
Assessment of the Effect on Thromboprophylaxis with Multifaceted Quality Improvement Intervention based on Clinical Decision Support System in Hospitalized Patients: A Pilot Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
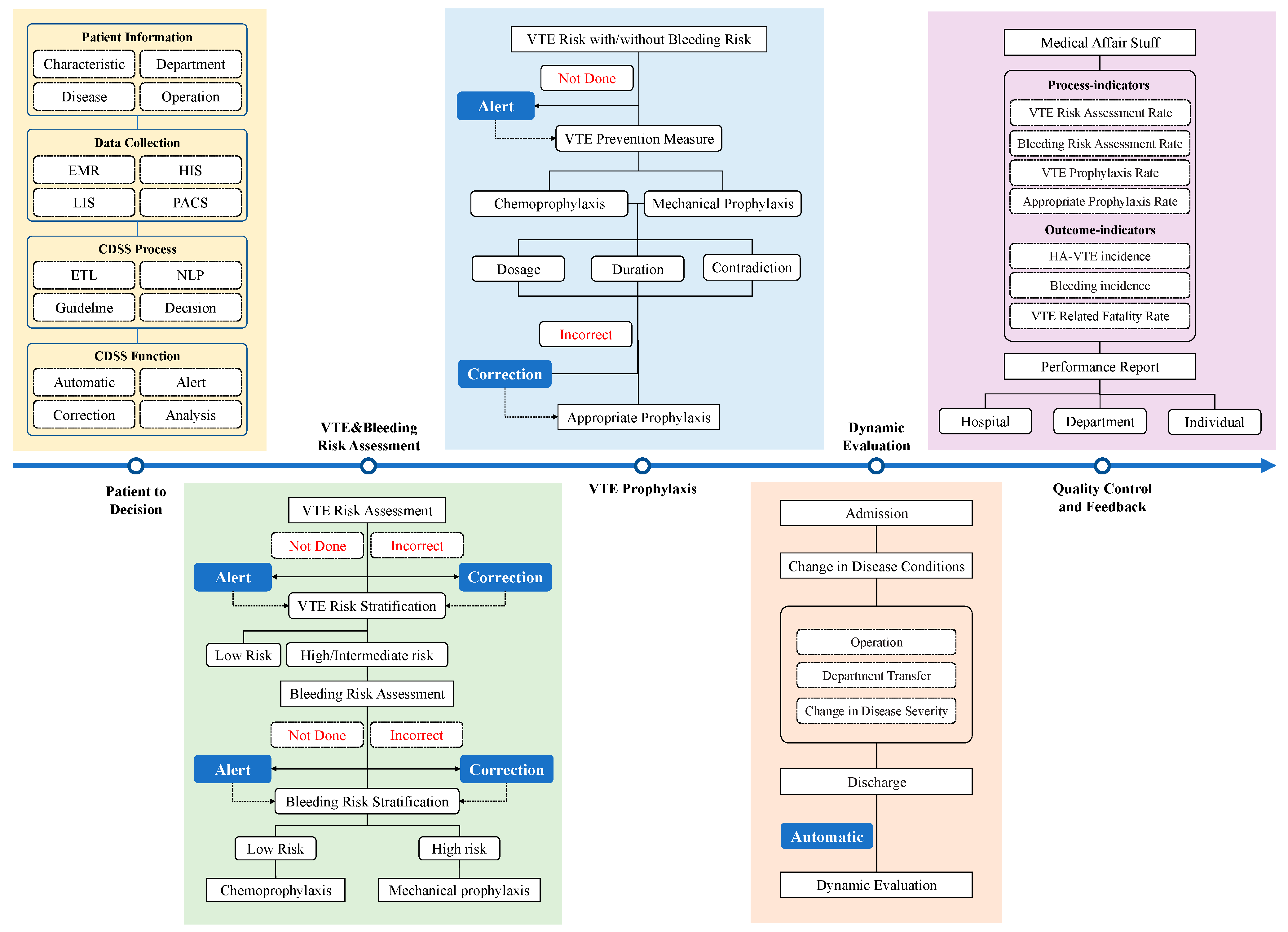
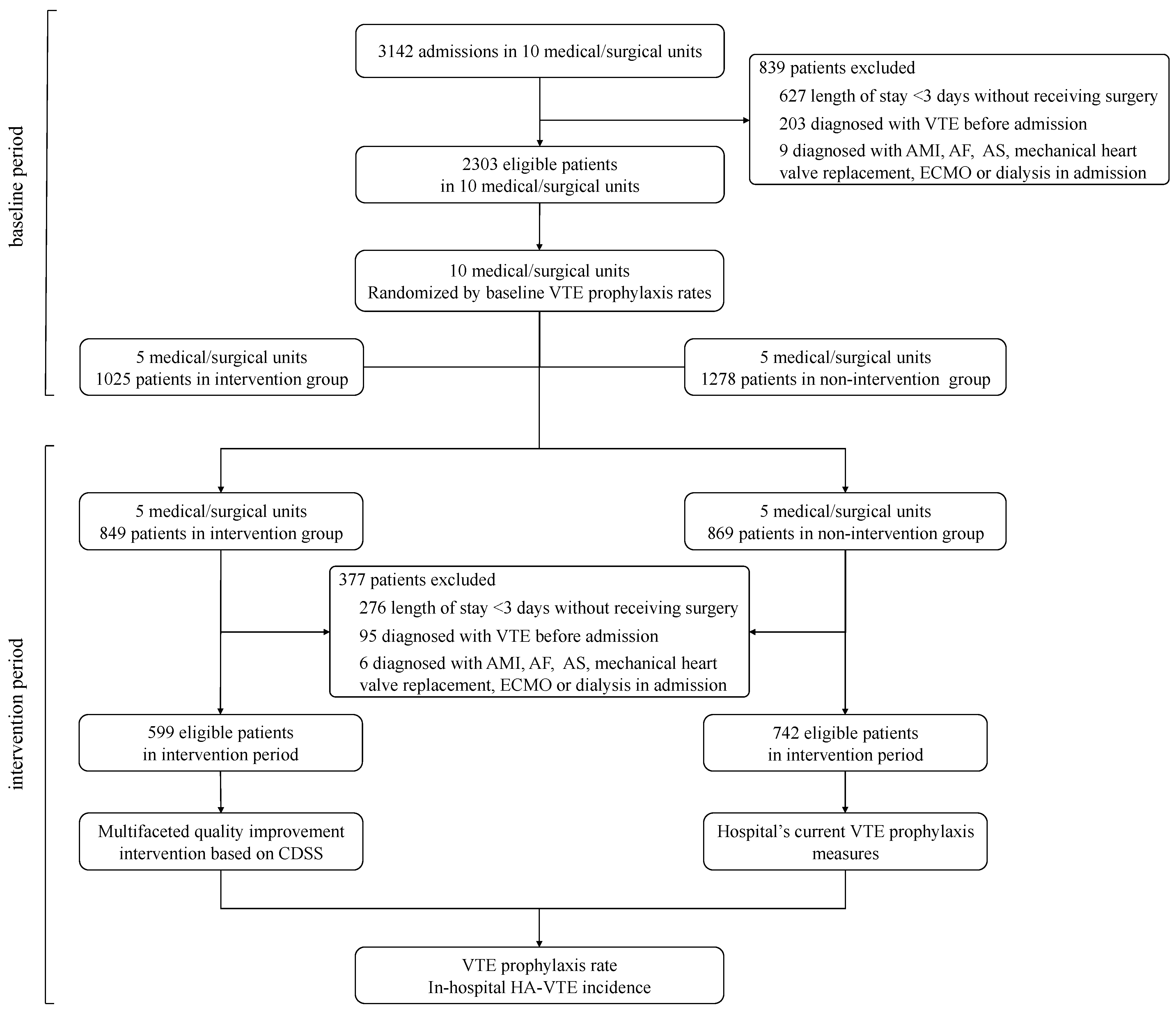
2.1. Study Design and Participants
2.2. Cluster Randomization and Intervention
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Improvement in VTE Risk Assessment
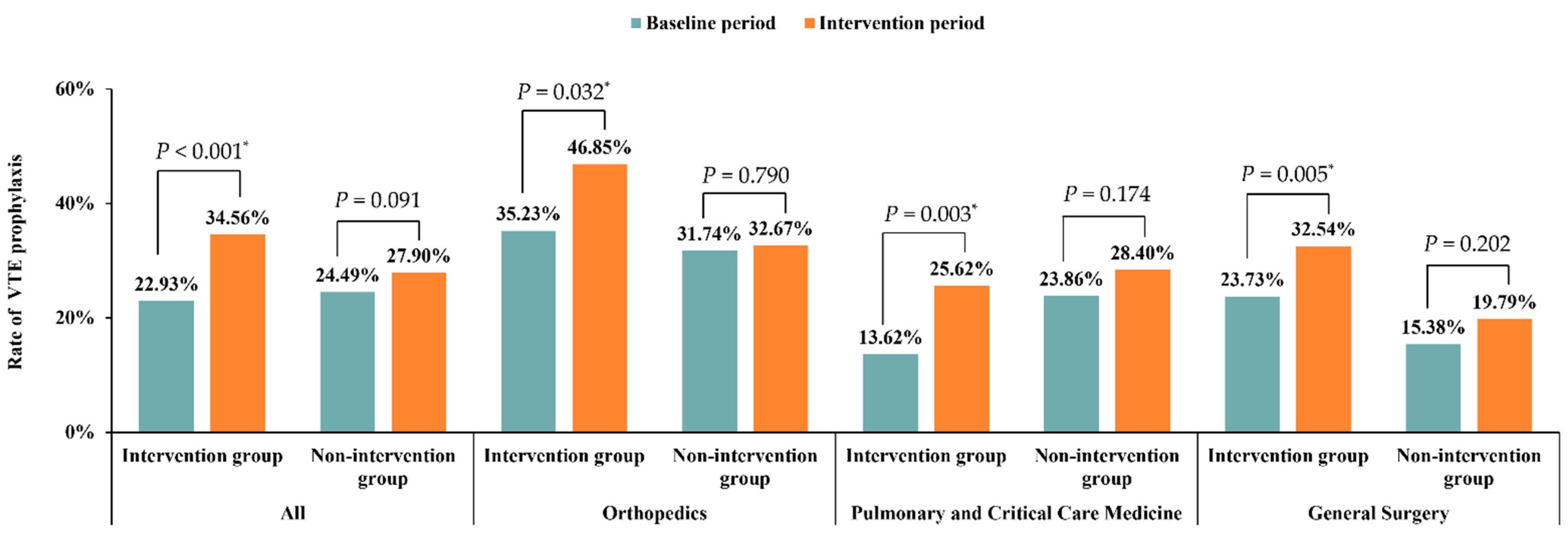
3.3. Improvement in VTE Prophylaxis
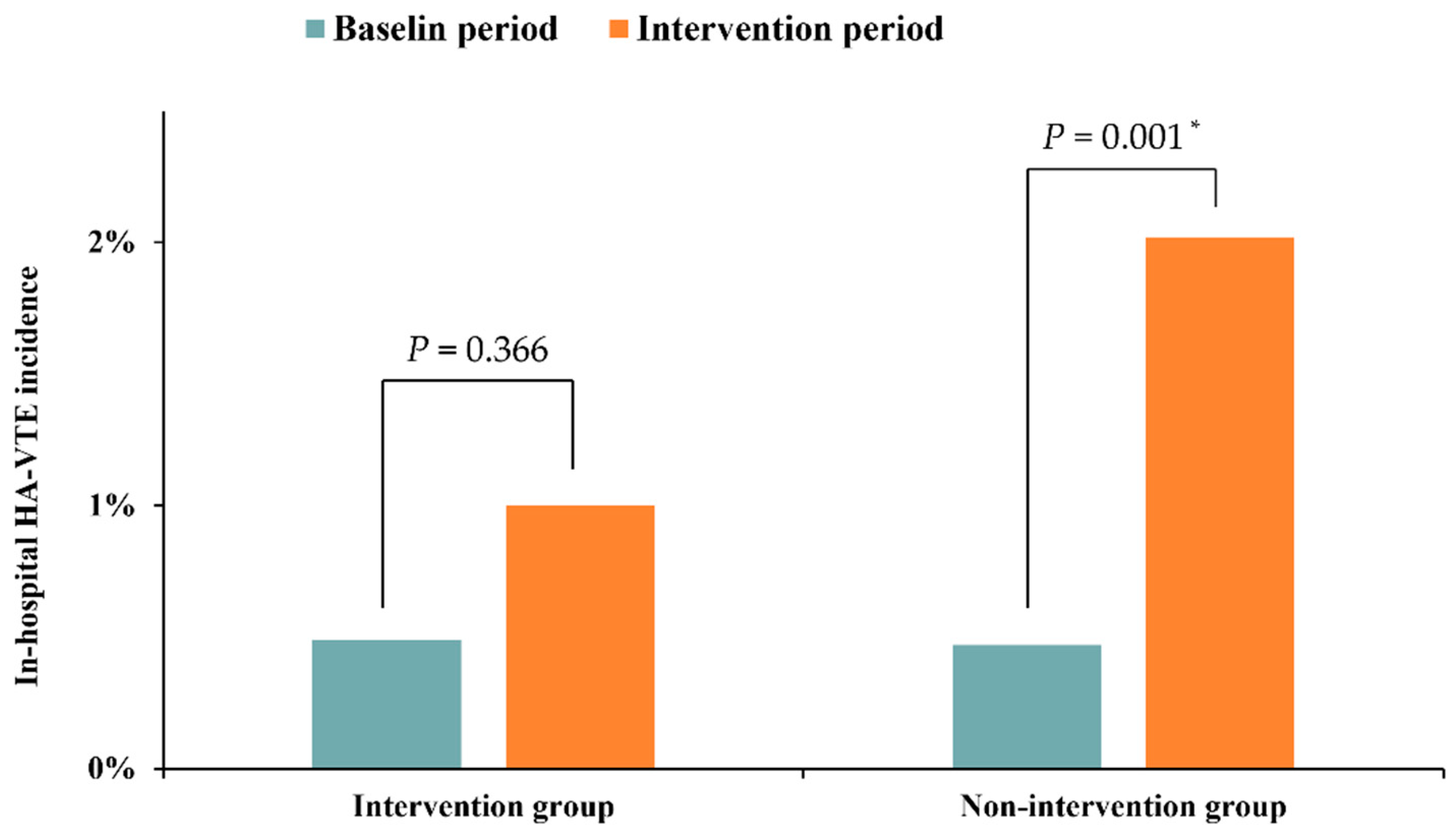
3.4. Change in In-Hospital HA-VTE Incidents
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barco, S.; Mahmoudpour, S.H.; Valerio, L.; Klok, E.; Münzel, T.; Middeldorp, S.; Ageno, W.; Cohen, A.T.; Hunt, B.J.; Konstantinides, S. Trends in Mortality Related to Pulmonary Embolism in the European Region, 2000–2015: Analysis of Vital Registration Data from the WHO Mortality Database. Lancet Respir. Med. 2020, 8, 277–287. [Google Scholar] [CrossRef]
- Wendelboe, A.M.; Raskob, G.E. Global Burden of Thrombosis: Epidemiologic Aspects. Circ. Res. 2016, 118, 1340–1347. [Google Scholar] [CrossRef] [PubMed]
- Hunt, B.J. Preventing Hospital Associated Venous Thromboembolism. BMJ 2019, 365, 14239. [Google Scholar] [CrossRef] [PubMed]
- Gould, M.K.; Garcia, D.A.; Wren, S.M.; Karanicolas, P.J.; Arcelus, J.I.; Heit, J.A.; Samama, C.M. Prevention of VTE in Nonorthopedic Surgical Patients. Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012, 141 (Suppl. S2), e227S–e277S. [Google Scholar] [CrossRef] [PubMed]
