
Decrease in Bone Formation and Bone Resorption during Intravenous Methylprednisolone Pulse Therapy in Patients with Graves’ Orbitopathy

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
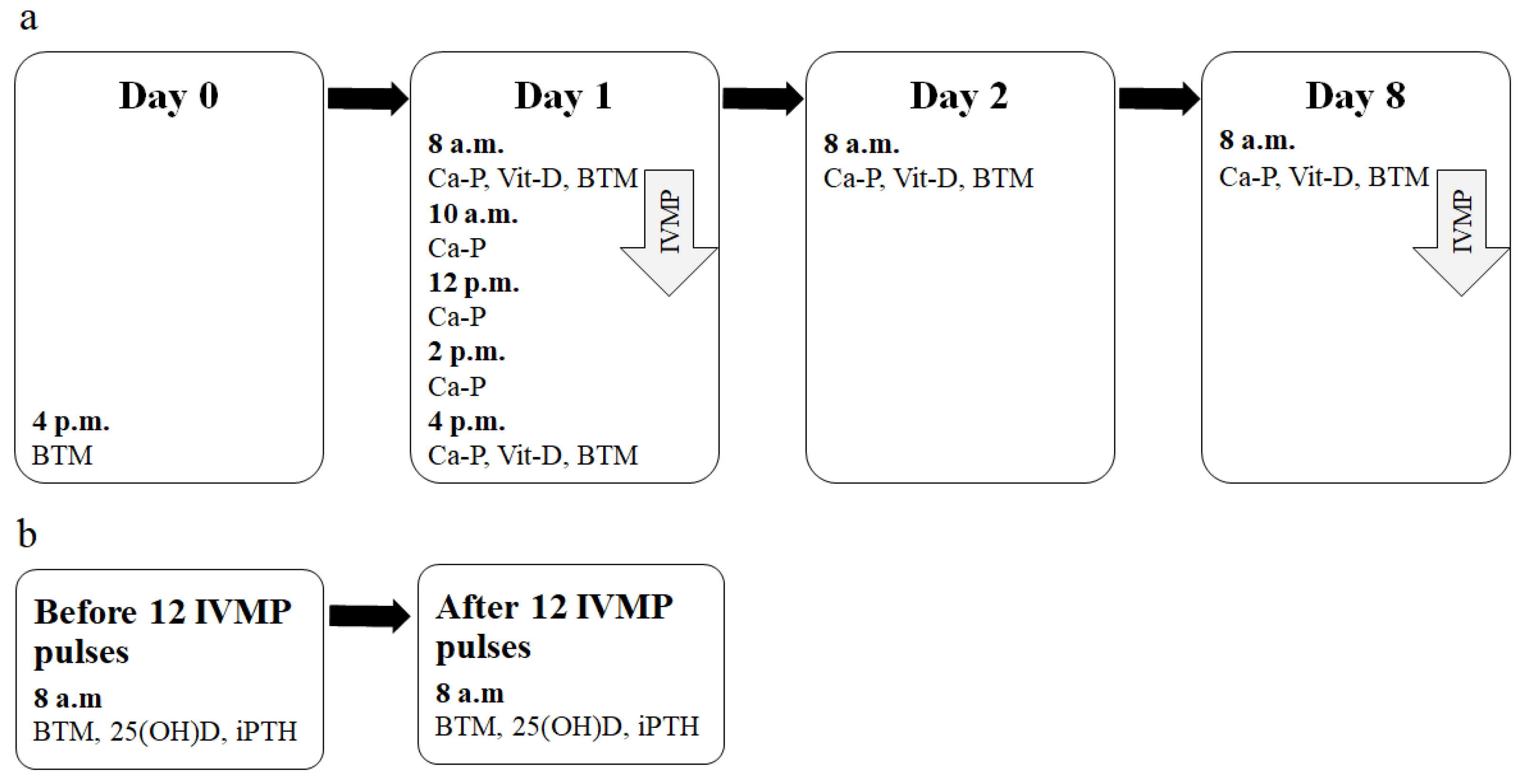
2.2. Study Design
2.3. Biochemical Evaluation
2.4. BMD Evaluation
2.5. Statistical Methods
3. Results
3.1. Markers of Bone Turnover and Calcium Metabolism Parameters at Baseline
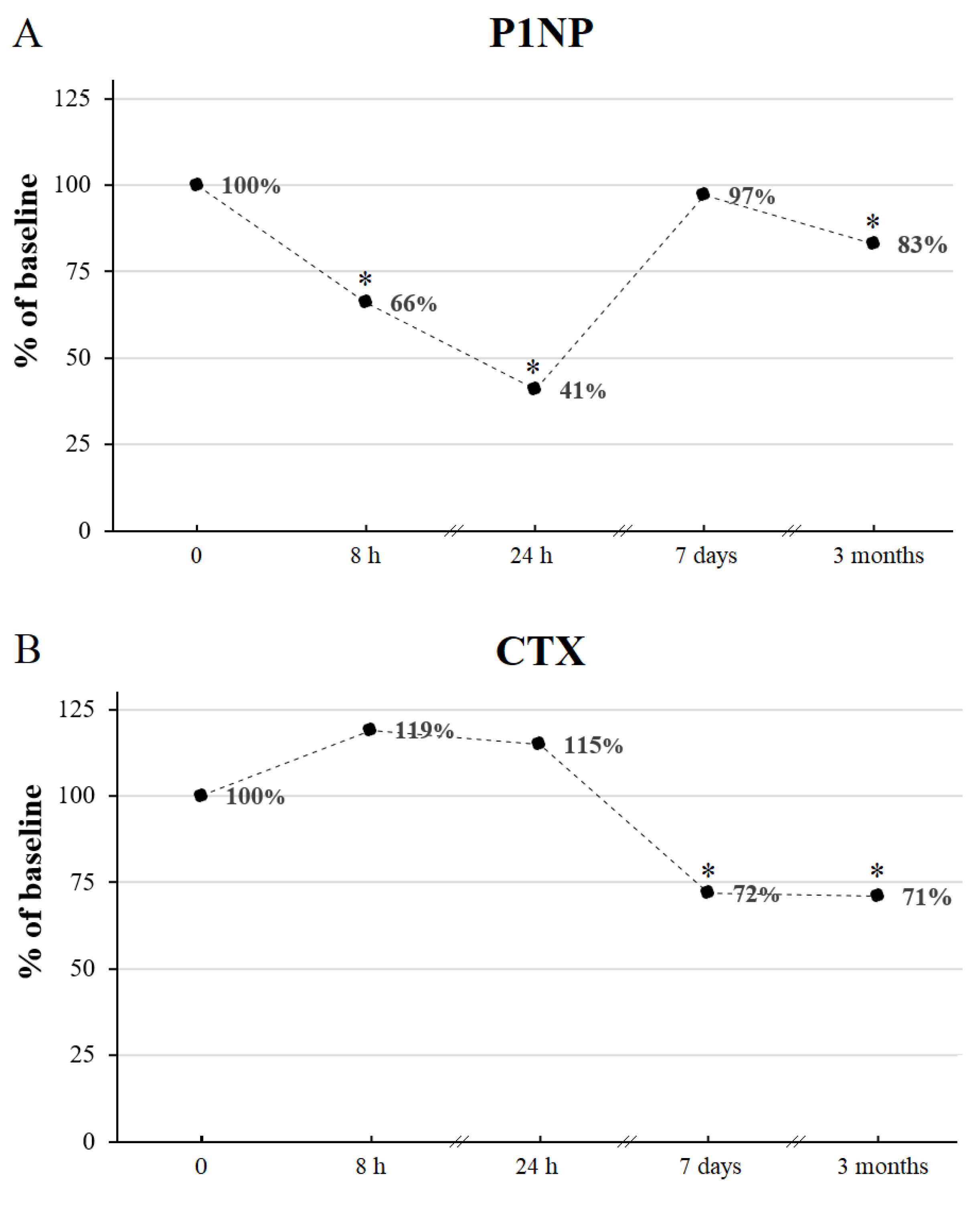
3.2. Early Effects of a Single Dose of 0.5 G IVMP on BTM
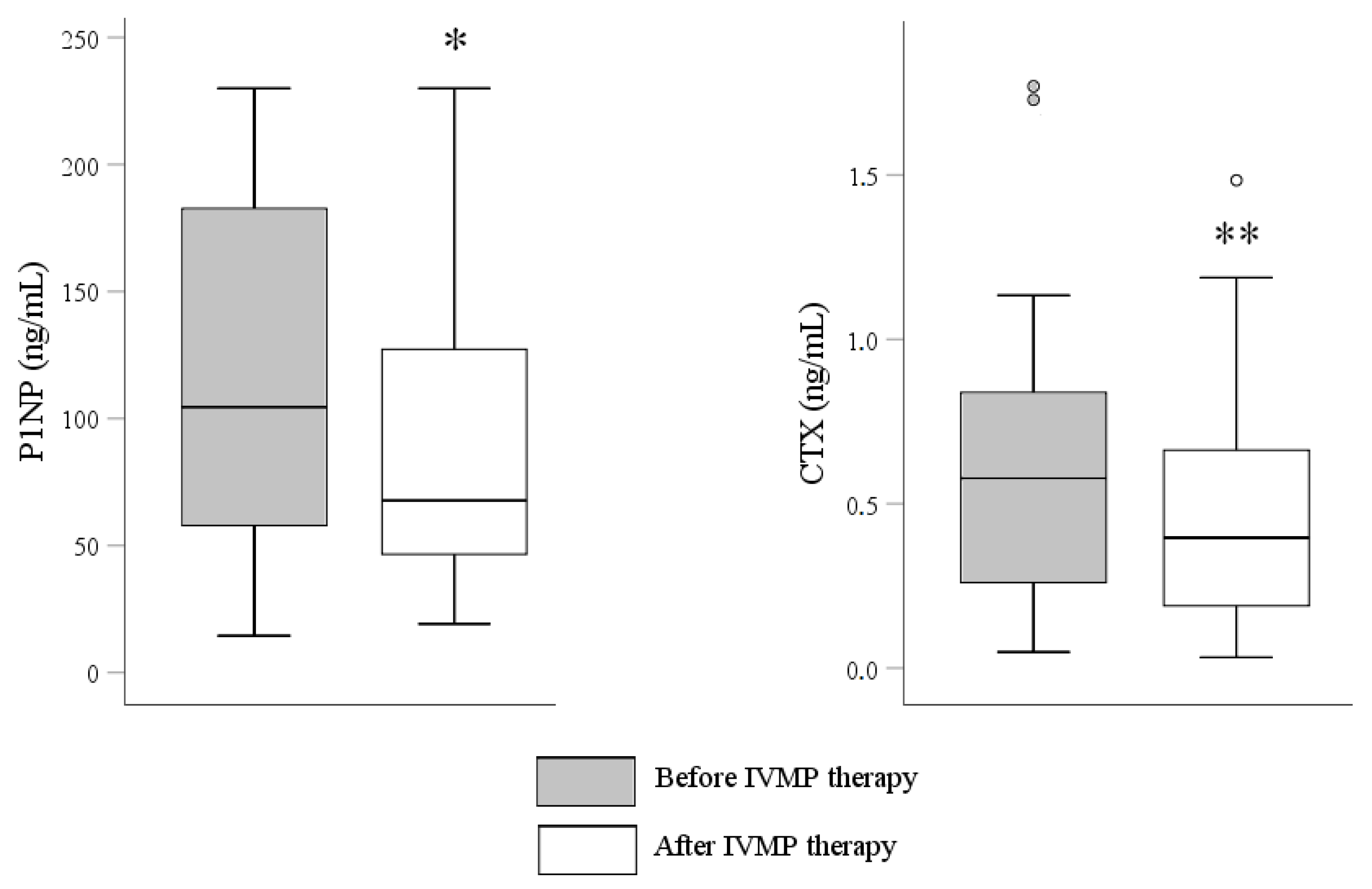
3.3. The Influence of the Full Course of IVMP Pulse Therapy on BTM and Calcium Metabolism Parameters
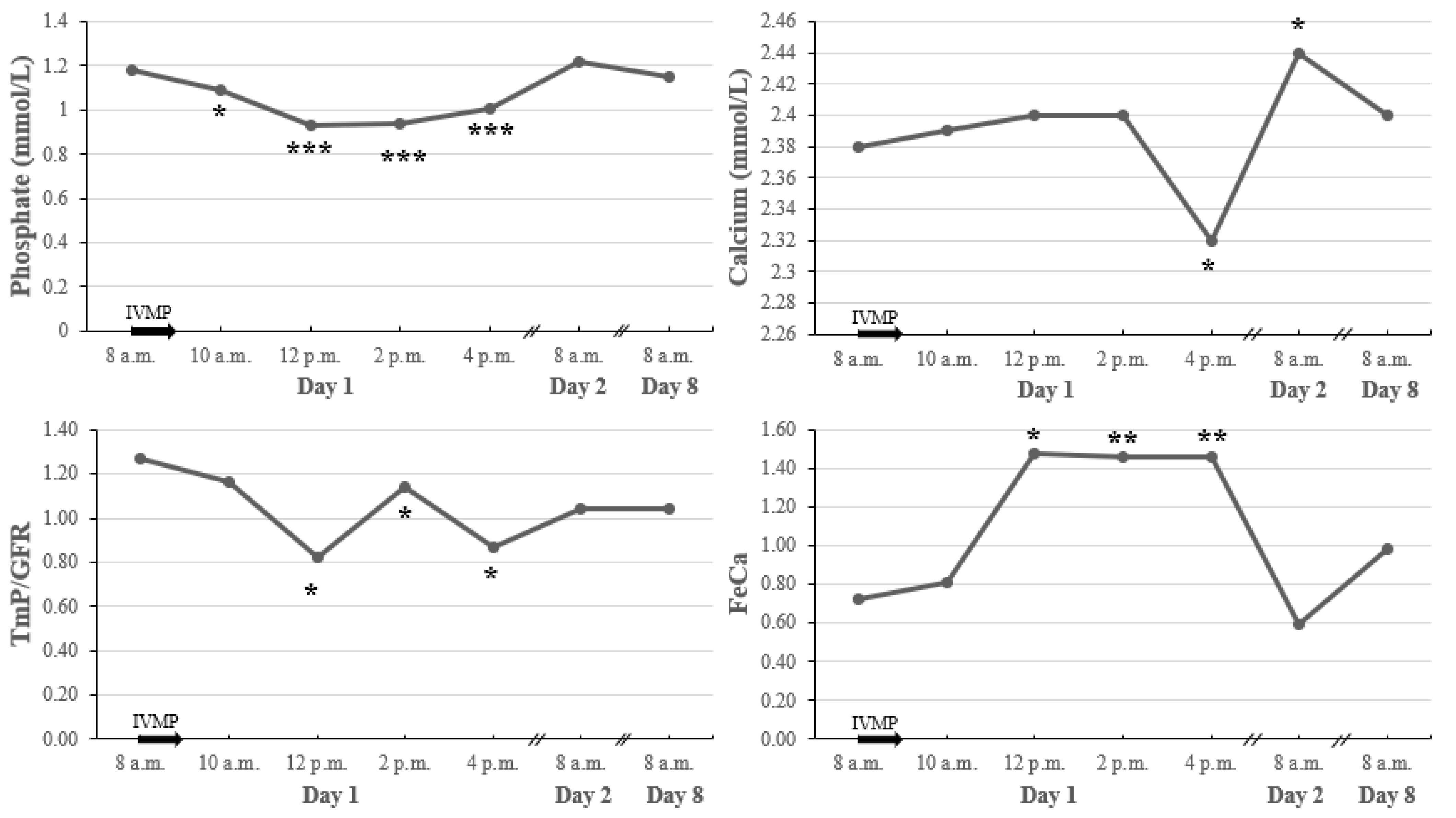
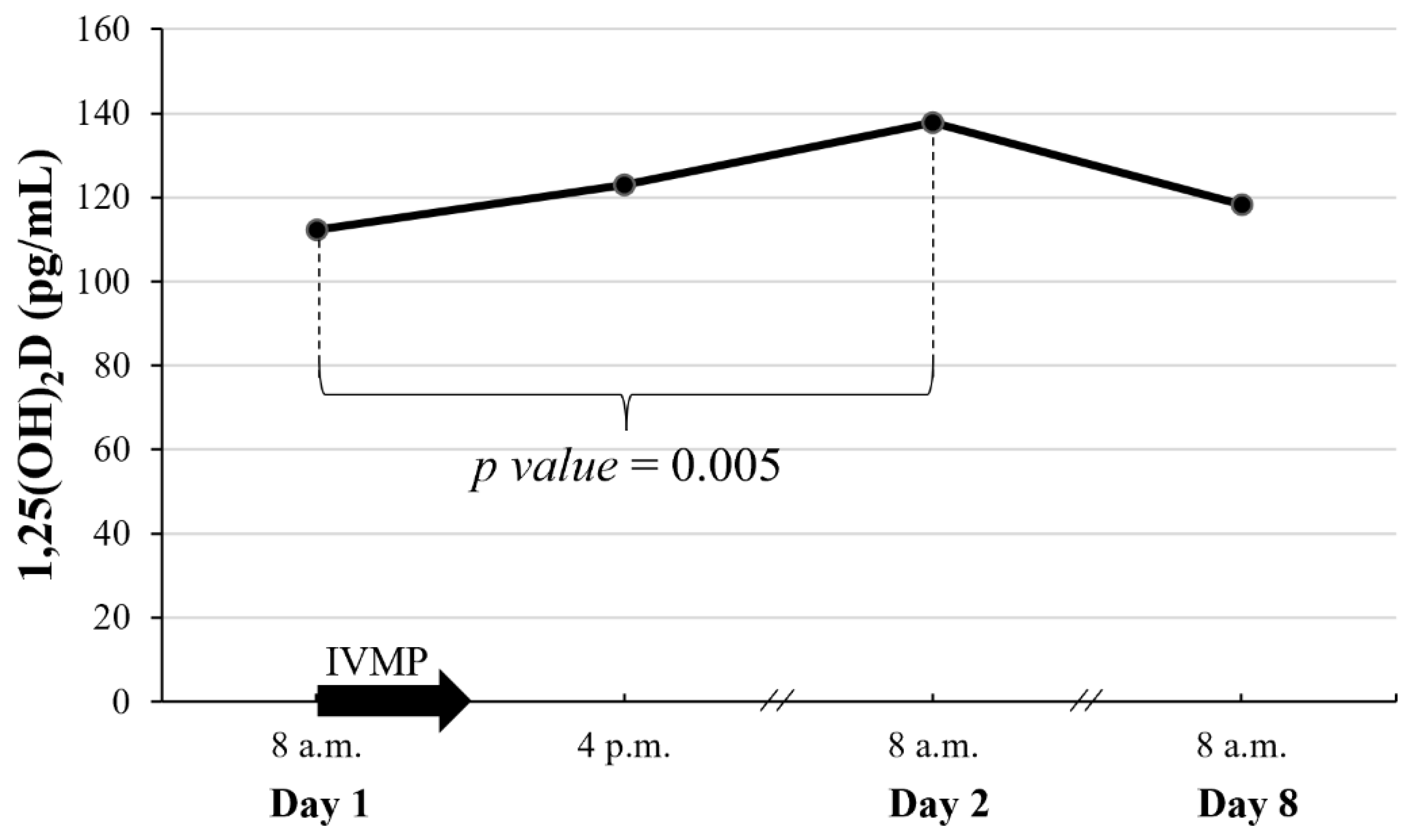
3.4. Early Effects of a Single Dose of 0.5 G IVMP on Calcium Metabolism Parameters and 1,25(OH)2D
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Bartalena, L.; Kahaly, G.J.; Baldeschi, L.; Dayan, C.M.; Eckstein, A.; Marcocci, C.; Marinò, M.; Vaidya, B.; Wiersinga, W.M.; EUGOGO. The 2021 European Group on Graves’ orbitopathy (EUGOGO) clinical practice guidelines for the medical management of Graves’ orbitopathy. Eur. J. Endocrinol. 2021, 4, G43–G67. [Google Scholar] [CrossRef] [PubMed]
- Miśkiewicz, P.; Kryczka, A.; Ambroziak, U.; Rutkowska, B.; Główczyńska, R.; Opolski, G.; Kahaly, G.; Bednarczuk, T. Is high dose intravenous methylprednisolone pulse therapy in patients with Graves’ orbitopathy safe? Endokrynol. Pol. 2014, 5, 402–413. [Google Scholar] [CrossRef] [PubMed]
- Pelewicz, K.; Szewczyk, S.; Miśkiewicz, P. Treatment with Intravenous Methylprednisolone in Patients with Graves’ Orbitopathy Significantly Affects Adrenal Function: Assessment of Serum, Salivary Cortisol and Serum Dehydroepiandrosterone Sulfate. J. Clin. Med. 2020, 10, 3233. [Google Scholar] [CrossRef] [PubMed]
- Miśkiewicz, P.; Jankowska, A.; Brodzińska, K.; Milczarek-Banach, J.; Ambroziak, U. Influence of Methylprednisolone Pulse Therapy on Liver Function in Patients with Graves’ Orbitopathy. Int. J. Endocrinol. 2018, 21, 1978590. [Google Scholar] [CrossRef]
