
Prognostic Value of C-Reactive Protein and Albumin in Neurocritically Ill Patients with Acute Stroke

Abstract
:1. Introduction
2. Methods
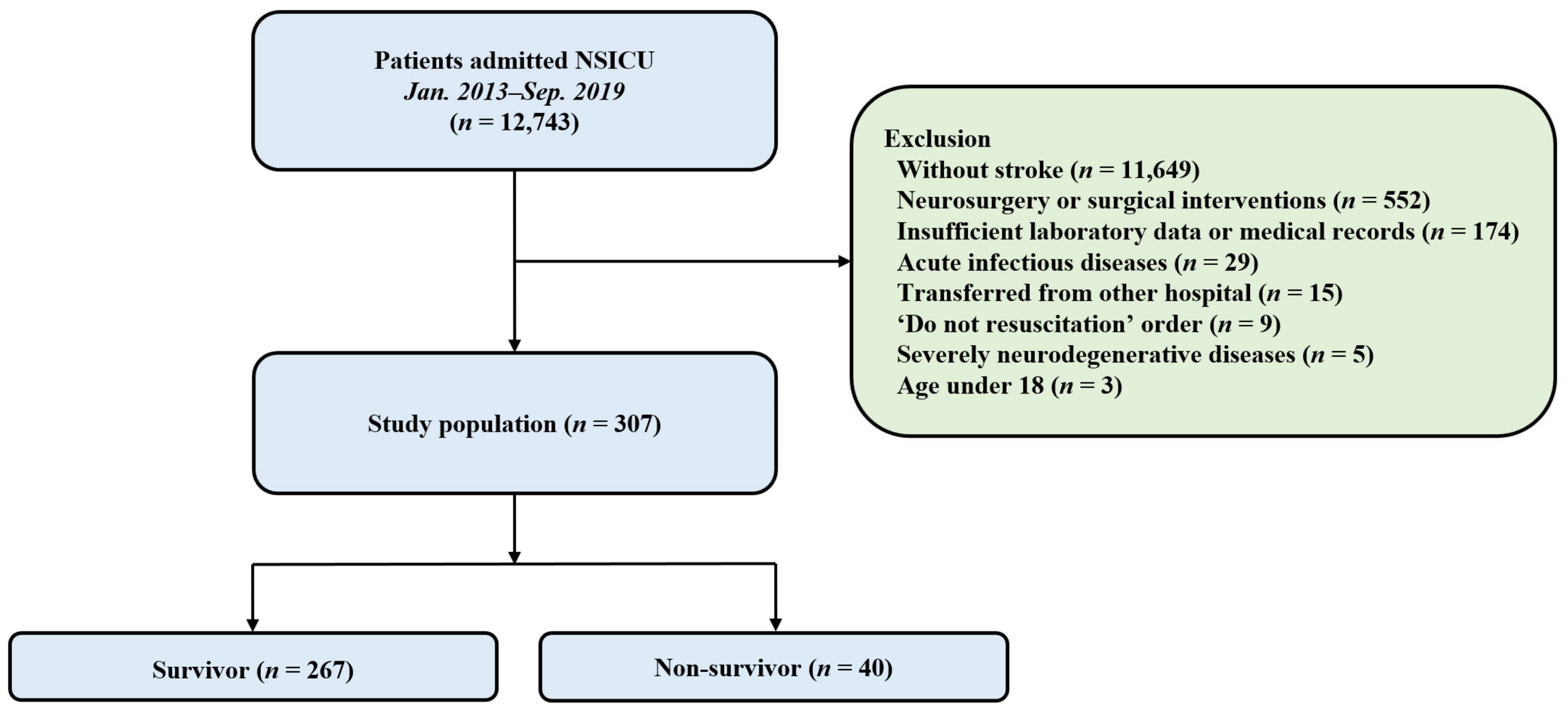
2.1. Study Population
2.2. Definitions and Endpoints
2.3. Statistical Analyses
3. Results
3.1. Baseline Characteristics and Clinical Outcome
3.2. Relationship between CRP, CRP Variants, and Albumin and Clinical Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bender, M.; Haferkorn, K.; Friedrich, M.; Uhl, E.; Stein, M. Impact of Early C-Reactive Protein/Albumin Ratio on Intra-Hospital Mortality Among Patients with Spontaneous Intracerebral Hemorrhage. J. Clin. Med. 2020, 9, 1236. [Google Scholar] [CrossRef] [PubMed]
- Devran, O.; Karakurt, Z.; Adıgüzel, N.; Güngör, G.; Moçin, O.Y.; Balcı, M.K.; Celik, E.; Saltürk, C.; Takır, H.B.; Kargın, F.; et al. C-reactive protein as a predictor of mortality in patients affected with severe sepsis in intensive care unit. Multidiscip. Respir. Med. 2012, 7, 47. [Google Scholar] [CrossRef] [PubMed]
- Quispe, E.Á.; Li, X.M.; Yi, H. Comparison and relationship of thyroid hormones, IL-6, IL-10 and albumin as mortality predictors in case-mix critically ill patients. Cytokine 2016, 81, 94–100. [Google Scholar] [CrossRef]
- Juvela, S.; Kuhmonen, J.; Siironen, J. C-reactive protein as predictor for poor outcome after aneurysmal subarachnoid haemorrhage. Acta Neurochir. 2012, 154, 397–404. [Google Scholar] [CrossRef] [PubMed]
- VanGilder, R.L.; Davidov, D.M.; Stinehart, K.R.; Huber, J.D.; Turner, R.C.; Wilson, K.S.; Haney, E.; Davis, S.M.; Chantler, P.D.; Theeke, L.; et al. C-reactive protein and long-term ischemic stroke prognosis. J. Clin. Neurosci. 2014, 21, 547–553. [Google Scholar] [CrossRef]
- Qu, R.; Hu, L.; Ling, Y.; Hou, Y.; Fang, H.; Zhang, H.; Liang, S.; He, Z.; Fang, M.; Li, J.; et al. C-reactive protein concentration as a risk predictor of mortality in intensive care unit: A multicenter, prospective, observational study. BMC Anesthesiol. 2020, 20, 292. [Google Scholar] [CrossRef]
- Ryu, J.A.; Yang, J.H.; Lee, D.; Park, C.M.; Suh, G.Y.; Jeon, K.; Cho, J.; Baek, S.Y.; Carriere, K.C.; Chung, C.R. Clinical Usefulness of Procalcitonin and C-Reactive Protein as Outcome Predictors in Critically Ill Patients with Severe Sepsis and Septic Shock. PLoS ONE 2015, 10, e0138150. [Google Scholar]
- Villet, S.; Chiolero, R.L.; Bollmann, M.D.; Revelly, J.P.; Cayeux, R.N.M.; Delarue, J.; Berger, M.M. Negative impact of hypocaloric feeding and energy balance on clinical outcome in ICU patients. Clin. Nutr. 2005, 24, 502–509. [Google Scholar] [CrossRef]
- Dvir, D.; Cohen, J.; Singer, P. Computerized energy balance and complications in critically ill patients: An observational study. Clin. Nutr. 2006, 25, 37–44. [Google Scholar] [CrossRef]