- Geerts, W.H.; Bergqvist, D.; Pineo, G.F.; Heit, J.A.; Samama, C.M.; Lassen, M.R.; Colwell, C.W. Prevention of Venous Thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest 2008, 133 (Suppl. S6), 381S–453S. [Google Scholar] [CrossRef]
- Maynard, G. Preventing Hospital-Acquired Venous Thromboembolism: A Guide for Effective Quality Improvement, 2nd ed.; Agency for Healthcare Research and Quality: Rockville, MA, USA, 2016. [Google Scholar]
- Expert Committee on the Special Fund for Thrombosis and Blood Vessels of China Health Promotion Foundation; Pulmonary Embolism and Pulmonary Vascular Diseases Group of Respiratory Disease Branch of Chinese Medical Association. Pulmonary embolism and Pulmonary Vascular Disease Working Committee of Chinese Association of Chest Physicians. Prophylaxis and Management of Venous Thromboembolism in Hospital. Chin. Med. J. 2018, 98, 1383–1388. [Google Scholar]
- Pulmonary Embolism and Pulmonary Vascular Diseases Group of Chinese Thoracic Society; Pulmonary Embolism and Pulmonary Vascular Disease Working Committee of Chinese Association of Chest Physicians. National Collaborative group on Prevention and Treatment of Pulmonary Embolism and Pulmonary Vascular Disease. Guidelines for the Diagnosis, Treatment and Prevention of Pulmonary Thromboembolism. Chin. Med. J. 2018, 98, 1060–1087. [Google Scholar]
