
Switching to Glycerol Phenylbutyrate in 48 Patients with Urea Cycle Disorders: Clinical Experience in Spain


 , , , , , , , , ,
, , , , , , , , ,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Endpoints and Variables
2.3. Statistical Analysis
3. Results
3.1. Demographics and Baseline Characteristics of the Series
3.2. Early Switching to GPB (T0 to T1)
3.3. Comparative Study after One Year of GPB Treatment (T0 to T2)
3.3.1. GPB Dosage
3.3.2. Anthropometric Values, Dietary Parameters and BCAA Levels
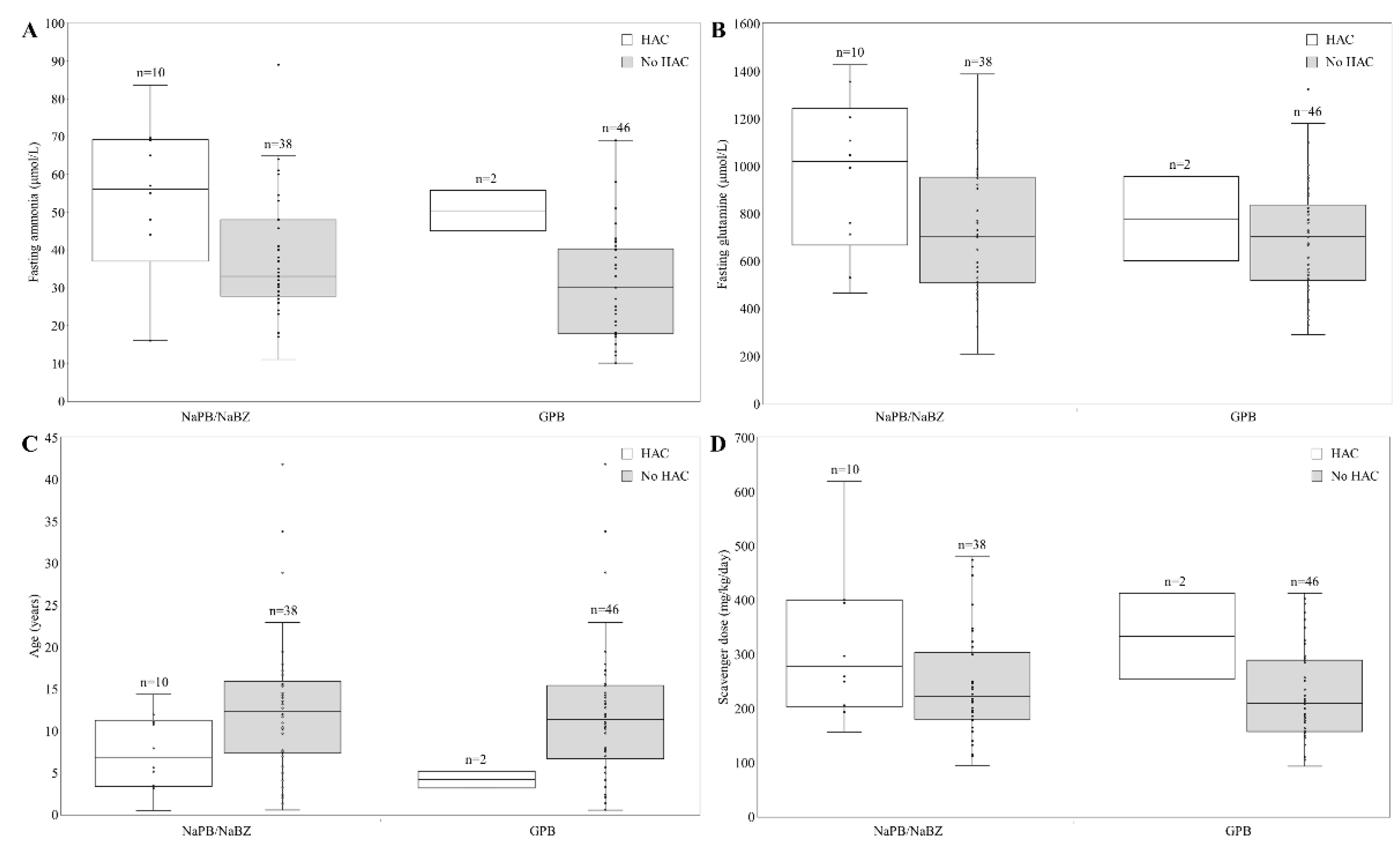
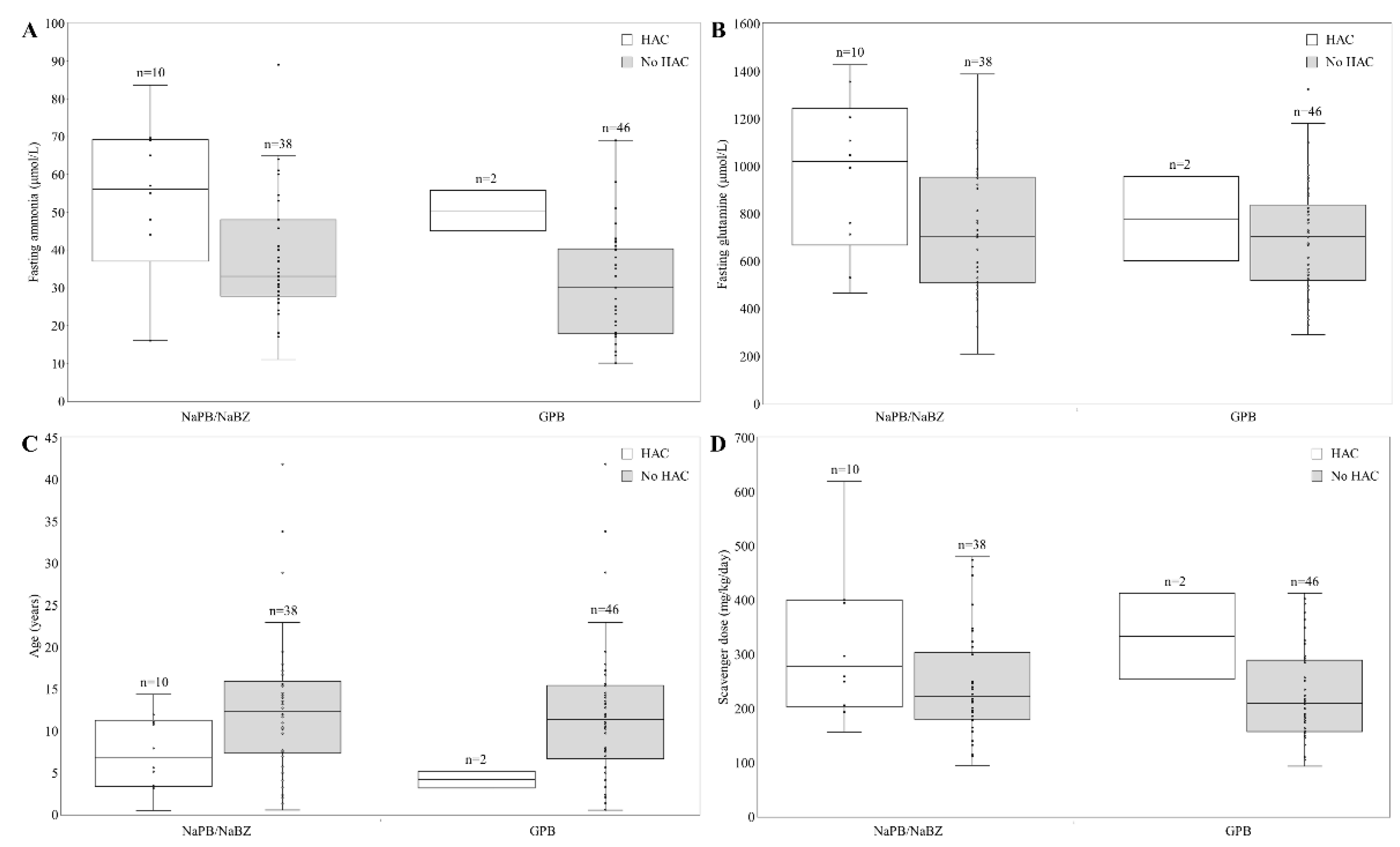
3.3.3. Ammonia, Glutamine and HAC
3.3.4. RAE and Drug Preference
3.3.5. U-PAG
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ah Mew, N.; Simpson, K.L.; Gropman, A.L.; Lanpher, B.C.; Chapman, K.A.; Summar, M.L. Urea Cycle Disorders Overview; GeneReviews® [Internet]; Pagon, R.A., Adam, M.P., Ardinger, H.H., Wallace, S.E., Amemiya, A., Bean, L.J.H., Bird, T.D., Dolan, C.R., Fong, C.T., Smith, R.J.H., et al., Eds.; University of Washington: Seattle, WA, USA, 2003; p. 1993. [Google Scholar]
- Summar, M.L.; Koelker, S.; Freedenberg, D.; Le Mons, C.; Häberle, J.; Lee, H.S.; Kirmse, B. The European Registry and Network for Intoxication Type Metabolic Diseases (E-IMD), and The Members of the Urea Cycle Disorders Consortium (UCDC). The incidence of urea cycle disorders. Mol. Genet. Metab. 2013, 110, 179–180. [Google Scholar] [CrossRef] [PubMed]
- Martín-Hernández, E.; Aldámiz-Echevarría, L.; Castejón-Ponce, E.; Pedrón-Giner, C.; Couce, M.L.; Serrano-Nieto, J.; Pintos-Morell, G.; Bélanger-Quintana, A.; Martínez-Pardo, M.; García-Silva, M.T.; et al. Urea cycle disorders in Spain: An observational, cross-sectional and multicentric study of 104 cases. Orphanet J. Rare Dis. 2014, 9, 187. [Google Scholar] [CrossRef] [PubMed]