- Miśkiewicz, P.; Milczarek-Banach, J.; Rutkowska-Hinc, B.; Kondracka, A.; Bednarczuk, T. High-dose intravenous methylprednisolone therapy in patients with Graves’ orbitopathy is associated with the increased activity of factor VIII. J. Endocrinol. Investig. 2019, 2, 217–225. [Google Scholar] [CrossRef]
- Miskiewicz, P.; Milczarek-Banach, J.; Bednarczuk, T.; Opolski, G.; Glowczynska, R. Blood Pressure Profile and N-Terminal-proBNP Dynamics in Response to Intravenous Methylprednisolone Pulse Therapy of Severe Graves’ Orbitopathy. Int. J. Mol. Sci. 2018, 10, 2918. [Google Scholar] [CrossRef]
- Ton, F.N.; Gunawardene, S.C.; Lee, H.; Neer, R.M. Effects of low-dose prednisone on bone metabolism. J. Bone Miner. Res. 2005, 20, 464–470. [Google Scholar] [CrossRef]
- Kanis, J.A.; Johansson, H.; Oden, A.; Johnell, O.; de Laet, C.; Melton III, L.J.; Tenenhouse, A.; Reeve, J.; Silman, A.J.; Pols, H.A.; et al. A meta-analysis of prior corticosteroid use and fracture risk. J. Bone Miner. Res. 2004, 6, 893–899. [Google Scholar] [CrossRef]
- Jia, D.; O’Brien, C.A.; Stewart, S.A.; Manolagas, S.C.; Weinstein, R.S. Glucocorticoids act directly on osteoclasts to increase their life span and reduce bone density. Endocrinology 2006, 12, 5592–5599. [Google Scholar] [CrossRef]
- Weinstein, R.S.; Jilka, R.L.; Parfitt, A.M.; Manolagas, S.C. Inhibition of osteoblastogenesis and promotion of apoptosis of osteoblasts and osteocytes by glucocorticoids. Potential mechanisms of their deleterious effects on bone. J. Clin. Investig. 1998, 2, 274–282. [Google Scholar]
- Weinstein, R.S.; Roberson, P.K.; Manolagas, S.C. Giant osteoclast formation and long-term oral bisphosphonate therapy. N. Engl. J. Med. 2009, 1, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Van Staa, T.P. The pathogenesis, epidemiology and management of glucocorticoid-induced osteoporosis. Calcif. Tissue Int. 2006, 3, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Huybers, S.; Naber, T.H.; Bindels, R.J.; Hoenderop, J.G. Prednisolone-induced Ca2+ malabsorption is caused by diminished expression of the epithelial Ca2+ channel TRPV6. Am. J. Physiol. Gastrointest. Liver Physiol. 2007, 1, G92–G97. [Google Scholar] [CrossRef] [PubMed]
