
Effect of Intravenous Ketamine on Hypocranial Pressure Symptoms in Patients with Spinal Anesthetic Cesarean Sections: A Systematic Review and Meta-Analysis


Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy and Selection Criteria
2.2. Data Extraction and Quality Assessment
2.3. Statistical Analysis
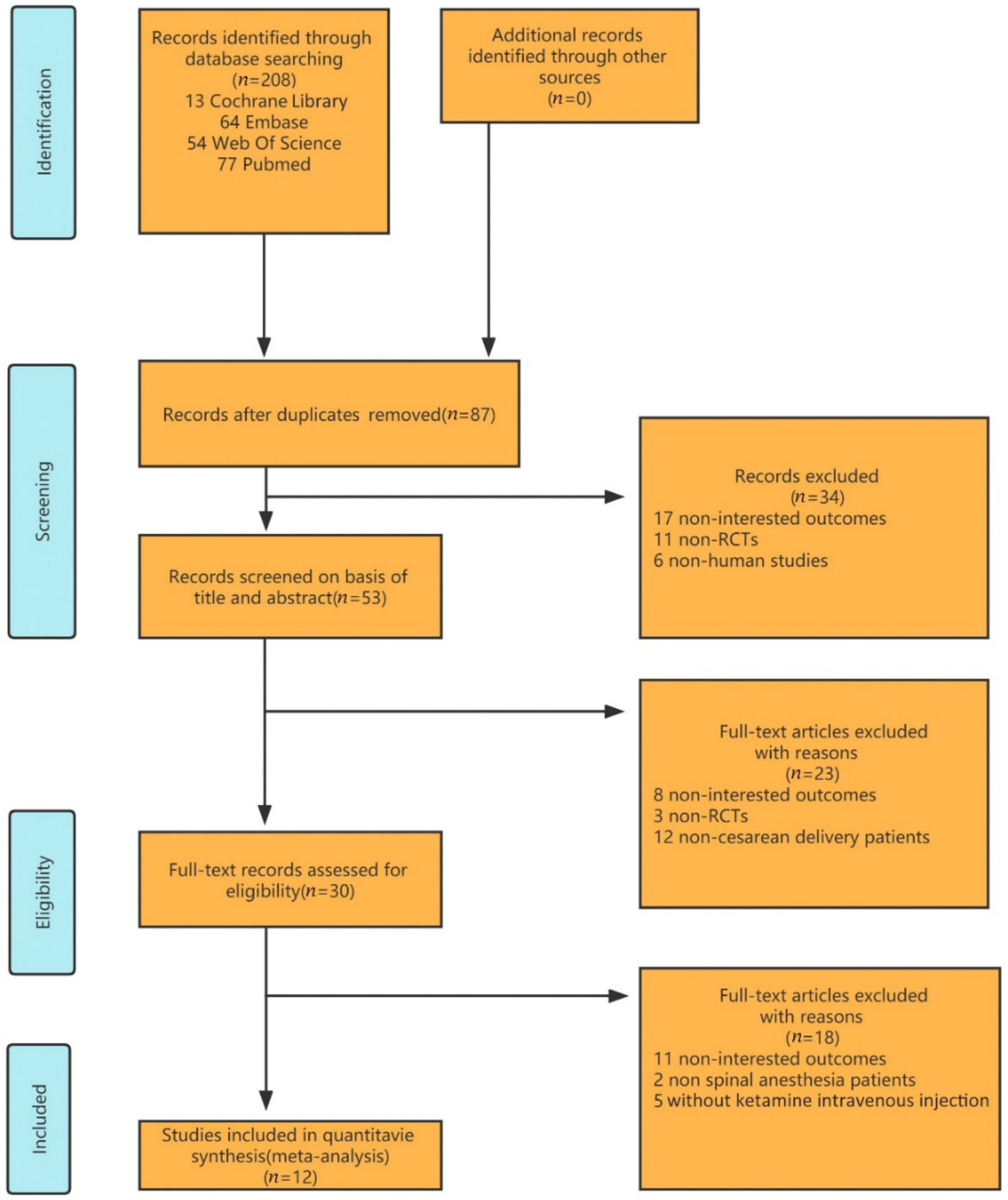
3. Results
3.1. Eligible Studies and the Characteristics
3.2. Quality Assessment of the Selected Studies
3.3. Effect of Interventions
3.3.1. Headaches
3.3.2. Nausea
3.3.3. Vomiting
3.4. Subgroup Analysis
3.5. Sensitivity Analysis and Publication Bias
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
- Search strategy for CENTRAL, the Cochrane Library
- 2.