- Häberle, J.; Burlina, A.; Chakrapani, A.; Dixon, M.; Karall, D.; Lindner, M.; Mandel, H.; Martinelli, D.; Pintos-Morell, G.; Santer, R.; et al. Suggested guidelines for the diagnosis and management of urea cycle disorders: First revision. J. Inherit. Metab. Dis. 2019, 42, 1192–1230. [Google Scholar] [CrossRef] [PubMed]
- Posset, R.; Gropman, A.L.; Nagamani, S.C.S.; Burrage, L.C.; Bedoyan, J.K.; Wong, D.; Berry, G.T.; Baumgartner, M.R.; Yudkoff, M.; Zielonka, M.; et al. Impact of diagnosis and therapy on cognitive function in urea cycle disorders. Ann. Neurol. 2019, 86, 116–128. [Google Scholar] [CrossRef]
- De Las Heras, J.; Aldámiz-Echevarría, L.; Martínez-Chantar, M.L.; Delgado, T. An update on the use of benzoate, phenylacetate and phenylbutyrate ammonia scavengers for interrogating and modifying liver nitrogen metabolism and its implications in urea cycle disorders and liver disease. Expert Opin. Drug Metab. Toxicol. 2017, 13, 439–448. [Google Scholar] [CrossRef]
- Nagamani, S.C.; Diaz, G.A.; Rhead, W.; Berry, S.A.; Le Mons, C.; Lichter-Konecki, U.; Bartley, J.; Feigenbaum, A.; Schulze, A.; Longo, N.; et al. Self-reported treatment-associated symptoms among patients with urea cycle disorders participating in glycerol phenylbutyrate clinical trials. Mol. Genet. Metab. 2015, 116, 29–34. [Google Scholar] [CrossRef]
- Longo, N.; Holt, R.J. Glycerol phenylbutyrate for the maintenance treatment of patients with deficiencies in enzymes of the urea cycle. Expert Opin. Orphan Drugs 2017, 5, 999–1010. [Google Scholar] [CrossRef]