- Canalis, E.; Mazziotti, G.; Giustina, A.; Bilezikian, J.P. Glucocorticoid-induced osteoporosis: Pathophysiology and therapy. Osteoporos. Int. 2007, 10, 1319–1328. [Google Scholar] [CrossRef]
- Hu, Y.X.; Zheng, R.D.; Fan, Y.F.; Sun, L.; Hu, X.; Liu, C. The effects of bone metabolism in different methylprednisolone pulse treatments for Graves’ ophthalmopathy. Exp. Ther. Med. 2020, 1, 333–338. [Google Scholar] [CrossRef]
- Censi, S.; Manso, J.; Pandolfo, G.; Franceschet, G.; Cavedon, E.; Zhu, Y.H.; Carducci, S.; Gomiero, W.; Plebani, M.; Zaninotto, M.; et al. Bone turnover markers, BMD and TBS after short-term, high-dose glucocorticoid therapy in patients with Graves’ orbitopathy: A small prospective pilot study. J. Endocrinol. Investig. 2019, 7, 859–865. [Google Scholar] [CrossRef]
- Rymuza, J.; Popow, M.; Żurecka, Z.; Przedlacki, J.; Bednarczuk, T.; Miśkiewicz, P. Therapy of moderate-to-severe Graves’ orbitopathy with intravenous methylprednisolone pulses is not associated with loss of bone mineral density. Endocrine 2019, 2, 308–315. [Google Scholar] [CrossRef]
- Gasińska, T.; Borowska, A.; Wichary, H.; Dec, R. Effect of methylprednisolone pulse therapy with and without alendronate on biochemical markers of bone turnover in patients with Graves’ ophthalmopathy. Pol. Arch. Med. Wewn. 2012, 7–8, 341–347. [Google Scholar] [CrossRef]
- Dovio, A.; Perazzolo, L.; Osella, G.; Ventura, M.; Termine, A.; Milano, E.; Bertolotto, A.; Angeli, A. Immediate fall of bone formation and transient increase of bone resorption in the course of high-dose, short-term glucocorticoid therapy in young patients with multiple sclerosis. J. Clin. Endocrinol. Metab. 2004, 10, 4923–4928. [Google Scholar] [CrossRef]
