
The Lack of Analgesic Efficacy of Nefopam after Video-Assisted Thoracoscopic Surgery for Lung Cancer: A Randomized, Single-Blinded, Controlled Trial

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Statements
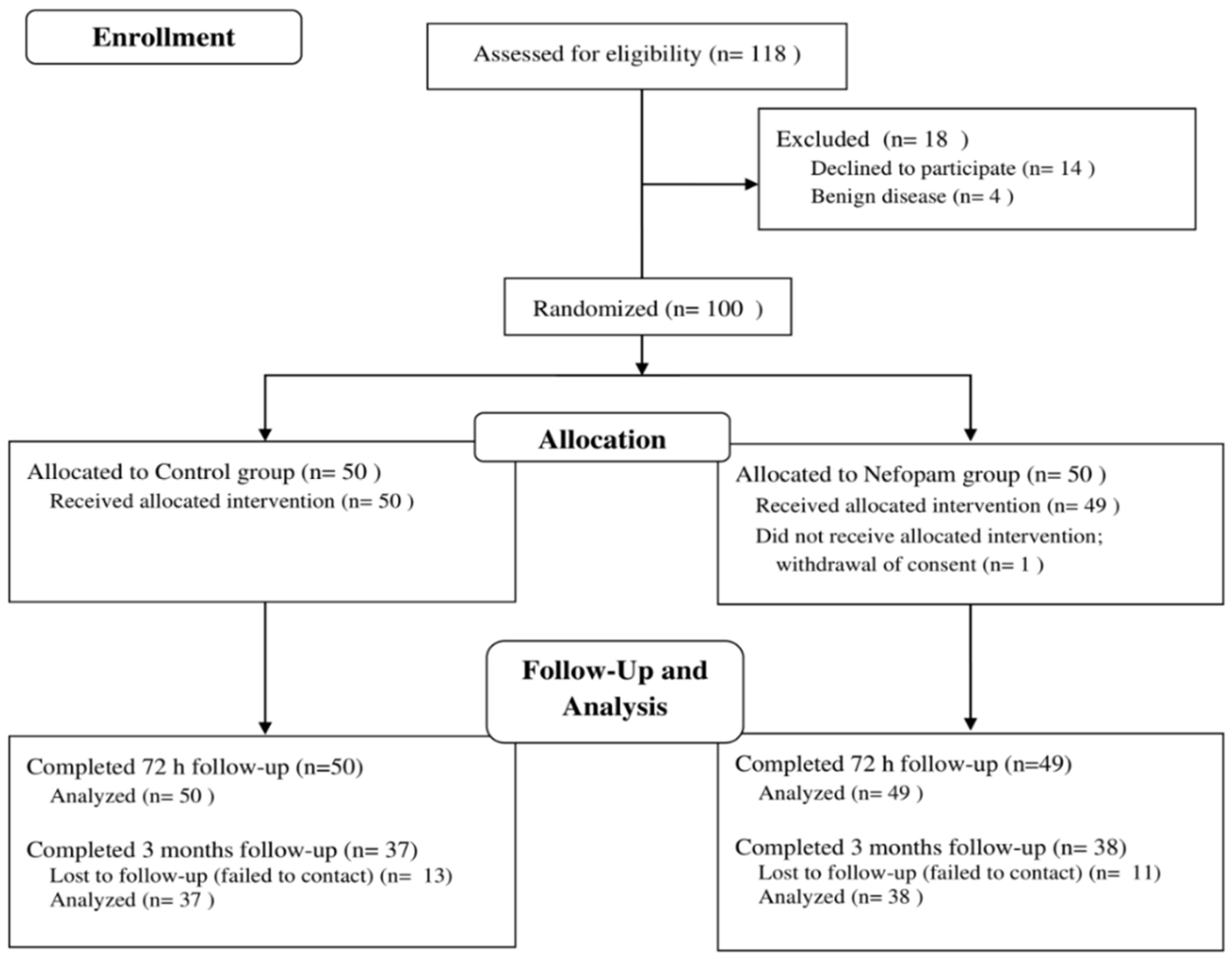
2.2. Participants
2.3. Randomization and Blinding Method
2.4. Intervention, Anesthesia Protocol, and Perioperative Pain Management
2.5. Outcome Measurements
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lederman, D.; Easwar, J.; Feldman, J.; Shapiro, V. Anesthetic considerations for lung resection: Preoperative assessment, intraoperative challenges and postoperative analgesia. Ann. Transl. Med. 2019, 7, 356. [Google Scholar] [CrossRef] [PubMed]
- Gerner, P. Postthoracotomy pain management problems. Anesthesiol. Clin. 2008, 26, 355–367. [Google Scholar] [CrossRef] [PubMed]
- Gotoda, Y.; Kambara, N.; Sakai, T.; Kishi, Y.; Kodama, K.; Koyama, T. The morbidity, time course and predictive factors for persistent post-thoracotomy pain. Eur. J. Pain 2001, 5, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Kampe, S.; Geismann, B.; Weinreich, G.; Stamatis, G.; Ebmeyer, U.; Gerbershagen, H.J. The Influence of Type of Anesthesia, Perioperative Pain, and Preoperative Health Status on Chronic Pain Six Months after Thoracotomy—A Prospective Cohort Study. Pain Med. 2017, 18, 2208–2213. [Google Scholar] [CrossRef]
- Katz, J.; Jackson, M.; Kavanagh, B.P.; Sandler, A.N. Acute pain after thoracic surgery predicts long-term post-thoracotomy pain. Clin. J. Pain 1996, 12, 50–55. [Google Scholar] [CrossRef]
- Bayman, E.O.; Parekh, K.R.; Keech, J.; Selte, A.; Brennan, T.J. A Prospective Study of Chronic Pain after Thoracic Surgery. Anesthesiology 2017, 126, 938–951. [Google Scholar] [CrossRef]
- Manion, S.C.; Brennan, T.J. Thoracic epidural analgesia and acute pain management. Anesthesiology 2011, 115, 181–188. [Google Scholar] [CrossRef]
- Wildsmith, J.A. Continuous thoracic epidural block for surgery: Gold standard or debased currency? Br. J. Anaesth. 2012, 109, 9–12. [Google Scholar] [CrossRef]
- Conacher, I.D. Pain relief after thoracotomy. Br. J. Anaesth. 1990, 65, 806–812. [Google Scholar] [CrossRef]
- Mesbah, A.; Yeung, J.; Gao, F. Pain after thoracotomy. BJA Educ. 2015, 16, 1–7. [Google Scholar] [CrossRef]
- Evans, M.S.; Lysakowski, C.; Tramèr, M.R. Nefopam for the prevention of postoperative pain: Quantitative systematic review. Br. J. Anaesth. 2008, 101, 610–617. [Google Scholar] [CrossRef]