- Search strategy for web of science (OvidSP)
- 3.
- Search strategy for Embase (OvidSP)
- 4.
- Search strategy for MEDLINE (OvidSP)
References
- Belizán, J.M.; Minckas, N.; McClure, E.M.; Saleem, S.; Moore, J.L.; Goudar, S.S.; Esamai, F.; Patel, A.; Chomba, E.; Garces, A.L.; et al. An approach to identify a minimum and rational proportion of caesarean sections in resource-poor settings: A global network study. Lancet Glob. Health 2018, 6, e894–e901. [Google Scholar] [CrossRef]
- Stjernholm, Y.; Petersson, K.; Eneroth, E. Changed indications for cesarean sections. Acta Obstet. Gynecol. Scand. 2010, 89, 49–53. [Google Scholar] [CrossRef] [PubMed]
- Gregory, K.D.; Curtin, S.C.; Taffel, S.M.; Notzon, F.C. Changes in indications for cesarean delivery: United States, 1985 and 1994. Am. J. Public Health 1998, 88, 1384–1387. [Google Scholar] [CrossRef]
- Mylonas, I.; Friese, K. Indications for and Risks of Elective Cesarean Section. Dtsch. Arztebl. Int. 2015, 112, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Butwick, A.; Carvalho, B.; Danial, C.; Riley, E. Retrospective analysis of anesthetic interventions for obese patients undergoing elective cesarean delivery. J. Clin. Anesth. 2010, 22, 519–526. [Google Scholar] [CrossRef]
- Ferede, Y.A.; Nigatu, Y.A.; Agegnehu, A.F.; Mustofa, S.Y. Incidence and associated factors of post dural puncture headache after cesarean section delivery under spinal anesthesia in University of Gondar Comprehensive Specialized Hospital, 2019, cross sectional study. Int. J. Surg. Open 2021, 33, 100348. [Google Scholar] [CrossRef]
- Gaiser, R.R. Postdural Puncture Headache: An Evidence-Based Approach. Anesthesiol. Clin. 2017, 35, 157–167. [Google Scholar] [CrossRef] [PubMed]
- D’Antona, L.; Merchan MA, J.; Vassiliou, A.; Watkins, L.D.; Davagnanam, I.; Toma, A.K.; Matharu, M.S. Clinical Presentation, Investigation Findings, and Treatment Outcomes of Spontaneous Intracranial Hypotension Syndrome: A Systematic Review and Meta-analysis. JAMA Neurol. 2021, 78, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Porter, S.B. Perioperative ketamine for acute analgesia and beyond. Rom. J. Anaesth. Intensiv. Care 2019, 26, 67–73. [Google Scholar]
- Gardner, A.; Olson, B.; Lichtiger, M.J.A. Cerebrospinal-fluid pressure during dissociative anesthesia with ketamine. Anesthesiology 1971, 35, 226–228. [Google Scholar] [CrossRef]
- Wyte, S.; Shapiro, H.M.; Turner, P.; Harris, A.B. Ketamine-induced intracranial hypertension. Anesthesiology 1972, 36, 174–176. [Google Scholar] [CrossRef] [PubMed]
- Zangouei, A.; Zahraei, S.A.H.; Sabertanha, A.; Nademi, A.; Golafshan, Z.; Zangoue, M. Effect of low-dose intravenous ketamine on prevention of headache after spinal anesthesia in patients undergoing elective cesarean section: A double-blind clinical trial study. Anesthesiol. Pain Med. 2019, 9, e97249. [Google Scholar] [CrossRef]
- Sen, S.; Ozmert, G.; Aydin, O.N.; Baran, N.; Calskan, E. The persisting analgesic effect of low-dose intravenous ketamine after spinal anaesthesia for caesarean section. Eur. J. Anaesthesiol. 2005, 22, 518–523. [Google Scholar] [CrossRef] [PubMed]
- Menkiti, I.D.; Desalu, I.; Kushimo, O.T. Low-dose intravenous ketamine improves postoperative analgesia after caesarean delivery with spinal bupivacaine in African parturients. Int. J. Obstet. Anesth. 2012, 21, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Rahmanian, M.; Leysi, M.; Hemmati, A.A.; Mirmohammadkhani, M. The effect of low-dose intravenous ketamine on postoperative pain following cesarean section with spinal anesthesia: A randomized clinical trial. Oman Med. J. 2015, 30, 11–16. [Google Scholar] [CrossRef]