- Cosman, F.; Nieves, J.; Herbert, J.; Shen, V.; Lindsay, R. High-dose glucocorticoids in multiple sclerosis patients exert direct effects on the kidney and skeleton. J. Bone Miner. Res. 1994, 7, 1097–1105. [Google Scholar] [CrossRef]
- Kanis, J.A.; Cooper, C.; Rizzoli, R.; Reginster, J.Y. Scientific Advisory Board of the European Society for Clinical and Economic Aspects of Osteoporosis (ESCEO) and the Committees of Scientific Advisors and National Societies of the International Osteoporosis Foundation (IOF). European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos. Int. 2019, 1, 3–44. [Google Scholar]
- Ekenstam, E.; Stålenheim, G.; Hällgren, R. The acute effect of high dose corticosteroid treatment on serum osteocalcin. Metabolism 1988, 2, 141–144. [Google Scholar] [CrossRef]
- Peretz, A.; Moris, M.; Willems, D.; Bergmann, P. Is bone alkaline phosphatase an adequate marker of bone metabolism during acute corticosteroid treatment? Clin. Chem. 1996, 1, 102–103. [Google Scholar] [CrossRef]
- Ardissone, P.; Rota, E.; Durelli, L.; Limone, P.; Isaia, G.C. Effects of high doses of corticosteroids on bone metabolism. J. Endocrinol. Investig. 2002, 2, 129–133. [Google Scholar] [CrossRef]
- Chen, X.; Abudukerimu, B.; Li, Q. Influence of 4-week or 12-week glucocorticoid treatment on metabolic changes in patients with active moderate-to-severe thyroid-associated ophthalmopathy. Clin. Trans. 2021, 14, 1734–1746. [Google Scholar] [CrossRef]
- Płudowski, P.; Karczmarewicz, E.; Bayer, M.; Carter, G.; Chlebna-Sokół, D.; Czech-Kowalska, J.; Dębski, R.; Decsi, T.; Dobrzańska, A.; Franek, E.; et al. Practical guidelines for the supplementation of vitamin D and the treatment of deficits in Central Europe—recommended vitamin D intakes in the general population and groups at risk of vitamin D deficiency. Endokrynol. Pol. 2013, 4, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Wheater, G.; Elshahaly, M.; Tuck, S.P.; Datta, H.K.; van Laar, J.M. The clinical utility of bone marker measurements in osteoporosis. J. Transl. Med. 2013, 11, 201. [Google Scholar] [CrossRef]