- Girard, P.; Chauvin, M.; Verleye, M. Nefopam analgesia and its role in multimodal analgesia: A review of preclinical and clinical studies. Clin. Exp. Pharmacol. Physiol. 2016, 43, 3–12. [Google Scholar] [CrossRef]
- Tiglis, M.; Neagu, T.P.; Elfara, M.; Diaconu, C.C.; Bratu, O.G.; Vacaroiu, I.A.; Grintescu, I.M. Nefopam and its role in modulating acute and chronic pain. Rev. Chim. 2018, 69, 2877–2880. [Google Scholar] [CrossRef]
- Verleye, M.; Andre, N.; Heulard, I.; Gillardin, J.M. Nefopam blocks voltage-sensitive sodium channels and modulates glutamatergic transmission in rodents. Brain Res. 2004, 1013, 249–255. [Google Scholar] [CrossRef]
- Na, H.S.; Oh, A.Y.; Ryu, J.H.; Koo, B.W.; Nam, S.W.; Jo, J.; Park, J.H. Intraoperative Nefopam Reduces Acute Postoperative Pain after Laparoscopic Gastrectomy: A Prospective, Randomized Study. J. Gastrointest. Surg. 2018, 22, 771–777. [Google Scholar] [CrossRef]
- Mimoz, O.; Incagnoli, P.; Josse, C.; Gillon, M.C.; Kuhlman, L.; Mirand, A.; Soilleux, H.; Fletcher, D. Analgesic efficacy and safety of nefopam vs. propacetamol following hepatic resection. Anaesthesia 2001, 56, 520–525. [Google Scholar] [CrossRef]
- Du Manoir, B.; Aubrun, F.; Langlois, M.; Le Guern, M.E.; Alquire, C.; Chauvin, M.; Fletcher, D. Randomized prospective study of the analgesic effect of nefopam after orthopaedic surgery. Br. J. Anaesth. 2003, 91, 836–841. [Google Scholar] [CrossRef]
- Ok, Y.M.; Cheon, J.H.; Choi, E.J.; Chang, E.J.; Lee, H.M.; Kim, K.H. Nefopam Reduces Dysesthesia after Percutaneous Endoscopic Lumbar Discectomy. Korean J. Pain 2016, 29, 40–47. [Google Scholar]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. J. Pharmacol. Pharmacother. 2010, 1, 100–107. [Google Scholar] [CrossRef]
- Gjeilo, K.H.; Stenseth, R.; Wahba, A.; Lydersen, S.; Klepstad, P. Validation of the brief pain inventory in patients six months after cardiac surgery. J. Pain Symptom Manag. 2007, 34, 648–656. [Google Scholar] [CrossRef]
- Backonja, M.M.; Krause, S.J. Neuropathic pain questionnaire—Short form. Clin. J. Pain 2003, 19, 315–316. [Google Scholar] [CrossRef]
- Zhao, T.; Shen, Z.; Sheng, S. The efficacy and safety of nefopam for pain relief during laparoscopic cholecystectomy: A meta-analysis. Medicine 2018, 97, e0089. [Google Scholar] [CrossRef]
- Jin, H.S.; Kim, Y.C.; Yoo, Y.; Lee, C.; Cho, C.W.; Kim, W.J. Opioid sparing effect and safety of nefopam in patient controlled analgesia after laparotomy: A randomized, double blind study. J. Int. Med. Res. 2016, 44, 844–854. [Google Scholar] [CrossRef]