- Moisey, L.L.; Mourtzakis, M.; Cotton, B.A.; Premji, T.; Heyland, D.K.; Wade, C.E.; Bulger, E.; Kozar, R.A.; Nutrition and Rehabilitation Investigators Consortium (NUTRIC). Skeletal muscle predicts ventilator-free days, ICU-free days, and mortality in elderly ICU patients. Crit. Care 2013, 17, R206. [Google Scholar] [CrossRef]
- Carriere, I.; Dupuy, A.M.; Lacroux, A.; Cristol, J.P.; Delcourt, C. Biomarkers of inflammation and malnutrition associated with early death in healthy elderly people. J. Am. Geriatr. Soc. 2008, 56, 840–846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Domínguez de Villota, E.; Mosquera, J.M.; Rubio, J.J.; Galdos, P.; Díez Balda, V.; de la Serna, J.L.; Tomás, M.I. Association of a low serum albumin with infection and increased mortality in critically ill patients. Intensive Care Med. 1980, 7, 19–22. [Google Scholar] [CrossRef] [PubMed]
- Kendall, H.; Abreu, E.; Cheng, A.L. Serum Albumin Trend Is a Predictor of Mortality in ICU Patients With Sepsis. Biol. Res. Nurs. 2019, 21, 237–244. [Google Scholar] [CrossRef]
- Yap, F.H.; Joynt, G.M.; Buckley, T.A.; Wong, E.L. Association of serum albumin concentration and mortality risk in critically ill patients. Anaesth. Intensive Care 2002, 30, 202–207. [Google Scholar] [CrossRef]
- Iwata, M.; Kuzuya, M.; Kitagawa, Y.; Iguchi, A. Prognostic value of serum albumin combined with serum C-reactive protein levels in older hospitalized patients: Continuing importance of serum albumin. Aging Clin. Exp. Res. 2006, 18, 307–311. [Google Scholar] [CrossRef] [PubMed]
- Donini, L.M.; Savina, C.; Ricciardi, L.M.; Coletti, C.; Paolini, M.; Scavone, L.; de Felice, M.R.; Laviano, A.; Rossi Fanelli, F.; Cannella, C. Predicting the outcome of artificial nutrition by clinical and functional indices. Nutrition 2009, 25, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Oh, T.K.; Song, I.A.; Lee, J.H. Clinical usefulness of C-reactive protein to albumin ratio in predicting 30-day mortality in critically ill patients: A retrospective analysis. Sci. Rep. 2018, 8, 14977. [Google Scholar] [CrossRef]
- Di Napoli, M.; Papa, F.; Bocola, V. C-reactive protein in ischemic stroke: An independent prognostic factor. Stroke 2001, 32, 917–924. [Google Scholar] [CrossRef]
- Kapoor, A.; Dhandapani, S.; Gaudihalli, S.; Dhandapani, M.; Singh, H.; Mukherjee, K.K. Serum albumin level in spontaneous subarachnoid haemorrhage: More than a mere nutritional marker! Br. J. Neurosurg. 2018, 32, 47–52. [Google Scholar] [CrossRef]
- Schuss, P.; Hadjiathanasiou, A.; Brandecker, S.; Güresir, Á.; Vatter, H.; Güresir, E. Elevated C-reactive protein and white blood cell count at admission predict functional outcome after non-aneurysmal subarachnoid hemorrhage. J. Neurol. 2018, 265, 2944–2948. [Google Scholar] [CrossRef]