- Raisz, L.; Trummel, C.; Wener, J.; Simmons, H. Effect of glucocorticoids on bone resorption in tissue culture. Endocrinology 1972, 90, 961–967. [Google Scholar] [CrossRef]
- Lukert, B.P.; Raisz, L.G. Glucocorticoid-induced osteoporosis: Pathogenesis and management. Ann. Intern. Med. 1990, 5, 352–364. [Google Scholar] [CrossRef]
- Van der Veen, M.J.; Bijlsma, J.W. Effects of different regimes of corticosteroid treatment on calcium and bone metabolism in rheumatoid arthritis. Clin. Rheumatol. 1992, 3, 388–392. [Google Scholar] [CrossRef]
- Levi, M.; Shayman, J.A.; Abe, A.; Gross, S.K.; McCluer, R.H.; Biber, J.; Murer, H.; Lötscher, M.; Cronin, R.E. Dexamethasone modulates rat renal brush border membrane phosphate transporter mRNA and protein abundance and glycosphingolipid composition. J. Clin. Investig. 1995, 1, 207–216. [Google Scholar] [CrossRef]
- Ferrari, P. Cortisol and the renal handling of electrolytes: Role in glucocorticoid-induced hypertension and bone disease. Best Pract. Res. Clin. Endocrinol. Metab. 2003, 4, 575–589. [Google Scholar] [CrossRef]
- Christakos, S.; Dhawan, P.; Verstuyf, A.; Verlinden, L.; Carmeliet, G. Vitamin D: Metabolism, Molecular Mechanism of Action, and Pleiotropic Effects. Physiol. Rev. 2016, 1, 365–408. [Google Scholar] [CrossRef] [PubMed]
- Rymuza, J.; Popow, M.; Bednarczuk, T.; Miśkiewicz, P. High dose intravenous methylprednisolone pulse therapy causes transient increase of serum calcium and phosphate levels. Pol. Merkur. Lekarski 2019, 279, 91–94. [Google Scholar]
- Garnero, P.; Vassy, V.; Bertholin, A.; Riou, J.P.; Delmas, P.D. Markers of bone turnover in hyperthyroidism and the effects of treatment. J. Clin. Endocrinol. Metab. 1994, 4, 955–959. [Google Scholar]
- Nagasaka, S.; Sugimoto, H.; Nakamura, T.; Kusaka, I.; Fujisawa, G.; Sakuma, N.; Tsuboi, Y.; Fukuda, S.; Honda, K.; Okada, K.; et al. Antithyroid therapy improves bony manifestations and bone metabolic markers in patients with Graves’ thyrotoxicosis. Clin. Endocrinol. 1997, 2, 215–221. [Google Scholar] [CrossRef]