- Cesarman-Maus, G.; Ruiz-Argüelles, G.J. News in the Indications of Direct Oral Anticoagulants According to the American College of Chest Physicians 2016 Guidelines. Curr. Drug Metab. 2017, 18, 651–656. [Google Scholar] [CrossRef]
- Hill, J.; Treasure, T. Reducing the Risk of Venous Thromboembolism (Deep Vein Thrombosis and Pulmonary Embolism) in Patients Admitted to Hospital: Summary of the NICE Guideline. Heart 2010, 96, 879–882. [Google Scholar] [CrossRef]
- Roberts, L.N.; Durkin, M.; Arya, R. Annotation: Developing a National Programme for VTE Prevention. Br. J. Haematol. 2017, 178, 162–170. [Google Scholar] [CrossRef]
- Henke, P.K.; Kahn, S.R.; Pannucci, C.J.; Secemksy, E.A.; Evans, N.S.; Khorana, A.A.; Creager, M.A.; Pradhan, A.D.; On behalf of the American Heart Association Advocacy Coordinating Committee. Call to Action to Prevent Venous Thromboembolism in Hospitalized Patients: A Policy Statement From the American Heart Association. Circulation 2020, 2010, 297–298. [Google Scholar] [CrossRef] [PubMed]
- Maynard, G.; Stein, J. Preventing Hospital-Acquired Venous Thromboembolism: A Guide for Effective Quality Improvement; AHRQ Publ. No. 08-0075; Society of Hospital Medicine: Philadelphia, PA, USA, 2008. [Google Scholar]
- Blumgart A, Merriman E G, Jackson S; Singh, V. ; Royle, G. National Policy Framework: VTE Prevention in Adult Hospitalised Patients in NZ; Health Quality & Safety Commission: Wellington, New Zealand, 2012. [Google Scholar]
- Zhang, Z.; Lei, J.; Shao, X.; Dong, F.; Wang, J.; Wang, D.; Wu, S.; Xie, W.; Wan, J.; Chen, H.; et al. Trends in Hospitalization and In-Hospital Mortality From VTE, 2007 to 2016, in China. Chest 2019, 155, 342–353. [Google Scholar] [CrossRef] [PubMed]