- Jeon, Y.T.; Lee, J.H.; Lee, H.; Lee, H.K.; Hwang, J.W.; Lim, Y.J.; Park, H.P. The postoperative C-reactive protein level can be a useful prognostic factor for poor outcome and symptomatic vasospasm in patients with aneurysmal subarachnoid hemorrhage. J. Neurosurg. Anesth. 2012, 24, 317–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, D.; Yan, H.; Wei, Y.; Liu, X.; Zhuang, Z.; Dai, W.; Li, J.; Li, W.; Hang, C. C-Reactive Protein/Albumin Ratio Correlates With Disease Severity and Predicts Outcome in Patients With Aneurysmal Subarachnoid Hemorrhage. Front. Neurol. 2019, 10, 1186. [Google Scholar] [CrossRef]
- Lee, S.; Kim, Y.O.; Ryu, J.A. Clinical usefulness of early serial measurements of C-reactive protein as outcome predictors in patients with subarachnoid hemorrhage. BMC Neurol. 2020, 20, 112. [Google Scholar] [CrossRef] [PubMed]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef]
- Capuzzo, M.; Valpondi, V.; Sgarbi, A.; Bortolazzi, S.; Pavoni, V.; Gilli, G.; Candini, G.; Gritti, G.; Alvisi, R. Validation of severity scoring systems SAPS II and APACHE II in a single-center population. Intensive Care Med. 2000, 26, 1779–1785. [Google Scholar] [CrossRef]
- Meredith, W.; Rutledge, R.; Fakhry, S.M.; Emery, S.; Kromhout-Schiro, S. The conundrum of the Glasgow Coma Scale in intubated patients: A linear regression prediction of the Glasgow verbal score from the Glasgow eye and motor scores. J. Trauma 1998, 44, 839–844. [Google Scholar] [CrossRef] [PubMed]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef]
- Vila, N.; Castillo, J.; Dávalos, A.; Chamorro, A. Proinflammatory cytokines and early neurological worsening in ischemic stroke. Stroke 2000, 31, 2325–2329. [Google Scholar] [CrossRef]
- Castell, J.V.; Gomez-Lechon, M.J.; David, M.; Fabra, R.; Trullenque, R.; Heinrich, P.C. Acute-phase response of human hepatocytes: Regulation of acute-phase protein synthesis by interleukin-6. Hepatology 1990, 12, 1179–1186. [Google Scholar] [CrossRef]
- Ormstad, H.; Aass, H.C.; Lund-Sørensen, N.; Amthor, K.F.; Sandvik, L. Serum levels of cytokines and C-reactive protein in acute ischemic stroke patients, and their relationship to stroke lateralization, type, and infarct volume. J. Neurol. 2011, 258, 677–685. [Google Scholar] [CrossRef]
- Turner, C.L.; Budohoski, K.; Smith, C.; Hutchinson, P.J.; Kirkpatrick, P.J.; Murray, G.D. Elevated Baseline C-Reactive Protein as a Predictor of Outcome After Aneurysmal Subarachnoid Hemorrhage: Data From the Simvastatin in Aneurysmal Subarachnoid Hemorrhage (STASH) Trial. Neurosurgery 2015, 77, 786–792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romero, F.R.; Bertolini Ede, F.; Figueiredo, E.G.; Teixeira, M.J. Serum C-reactive protein levels predict neurological outcome after aneurysmal subarachnoid hemorrhage. Arq. Neuropsiquiatr. 2012, 70, 202–205. [Google Scholar] [CrossRef] [PubMed]
