
Long-Term Prognosis after Coronary Artery Bypass Grafting: The Impact of Arterial Stiffness and Multifocal Atherosclerosis


Abstract
1. Introduction
2. Methods
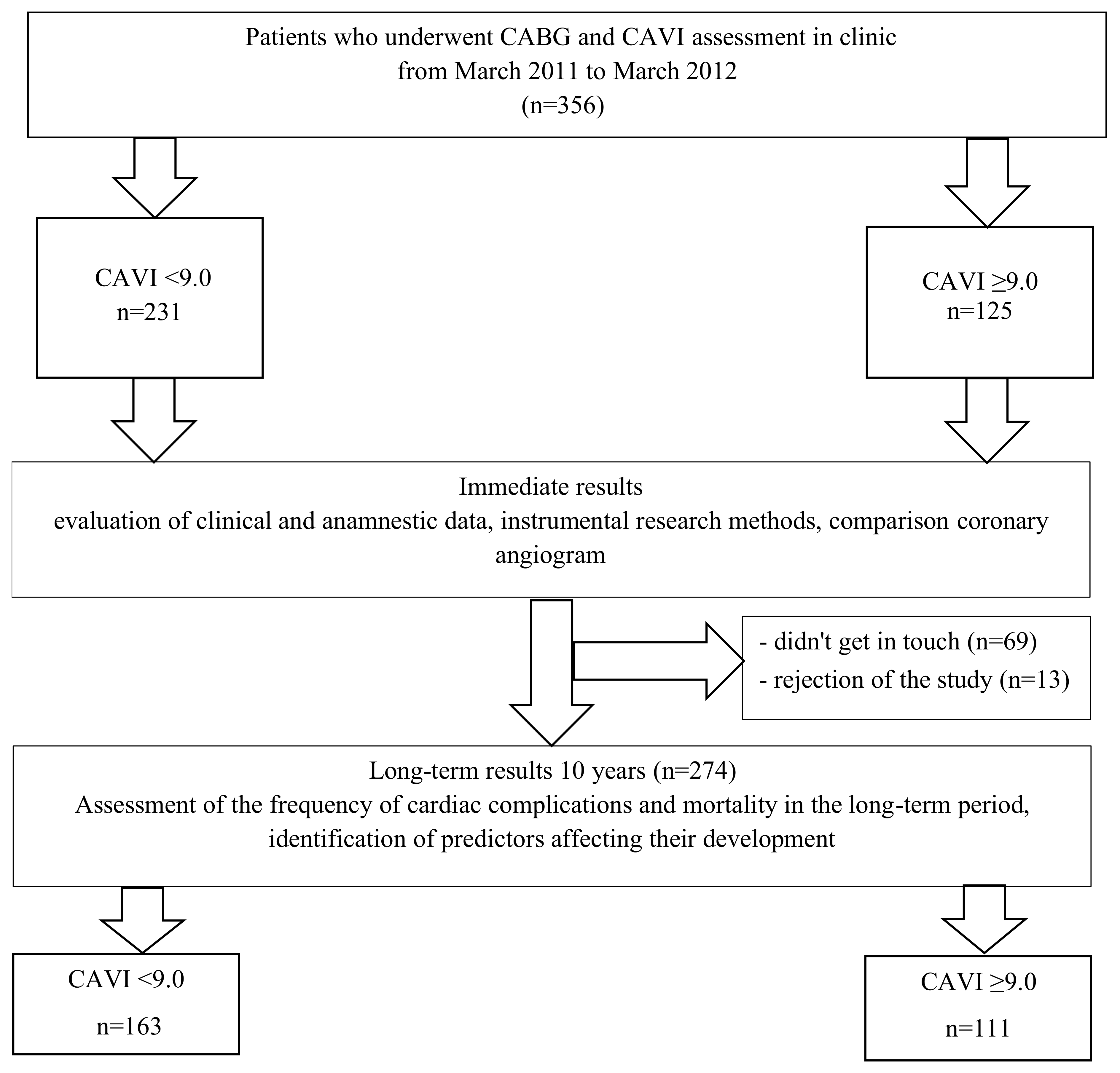
2.1. Participants
2.2. Baseline Data
2.3. Measurement of CAVI
2.4. Duplex Ultrasonography Assessment
2.5. Echocardiographic Examination
2.6. Follow-Up
2.7. Statistical Analysis
3. Results
3.1. Baseline Characteristics
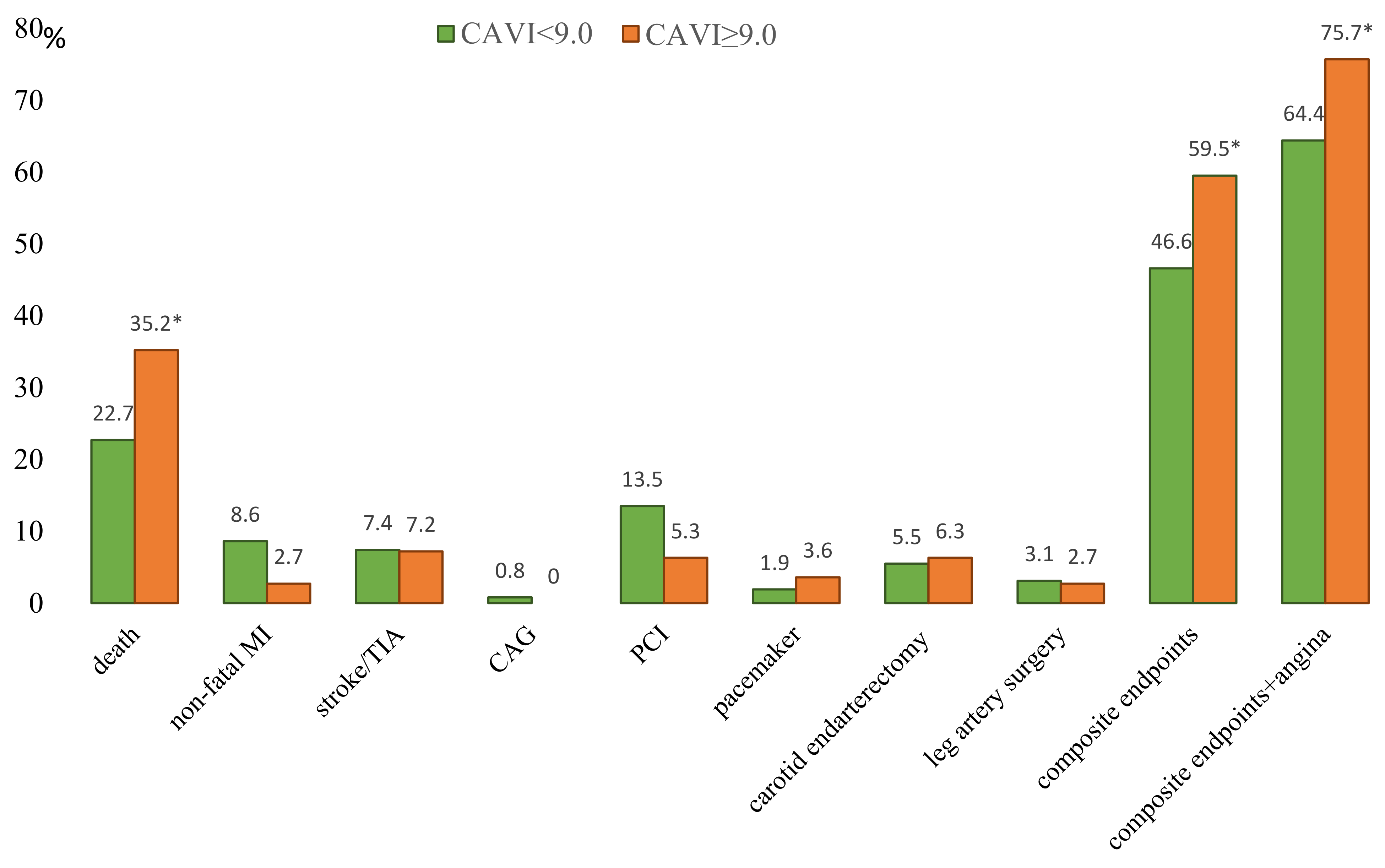
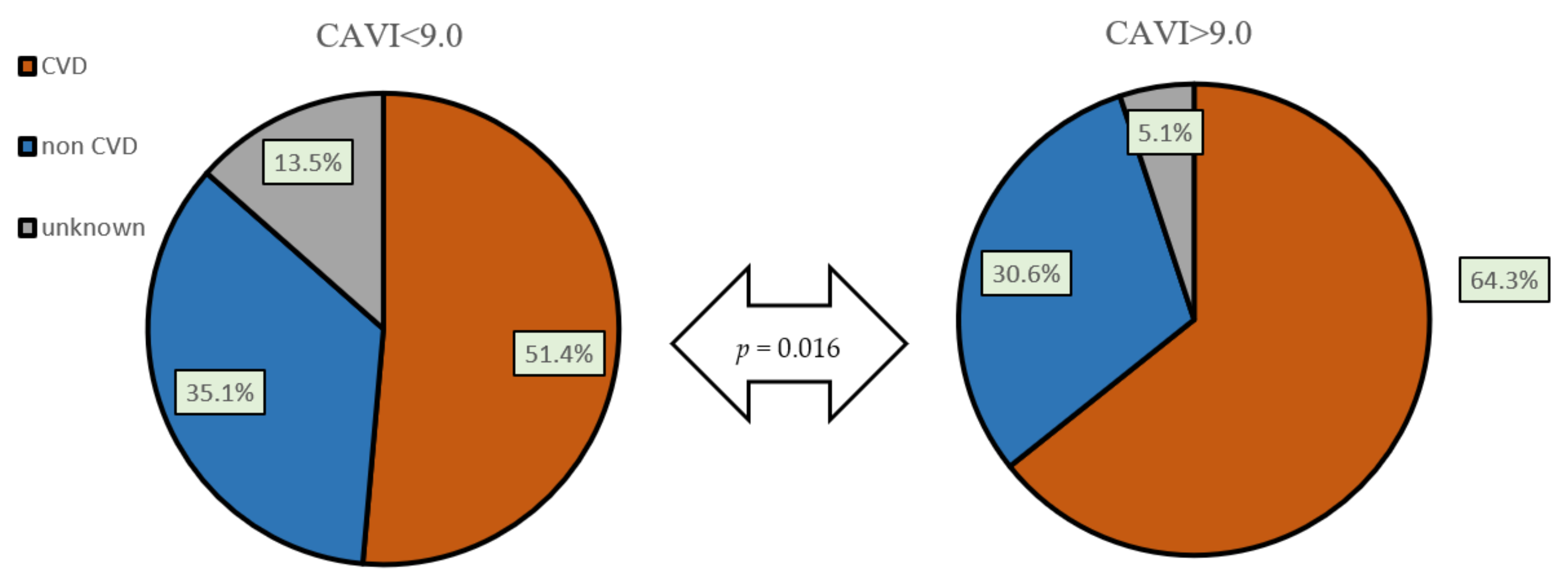
3.2. Long-Time Outcomes after CABG in Patients with Pathological and Normal CAVI
3.3. Predictors of the Unfavorable Long-Time Outcomes after CABG (Binary Logistic Regression Analysis, Forward LR Method)
4. Discussion
5. Study Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. ESC Scientific Document Group. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef] [PubMed]
- Sattartabar, B.; Ajam, A.; Pashang, M.; Jalali, A.; Sadeghian, S.; Mortazavi, H.; Mansourian, S.; Bagheri, J.; Karimi, A.A.; Hosseini, K. Sex and age difference in risk factor distribution, trend, and long-term outcome of patients undergoing isolated coronary artery bypass graft surgery. BMC Cardiovasc. Disord. 2021, 21, 460. [Google Scholar] [CrossRef] [PubMed]
- Morikami, Y.; Natsuaki, M.; Morimoto, T.; Ono, K.; Nakagawa, Y.; Furukawa, Y.; Sakata, R.; Aota, M.; Okada, Y.; Onoe, M.; et al. CREDO-Kyoto PCI/CABG registry cohort-2 investigators. Impact of polyvascular disease on clinical outcomes in patients undergoing coronary revascularization: An observation from the CREDO-Kyoto Registry Cohort-2. Atherosclerosis 2013, 228, 426–431. [Google Scholar] [CrossRef] [PubMed]
- Gajfulin, R.A.; Sumin, A.N.; Ivanov, S.V.; Barbarash, L.S. Survival after surgical treatment of multifocal atherosclerosis in different age groups. Kompleks. Probl. Serdechno-Sosud. Zabol. 2017, 6, 6–18. (In Russian) [Google Scholar] [CrossRef][Green Version]