- Zhai, Z.; Kan, Q.; Li, W.; Qin, X.; Qu, J.; Shi, Y.; Xu, R.; Xu, Y.; Zhang, Z.; Wang, C.; et al. VTE Risk Profiles and Prophylaxis in Medical and Surgical Inpatients: The Identification of Chinese Hospitalized Patients’ Risk Profile for Venous Thromboembolism (DissolVE-2)—A Cross-Sectional Study. Chest 2019, 155, 114–122. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.T.; Tapson, V.F.; Bergmann, J.-F.; Goldhaber, S.Z.; Kakkar, A.K.; Deslandes, B.; Huang, W.; Zayaruzny, M.; Emery, L.; A Anderson, F. Venous Thromboembolism Risk and Prophylaxis in the Acute Hospital Care Setting (ENDORSE Study): A Multinational Cross-Sectional Study. Lancet 2008, 371, 387–394. [Google Scholar] [CrossRef]
- Mahadevaiah, G.; Rv, P.; Bermejo, I.; Jaffray, D.; Dekker, A.; Wee, L. Artificial Intelligence-Based Clinical Decision Support in Modern Medical Physics: Selection, Acceptance, Commissioning, and Quality Assurance. Med. Phys. 2020, 47, e228–e235. [Google Scholar] [CrossRef]
- Dong, F.; Zhen, K.; Zhang, Z.; Si, C.; Xia, J.; Zhang, T.; Xia, L.; Wang, W.; Jia, C.; Shan, G.; et al. Effect on Thromboprophylaxis among Hospitalized Patients Using a System-Wide Multifaceted Quality Improvement Intervention: Rationale and Design for a Multicenter Cluster Randomized Clinical Trial in China. Am. Heart J. 2020, 225, 44–54. [Google Scholar] [CrossRef]