- Rajaii, F.; McCoy, A.N.; Smith, T.J. Cytokines are both villains and potential therapeutic targets in thyroid-associated ophthalmopathy: From bench to bedside. Expert Rev. Ophthalmol. 2014, 3, 227–234. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Number of Patients (%) or Mean ± SD (Range) |
|---|---|
| Age (years) | 54 ± 12 (31 ÷ 74) |
| Female sex | 20 (87%) |
| Postmenopausal women | 11 (55%) |
| Body mass index (kg/m2) | 26.5 ± 6.2 (17.1 ÷ 41.3) |
| Thyroid disease | |
| Graves’ disease treated for hyperthyroidism | 15 (65%) |
| Graves’ disease after radical treatment | 6 (26%) |
| Hashimoto thyroiditis on levothyroxine | 2 (9%) |
| Duration of treatment with antithyroid drugs before IVMP therapy 1 (month) | 10.0 ± 5.0 (3 ÷ 18) |
| TSH (normal range: 0.27–4.2 µIU/mL) | 1.5 ± 1.5 (0.005 ÷ 3.9) |
| fT4 (normal range: 12.0–22.0 pmol/L) | 16.2 ± 4.2 (12.2 ÷ 22.0) |
| fT3 (normal range: 3.1–6.8 pmol/L) | 4.6 ± 0.9 (3.1 ÷ 6.6) |
| TRAB (normal range: <1.75 IU/L) | 17.6 ± 12.4 (2.8 ÷ 40) |
| 25(OH)D | 28.0 ± 9.5 (7.2 ÷ 57.0) |
| Deficiency | 3 (13%) |
| Suboptimal | 9 (39%) |
| Optimal | 11 (48%) |
| P1NP (normal range: 27.7–127.6 ng/mL) | 121.2 ± 67.02 (14.4 ÷ 230.0) |
| CTX (normal range: 0.038–0.724 ng/mL in men, 0.034–0.635 ng/mL in premenopausal women, 0.034–1.037 ng/mL in postmenopausal women) | 0.7 ± 0.5 (0.05 ÷ 1.8) |
| iPTH (normal range: 15–65 pg/mL) | 44.9 ± 11.2 (23 ÷ 62.2) |
| Lumbar BMD at baseline | 1.0 ± 0.1 (0.8 ÷ 1.3) |
| Normal body mass | 16 (70%) |
| Osteopenic | 7 (30%) |
| Femoral neck BMD at baseline | 0.7 ± 0.5 (−1.0 ÷ 1.4) |
| Normal body mass | 16 (70%) |
| Osteopenic | 7 (30%) |
| Variable | before IVMP | after IVMP | p Value |
|---|---|---|---|
| P1NP (ng/mL) | 114.6 ± 70.8 | 95.38 ± 70.85 | 0.04 |
| CTX (pg/mL) | 0.7 ± 0.5 | 0.5 ± 0.4 | 0.002 |
| 25(OH)D (ng/mL) | 29.9 ± 9.9 | 30.9 ± 8.3 | 0.49 |
| iPTH (pg/mL) | 45.1 ± 11.5 | 41.7 ± 6.4 | 0.18 |
