
Laser-Assisted In Situ Keratomileusis (LASIK) Enhancement for Residual Refractive Error after Primary LASIK

 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Primary LASIK
2.2. LASIK Enhancement
3. Results
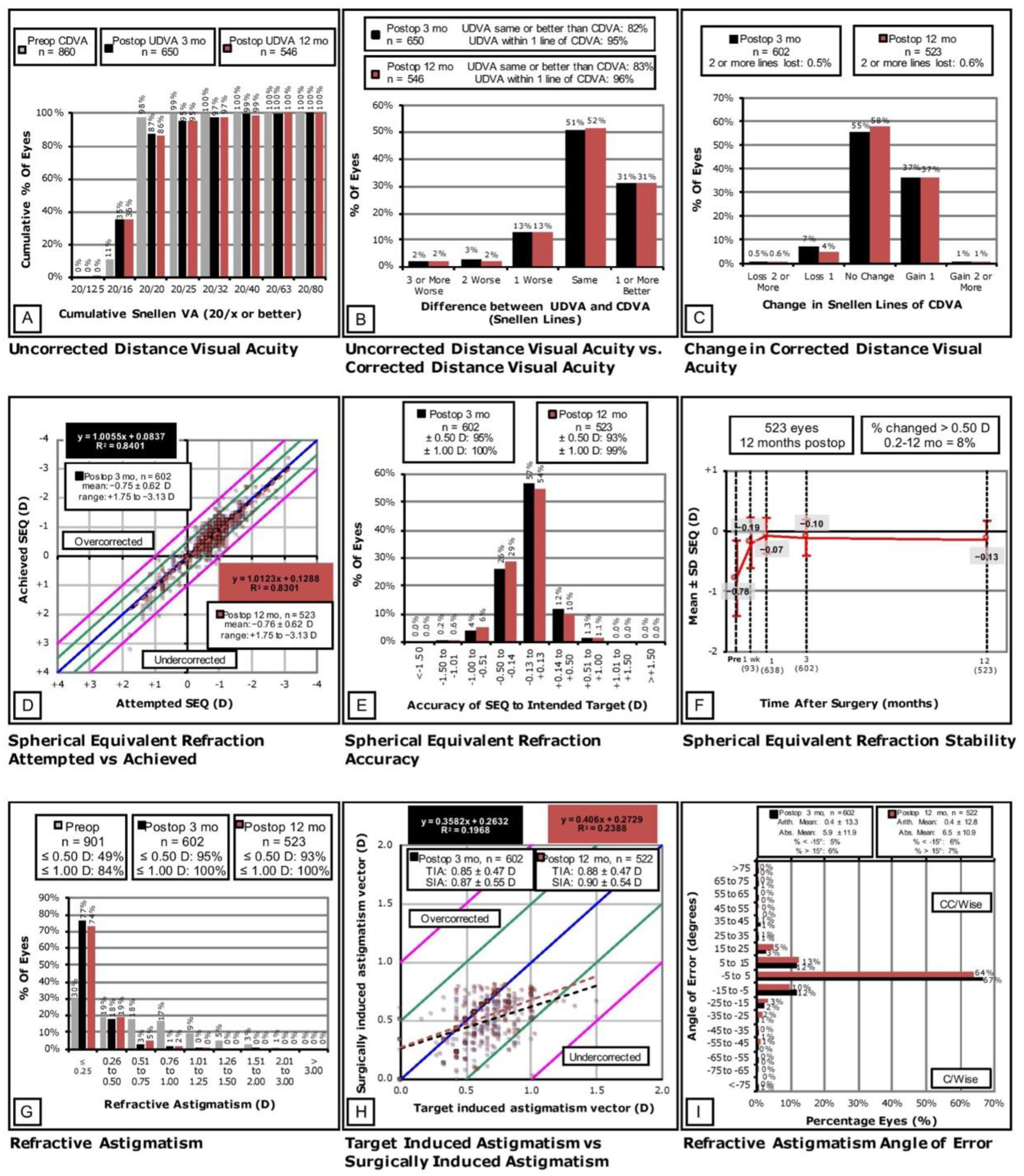
3.1. Efficacy
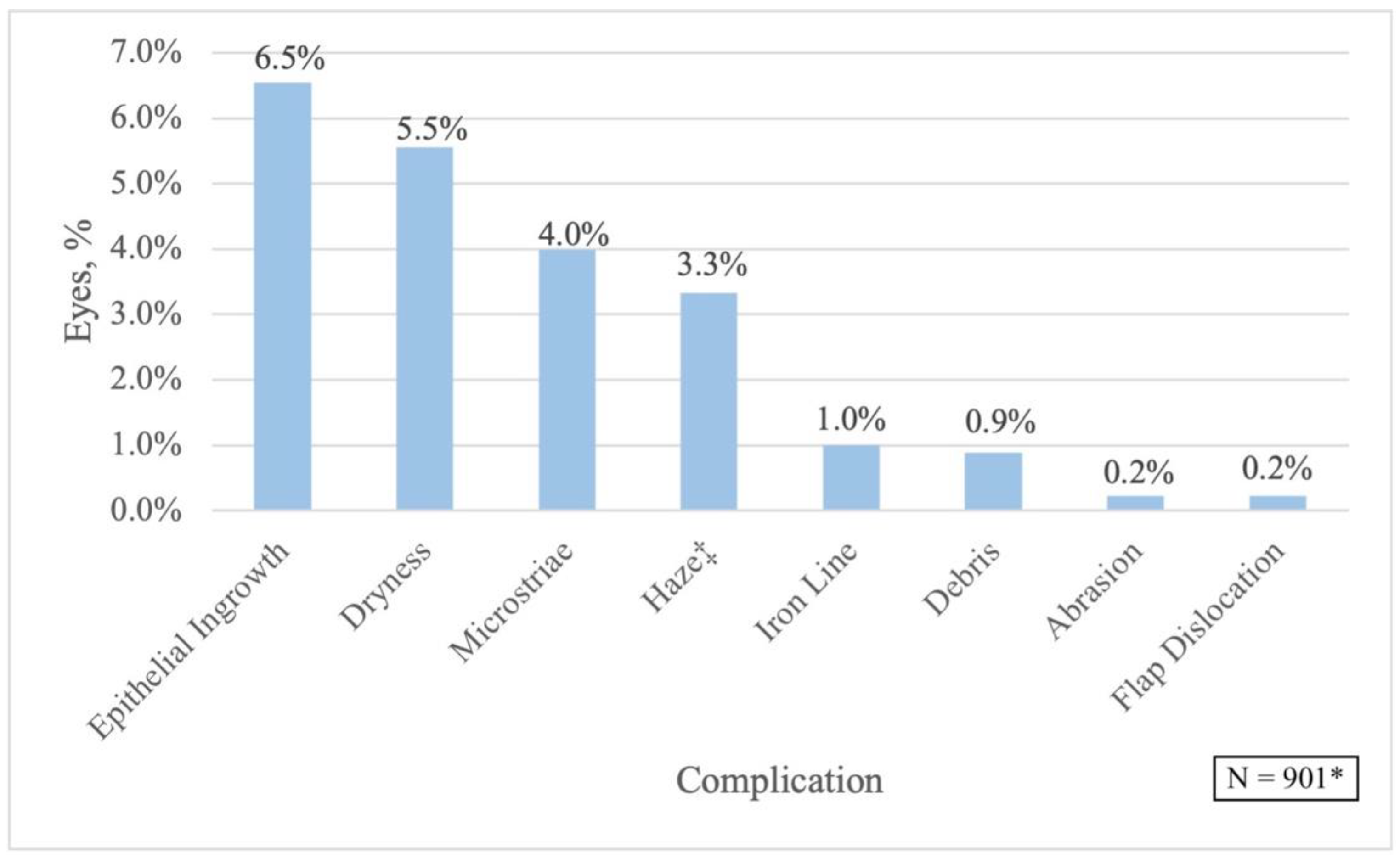
3.2. Safety
3.3. Predictability
3.4. Stability
3.5. Refractive Astigmatism
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Resnikoff, S.; Pascolini, D.; Mariotti, S.P.; Pokharel, G.P. Global magnitude of visual impairment caused by uncorrected refractive errors in 2004. Bull. World Health Organ. 2008, 86, 63. [Google Scholar] [CrossRef] [PubMed]
- McCarty, C.A.; Nanjan, M.B.; Taylor, H.R. Vision impairment predicts 5 year mortality. Br. J. Ophthalmol. 2001, 85, 322–326. [Google Scholar] [CrossRef] [PubMed]
- Smith, T. Potential lost productivity resulting from the global burden of uncorrected refractive error. Bull. World Health Organ. 2009, 87, 431–437. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, J.M.; Cozine, E.W.; Khan, A.R. Refractive Eye Surgery: Helping Patients Make Informed Decisions About LASIK. Am. Fam. Physician 2017, 95, 637–644. Available online: www.aafp.org/afp (accessed on 15 June 2022).