- Depietri, L.; Marietta, M.; Scarlini, S.; Marcacci, M.; Corradini, E.; Pietrangelo, A.; Ventura, P. Clinical Impact of Application of Risk Assessment Models (Padua Prediction Score and Improve Bleeding Score) on Venous Thromboembolism, Major Hemorrhage and Health Expenditure Associated with Pharmacologic VTE Prophylaxis: A “Real Life” Prospective and Re. Intern. Emerg. Med. 2018, 13, 527–534. [Google Scholar] [CrossRef]
- Kahn, S.R.; Morrison, D.R.; Diendéré, G.; Piché, A.; Filion, K.B.; Klil-Drori, A.J.; Douketis, J.D.; Emed, J.; Roussin, A.; Tagalakis, V.; et al. Interventions for Implementation of Thromboprophylaxis in Hospitalized Patients at Risk for Venous Thromboembolism. Cochrane Database Syst. Rev. 2018, 2018, CD008201. [Google Scholar] [CrossRef]
- Kucher, N.; Tapson, V.F.; Goldhaber, S.Z. Risk Factors Associated with Symptomatic Pulmonary Embolism in a Large Cohort of Deep Vein Thrombosis Patients. Thromb. Haemost. 2005, 93, 494–498. [Google Scholar] [CrossRef]
- Haut, E.R.; Lau, B.D.; Kraenzlin, F.S.; Hobson, D.B.; Kraus, P.S.; Carolan, H.T.; Haider, A.H.; Holzmueller, C.G.; Efron, D.T.; Pronovost, P.J.; et al. Improved Prophylaxis and Decreased Rates of Preventable Harm with the Use of a Mandatory Computerized Clinical Decision Support Tool for Prophylaxis for Venous Thromboembolism in Trauma. Arch. Surg. 2012, 147, 901–907. [Google Scholar] [CrossRef]
- Turrentine, F.E.; Sohn, M.