- Edipoglu, I.S.; Celik, F.S.; Omaygenc, D.O. Perioperative low-dose ketamine diminishes post-operative caesarean pain, nausea & vomiting after spinal anaesthesia. J. Istanb. Fac. Med.-Istanb. Tip Fak. Derg. 2017, 80, 7–12. [Google Scholar]
- Xu, Y.; Li, Y.; Huang, X.; Chen, D.; She, B.; Ma, D. Single bolus low-dose of ketamine does not prevent postpartum depression: A randomized, double-blind, placebo-controlled, prospective clinical trial. Arch. Gynecol. Obstet. 2017, 295, 1167–1174. [Google Scholar] [CrossRef]
- Yao, J.; Song, T.; Zhang, Y.; Guo, N.; Zhao, P. Intraoperative ketamine for reduction in postpartum depressive symptoms after cesarean delivery: A double-blind, randomized clinical trial. Brain Behav. 2020, 10, e01715. [Google Scholar] [CrossRef]
- Kose, E.A.; Honca, M.; Dal, D.; Akinci, S.B.; Aypar, U. Prophylactic ketamine to prevent shivering in parturients undergoing Cesarean delivery during spinal anesthesia. J. Clin. Anesth. 2013, 25, 275–280. [Google Scholar] [CrossRef]
- Hassanein, A.; Mahmoud, E. Effect of low dose ketamine versus dexamethasone on intraoperative nausea and vomiting during cesarean section under spinal anesthesia. Egypt. J. Anaesth. 2015, 31, 59–63. [Google Scholar] [CrossRef][Green Version]
- Lema, G.F.; Gebremedhn, E.G.; Gebregzi, A.H.; Desta, Y.T.; Kassa, A.A. Efficacy of intravenous tramadol and low-dose ketamine in the prevention of post-spinal anesthesia shivering following cesarean section: A double-blinded, randomized control trial. Int. J. Womens Health 2017, 9, 681–688. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.H.; Wang, S.-Y.; Yu, H.-Y.; Li, D.-Y.; Luo, S.-C.; Zheng, S.-S.; Wan, L.-F.; Duan, K.-M. Prophylactic use of ketamine reduces postpartum depression in Chinese women undergoing cesarean section. Psychiatry Res. 2019, 279, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Sarshivi, F.; Ghaderi, E.; Sarshivi, A.; Shami, S.; Nasseri, K. Intravenous ketamine for the prevention of post anesthetic shivering in spinal anesthesia: A randomized double-blind placebo-controlled trial. Acta Med. Iran. 2020, 58, 479–485. [Google Scholar] [CrossRef]
- Sachs, A.; Smiley, R. Post-dural puncture headache: The worst common complication in obstetric anesthesia. Semin. Perinatol. 2014, 38, 386–394. [Google Scholar] [CrossRef]
- Grände, P.O. Mechanisms behind postspinal headache and brain stem compression following lumbar dural puncture—A physiological approach. Acta Anaesthesiol. Scand. 2005, 49, 619–626. [Google Scholar] [CrossRef] [PubMed]
- Davignon, K.R.; Dennehy, K.C. Update on postdural puncture headache. Int. Anesthesiol. Clin. 2002, 40, 89–102. [Google Scholar] [CrossRef]
- Antoine, C.; Young, B.K. Cesarean section one hundred years 1920–2020: The Good, the Bad and the Ugly. J. Perinat. Med. 2020, 49, 5–16. [Google Scholar] [CrossRef]
- Kuntz, K.; Kokmen, E.; Stevens, J.C.; Miller, P.; Offord, K.P.; Ho, M.M. Post-lumbar puncture headaches: Experience in 501 consecutive procedures. Neurology 1992, 42, 1884. [Google Scholar] [CrossRef]
- Brownridge, P. The management of headache following accidental dural puncture in obstetric patients. Anaesth. Intensiv. Care 1983, 11, 4–15. [Google Scholar] [CrossRef]
- Haider, A.; Sulhan, S.; Watson, I.T.; Leonard, D.; Arrey, E.N.; Khan, U.; Nguyen, P.; Layton, K.F. Spontaneous Intracranial Hypotension Presenting as a “Pseudo-Chiari 1”. Cureus 2017, 9, e1034. [Google Scholar] [CrossRef]