- Ambrósio, R.; Wilson, S.E. LASIK vs. LASEK vs. PRK: Advantages and indications. Semin. Ophthalmol. 2003, 18, 2–10. [Google Scholar] [CrossRef]
- Lim, S.A.; Park, Y.; Cheong, Y.J.; Na, K.S.; Joo, C.K. Factors Affecting Long-term Myopic Regression after Laser In Situ Keratomileusis and Laser-assisted Subepithelial Keratectomy for Moderate Myopia. Korean J. Ophthalmol. 2016, 30, 92. [Google Scholar] [CrossRef]
- Moshirfar, M.; Jehangir, N.; Fenzl, C.R.; McCaughey, M. LASIK Enhancement: Clinical and Surgical Management. J. Refract. Surg. 2017, 33, 116–127. [Google Scholar] [CrossRef]
- Yan, M.K.; Chang, J.S.M.; Chan, T.C.Y. Refractive regression after laser in situ keratomileusis. Clin. Exp. Ophthalmol. 2018, 46, 934–944. [Google Scholar] [CrossRef]
- Sharma, N.; Balasubramanya, R.; Sinha, R.; Titiyal, J.S.; Vajpayee, R.B. Retreatment of LASIK. J. Refract. Surg. 2006, 22, 396–401. [Google Scholar] [CrossRef]
- Quito, C.F.G.; Agahan, A.L.D.; Evangelista, R.P. Long-Term Followup of Laser In Situ Keratomileusis for Hyperopia Using a 213 nm Wavelength Solid-State Laser. ISRN Ophthalmol. 2013, 2013, 276984. [Google Scholar] [CrossRef]
- Hersh, P.S.; Fry, K.L.; Bishop, D.S. Incidence and associations of retreatment after LASIK. Ophthalmology 2003, 110, 748–754. [Google Scholar] [CrossRef]
- Premarket Approval (PMA). Available online: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpma/pma.cfm?id=P020050S023 (accessed on 21 June 2022).
- Reinstein, D.Z.; Waring, G.O. Graphic reporting of outcomes of refractive surgery. J. Refract. Surg. 2009, 25, 975–978. [Google Scholar] [CrossRef] [PubMed]
- Refractive Surgery Outcomes|London Vision Clinic. Available online: https://www.londonvisionclinic.com/refractivesurgeryoutcomes/ (accessed on 8 August 2022).
- Rojas, M.C.; Haw, W.W.; Manche, E.E. Laser in situ keratomileusis enhancement for consecutive hyperopia after myopic overcorrection. J. Cataract Refract. Surg. 2002, 28, 37–43. [Google Scholar] [CrossRef]
- Davis, E.A.; Hardten, D.R.; Lindstrom, M.; Samuelson, T.W.; Lindstrom, R.L. Lasik enhancements: A comparison of lifting to recutting the flap. Ophthalmology 2002, 109, 2308–2313. [Google Scholar] [CrossRef]
- Lyle, W.A.; Jin, G.J.C. Laser in situ keratomileusis for consecutive hyperopia after myopic LASIK and radial keratotomy. J. Cataract Refract. Surg. 2003, 29, 879–888. [Google Scholar] [CrossRef]
- Rani, A.; Balasubramanya, R.; Sharma, N.; Tandon, R.; Vajpayee, R.B.; Dada, V.K.; Singh, R. Outcomes after laser in situ keratomileusis retreatment in high myopes. J. Refract. Surg. 2003, 19, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Netto, M.V.; Wilson, S.E. Flap lift for LASIK retreatment in eyes with myopia. Ophthalmology 2004, 111, 1362–1367. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, G.S.; Park, D.H.; Lane, S.S. CustomCornea wavefront retreatment after conventional laser in situ keratomileusis. J. Cataract Refract. Surg. 2005, 31, 1502–1505. [Google Scholar] [CrossRef] [PubMed]