- Monteleone, J.P.; Mokhtarani, M.; Diaz, G.A.; Rhead, W.; Lichter-Konecki, U.; Berry, S.A.; LeMons, C.; Dickinson, K.; Coakley, D.; Lee, B.; et al. Population Pharmacokinetic Modeling and Dosing Simulations of Nitrogen-Scavenging Compounds: Disposition of Glycerol Phenylbutyrate and Sodium Phenylbutyrate in Adult and Pediatric Patients with Urea Cycle Disorders. J. Clin. Pharmacol. 2013, 53, 699–710. [Google Scholar] [CrossRef]
- Lee, B.; Rhead, W.; Diaz, G.A.; Scharschmidt, B.F.; Mian, A.; Shchelochkov, O.; Marier, J.F.; Beliveau, M.; Mauney, J.; Dickinson, K.; et al. Phase 2 comparison of a novel ammonia scavenging agent with sodium phenylbutyrate in patients with urea cycle disorders: Safety, pharmacokinetics and ammonia control. Mol. Genet. Metab. 2010, 100, 221–228. [Google Scholar] [CrossRef]
- Lichter-Konecki, U.; Diaz, G.; Merritt, J.; Feigenbaum, A.; Jomphe, C.; Marier, J.; Beliveau, M.; Mauney, J.; Dickinson, K.; Martinez, A.; et al. Ammonia control in children with urea cycle disorders (UCDs); Phase 2 comparison of sodium phenylbutyrate and glycerol phenylbutyrate. Mol. Genet. Metab. 2011, 103, 323–329. [Google Scholar] [CrossRef] [Green Version]
- Smith, W.; Diaz, G.A.; Lichter-Konecki, U.; Berry, S.A.; Harding, C.O.; McCandless, S.E.; LeMons, C.; Mauney, J.; Dickinson, K.; Coakley, D.F.; et al. Ammonia Control in Children Ages 2 Months through 5 Years with Urea Cycle Disorders: Comparison of Sodium Phenylbutyrate and Glycerol Phenylbutyrate. J. Pediatr. 2013, 162, 1228–1234. [Google Scholar] [CrossRef] [PubMed]
- Diaz, G.A.; Krivitzky, L.S.; Mokhtarani, M.; Rhead, W.; Bartley, J.; Feigenbaum, A.; Longo, N.; Berquist, W.; Berry, S.; Gallagher, R.; et al. Ammonia control and neurocognitive outcome among urea cycle disorder patients treated with glycerol phenylbutyrate. Hepatology 2013, 57, 2171–2179. [Google Scholar] [CrossRef] [PubMed]