- Le Bivic, L.; Magne, J.; Blossier, J.D.; Piccardo, A.; Wojtyna, H.; Lacroix, P.; Mohty, D.; Cornu, E.; Le Guyader, A.; Aboyans, V. Mid- and long-term prognosis of off- vs. on-pump coronary artery bypass graft in patients with multisite artery disease. J. Cardiovasc. Surg. 2019, 60, 388–395. [Google Scholar] [CrossRef]
- Huang, N.W.; Lin, J.H.; Jhan, J.Y.; Hsu, B.G.; Chang, J.C. Age and Serum Adipocyte Fatty-Acid-Binding Protein Level Are Associated with Aortic Stiffness in Coronary Artery Bypass Graft Patients. J. Cardiovasc. Dev. Dis. 2022, 9, 105. [Google Scholar] [CrossRef]
- Janner, J.H.; Godtfredsen, N.S.; Ladelund, S.; Vestbo, J.; Prescott, E. High aortic augmentation index predicts mortality and cardiovascular events in men from a general population, but not in women. Eur. J. Prev. Cardiol. 2013, 20, 1005–1012. [Google Scholar] [CrossRef]
- Ikonomidis, I.; Makavos, G.; Lekakis, J. Arterial stiffness and coronary artery disease. Curr. Opin. Cardiol. 2015, 30, 422–431. [Google Scholar] [CrossRef]
- Maruhashi, T.; Soga, J.; Fujimura, N.; Idei, N.; Mikami, S.; Iwamoto, Y.; Iwamoto, A.; Kajikawa, M.; Matsumoto, T.; Oda, N.; et al. Endothelial Dysfunction, Increased Arterial Stiffness, and Cardiovascular Risk Prediction in Patients with Coronary Artery Disease: FMD-J (Flow-Mediated Dilation Japan) Study A. J. Am. Heart Assoc. 2018, 7, e008588. [Google Scholar] [CrossRef]
- Park, H.W.; Kang, M.G.; Kim, K.; Koh, J.S.; Park, J.R.; Hwang, S.J.; Jeong, Y.H.; Ahn, J.H.; Jang, J.Y.; Kwak, C.H.; et al. Prognostic value of brachial-ankle pulse wave velocity in patients with non-ST-elevation myocardial infarction. Coron. Artery Dis. 2017, 28, 642–648. [Google Scholar] [CrossRef]