- Jin, G.J.C.; Merkley, K.H. Retreatment after Wavefront-Guided and Standard Myopic LASIK. Ophthalmology 2006, 113, 1623–1628. [Google Scholar] [CrossRef]
- Kanellopoulos, A.J.; Pe, L.H. Wavefront-guided enhancements using the wavelight excimer laser in symptomatic eyes previously treated with LASIK. J. Refract. Surg. 2006, 22, 345–349. [Google Scholar] [CrossRef]
- Alió, J.L.; Galal, A.; Artola, A.; Ayala, M.J.; Merayo, J. Hyperopic LASIK retreatments with the technolas laser. J. Refract. Surg. 2006, 22, 596–603. [Google Scholar] [CrossRef] [PubMed]
- Montague, A.A.; Manche, E.E. CustomVue laser in situ keratomileusis treatment after previous keratorefractive surgery. J. Cataract Refract. Surg. 2006, 32, 795–798. [Google Scholar] [CrossRef]
- Alió, J.L.; Montés-Mico, R. Wavefront-Guided versus Standard LASIK Enhancement for Residual Refractive Errors. Ophthalmology 2006, 113, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Saeed, A.; O’Doherty, M.; O’Doherty, J.; O’Keefe, M. Analysis of the visual and refractive outcome following laser in situ keratomileusis (LASIK) retreatment over a four-year follow-up period. Int. Ophthalmol. 2007, 27, 23–29. [Google Scholar] [CrossRef]
- Harter, D.E.; Hardten, D.R. Retreatment after LASIK using epithelial ablation alone. J. Refract. Surg. 2007, 23, 518–520. [Google Scholar] [CrossRef]
- Ortega-Usobiaga, J.; Cobo-Soriano, R.; Llovet, F.; Ramos, F.; Beltrán, J.; Baviera-Sabater, J. Retreatment of Hyperopia After Primary Hyperopic LASIK. J. Refract. Surg. 2007, 23, 201–205. [Google Scholar] [CrossRef]
- Urbano, A.P.; Nosé, W. Refractional results of LASIK retreatment with wavefront-guided ablation versus standard ablation. Arq. Bras. Oftalmol. 2008, 71, 651–659. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Bragheeth, M.A.; Fares, U.; Dua, H.S. Re-treatment after laser in situ keratomileusis for correction of myopia and myopic astigmatism. Br. J. Ophthalmol. 2008, 92, 1506–1510. [Google Scholar] [CrossRef]
- Bababeygy, S.R.; Zoumalan, C.I.; Chien, F.Y.; Manche, E.E. Wavefront-guided laser in situ keratomileusis retreatment for consecutive hyperopia and compound hyperopic astigmatism. J. Cataract Refract. Surg. 2008, 34, 1260–1266. [Google Scholar] [CrossRef]
- Kashani, S.; Rajan, M.; Gartry, D. Wavefront-Guided Retreatment After Primary Wavefront-Guided Laser In Situ Keratomileusis in Myopes and Hyperopes: Long-term Follow-up. Am. J. Ophthalmol. 2009, 147, 417–423.e2. [Google Scholar] [CrossRef]
- McAlinden, C.; Moore, J.E. Retreatment of residual refractive errors with flap lift laser in situ keratomileusis. Eur. J. Ophthalmol. 2011, 21, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Coskunseven, E.; Kymionis, G.D.; Grentzelos, M.A.; Portaliou, D.M.; Kolli, S.; Jankov, M.R. Femtosecond LASIK retreatment using side cutting only. J. Refract. Surg. 2012, 28, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Santhiago, M.R.; Smadja, D.; Zaleski, K.; Espana, E.M.; Armstrong, B.K.; Wilson, S.E. Flap Relift for Retreatment After Femtosecond Laser–assisted LASIK. J. Refract. Surg. 2012, 28, 482–487. [Google Scholar] [CrossRef] [PubMed]