-W.; Wilson, S.L.; Stanley, C.; Novicoff, W.; Sawyer, R.G.; Williams, M.D. Fewer Thromboembolic Events after Implementation of a Venous Thromboembolism Risk Stratification Tool. J. Surg. Res. 2018, 225, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Cassidy, M.R.; Rosenkranz, P.; McAneny, D. Reducing Postoperative Venous Thromboembolism Complications with a Standardized Risk-Stratified Prophylaxis Protocol and Mobilization Program. J. Am. Coll. Surg. 2014, 218, 1095–1104. [Google Scholar] [CrossRef] [PubMed]
- Spyropoulos, A.C.; Ageno, W.; Albers, G.W.; Elliott, C.G.; Halperin, J.L.; Hiatt, W.R.; Maynard, G.A.; Steg, P.G.; Weitz, J.I.; Suh, E.; et al. Rivaroxaban for Thromboprophylaxis after Hospitalization for Medical Illness. N. Engl. J. Med. 2018, 379, 1118–1127. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Period | Intervention Period # | ||
|---|---|---|---|
| Intervention Group | Nonintervention Group | ||
| (n = 2303) | (n = 599) | (n = 742) | |
| Male | 1088 (47.24%) | 349 (58.26%) | 339 (45.69%) |
| Age (Years) | |||
| ≤40 | 370 (16.07%) | 104 (17.36%) | 79 (10.65%) |
| 41–60 | 758 (32.91%) | 180 (30.05%) | 219 (29.51%) |
| 61–74 | 838 (36.39%) | 219 (36.56%) | 298 (40.16%) |
| ≥75 | 337 (14.63%) | 96 (16.03%) | 146 (19.68%) |
| Medical disease | 829 (36.00%) | 121 (20.20%) | 250 (33.69%) |
| Malignancy | 567 (24.62%) | 249 (41.57%) | 185 (24.93%) |
| Surgery | 1474 (64.00%) | 478 (79.80%) | 492 (66.31%) |
| VTE prophylaxis | 548 (23.80%) * | 207 (34.56%) | 207 (27.90%) |
| Length of stay (Days) | 8 | 8 | 8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gao, Q.; Zhen, K.; Xia, L.; Wang, W.; Xu, Y.; Si, C.; Zhang, Z.; Dong, F.; Lei, J.; Yang, P.; et al. Assessment of the Effect on Thromboprophylaxis with Multifaceted Quality Improvement Intervention based on Clinical Decision Support System in Hospitalized Patients: A Pilot Study. J. Clin. Med. 2022, 11, 4997. https://doi.org/10.3390/jcm11174997