- Park, H.W.; Kim, H.R.; Kang, M.G.; Kim, K.; Koh, J.S.; Park, J.R.; Hwang, S.J.; Jeong, Y.H.; Ahn, J.H.; Park, Y.; et al. Predictive value of the combination of brachial-ankle pulse wave velocity and ankle-brachial index for cardiovascular outcomes in patients with acute myocardial infarction. Coron. Artery Dis. 2020, 31, 157–165. [Google Scholar] [CrossRef]
- Chen, B.W.; Wang, Z.G.; Liu, Q.; Wang, X.; Dang, A. Combination of pulse wave velocity with clinical factors as a promising tool to predict major adverse cardiac events after percutaneous coronary intervention. J. Cardiol. 2015, 65, 318–323. [Google Scholar] [CrossRef][Green Version]
- Fontes, M.L.; Aronson, S.; Mathew, J.P.; Miao, Y.; Drenger, B.; Barash, P.G.; Mangano, D.T. Multicenter Study of Perioperative Ischemia (McSPI) Research Group; Ischemia Research and Education Foundation (IREF) Investigators. Pulse pressure and risk of adverse outcome in coronary bypass surgery. Anesth. Analg. 2008, 107, 1122–1129. [Google Scholar] [CrossRef]
- Nikolov, N.M.; Fontes, M.L.; White, W.D.; Aronson, S.; Bar-Yosef, S.; Gaca, J.G.; Podgoreanu, M.V.; Stafford-Smith, M.; Newman, M.F.; Mathew, J.P. Pulse pressure and long-term survival after coronary artery bypass graft surgery. Anesth. Analg. 2010, 110, 335–340. [Google Scholar] [CrossRef]
- Laurent, S.; Cockcroft, J.; Van Bortel, L.; Boutouyrie, P.; Giannattasio, C.; Hayoz, D.; Pannier, B.; Vlachopoulos, C.; Wilkinson, I.; Struijker-Boudier, H. European Network for Non-invasive Investigation of Large Arteries. Expert consensus document on arterial stiffness: Methodological issues and clinical applications. Eur. Heart J. 2006, 27, 2588–2605. [Google Scholar] [CrossRef]
- Wang, K.L.; Cheng, H.M.; Chuang, S.Y.; Spurgeon, H.A.; Ting, C.T.; Lakatta, E.G.; Yin, F.C.; Chou, P.; Chen, C.H. Central or peripheral systolic or pulse pressure: Which best relates to target organs and future mortality? J. Hypertens. 2009, 27, 461–467. [Google Scholar] [CrossRef]