- Schallhorn, S.C.; Venter, J.A.; Hannan, S.J.; Hettinger, K.A.; Teenan, D. Flap lift and photorefractive keratectomy enhancements after primary laser in situ keratomileusis using a wavefront-guided ablation profile: Refractive and visual outcomes. J. Cataract Refract. Surg. 2015, 41, 2501–2512. [Google Scholar] [CrossRef]
- Frings, A.; Intert, E.; Steinberg, J.; Druchkiv, V.; Linke, S.J.; Katz, T. Outcomes of retreatment after hyperopic laser in situ keratomileusis. J. Cataract Refract. Surg. 2017, 43, 1436–1442. [Google Scholar] [CrossRef] [PubMed]
- Caster, A.I. Flap-Lift LASIK 10 or More Years After Primary LASIK. J. Refract. Surg. 2018, 34, 604–609. [Google Scholar] [CrossRef]
- Ortega-Usobiaga, J.; Llovet-Osuna, F.; Katz, T.; Djodeyre, M.; Druchkiv, V.; Bilbao-Calabuig, R.; Baviera, J. Comparison of 5468 retreatments after laser in situ keratomileusis by lifting the flap or performing photorefractive keratectomy on the flap. Arch. Soc. Esp. Oftalmol. 2018, 93, 60–68. [Google Scholar] [CrossRef]
- Alió del Barrio, J.L.; Hanna, R.; Canto-Cerdan, M.; Vega-Estrada, A.; Alió, J.L. Laser flap enhancement 5 to 9 years and 10 or more years after laser in situ keratomileusis: Safety and efficacy. J. Cataract Refract. Surg. 2019, 45, 1463–1469. [Google Scholar] [CrossRef]
- Chan, C.; Lawless, M.; Sutton, G.; Hodge, C. Re-treatment in LASIK: To Flap Lift or Perform Surface Ablation. J. Refract. Surg. 2020, 36, 6–11. [Google Scholar] [CrossRef]
- Bamashmus, M.; Al-Akhlee, H.; Al-Azani, Y.; Al-Kershy, N. Results of laser enhancement for residual myopia after primary laser in situ keratomileusis. Taiwan J. Ophthalmol. 2019, 10, 264–268. [Google Scholar] [CrossRef]
- Lee, M.D.; Chen, L.Y.; Tran, E.M.; Manche, E.E. A Prospective Comparison of Wavefront-Guided LASIK versus Wavefront-Guided PRK After Previous Keratorefractive Surgery. Clin. Ophthalmol. 2020, 14, 3411. [Google Scholar] [CrossRef] [PubMed]
- Hecht, I.; Mimouni, M.; Rabina, G.; Kaiserman, I. Re-Treatment by Flap Relift Versus Surface Ablation After Myopic Laser In Situ Keratomileusis. Cornea 2020, 39, 443–450. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.S.M.; Liu, S.C.T.; Ma, N.T.C.; Katsev, B.; Ng, J.C.M. Effect of time since primary laser-assisted in situ keratomileusis on flap relift success and epithelial ingrowth risk. J. Cataract Refract. Surg. 2022, 48, 705–709. [Google Scholar] [CrossRef] [PubMed]
- Kruh, J.N.; Garrett, K.A.; Huntington, B.; Robinson, S.; Melki, S.A. Risk Factors for Retreatment Following Myopic LASIK with Femtosecond Laser and Custom Ablation for the Treatment of Myopia. Semin. Ophthalmol. 2017, 32, 316–320. [Google Scholar] [CrossRef] [PubMed]
- Eser, I.; Durrie, D.S.; Schwendeman, F.; Stahl, J.E. Association between ocular dominance and refraction. J. Refract. Surg. 2008, 24, 685–689. [Google Scholar] [CrossRef]