Gao Q, Zhen K, Xia L, Wang W, Xu Y, Si C, Zhang Z, Dong F, Lei J, Yang P, et al. Assessment of the Effect on Thromboprophylaxis with Multifaceted Quality Improvement Intervention based on Clinical Decision Support System in Hospitalized Patients: A Pilot Study. Journal of Clinical Medicine. 2022; 11(17):4997. https://doi.org/10.3390/jcm11174997
Chicago/Turabian StyleGao, Qian, Kaiyuan Zhen, Lei Xia, Wei Wang, Yaping Xu, Chaozeng Si, Zhu Zhang, Fen Dong, Jieping Lei, Peiran Yang, and et al. 2022. "Assessment of the Effect on Thromboprophylaxis with Multifaceted Quality Improvement Intervention based on Clinical Decision Support System in Hospitalized Patients: A Pilot Study" Journal of Clinical Medicine 11, no. 17: 4997. https://doi.org/10.3390/jcm11174997
APA StyleGao, Q., Zhen, K., Xia, L., Wang, W., Xu, Y., Si, C., Zhang, Z., Dong, F., Lei, J., Yang, P., Liu, J., Sun, Z., Zhang, T., Wan, J., Xie, W., Liu, P., Jia, C., Zhai, Z., & Wang, C., on behalf of the Chinese Prevention Strategy for Venous Thromboembolism (CHIPS-VTE) Study Group. (2022). Assessment of the Effect on Thromboprophylaxis with Multifaceted Quality Improvement Intervention based on Clinical Decision Support System in Hospitalized Patients: A Pilot Study. Journal of Clinical Medicine, 11(17), 4997. https://doi.org/10.3390/jcm11174997