- Choi, J.S.; Oh, S.J.; Sung, Y.W.; Moon, H.J.; Lee, J.S. Pulse wave velocity is a new predictor of acute kidney injury development after off-pump coronary artery bypass grafting. PLoS ONE 2020, 15, e0232377. [Google Scholar] [CrossRef]
- Greenwood, S.A.; Mangahis, E.; Castle, E.M.; Wang, J.; Campbell, J.; Deshpande, R.; Jayawardene, S. Arterial stiffness is a predictor for acute kidney injury following coronary artery bypass graft surgery. J. Cardiothorac. Surg. 2019, 14, 51. [Google Scholar] [CrossRef]
- Sumin, A.N.; Shcheglova, A.V.; Osokina, A.V.; Fedorova, N.V.; Zhuchkova, E.A.; Barbarash, O.L. Cardiac-Ankle Vessel Index and short term results of coronary bypass grafting in coronary heart disease. Russ. J. Cardiol. 2015, 1, 78–84. [Google Scholar] [CrossRef]
- Sumin, A.N.; Shcheglova, A.V.; Bashtanova, T.B.; Barbarash, O.L. The influence of pathological Cardio-Ankle Vessel Index on annual results of coronary bypass in patients with ischemic heart disease. Cardiovasc. Ther. Prev. 2015, 14, 18–24. [Google Scholar] [CrossRef][Green Version]
- Olsson, D.; Sartipy, U.; Braunschweig, F.; Holzmann, M.J. Acute kidney injury following coronary artery bypass surgery and long-term risk of heart failure. Circ. Heart Fail. 2013, 6, 83–90. [Google Scholar] [CrossRef][Green Version]
- Sumin, A.N.; Shcheglova, A.V.; ZHidkova, I.I.; Ivanov, S.V.; Barbarash, O.L. Assessment of Arterial Stiffness by Cardio-Ankle Vascular Index for Prediction of Five-Year Cardiovascular Events After Coronary Artery Bypass Surgery. Glob. Heart 2021, 16, 90. [Google Scholar] [CrossRef]
- Shirai, K.; Utino, J.; Otsuka, K.; Takata, M. A novel blood pressure-independent arterial wall stiffness parameter: Cardio-ankle vascular index (CAVI). J. Atheroscler. Thromb. 2006, 13, 101–107. [Google Scholar] [CrossRef]
- Shirai, K.; Hiruta, N.; Song, M.; Kurosu, T.; Suzuki, J.; Tomaru, T.; Miyashita, Y.; Saiki, A.; Takahashi, M.; Suzuki, K.; et al. Cardio-ankle vascular index (CAVI) as a novel indicator of arterial stiffness: Theory, evidence and perspectives. J. Atheroscler. Thromb. 2011, 18, 924–938. [Google Scholar] [CrossRef]