- López-Prats, M.J.; Hidalgo-Mora, J.J.; Sanz-Marco, E.; Pellicer, A.; Perales, A.; Díaz-Llopis, M. Influencia del embarazo sobre los parámetros refractivos tras cirugía laser in situ keratomileusis. Arch. De La Soc. Esp. De Oftalmol. 2012, 87, 173–178. [Google Scholar] [CrossRef]
- Kanellopoulos, A.J.; Vingopoulos, F. Does pregnancy affect refractive and corneal stability or corneal epithelial remodeling after myopic LASIK? J. Refract. Surg. 2020, 36, 118–122. [Google Scholar] [CrossRef]
- Wang, M.Y.; Maloney, R.K. Epithelial ingrowth after laser in situ keratomileusis. Am. J. Ophthalmol. 2000, 129, 746–751. [Google Scholar] [CrossRef]
- Pérez-Santonja, J.J.; Ayala, M.J.; Sakla, H.F.; Ruíz-Moreno, J.M.; Alió, J.L. Retreatment after laser in situ keratomileusis. Ophthalmology 1999, 106, 21–28. [Google Scholar] [CrossRef]
- Mackool, R.J.; Monsanto, V.R. Epithelial ingrowth after LASIK. J. Cataract Refract. Surg. 2002, 28, 1884. [Google Scholar] [CrossRef]
- Wilson, S.E.; Santhiago, M.R. Flaporhexis: Rapid and effective technique to limit epithelial ingrowth after LASIK enhancement. J. Cataract Refract. Surg. 2012, 38, 2–4. [Google Scholar] [CrossRef] [PubMed]
- Cosgrove, R.J.; Borr, M.J.; Keil, M.L. Disruption of ingrown epithelium via Nd:YAG laser or DIEYAG. A retrospective case series of Post-LASIK patients. Am. J. Ophthalmol. Case Rep. 2021, 22, 101071. [Google Scholar] [CrossRef] [PubMed]
- Rojas, M.C.; Lumba, J.D.; Manche, E.E. Treatment of epithelial ingrowth after laser in situ keratomileusis with mechanical debridement and flap suturing. Arch. Ophthalmol. 2004, 122, 997–1001. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Caster, A.I.; Friess, D.W.; Schwendeman, F.J. Incidence of epithelial ingrowth in primary and retreatment laser in situ keratomileusis. J. Cataract Refract. Surg. 2010, 36, 97–101. [Google Scholar] [CrossRef]
- Christiansen, S.M.; Neuffer, M.C.; Sikder, S.; Semnani, R.T.; Moshirfar, M. The effect of preoperative keratometry on visual outcomes after moderate myopic LASIK. Clin. Ophthalmol. 2012, 6, 459–464. [Google Scholar] [CrossRef]
- Young, J.J.; Schallhorn, S.C.; Brown, M.C.; Hettinger, K.A. Effect of keratometry on visual outcomes 1 month after hyperopic LASIK. J. Refract. Surg. 2009, 25 (Suppl. 7), S672–S676. [Google Scholar] [CrossRef]
- Djodeyre, M.R.; Beltran, J.; Ortega-Usobiaga, J.; Gonzalez-Lopez, F.; Ruiz-Rizaldos, A.I.; Baviera, J. Long-term evaluation of eyes with central corneal thickness <400 μm following laser in situ keratomileusis. Clin. Ophthalmol. 2016, 10, 535. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Preoperative Parameters a | LASIK Enhancement after LASIK N = 901 | LASIK with No Enhancement N = 1127 | p-Value |
|---|---|---|---|
| Age, years Mean ± SD Range | 37.56 ± 9.051 (22 to 62) | 33.88 ± 8.392 (18 to 65) | <0.0001 * |
| Sex (n, %) Male Female | 372 (41.29) 529 (58.71) | 558 (49.51) 569 (50.49) | 0.0002 * |