- Cuvillon, P.; Zoric, L.; Demattei, C.; Alonso, S.; Casano, F.; L’hermite, J.; Ripart, J.; Lefrant, J.; Muller, L. Opioid-sparing effect of nefopam in combination with paracetamol after major abdominal surgery: A randomized double-blind study. Minerva Anestesiol. 2017, 83, 914–920. [Google Scholar] [CrossRef]
- Koh, H.J.; Joo, J.; Kim, Y.S.; Lee, Y.J.; Yoo, W.; Lee, M.S.; Park, H.J. Analgesic Effect of Low Dose Nefopam Hydrochloride after Arthroscopic Rotator Cuff Repair: A Randomized Controlled Trial. J. Clin. Med. 2019, 8, 553. [Google Scholar] [CrossRef]
- Eiamcharoenwit, J.; Chotisukarat, H.; Tainil, K.; Attanath, N.; Akavipat, P. Analgesic efficacy of intravenous nefopam after spine surgery: A randomized, double-blind, placebo-controlled trial. F1000Research 2020, 9, 516. [Google Scholar] [CrossRef]
- Richebe, P.; Picard, W.; Rivat, C.; Jelacic, S.; Branchard, O.; Leproust, S.; Cahana, A.; Janvier, G. Effects of nefopam on early postoperative hyperalgesia after cardiac surgery. J. Cardiothorac. Vasc. Anesth. 2013, 27, 427–435. [Google Scholar] [CrossRef] [PubMed]
- Remerand, F.; Le Tendre, C.; Rosset, P.; Peru, R.; Favard, L.; Pourrat, X.; Laffon, M.; Fusciardi, J. Nefopam after total hip arthroplasty: Role in multimodal analgesia. Orthop. Traumatol. Surg. Res. 2013, 99, 169–174. [Google Scholar] [CrossRef]
- Chalermkitpanit, P.; Limthongkul, W.; Yingsakmongkol, W.; Thepsoparn, M.; Pannangpetch, P.; Tangchitcharoen, N.; Tanasansomboon, T.; Singhatanadgige, W. Analgesic Effect of Intravenous Nefopam for Postoperative Pain in Minimally Invasive Spine Surgery: A Randomized Prospective Study. Asian Spine J. 2022. [Google Scholar] [CrossRef]
- Na, H.S.; Oh, A.Y.; Koo, B.W.; Lim, D.J.; Ryu, J.H.; Han, J.W. Preventive Analgesic Efficacy of Nefopam in Acute and Chronic Pain After Breast Cancer Surgery: A Prospective, Double-Blind, and Randomized Trial. Medicine 2016, 95, e3705. [Google Scholar] [CrossRef]
- Kim, B.G.; Moon, J.Y.; Choi, J.Y.; Park, I.S.; Oh, A.Y.; Jeon, Y.T.; Hwang, J.W.; Ryu, J.H. The Effect of Intraoperative Nefopam Administration on Acute Postoperative Pain and Chronic Discomfort After Robotic or Endoscopic Assisted Thyroidectomy: A Randomized Clinical Trial. World J. Surg. 2018, 42, 2094–2101. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.Y.; Lim, B.G.; Kim, H.; Kong, M.H.; Lee, I.O.; Kim, N.S. The analgesic effect of nefopam combined with low dose remifentanil in patients undergoing middle ear surgery under desflurane anesthesia: A randomized controlled trial. Korean J. Anesthesiol. 2015, 68, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Sunshine, A.; Laska, E. Nefopam and morphine in man. Clin. Pharmacol. Ther. 1975, 18, 530–534. [Google Scholar] [CrossRef] [PubMed]
- Delage, N.; Maaliki, H.; Beloeil, H.; Benhamou, D.; Mazoit, J.X. Median effective dose (ED50) of nefopam and ketoprofen in postoperative patients: A study of interaction using sequential analysis and isobolographic analysis. Anesthesiology 2005, 102, 1211–1216. [Google Scholar] [CrossRef]
- Van Elstraete, A.C.; Sitbon, P. Median effective dose (ED50) of paracetamol and nefopam for postoperative pain: Isobolographic analysis of their antinociceptive interaction. Minerva Anestesiol. 2013, 79, 232–239. [Google Scholar]
- Beloeil, H.; Eurin, M.; Thevenin, A.; Benhamou, D.; Mazoit, J.X. Effective dose of nefopam in 80% of patients (ED80): A study using the continual reassessment method. Br. J. Clin. Pharmacol. 2007, 64, 686–693. [Google Scholar] [CrossRef]
- Kim, K.H.; Abdi, S. Rediscovery of nefopam for the treatment of neuropathic pain. Korean J. Pain 2014, 27, 103–111. [Google Scholar] [CrossRef]
- Lim, H.; Kang, S.; Kim, B.; Ko, S. Comparison Between Preoperative and Intraoperative Administration of Nefopam for Acute and Chronic Postoperative Pain in Colon Cancer Patients: A Prospective, Randomized, Double-Blind Study. World J. Surg. 2019, 43, 3191–3197. [Google Scholar] [CrossRef]
- Kim, S.H.; Stoicea, N.; Soghomonyan, S.; Bergese, S.D. Intraoperative use of remifentanil and opioid induced hyperalgesia/acute opioid tolerance: Systematic review. Front. Pharmacol. 2014, 5, 108. [Google Scholar] [CrossRef]

{kind=link}
| Control Group (n = 50) | Nefopam Group (n = 49) | p-Value | |
|---|---|---|---|
| Age, year | 59.5 [55.0, 63.0] | 59.0 [53.0, 63.0] | 0.606 |
| Males/Females, n | 17 (34)/33 (66) | 21 (43)/28 (57) | 0.484 |
| Weight, kg | 62.7 [55.0, 67.6] | 64.5 [56.5, 69.9] | 0.566 |
| Height, cm | 160.6 ± 7.8 | 162.8 ± 8.4 | 0.181 |
| Body mass index, kg/m2 | 24.1 [21.9, 26.4] | 24.1 [22.7, 24.9] | 0.740 |
| Smoking, n | 16 (32) | 21 (43) | 0.573 |
| Hypertension, n | 10 (20) | 10 (20) | >0.999 |
| Diabetes mellitus, n | 5 (10) | 6 (12) | 0.972 |
| ASA physical class (I/II/III), n | 5/42/3 | 10/36/3 | 0.383 |