- Matsushita, K.; Ding, N.; Kim, E.D.; Budoff, M.; Chirinos, J.A.; Fernhall, B.; Hamburg, N.; Kario, K.; Miyoshi, T.; Tanaka, H.; et al. Cardio-ankle vascular index and cardiovascular disease: Systematic review and meta-analysis of prospective and cross-sectional studies. J. Clin. Hypertens. 2019, 21, 16–24. [Google Scholar] [CrossRef]
- Piko, N.; Bevc, S.; Hojs, R.; Naji, F.H.; Ekart, R. The association between pulse wave analysis, carotid-femoral pulse wave velocity and peripheral arterial disease in patients with ischemic heart disease. BMC Cardiovasc. Disord. 2021, 21, 33. [Google Scholar] [CrossRef]
- Carr, B.M.; Romeiser, J.; Ruan, J.; Gupta, S.; Seifert, F.C.; Zhu, W.; Shroyer, A.L. Long-Term Post-CABG Survival: Performance of Clinical Risk Models Versus Actuarial Predictions. J. Card. Surg. 2016, 31, 23–30. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–271. [Google Scholar] [CrossRef]
- Smeltz, A.M.; Cooter, M.; Rao, S.; Karhausen, J.A.; Stafford-Smith, M.; Fontes, M.L.; Kertai, M.D. Elevated Pulse Pressure, Intraoperative Hemodynamic Perturbations, and Acute Kidney Injury After Coronary Artery Bypass Grafting Surgery. J. Cardiothorac. Vasc. Anesth. 2018, 32, 1214–1224. [Google Scholar] [CrossRef]
- Zhang, K.; Alfirevic, A.; Ramos, D.; Liang, C.; Soltesz, E.G.; Duncan, A.E. Neither Preoperative Pulse Pressure nor Systolic Blood Pressure Is Associated with Cardiac Complications After Coronary Artery Bypass Grafting. Anesth. Analg. 2020, 131, 1491–1499. [Google Scholar] [CrossRef]
- Prskalo, Z.; Brizić, I.; Markota, D.; Markota, I.; Boban, M.; Tomic, M.; Starcevic, B. Arterial stiffness in patients with coronary artery disease: Relation with in-stent restenosis following percutaneous coronary intervention. BMC Cardiovasc. Disord. 2016, 16, 128. [Google Scholar] [CrossRef] [PubMed]