| Surgical Eye (n, %) Right Left | 532 (59.05) 369 (40.95) | 588 (52.17) 539 (47.83) | 0.002 * |
| CDVA, logMAR Mean ± SD Range | −0.005 ± 0.037 (−0.13 to +0.18) | −0.006 ± 0.034 (−0.13 to +0.30) | 0.314 |
| Sphere, D Mean ± SD Range | −3.697 ± 2.831 (−11.50 to +6.00) | −3.242 ± 2.229 (−12.50 to +4.50) | <0.0001 * |
| Cylinder, D Mean ± SD Range | −1.291 ± 1.238 (−7.25 to 0.00) | −0.900 ± 0.944 (−7.25 to 0.00) | <0.0001 * |
| SE, D Mean ± SD Range | −4.006 ± 2.849 (−12.13 to +5.75) | −3.692 ± 2.186 (−12.50 to 2.88) | 0.004 * |
| Parameter | FDA Criteria % | 3 mo Post-Enhancement % | 12 mo Post-Enhancement % | |
|---|---|---|---|---|
| Safety | Treated eyes with each ocular serious adverse event | <1 | 0 | 0 |
| Loss of at least 2 lines of CDVA | <5 | 0.5 | 0.6 | |
| Preoperative CDVA 20/20 or better with postoperative CDVA worse than 20/40 | <1 | 0 | 0.4 | |
| >2.00 D induced MRC at refractive stability compared to baseline value | <5 | 0 | 0 | |
| Efficacy | Preoperative CDVA 20/20 or better with postoperative UDVA of 20/40 or better | ≥85 | 99 | 99 |
| Stability | Change of ≤1.00 D in MRC and MRSE between two refractions postoperatively, either at 1 and 3 months, or over 3 months | ≥95 | 100 | 100 |
| Predictability | Achievement of MRSE within ±0.50 D of target outcome | ≥50 | 95 | 93 |
| Achievement of MRSE within ±1.00 D of target outcome | ≥75 | 100 | 99 |
| Study | Year | Eyes, n | Interval between Procedures, Months | Mean/Main Follow-Up Interval, Months | UDVA 20/20 or Better, % | UDVA 20/40 or Better, % | CDVA Loss of 1 Line, % | CDVA Loss of ≥2 Line, % | MRSE within ±0.50 D of Intended, % | MRSE within ±1.00 D of Intended, % |
|---|---|---|---|---|---|---|---|---|---|---|
| Rojas [15] | 2002 | 36 | 7.83 | 3 | 66.6 | 94.4 | 28 | 0 | 55.6 | 94.4 |
| Davis a [16] | 2002 | 164 | 10 | 4.8 | 44.4 | 98.1 | - | - | - | - |
| 48 | 10.9 | 5.63 | 21.1 | 78.9 | - | - | - | - | ||
| Lyle [17] | 2003 | 34 | 15.5 | 11.53 | 37 | 93 | 7 | 0 | 59 | 81 |
| Rani [18] | 2003 | 33 | 6.48 | 6 | - | 91 | 0 | 0 | - | - |
| Netto [19] | 2004 | 334 | 8 | 12 | 58 | 92 | 5 | 1 | 80 | 96 |
| Schwartz [20] | 2005 | 14 | 10.8 | 5.3 | - | - | 0 | 0 | 71.4 | 78.6 |
| Jin a [21] | 2006 | 53 | 6.1 | 6.9 | 75 | - | 26 | 0 | 91 | 100 |
| 101 | 10.1 | 8.3 | 75 | - | 13 | 0 | 87 | 96 | ||
| Kanellopoulos [22] | 2006 | 22 | - | 8 | - | - | 0 | 0 | 100 | 100 |
| Alio a [23] | 2006 | 44 | 6.4 | 12 | - | 72.6 | 20.5 | 31.8 | 70.5 | 84.1 |
| 41 | - | 73.2 | 19.5 | 29.2 | 46.4 | 63.4 | ||||
| Montague b [24] | 2006 | 120 | - | 1 | 92.3 | 100 | 12 | 1 | 91 | 100 |
| 3 | 88.1 | 100 | 5 | 0 | 83 | 100 | ||||
| Alio a [25] | 2006 | 20 | >3 | 6 | - | 100 | 0 | 0 | 94.4 | 100 |
| 20 | - | 100 | 0 | 0 | 88.8 | 100 | ||||
| Saeed [26] | 2007 | 60 | 7.8 | 22.3 | 60 | 95 | 0 | 0 | 77 | 83 |
| Harter [27] | 2007 | 27 | - | 12 | 28.6 | 100 | 0 | 0 | 57.1 | 100 |
| Ortega-Usobiaga [28] | 2007 | 86 | 5.54 | 5.62 | 53.49 | 98.84 | 17.44 | 4.65 | 72.09 | 96.51 |
