ng/L) | 581 (238–1316) | 1866 (260–6972) | 0.13 |
| TNI peak value (ng/L) | 56,925 (10,258–188,560) | 51,180 (8377–89,998) | 0.45 |
| CK on admission (U/L) | 177 (118–349) | 318 (151–633) | 0.03 |
| CK peak value (U/L) | 2310 (1201–5388) | 1869 (765–3301) | 0.49 |
| Hb on admission (g/dL) | 14.4 ± 1.5 | 13.1 ± 1.9 | 0.0005 |
| Survival at discharge | 32 (86.5%) | 41 (50.6%) | 0.0002 |
| Variable | Univariable Logistic Regression Analysis for the Probability of Receiving a Complete Revascularization | Multivariable Logistic Regression Analysis for the Probability of Receiving a Complete Revascularization | ||||
|---|---|---|---|---|---|---|
| Odds Ratio | CI 95% | p Value | Odds Ratio | CI 95% | p Value | |
| Age | 0.98 | 0.94–1.01 | 0.20 | |||
| Diabetes | 0.3 | 0.08–1.1 | 0.07 | |||
| Previous myocardial infarction | 0.44 | 0.16–1.2 | 0.11 | |||
| Previous myocardial revascularization | ||||||
| CABG | 1.18 | 0.3–5.3 | 0.83 | |||
| PCI | 0.39 | 0.1–1.5 | 0.16 | |||
| Shockable rhythm at presentation | 5.1 | 1.12–22.9 | 0.03 | 2.7 | 0.5–13.5 | 0.23 |
| Cardiac arrest duration (min) | 0.4 | 0.2–0.9 | 0.02 | 0.99 | 0.97–1 | 0.34 |
| Two versus three-vessels disease | 1 | 0.5–2.2 | 0.98 | |||
| Chronic total occlusion | 0.37 | 0.16–0.85 | 0.02 | 0.4 | 0.2–1 | 0.049 |
| SCr on admission (mg/dL) | 0.16 | 0.04–0.7 | 0.018 | 0.3 | 0.1–1.6 | 0.17 |
| TNI on admission (ng/L) | 0.7 | 0.5–1.1 | 0.17 | |||
| TNI peak value (ng/L) | 1.4 | 0.8–2.5 | 0.3 | |||
| CK on admission (U/L) | 0.4 | 0.1–1 | 0.06 | |||
| CK peak value (U/L) | 1.4 | 0.5–4.3 | 0.52 | |||
| Pharmacological or mechanical circulatory support | 0.9 | 0.3–2.6 | 0.86 | |||
| Univariable Cox Regression Model for the Probability of Death or Poor Neurologic Outcome | Multivariable Cox Regression Model for the Probability of Death or Poor Neurologic Outcome | |||||
|---|---|---|---|---|---|---|
| Variable | HR | 95%CI | p | HR | 95%CI | p |
| Age (year) | 1 | 0.99–1.02 | 0.34 | |||
| Cardiac arrest duration (min) | 1.02 | 1.01–1.02 | <0.001 | 1.02 | 1.01–1.04 | 0.04 |
| Shockable presenting rhythm | 0.3 | 0.2–0.4 | <0.001 | 0.35 | 0.1–0.9 | 0.03 |
| Complete revascularization | 0.2 | 0.1–0.4 | <0.001 | 0.33 | 0.1–0.9 | 0.04 |
| Number of vessels involved | ||||||
| 0 | Ref | |||||
| 1 | 0.6 | 0.4–1.1 | 0.13 | |||
| 2 | 0.6 | 0.3–1.1 | 0.12 | |||
| 3 | 1.3 | 0.7–2.2 | 0.42 | |||
| LVEF > 40% | 0.8 | 0.4–1.4 | 0.37 | |||
| CTO | 1.3 | 0.8–1.9 | 0.30 | |||
| Previous revascularization | ||||||
| No | Ref | |||||
| CABG | 0.8 | 0.3–1.9 | 0.6 | |||
| PCI | 1.5 | 0.8–2.7 | 0.18 | |||
| Previous STEMI | 1.2 | 0.7–1.9 | 0.5 | |||
| TNI (peak) (ng/L) | 1.6 | 1–2.4 | 0.04 | 1.3 | 0.7–2.6 | 0.41 |
| CK (peak) (U/L) | 1.8 | 1–3.2 | 0.05 | |||
| SCr on admission (mg/dL) | 1.3 | 1–1.7 | 0.016 | 0.9 | 0.5–1.7 | 0.76 |
| Pharmacological or mechanical circulatory support | 2.8 | 1.8–4.4 | <0.001 | 1.6 | 0.6–4.1 | 0.33 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kajana, V.; Baldi, E.; Gentile, F.R.; Compagnoni, S.; Quilico, F.; Vicini Scajola, L.; Repetto, A.; Mandurino-Mirizzi, A.; Ferlini, M.; Marinoni, B.; et al. Complete Revascularization and One-Year Survival with Good Neurological Outcome in Patients Resuscitated from an Out-of-Hospital Cardiac Arrest. J. Clin. Med. 2022, 11, 5071. https://doi.org/10.3390/jcm11175071
Kajana V, Baldi E, Gentile FR, Compagnoni S, Quilico F, Vicini Scajola L, Repetto A, Mandurino-Mirizzi A, Ferlini M, Marinoni B, et al. Complete Revascularization and One-Year Survival with Good Neurological Outcome in Patients Resuscitated from an Out-of-Hospital Cardiac Arrest. Journal of Clinical Medicine. 2022; 11(17):5071. https://doi.org/10.3390/jcm11175071
Chicago/Turabian StyleKajana, Vilma, Enrico Baldi, Francesca Romana Gentile, Sara Compagnoni, Federico Quilico, Luca Vicini Scajola, Alessandra Repetto, Alessandro Mandurino-Mirizzi, Marco Ferlini, Barbara Marinoni, and et al. 2022. "Complete Revascularization and One-Year Survival with Good Neurological Outcome in Patients Resuscitated from an Out-of-Hospital Cardiac Arrest" Journal of Clinical Medicine 11, no. 17: 5071. https://doi.org/10.3390/jcm11175071
APA StyleKajana, V., Baldi, E., Gentile, F. R., Compagnoni, S., Quilico, F., Vicini Scajola, L., Repetto, A., Mandurino-Mirizzi, A., Ferlini, M., Marinoni, B., Ferrario Ormezzano, M., Primi, R., Bendotti, S., Currao, A., & Savastano, S. (2022). Complete Revascularization and One-Year Survival with Good Neurological Outcome in Patients Resuscitated from an Out-of-Hospital Cardiac Arrest. Journal of Clinical Medicine, 11(17), 5071. https://doi.org/10.3390/jcm11175071