| Type of surgical incision, n | 0.362 | ||
| VATS | 49 (98) | 46 (94) | |
| Thoracotomy | 1 (2) | 3 (6) | |
| Type of surgery, n | 0.189 | ||
| Lobectomy | 47 (94) | 41 (84) | |
| Wedge resection or Segmentectomy | 3 (6) | 8 (16) | |
| Operator (1/2/3/4/5/6/7), n | 7/9/5/17/0/1/11 | 11/11/4/12/2/4/5 | 0.257 |
| Duration of anesthesia, min | 157.5 [135.0, 197.0] | 166.0 [143.0, 193.0] | 0.669 |
| Duration of operation, min | 104.5 [84.0, 145.0] | 109.0 [88.0, 148.0] | 0.583 |
| Amount of intraoperative remifentanil administration, μg | 300.0 [250.0, 450.0] | 450.0 [300.0, 550.0] | 0.013 1 |
| Control Group (n = 50) | Nefopam Group (n = 49) | Median Difference 95% CI | p-Value | |
|---|---|---|---|---|
| Total opioid consumption (mg) | ||||
| 6 h postoperatively 1 | 20.3 [13.9, 27.0] | 19.8 [13.5, 25.3] | −1.55 [−6.64, 3.69] | 0.356 |
| During PACU stay | 8.9 [6.9, 10.1] | 7.4 [6.1, 9.4] | −1.45 [−2.76, 0.07] | 0.196 2 |
| 12 h postoperatively 3 | 31.6 [26.3, 39.7] | 31.5 [22.7, 41.0] | −0.04 [−7.93, 8.10] | >0.999 2 |
| 24 h postoperatively | 58.5 [48.8, 78.7] | 63.0 [48.8, 83.5] | 4.45 [−8.96, 16.29] | >0.999 2 |
| 72 h postoperatively | 120.0 [85.0, 166.4] | 130.6 [109.0, 178.0] | 10.57 [−9.53, 33.50] | 0.618 2 |
| Time to first rescue analgesia (min) | 259.5 [142.0, 432.0] | 212.5 [104.0, 371.0] | −47.00 [−169.00, 73.95] | 0.302 |
| Control Group (n = 50) | Nefopam Group (n = 49) | Median/Risk Difference 95% CI | p-Value | ||
|---|---|---|---|---|---|
| NRS pain score during 72 h postoperatively | |||||
| PACU stay 1 | 6.0 [5.0, 7.0] | 5.0 [3.0, 6.0] | −1.0 [−2.0, 0.0] | 0.355 2 | |
| 6 h postoperatively | 3.0 [3.0, 4.0] | 3.0 [3.0, 4.0] | 0.0 [−1.0, 1.0] | >0.999 2 | |
| 12 h postoperatively | 3.0 [3.0, 5.0] | 3.0 [3.0, 4.0] | 0.0 [−1.0, 0.0] | >0.999 2 | |
| 24 h postoperatively | 3.0 [2.0, 5.0] | 3.0 [2.0, 4.0] | 0.0 [−1.0, 1.0] | >0.999 2 | |
| 72 h postoperatively | 2.0 [2.0, 3.0] | 2.5 [1.0, 3.0] | 0.5 [0.0, 1.0] | >0.999 2 | |
| Incidence of adverse events | |||||
| PONV | 33 (66) | 34 (69) | 3.4 [−15.0, 21.8] | 0.884 | |
| Dizziness | 24 (48) | 19 (39) | −9.2 [−28.7, 10.2] | 0.470 | |
| Desaturation | 8 (16) | 8 (16) | 0.3 [−14.2, 14.8] | >0.999 | |
| Sedation | 1 (2) | 2 (4) | 2.1 [−4.7, 8.9] | 0.617 | |
| Changes in AST and ALT at POD1 and POD3 2,3 | |||||
| AST | POD1 | 3.0 [0.0, 6.0] | 5.0 [0.0,11.0] | 2.0 [−1.0, 7.0] | 0.144 |
| POD3 | 0.0 [−3.0, 5.0] | 0.5 [−4.5, 4.0] | 0.5 [−3.0, 3.0] | >0.999 | |