- Berry, S.A.; Lichter-Konecki, U.; Diaz, G.A.; McCandless, S.E.; Rhead, W.; Smith, W.; LeMons, C.; Nagamani, S.C.; Coakley, D.F.; Mokhtarani, M.; et al. Glycerol phenylbutyrate treatment in children with urea cycle disorders: Pooled analysis of short and long-term ammonia control and outcomes. Mol. Genet. Metab. 2014, 112, 17–24. [Google Scholar] [CrossRef]
- Berry, S.A.; Longo, N.; Diaz, G.A.; McCandless, S.E.; Smith, W.E.; Harding, C.O.; Zori, R.; Ficicioglu, C.; Lichter-Konecki, U.; Robinson, B.; et al. Safety and efficacy of glycerol phenylbutyrate for management of urea cycle disorders in patients aged 2 months to 2 years. Mol. Genet. Metab. 2017, 122, 46–53. [Google Scholar] [CrossRef]
- Diaz, G.A.; Schulze, A.; Longo, N.; Rhead, W.; Feigenbaum, A.; Wong, D.; Merritt, J.L.; Berquist, W.; Gallagher, R.C.; Bartholomew, D.; et al. Long-term safety and efficacy of glycerol phenylbutyrate for the management of urea cycle disorder patients. Mol. Genet. Metab. 2019, 127, 336–345. [Google Scholar] [CrossRef] [PubMed]
- Longo, N.; Diaz, G.A.; Lichter-Konecki, U.; Schulze, A.; Inbar-Feigenberg, M.; Conway, R.L.; Bannick, A.A.; McCandless, S.E.; Zori, R.; Hainline, B.; et al. Glycerol phenylbutyrate efficacy and safety from an open label study in pediatric patients under 2 months of age with urea cycle disorders. Mol. Genet. Metab. 2021, 132, 19–26. [Google Scholar] [CrossRef]
- U.S. Food and Drugs Administration (FDA). Drug Approval Pachage RAVICTI. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2013/203284orig1s000toc.cfm (accessed on 24 May 2022).