| Study | Size of the Group (n) | Diagnosis | IVMP Regimen | BTM Evaluation | Results—Markers of Bone Formation | Results—Markers of Bone Resorption |
|---|---|---|---|---|---|---|
| Cosman [20] 1994 | 56 | MS | 1.0 g over 1 h daily for 10 days, 0.5 g/day for 2 days, 0.25 g/day for 2 days (cumulative dose 11.5 g) | In 9 pts: at baseline, after 1, 3, 5, 8 h, and then after 3 days and 2 weeks | Decrease of OC after 8 h persistent though the IVMP therapy | Increase of TRAP after 2 weeks |
| Peretz [23] 1996 | 7 | RD | 1.0 g over 30 min | At baseline and after 3, 6, 12, 24, 48, 72 h | Decrease of OC after 6, 24 h, Decrease of P1CP after 12 h | |
| Ardissone [24] 2002 | 23 | MS | 1.0 g daily for 10 days (cumulative dose 10.0 g) | At baseline, and after 3, 10, 30 days | Decrease of OC after 3 and 10 | |
| Dovio [19] 2004 | 13 | MS | 15 mg/kg daily for 10 days | At baseline and every day over 10 days, and then after 3 months | Decrease of OC and P1NP after 48 h, increase of BTM after 3 months | Increase of CTX after 1 week, and 3 months |
| Gasińska [18] 2012 | 30 | GO | 1.0 g twice a week over 4 weeks (cumulative dose 8.0 g) | At baseline and after 1 month | Decrease of OC and P1CP after 1 month | Decrease of ICTP after 1 month |
| Censi [16] 2018 | 11 | GO | In 6/11 pts: 0.5 g/week for 6 weeks, then 0.25 g/week for 6 weeks (cumulative dose 4.5 g) In 4/11 pts—cumulative dose—1.5 g; in 1 patient—5.25 g 300,000 IU of vitamin D3 a week before IVMP | At baseline, after 1 week, and then 1, 3, 6 and 12 months | No change of P1NP | Decrease of CTX after 1 month |
| Hu [15] 2020 | 45 | GO | 0.5 g/week for 6 weeks, then 0.25 g/week for 6 weeks (cumulative dose 4.5 g) In a subset of 16 pts—the 2nd course of IVMP pulse therapy 0.25 ug of alfacalcidol and 600 mg of calcium daily | At baseline and after 3 months In a subset of 16 pts—3 months after the start of the 2nd course | Decrease of P1NP after 3 months in a subset of 16 pts subjected to a 2nd course of IVMP therapy | Decrease of CTX after 3 months |