- Angle, P.; Thompson, D.; Szalai, J.P.; Tang, S.L.T. Expectant management of postdural puncture headache increases hospital length of stay and emergency room visits. Can. J. Anaesth. 2005, 52, 397–402. [Google Scholar] [CrossRef] [PubMed]
- International Headache Society. Headache classification subcommittee of the international headache society. Cephalgia 2004, 24, 9–160. [Google Scholar]
- Ahmed, S.; Jayawarna, C.; Jude, E. Post lumbar puncture headache: Diagnosis and management. Postgrad. Med. J. 2006, 82, 713–716. [Google Scholar] [CrossRef] [PubMed]
- Dakwar, E.; Levin, F.; Foltin, R.W.; Nunes, E.V.; Hart, C.L. The Effects of Subanesthetic Ketamine Infusions on Motivation to Quit and Cue-Induced Craving in Cocaine-Dependent Research Volunteers. Biol. Psychiatry 2014, 76, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Sari, A.; Okuda, Y.; Takeshita, H. The effect of ketamine on cerebrospinal fluid pressure. Anesth. Analg. 1972, 51, 560–565. [Google Scholar] [CrossRef]
- Himmelseher, S.; Durieux, M.E. Revising a dogma: Ketamine for patients with neurological injury? Anesth. Analg. 2005, 101, 524–534. [Google Scholar] [CrossRef]
- Zeiler, F.; Teitelbaum, J.; West, M.; Gillman, L.M. The ketamine effect on intracranial pressure in nontraumatic neurological illness. J. Crit. Care 2014, 29, 1096–1106. [Google Scholar] [CrossRef]
- Godoy, D.; Badenes, R.; Pelosi, P.; Robba, C. Ketamine in acute phase of severe traumatic brain injury “an old drug for new uses?”. Crit. Care 2021, 25, 19. [Google Scholar] [CrossRef]
- Albanese, J.; Arnaud, S.; Rey, M.; Thomachot, L.; Alliez, B.; Martin, C. Ketamine decreases intracranial pressure and electroencephalographic activity in traumatic brain injury patients during propofol sedation. Anesthesiology 1997, 87, 1328–1334. [Google Scholar] [CrossRef]
- Cohen, L.; Athaide, V.; Wickham, M.E.; Doyle-Waters, M.M.; Rose, N.G.; Hohl, C.M. The effect of ketamine on intracranial and cerebral perfusion pressure and health outcomes: A systematic review. Ann. Emerg. Med. 2015, 65, 43–51.e2. [Google Scholar] [CrossRef]
- Morgan, C.J.; Mofeez, A.; Brandner, B.; Bromley, L.; Curran, H.V. Acute effects of ketamine on memory systems and psychotic symptoms in healthy volunteers. Neuropsychopharmacology 2004, 29, 208–218. [Google Scholar] [CrossRef] [PubMed]
- Wan, L.B.; Levitch, C.F.; Perez, A.M.; Brallier, J.W.; Iosifescu, D.V.; Chang, L.C.; Foulkes, A.; Mathew, S.J.; Charney, D.S.; Murrough, J.W. Ketamine safety and tolerability in clinical trials for treatment-resistant depression. J. Clin. Psychiatry 2015, 76, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Huang, J.; Yang, S.; Cui, C.; Ye, L.; Wang, S.-Y.; Yang, G.-P.; Pei, Q. Pharmacokinetics and Safety of Esketamine in Chinese Patients Undergoing Painless Gastroscopy in Comparison with Ketamine: A Randomized, Open-Label Clinical Study. Drug. Des. Dev. Ther. 2019, 13, 4135–4144. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author | Year | Number (K; C) | Age, Years (K; C) | BMI | Height, cm (K; C) | Weight, kg (K; C) | Surgery Time, min (K; C) | Ketamine Dose (mg/kg) | Needle Size (G) | Relevant Outcomes | Reported Results (K; C) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Sen, S. et al. [13]. | 2005 | 30; 30 | 26.3 ± 5.3; 27.1 ± 4.6 | / | 162 ± 6.1; 160.0 ± 5.2 | 78.1 ± 7.8; 73.2 ± 9.4 | 41.9 ± 9.2; 48.3 ± 6.4 | 0.15 | 25 | Headache, nausea | 1. Headache 2; 5 2. Nausea 2; 3 |