| ALT | POD1 | −1.0 [−7.0, 1.0] | −1.0 [−5.0, 4.0] | 0.0 [−3.0, 4.0] | 0.864 |
| POD3 | −2.0 [−7.0, 0.0] | −2.0 [−8.0, 3.5] | 0.0 [−4.0, 3.0] | >0.999 | |
| Duration of ICU stay (min) | 1140.0 [1020.0, 1280.0] | 1177.0 [1050.0, 1339.0] | 37.0 [−35.5, 50.0] | 0.283 | |
| Duration of hospitalization (day) | 6.0 [5.0, 7.0] | 6.0 [5.0, 7.0] | 0.0 [−1.0, 1.0] | 0.904 | |
| Control Group (n = 37) | Nefopam Group (n = 38) | Median Difference 95% CI | p-Value | |
|---|---|---|---|---|
| Presence of pain | 24 (65) | 21 (55) | 0.540 | |
| Pain intensity 1 | ||||
| Worst pain | 3.00 [2.00, 4.00] | 2.00 [1.00, 3.00] | −1.0 [−2.0, 1.0] | 0.150 |
| Least pain | 0.00 [0.00, 0.00] | 0.00 [0.00, 0.00] | 0.0 [0.0, 0.0] | 0.189 |
| Average Pain | 1.00 [0.75, 2.00] | 1.00 [0.00, 2.00] | 0.0 [−2.0, 1.0] | 0.299 |
| Current Pain | 0.00 [0.00, 1.25] | 0.00 [0.00, 0.00] | 0.0 [−1.0, 0.0] | 0.272 |
| Pain interference with daily activities 2 | 0.00 [0.00, 0.00] | 0.00 [0.00, 0.00] | 0.0 [0.0, 0.0] | NS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yeo, H.; Choi, J.W.; Lee, S.; Sim, W.S.; Park, S.J.; Jeong, H.; Yang, M.; Ahn, H.J.; Kim, J.A.; Lee, E.J. The Lack of Analgesic Efficacy of Nefopam after Video-Assisted Thoracoscopic Surgery for Lung Cancer: A Randomized, Single-Blinded, Controlled Trial. J. Clin. Med. 2022, 11, 4849. https://doi.org/10.3390/jcm11164849
Yeo H, Choi JW, Lee S, Sim WS, Park SJ, Jeong H, Yang M, Ahn HJ, Kim JA, Lee EJ. The Lack of Analgesic Efficacy of Nefopam after Video-Assisted Thoracoscopic Surgery for Lung Cancer: A Randomized, Single-Blinded, Controlled Trial. Journal of Clinical Medicine. 2022; 11(16):4849. https://doi.org/10.3390/jcm11164849
Chicago/Turabian StyleYeo, Hyean, Ji Won Choi, Seungwon Lee, Woo Seog Sim, Soo Jung Park, Heejoon Jeong, Mikyung Yang, Hyun Joo Ahn, Jie Ae Kim, and Eun Ji Lee. 2022. "The Lack of Analgesic Efficacy of Nefopam after Video-Assisted Thoracoscopic Surgery for Lung Cancer: A Randomized, Single-Blinded, Controlled Trial" Journal of Clinical Medicine 11, no. 16: 4849. https://doi.org/10.3390/jcm11164849
APA StyleYeo, H., Choi, J. W., Lee, S., Sim, W. S., Park, S. J., Jeong, H., Yang, M., Ahn, H. J., Kim, J. A., & Lee, E. J. (2022). The Lack of Analgesic Efficacy of Nefopam after Video-Assisted Thoracoscopic Surgery for Lung Cancer: A Randomized, Single-Blinded, Controlled Trial. Journal of Clinical Medicine, 11(16), 4849. https://doi.org/10.3390/jcm11164849