- Aboyans, V.; Lacroix, P.; Postil, A.; Guilloux, J.; Rollé, F.; Cornu, E.; Laskar, M. Subclinical peripheral arterial disease and incompressible ankle arteries are both long-term prognostic factors in patients undergoing coronary artery bypass grafting. J. Am. Coll. Cardiol. 2005, 46, 815–820. [Google Scholar] [CrossRef] [PubMed]
- Saiki, A.; Ohira, M.; Yamaguchi, T.; Nagayama, D.; Shimizu, N.; Shirai, K.; Tatsuno, I. New Horizons of Arterial Stiffness Developed Using Cardio-Ankle Vascular Index (CAVI). J. Atheroscler. Thromb. 2020, 27, 732–748. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Camacho, F.T.; Wechsler, A.S.; Lahey, S.; Culliford, A.T.; Jordan, D.; Gold, J.P.; Higgins, R.S.; Smith, C.R.; Hannan, E.L. Risk score for predicting long-term mortality after coronary artery bypass graft surgery. Circulation 2012, 125, 2423–2430. [Google Scholar] [CrossRef]
- Urbanowicz, T.K.; Michalak, M.; Gąsecka, A.; Olasińska-Wiśniewska, A.; Perek, B.; Rodzki, M.; Bociański, M.; Jemielity, M. A Risk Score for Predicting Long-Term Mortality Following Off-Pump Coronary Artery Bypass Grafting. J. Clin. Med. 2021, 10, 3032. [Google Scholar] [CrossRef]
- Otsuka, K.; Fukuda, S.; Shimada, K.; Suzuki, K.; Nakanishi, K.; Yoshiyama, M.; Yoshikawa, J. Serial assessment of arterial stiffness by cardio-ankle vascular index for prediction of future cardiovascular events in patients with coronary artery disease. Hypertens. Res. 2014, 37, 1014–1020. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Group 1 CAVI < 9.0 n = 163 | Group 2 CAVI ≥ 9.0 n = 111 | p | ||
|---|---|---|---|---|---|
| No. of Events | % | No. of Events | % | ||
| Age, Me [LQ; UQ] years | 57.0 [52.0; 61.0] | 63.0 [55.0; 69.0] | <0.001 | ||
| BMI, Me [LQ; UQ] kg/m2 | 28.02 [24.5; 32.1] | 28.37 [26.6; 30.5] | 0.57 | ||
| EuroScore, Me [LQ; UQ] | 2.0 [1.0; 3.0] | 3.0 [2.0; 4.0] | 0.005 | ||