- Di Napoli, M.; Behrouz, R.; Topel, C.H.; Misra, V.; Pomero, F.; Giraudo, A.; Pennati, P.; Masotti, L.; Schreuder, F.; Staals, J.; et al. Hypoalbuminemia, systemic inflammatory response syndrome, and functional outcome in intracerebral hemorrhage. J. Crit. Care 2017, 41, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Hart, P.C.; Rajab, I.M.; Alebraheem, M.; Potempa, L.A. C-Reactive Protein and Cancer-Diagnostic and Therapeutic Insights. Front. Immunol. 2020, 11, 595835. [Google Scholar] [CrossRef]
- Shrotriya, S.; Walsh, D.; Bennani-Baiti, N.; Thomas, S.; Lorton, C. C-Reactive Protein Is an Important Biomarker for Prognosis Tumor Recurrence and Treatment Response in Adult Solid Tumors: A Systematic Review. PLoS ONE 2015, 10, e0143080. [Google Scholar]
- Shrotriya, S.; Walsh, D.; Nowacki, A.S.; Lorton, C.; Aktas, A.; Hullihen, B.; Benanni-Baiti, N.; Hauser, K.; Ayvaz, S.; Estfan, B. Serum C-reactive protein is an important and powerful prognostic biomarker in most adult solid tumors. PLoS ONE 2018, 13, e0202555. [Google Scholar] [CrossRef]
- Ay, C.; Dunkler, D.; Pirker, R.; Thaler, J.; Quehenberger, P.; Wagner, O.; Zielinski, C.; Pabinger, I. High D-dimer levels are associated with poor prognosis in cancer patients. Haematologica 2012, 97, 1158–1164. [Google Scholar] [CrossRef]
- Inal, T.; Anar, C.; Polat, G.; Unsal, I.; Halilcolar, H. The prognostic value of D-dimer in lung cancer. Clin. Respir. J. 2015, 9, 305–313. [Google Scholar] [CrossRef]
- Gallo, M.; Sapio, L.; Spina, A.; Naviglio, D.; Calogero, A.; Naviglio, S. Lactic dehydrogenase and cancer: An overview. Front. Biosci. 2015, 20, 1234–1249. [Google Scholar]
- Forkasiewicz, A.; Dorociak, M.; Stach, K.; Szelachowski, P.; Tabola, R.; Augoff, K. The usefulness of lactate dehydrogenase measurements in current oncological practice. Cell Mol. Biol. Lett. 2020, 25, 35. [Google Scholar] [CrossRef]
- Caliskan, S.; Sungur, M. Fibrinogen and D-dimer levels in prostate cancer: Preliminary results. Prostate Int. 2017, 5, 110–112. [Google Scholar] [CrossRef] [PubMed]
- Luan, Y.Y.; Yao, Y.M. The Clinical Significance and Potential Role of C-Reactive Protein in Chronic Inflammatory and Neurodegenerative Diseases. Front. Immunol. 2018, 9, 1302. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
| Characteristics | Survivor (n = 267) | Non-Survivor (n = 40) | p |
|---|---|---|---|
| Age, years, (mean ± SD) | 59.35 ± 16.52 | 60.77 ± 14.12 | 0.606 |
| Male, n (%) | 127 (47.6) | 20 (50.0) | 0.906 |
| Comorbidities, n (%) | |||
| Hypertension | 123 (46.1) | 22 (55.0) | 0.376 |
| Malignancy | 83 (31.1) | 13 (32.5) | 0.999 |
| Diabetes mellitus | 42 (15.7) | 8 (20.0) | 0.651 |
| Chronic kidney disease | 17 (6.4) | 6 (15.0) | 0.107 |
| Chronic liver disease | 9 (3.4) | 0 (0.0) | 0.499 |
| Habitual risk factors, n (%) | |||
| Alcohol intake | 82 (30.7) | 15 (37.5) | 0.497 |