| Menkiti, I. D. et al. [14]. | 2012 | 28; 28 | 30.3 ± 4.0; 29.8 ± 3.1 | / | 1.64 ± 0.03; 1.61 ± 0.12 | 73.7 ± 6.2; 72.2 ± 5.0 | 56.3 ± 8.6; 55.6 ± 8.6 | 0.15 | 26 | Headaches, nausea, and vomiting | 1. Headaches 1; 1 2. Nausea 0; 2 3. Vomiting 2; 1 |
| Rahmanian, M. et al. [15]. | 2015 | 80; 80 | 27.4 ± 4.8; 27.6 ± 4.4 | / | / | 78.5 ± 11.9; 77.7 ± 10.8 | 40.2 ± 3.8; 39.8 ± 3.2 | 0.25 | 25 | Headaches, nausea, and vomiting | 1. Headaches 21; 27 2. Nausea 26; 25 3. Vomiting 15; 28 |
| Edipoglu, I. S. et al. [16]. | 2017 | 60; 60 | 28.68 ± 5.82; 28.43 ± 4.82 | 33.54 ± 4.61; 33.85 ± 4.94 | / | / | 27.30 ± 7.36; 27.93 ± 5.34 | 0.15 | 26 | Headaches, nausea, and vomiting | 1. Headaches 0; 2 2. Nausea 2; 11 3. Vomiting 2; 11 |
| Xu, Y. et al. [17]. | 2017 | 162; 163 | 31 ± 4; 32 ± 4 | 27 ± 3; 28 ± 3 | / | / | 43.8 ± 14.4; 44.0 ± 12.6 | 0.25 | 25 | Headaches and vomiting | 1. Headaches 8; 1 2. Vomiting 7; 2 |
| Zangouei, A. et al. [12]. | 2019 | 32; 32 | / | / | / | / | / | 0.15 | 27 | Headaches | 1. Headaches 10; 14 |
| Yao, J. et al. [18]. | 2020 | 153; 155 | 30 ± 4; 30 ± 3 | 29 ± 3; 28 ± 3 | / | / | / | 0.25 | / | Headaches | 1. Headache 15; 3 |
| Kose, E. A. et al. [19]. | 2013 | (30 + 30); 30 | {28.2(18–43) + 26.8 (20–45)}; 27.3 (18–43) | {26.9 ± 5.9+ 26.3 ± 6.1}; 27.8 ± 6.8 | / | / | 68 ± 6; 71 ± 5; 65 ± 7 | 0.25 and 0.5 | 25 | Nausea and vomiting | 1. Nausea 10; 13 2. Vomiting 5; 6 |
| Hassanein, A. et al. [20]. | 2015 | 45; 45 | 29.4 ± 7.2; 30 ± 6 | / | 163 ± 4; 162 ± 6.5 | 72 ± 9; 69 ± 13 | / | 0.4 | 25 | Nausea and vomiting | 1. Nausea 6; 13 2. Vomiting 4; 9 |
| Lema, G. F. et al. [21]. | 2017 | 41; 41 | 26 (6); 26 (7) | / | 160 (10); 160 (11) | 60 (9); 60 (14) | 50 (20); 45 (20) | 0.2 | 22–25 | Nausea and vomiting | 1. Nausea 5; 6 2. Vomiting 5; 6 |
| Ma, J. H. et al. [22]. | 2019 | 327; 327 | / | 27.5 ± 3.1; 29.4 ± 26.6 | / | / | / | 0.5 | 25 | Vomiting | 1. Vomiting 62; 30 |
| Sarshivi, F. et al. [23]. | 2020 | 45; 45 | 30.8 (±4.5); 29.8 (±4.5) | 29.4 ± 3.3; 29.1 ± 8.8 | 159.12 ± 4.52; 158.14 ± 4.22 | 68.19 ±5.48; 67.37 ± 8.12 | 51 (±18); 54 (±15) | 0.3 | 25 | Nausea and vomiting | 1. Nausea 18; 12 2. Vomiting 14; 8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liang, X.; Yang, X.; Liang, S.; Zhang, Y.; Ding, Z.; Guo, Q.; Huang, C. Effect of Intravenous Ketamine on Hypocranial Pressure Symptoms in Patients with Spinal Anesthetic Cesarean Sections: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 4129. https://doi.org/10.3390/jcm11144129
Liang X, Yang X, Liang S, Zhang Y, Ding Z, Guo Q, Huang C. Effect of Intravenous Ketamine on Hypocranial Pressure Symptoms in Patients with Spinal Anesthetic Cesarean Sections: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2022; 11(14):4129. https://doi.org/10.3390/jcm11144129
Chicago/Turabian StyleLiang, Xiaoshen, Xin Yang, Shuang Liang, Yu Zhang, Zhuofeng Ding, Qulian Guo, and Changsheng Huang. 2022. "Effect of Intravenous Ketamine on Hypocranial Pressure Symptoms in Patients with Spinal Anesthetic Cesarean Sections: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 11, no. 14: 4129. https://doi.org/10.3390/jcm11144129
APA StyleLiang, X., Yang, X., Liang, S., Zhang, Y., Ding, Z., Guo, Q., & Huang, C. (2022). Effect of Intravenous Ketamine on Hypocranial Pressure Symptoms in Patients with Spinal Anesthetic Cesarean Sections: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 11(14), 4129. https://doi.org/10.3390/jcm11144129