- European Medicines Agency (EMA). Drug Approval RAVICTI. 2019. Available online: https://www.ema.europa.eu/en/documents/overview/ravicti-epar-summary-public_es.pdf (accessed on 24 May 2022).
- Laemmle, A.; Stricker, T.; Häberle, J. Switch from Sodium Phenylbutyrate to Glycerol Phenylbutyrate Improved Metabolic Stability in an Adolescent with Ornithine Transcarbamylase Deficiency. JIMD Rep. 2016, 31, 11–14. [Google Scholar] [CrossRef]
- Yeo, M.; Rehsi, P.; Dorman, M.; Grunewald, S.; Baruteau, J.; Chakrapani, A.; Footitt, E.; Prunty, H.; McSweeney, M. Direct replacement of oral sodium benzoate with glycerol phenylbutyrate in children with urea cycle disorders. JIMD Rep. 2022, 63, 137–145. [Google Scholar] [CrossRef]
- Mokhtarani, M.; Diaz, G.; Rhead, W.; Lichter-Konecki, U.; Bartley, J.; Feigenbaum, A.; Longo, N.; Berquist, W.; Berry, S.; Gallagher, R.; et al. Urinary phenylacetylglutamine as dosing biomarker for patients with urea cycle disorders. Mol. Genet. Metab. 2012, 107, 308–314. [Google Scholar] [CrossRef]
- Sociedad Española de Gastroenterología, Hepatología y Nutrición pediátrica (SEGHNP). Available online: http://www.seghnp.org (accessed on 24 May 2022).
- Fernández, C.; Lorenzo, H.; Vrotsou, K.; Aresti, U.; Rica, I.; Sánchez, E.; Estudio de Crecimiento de Bilbao. Curvas y Tablas de Crecimiento (Estudio Transversal). 2011. Available online: http://www.fundacionorbegozo.com/el-instituto-de-investigacion-del-crecimiento-y-desarrollo/graficas-y-tablas/ (accessed on 24 May 2022).
- Ravicti (Glycerol Phenylbutyrate). Summary of Product Characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/ravicti-epar-product-information_en.pdf (accessed on 24 May 2022).
- Hook, D.; Diaz, G.A.; Lee, B.; Bartley, J.; Longo, N.; Berquist, W.; Le Mons, C.; Rudolph-Angelich, I.; Porter, M.; Scharschmidt, B.F.; et al. Protein and calorie intakes in adult and pediatric subjects with urea cycle disorders participating in clinical trials of glycerol phenylbutyrate. Mol. Genet. Metab. Rep. 2016, 6, 34–40. [Google Scholar] [CrossRef]
- Burrage, L.C.; Jain, M.; Gandolfo, L.; Lee, B.H.; Nagamani, S.C.; Urea Cycle Disorders Consortium. Sodium phenylbutyrate decreases plasma branched-chain amino acids in patients with urea cycle disorders. Mol. Genet. Metab. 2014, 113, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.; Diaz, G.A.; Rhead, W.; Lichter-Konecki, U.; Feigenbaum, A.; Berry, S.A.; Le Mons, C.; Bartley, J.A.; Longo, N.; Nagamani, S.C.; et al. Blood ammonia and glutamine as predictors of hyperammonemic crises in patients with urea cycle disorder. Genet. Med. 2014, 17, 561–568. [Google Scholar] [CrossRef] [PubMed]
- Kent, J.D.; Holt, R.J. Hyperammonemic crises in patients with urea cycle disorders on chronic nitrogen scavenger therapy with either sodium phenylbutyrate or glycerol phenylbutyrate. Neuropsychiatry 2017, 7, 131–136. [Google Scholar] [CrossRef]