| Current smoker | 59 (22.1) | 7 (17.5) | 0.650 |
| Classification of subtype of stroke, n (%) | 0.623 | ||
| Intracerebral hemorrhage | 145 (54.3) | 25 (62.5) | |
| Subarachnoid hemorrhage | 114 (42.7) | 14 (35.0) | |
| Cerebral infarction | 8 (3.0) | 1 (2.5) | |
| APACHE II score on ICU admission (mean ± SD) | 5.42 ± 5.23 | 11.12 ± 6.84 | <0.001 |
| GCS on ICU admission (mean ± SD) | 13.75 ± 2.18 | 8.07 ± 3.79 | <0.001 |
| ICU management, n (%) | |||
| Mechanical ventilation | 93 (34.8) | 35 (87.5) | <0.001 |
| Invasive ICP monitoring | 19 (7.1) | 1 (2.5) | 0.447 |
| Continuous renal replacement therapy | 2 (0.7) | 2 (5.0) | 0.143 |
| Use of one hyperosmolar agent | 120 (44.9) | 12 (30.0) | 0.108 |
| Use of more than one hyperosmolar agent | 81 (30.3) | 23 (57.5) | 0.001 |
| Use of vasopressor | 9 (3.4) | 12 (30.0) | <0.001 |
| Variable | Survivor (n = 267) | Non-Survivor (n = 40) | p |
|---|---|---|---|
| CRP, mg/L | 3.43 ± 5.51 | 11.33 ± 10.08 | <0.001 |
| Albumin, g/L | 3.58 ± 0.50 | 3.17 ± 0.50 | <0.001 |
| CAR | 110.51 ± 202.81 | 394.03 ± 393.95 | <0.001 |
| ΔCRP | 2.30 ± 4.95 | 1.28 ± 7.56 | 0.261 |
| CRPc | −12.68 ± 271.27 | 3.92 ± 72.77 | 0.701 |
| Variable | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | |
| CRP | 1.12 (1.08–1.18) | <0.001 | 1.41 (1.05–1.91) | 0.023 |
| CRPc | 1.00 (0.98–1.00) | 0.702 | ||
| Albumin | 0.21 (0.10–0.42) | <0.001 | ||
| CAR | 1.01 (1.01–1.03) | <0.001 | ||
| APACHEII score on ICU admission | 1.15 (1.09–1.22) | <0.001 | 1.09 (1.01–1.17) | 0.020 |
| Use of mechanical ventilator | 13.10 (5.40–39.16) | <0.001 | 7.74 (2.48–30.03) | 0.001 |
| Use of vasopressor | 12.29 (4.80–32.64) | <0.001 | 4.46 (1.15–18.25) | 0.032 |
| Use of mannitol | 0.53 (0.25–1.05) | 0.079 | 0.24 (0.07–0.67) | 0.011 |
| Use of more than one hyperosmolar agent | 3.11 (1.58–6.21) | 0.001 | 4.21 (1.67–11.33) | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jang, J.H.; Hong, S.; Ryu, J.-A. Prognostic Value of C-Reactive Protein and Albumin in Neurocritically Ill Patients with Acute Stroke. J. Clin. Med. 2022, 11, 5067. https://doi.org/10.3390/jcm11175067
Jang JH, Hong S, Ryu J-A. Prognostic Value of C-Reactive Protein and Albumin in Neurocritically Ill Patients with Acute Stroke. Journal of Clinical Medicine. 2022; 11(17):5067. https://doi.org/10.3390/jcm11175067
Chicago/Turabian StyleJang, Ji Hoon, SungMin Hong, and Jeong-Am Ryu. 2022. "Prognostic Value of C-Reactive Protein and Albumin in Neurocritically Ill Patients with Acute Stroke" Journal of Clinical Medicine 11, no. 17: 5067. https://doi.org/10.3390/jcm11175067
APA StyleJang, J. H., Hong, S., & Ryu, J.-A. (2022). Prognostic Value of C-Reactive Protein and Albumin in Neurocritically Ill Patients with Acute Stroke. Journal of Clinical Medicine, 11(17), 5067. https://doi.org/10.3390/jcm11175067