| Urbano a [29] | 2008 | 37 | 18.07 | 6 | 93.3 | 100 | 3.3 | 0 | 93.6 | 100 |
| 37 | 86.7 | 100 | 13.3 | 0 | 86.7 | 100 | ||||
| Bragheeth [30] | 2008 | 34 | >3 | 12 | 43 | 89 | 20 | 0 | 56 | 78 |
| Bababeygy [31] | 2008 | 19 | 23.6 | 1 | 55.6 | - | 15.8 | 0 | 55.6 | 66.7 |
| 3 | 66.7 | - | 11.1 | 0 | 55.6 | 88.9 | ||||
| Kashani a [32] | 2009 | 46 | 7.8 | 17.75 | 86.9 | 97.8 | 15.2 | 0 | 82.6 | 95.6 |
| 17 | 11 | 14.6 | 70.6 | 88.2 | 7.6 | 0 | 88.2 | 100 | ||
| McAlinden [33] | 2011 | 60 | 8.3 | 6 | 73.3 | - | 3.3 | 0 | 88.3 | 98.3 |
| Coskunseven c [34] | 2012 | 11 | 18.18 | 7.72 | - | - | 0 | 0 | - | - |
| Santhiago [35] | 2012 | 88 | 7.3 | 1 d–12 | 82 | 95 | 2.2 | 1.1 | - | - |
| Schallhorn [36] | 2015 | 119 | 14 | 4 | 87.4 | 100 | 10.1 | 0.8 | 87.4 | 99.2 |
| Frings [37] | 2017 | 113 | 10.41 | 1–12 | - | - | 8 | 0 | 78 | - |
| Caster [38] | 2018 | 23 | 13.9 | - | 70 | 100 | 4 | 0 | 85 | 100 |
| Ortega-Usobiaga a [39] | 2018 | 3772 | 14 | 12 h–3 | - | - | - | 0.2 | 81.9 | 93.6 |
| 1424 | 17 | - | - | - | 0.6 | 70.3 | 85.2 | |||
| Alio del Barrio a [40] | 2019 | 40 | 12.3y | 3 | 88 | 100 | 14 | 0 | 97 | 100 |
| 19 | 74 | 100 | 12 | 0 | 76 | 88 | ||||
| Chan [41] | 2020 | 58 | 27.4 | 7.18 | 91.5 | 100 | 17.2 | 0 | - | - |
| Bamashmus [42] | 2020 | 112 | 15.5 | 12 | 43.8 | 92.8 | 1.8 | 0.9 | 83.9 | 94.6 |
| Lee [43] | 2020 | 12 | 14.5 | 6.3 | 92 | 100 | 18.2 | 0 | 100 | 100 |
| Hecht [44] | 2020 | 263 | 29 | 5.16 | 49 | 96 | 14 | 1.5 | 73 | 90.8 |
| Chang [45] | 2022 | 73 | 8.6 | 4.3 | - | - | 9 | 0 | - | - |
| Current Study | 2022 | 901 | 15.33 | 3 | 87 | 99 | 7 | 0.5 | 95 | 100 |
| 12 | 86 | 99 | 4 | 0.6 | 93 | 99 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moshirfar, M.; Basharat, N.F.; Bundogji, N.; Ungricht, E.L.; Darquea, I.M.; Conley, M.E.; Ronquillo, Y.C.; Hoopes, P.C. Laser-Assisted In Situ Keratomileusis (LASIK) Enhancement for Residual Refractive Error after Primary LASIK. J. Clin. Med. 2022, 11, 4832. https://doi.org/10.3390/jcm11164832
Moshirfar M, Basharat NF, Bundogji N, Ungricht EL, Darquea IM, Conley ME, Ronquillo YC, Hoopes PC. Laser-Assisted In Situ Keratomileusis (LASIK) Enhancement for Residual Refractive Error after Primary LASIK. Journal of Clinical Medicine. 2022; 11(16):4832. https://doi.org/10.3390/jcm11164832
Chicago/Turabian StyleMoshirfar, Majid, Noor F. Basharat, Nour Bundogji, Emilie L. Ungricht, Ines M. Darquea, Matthew E. Conley, Yasmyne C. Ronquillo, and Phillip C. Hoopes. 2022. "Laser-Assisted In Situ Keratomileusis (LASIK) Enhancement for Residual Refractive Error after Primary LASIK" Journal of Clinical Medicine 11, no. 16: 4832. https://doi.org/10.3390/jcm11164832
APA StyleMoshirfar, M., Basharat, N. F., Bundogji, N., Ungricht, E. L., Darquea, I. M., Conley, M. E., Ronquillo, Y. C., & Hoopes, P. C. (2022). Laser-Assisted In Situ Keratomileusis (LASIK) Enhancement for Residual Refractive Error after Primary LASIK. Journal of Clinical Medicine, 11(16), 4832. https://doi.org/10.3390/jcm11164832