| Chen [25] 2021 | 48 | GO | In 26/48 pts: 0.5 g/week for 6 weeks, then 0.25 g/week for 6 weeks (cumulative dose 4.5 g) In 22/48 pts: 0.5 g for three consecutive days/twice every two weeks, then 0.25 g for 3 consecutive days/twice every two weeks | At baseline and after 3 months | Decrease of P1NP Decrease of P1NP | Decrease of CTX Decrease of CTX |
| Current study | 23 | GO | 0.5 g/week for 6 weeks, then 0.25 g/week for 6 weeks (cumulative dose of 4.5 g) 2000 IU of vitamin D3 and 1.0 g of calcium daily | At baseline, after 8, 24 h, and then after 1 week and 3 months | Decrease of P1NP after 8 and 24 h, normalization after 1 week, and then decrease after 3 months | Decrease of CTX after 1 week, and after 3 months |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rymuza, J.; Gutowska, K.; Kurpios-Piec, D.; Struga, M.; Miśkiewicz, P. Decrease in Bone Formation and Bone Resorption during Intravenous Methylprednisolone Pulse Therapy in Patients with Graves’ Orbitopathy. J. Clin. Med. 2022, 11, 5005. https://doi.org/10.3390/jcm11175005
Rymuza J, Gutowska K, Kurpios-Piec D, Struga M, Miśkiewicz P. Decrease in Bone Formation and Bone Resorption during Intravenous Methylprednisolone Pulse Therapy in Patients with Graves’ Orbitopathy. Journal of Clinical Medicine. 2022; 11(17):5005. https://doi.org/10.3390/jcm11175005
Chicago/Turabian StyleRymuza, Joanna, Klaudia Gutowska, Dagmara Kurpios-Piec, Marta Struga, and Piotr Miśkiewicz. 2022. "Decrease in Bone Formation and Bone Resorption during Intravenous Methylprednisolone Pulse Therapy in Patients with Graves’ Orbitopathy" Journal of Clinical Medicine 11, no. 17: 5005. https://doi.org/10.3390/jcm11175005
APA StyleRymuza, J., Gutowska, K., Kurpios-Piec, D., Struga, M., & Miśkiewicz, P. (2022). Decrease in Bone Formation and Bone Resorption during Intravenous Methylprednisolone Pulse Therapy in Patients with Graves’ Orbitopathy. Journal of Clinical Medicine, 11(17), 5005. https://doi.org/10.3390/jcm11175005