- Lee, B.; Diaz, G.; Rhead, W.; Lichter-Konecki, U.; Feigenbaum, A.; Berry, S.; Le Mons, C.; Bartley, J.; Longo, N.; Nagamani, S.; et al. Glutamine and hyperammonemic crises in patients with urea cycle disorders. Mol. Genet. Metab. 2016, 117, 27–32. [Google Scholar] [CrossRef]
- Yeowell, G.; Burns, D.S.; Fataoye, F. The burden of pharmacological treatment on health related quality of life in people with urea cycle disorders: A qualitative study. J. Patient-Rep. Outcomes 2021, 5, 110. [Google Scholar] [CrossRef]
- Mokhtarani, M.; Diaz, G.; Lichter-Konecki, U.; Berry, S.; Bartley, J.; McCandless, S.; Smith, W.; Harding, C.; Le Mons, C.; Coakley, D.; et al. Urinary phenylacetylglutamine (U-PAGN) concentration as biomarker for adherence in patients with urea cycle disorders (UCD) treated with glycerol phenylbutyrate. Mol. Genet. Metab. Rep. 2015, 5, 12–14. [Google Scholar] [CrossRef]
- Andrade, F.; Vitoria, I.; Martín-Hernández, E.; Pintos-Morell, G.; Correcher, P.; Puig, R.; Quijada-Fraile, P.; Peña-Quintana, L.; Marquez, A.M.; Villate, O.; et al. Quantification of urinary derivatives of Phenylbutyric and Benzoic acids by LC-MS/MS as treatment compliance biomarkers in Urea Cycle disorders. J. Pharm. Biomed. Anal. 2019, 176, 112798. [Google Scholar] [CrossRef]
- Peña-Quintana, L.; Llarena, M.; Reyes-Suárez, D.; Aldámiz-Echevarria, L. Profile of sodium phenylbutyrate granules for the treatment of urea-cycle disorders: Patient perspectives. Patient Prefer. Adherence 2017, 11, 1489–1496. [Google Scholar]
- Canadian Agency for Drugs and Technologies in Health. Glycerol Phenylbutyrate (Ravicti); Canadian Agency for Drugs and Technologies in Health: Ottawa, ON, Canada, 2017. [Google Scholar]

{kind=link}
| Patients (n = 48) | |
|---|---|
| Gender, n (%) | |
| Male | 19 (39.6) |
| Female | 29 (60.4) |
| Age at treatment switching to GPB, years (SD) | 11.7 (8.2) |
| Height, z-score (SD) | −1.04 (1.5) |
| Weight, z-score (SD) | −0.34 (1.2) |
| UCD diagnosis, n (%) | |
| Ornithine transcarbamylase deficiency | 27 (56.2) |
| Arginosuccinate lyase deficiency | 9 (18.7) |
| Arginosuccinate synthetase1 deficiency | 8 (16.6) |
| Carbamylphosphate synthetase1 deficiency | 3 (6.2) |
| Arginase 1 deficiency | 1 (2.1) |
| UCD Onset, n (%) | |
| Neonatal | 19 (39.6) |
| Late | 26 (54.2) |
| Asymptomatic (screening/high risk) | 3 (6.2) |
| Previous scavenger, n (%) | |
| NaPB | 46 (95.8) |
| NaBZ | 2 (4.2) |
| NaPB/NaBZ | GPB | p | |
|---|---|---|---|
| Dose, mg/kg/day (SD) | 262.6 (126.1) | 247.8 (102.1) | 0.25 |
| Ammonia, μmol/L (SD) | 40.2 (17.3) | 32.5 (13.9) | <0.001 |
| Glutamine, μmol/L (SD) | 791.4 (289.8) | 648.6 (247.4) | <0.001 |
| n | T0 | T2 | p | |
|---|---|---|---|---|
| Weight, z-score (SD) | 48 | −0.3 (1.2) | −0.4 (1.1) | NS |
| Height, z-score (SD) | 47 | −1.0 (1.4) | −1.0 (1.4) | NS |
| Cranial perimeter, z-score (SD) | 13 | −1.0 (0.9) | −0.7 (1.3) | NS |
| Total proteins, g/kg/day (SD) | 48 | 0.8 (0.3) | 0.8 (0.3) | NS |
| Age group, years (SD) | ||||
| <2 | 3 | 1.1 (0.3) | 1.1 (0.1) | NS |
| 2–5 | 10 | 0.9 (0.3) | 1.0 (0.3) | NS |
| 6–11 | 15 | 0.8 (0.3) | 0.7 (0.2) | NS |
| 12–17 | 15 | 0.7 (0.2) | 0.8 (0.2) | NS |
| >18 | 5 | 0.7 (0.3) | 0.7 (0.2) | NS |
| EAA, g/kg/day (SD) | 30 | 0.3 (0.2) | 0.3 (0.2) | NS |
| BCAA levels,µmol/L (SD) | ||||
| Leucine (50–150) | 75.5 (25.3) | 83.2 (22.6) | 0.038 | |
| Isoleucine (30–85) | 40.1 (15.8) | 44.7 (15.3) | NS | |
| Valine (130–300) | 133.4 (36.0) | 149.6 (36.1) | 0.002 |
| T0 | T2 | p | |
|---|---|---|---|
| Ammonia, μmol/L (SD) | 40.23 (17.29) | 31.22 (14.83) | <0.001 |
| Glutamine, μmol/L (SD) | 791.42 (289.80) | 700.35 (234.43) | 0.017 |
| HAC/year/patient (SD) | 0.31 (0.68) | 0.06 (0.32) | 0.02 |
| NaPB (n = 46) | GPB (n = 48) | |
|---|---|---|
| Gastrointestinal disorders | ||
| Abdominal pain | 5 | |
| Abdominal distension | 4 | |
| Vomiting | 2 | |
| Constipation | 4 | |
| Oral discomfort | 2 | |
| Dysgeusia | 2 | |
| Dyspepsia | 1 | |
| Decreased appetite | 1 | |
| Other symptoms | ||
| Body odour | 1 | |
| Poor weight gain | 1 | |
| Dizziness | 1 | |
| Hair thinning | 1 | |
| Laboratory abnormalities (including blood count and functions of vital organs) | ||
| Hypertransaminasemia | 2 | |
| Total events | 25 | 2 |
| Total patients | 10 (21.7%) | 2 (4.1%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martín-Hernández, E.; Quijada-Fraile, P.; Correcher, P.; Meavilla, S.; Sánchez-Pintos, P.; de las Heras Montero, J.; Blasco-Alonso, J.; Dougherty, L.; Marquez, A.; Peña-Quintana, L.; et al. Switching to Glycerol Phenylbutyrate in 48 Patients with Urea Cycle Disorders: Clinical Experience in Spain. J. Clin. Med. 2022, 11, 5045. https://doi.org/10.3390/jcm11175045
Martín-Hernández E, Quijada-Fraile P, Correcher P, Meavilla S, Sánchez-Pintos P, de las Heras Montero J, Blasco-Alonso J, Dougherty L, Marquez A, Peña-Quintana L, et al. Switching to Glycerol Phenylbutyrate in 48 Patients with Urea Cycle Disorders: Clinical Experience in Spain. Journal of Clinical Medicine. 2022; 11(17):5045. https://doi.org/10.3390/jcm11175045
Chicago/Turabian StyleMartín-Hernández, Elena, Pilar Quijada-Fraile, Patricia Correcher, Silvia Meavilla, Paula Sánchez-Pintos, Javier de las Heras Montero, Javier Blasco-Alonso, Lucy Dougherty, Ana Marquez, Luis Peña-Quintana, and et al. 2022. "Switching to Glycerol Phenylbutyrate in 48 Patients with Urea Cycle Disorders: Clinical Experience in Spain" Journal of Clinical Medicine 11, no. 17: 5045. https://doi.org/10.3390/jcm11175045
APA StyleMartín-Hernández, E., Quijada-Fraile, P., Correcher, P., Meavilla, S., Sánchez-Pintos, P., de las Heras Montero, J., Blasco-Alonso, J., Dougherty, L., Marquez, A., Peña-Quintana, L., Cañedo, E., García-Jimenez, M. C., Moreno Lozano, P. J., Murray Hurtado, M., Camprodon Gómez, M., Barrio-Carreras, D., de los Santos, M., del Toro, M., Couce, M. L., ... Bellusci, M. (2022). Switching to Glycerol Phenylbutyrate in 48 Patients with Urea Cycle Disorders: Clinical Experience in Spain. Journal of Clinical Medicine, 11(17), 5045. https://doi.org/10.3390/jcm11175045