| Male gender | 129 | 79.14 | 80 | 72.07 | 0.17 |
| Myocardial infarction history | 106 | 65.03 | 64 | 57.66 | 0.21 |
| Hypertension | 133 | 81.6 | 104 | 93.69 | 0.004 |
| Stroke history | 8 | 4.91 | 9 | 8.11 | 0.28 |
| Transitory ischemic attack | 1 | 0.61 | 2 | 1.8 | 0.35 |
| Diabetes mellitus | 19 | 11.66 | 23 | 20.72 | 0.04 |
| PCI history | 13 | 7.98 | 9 | 8.11 | 0.96 |
| CABG history | 1 | 0.61 | 1 | 0.9 | 0.78 |
| Carotid endarterectomy | 2 | 1.23 | 3 | 2.7 | 0.37 |
| Current smoking | 53 | 32.52 | 28 | 25.23 | 0.19 |
| No angina | 29 | 17.9 | 27 | 24.32 | 0.19 |
| Angina I functional class | 8 | 4.94 | 3 | 2.7 | 0.35 |
| Angina II functional class | 55 | 33.95 | 29 | 26.13 | 0.16 |
| Angina III functional class | 68 | 41.98 | 48 | 43.24 | 0.83 |
| Angina IV functional class | 2 | 1.23 | 4 | 3.6 | 0.18 |
| Heart failure, class NYHA I | 109 | 66.87 | 60 | 54.1 | 0.032 |
| Heart failure, class NYHA II | 42 | 25.77 | 41 | 39.94 | 0.048 |
| Heart failure, class NYHA III | 4 | 2.45 | 4 | 43.6 | 0.57 |
| Preoperative Drug Therapy | |||||
| β-blockers | 107 | 65.6 | 75 | 67.6 | 0.840 |
| Calcium channel blockers | 57 | 35.0 | 33 | 30.0 | 0.438 |
| Statins | 81 | 49.6 | 60 | 54.1 | 0.557 |
| Angiotensin-converting enzyme inhibitors | 78 | 47.8 | 53 | 47.7 | 0.707 |
| aspirin | 108 | 66.2 | 79 | 71.2 | 0.285 |
| Oral antihyperglycemic therapy | 9 | 5.5 | 10 | 9.0 | 0.264 |
| Insulin therapy | 5 | 3.1 | 5 | 4.5 | 0.534 |
| Variables | Group 1 CAVI < 9.0 n = 163 | Group 2 CAVI ≥ 9.0 n = 111 | p |
|---|---|---|---|
| Laboratory data | |||
| Total cholesterol (mmol/L) | 4.9 [4.1; 5.9] | 5.05 [4.2; 6.1] | 0.27 |
| HDL cholesterol (mmol/L) | 0.96 [0.82; 1.165] | 1.01 [0.84; 1.2] | 0.33 |
| LDL cholesterol (mmol/L) | 2.91 [2.28; 3.79] | 2.96 [2.2; 3.74] | 0.37 |
| Triglycerides (mmol/L) | 1.76 [1.37; 2.43] | 1.66 [1.22; 2.3] | 0.45 |
| Creatinine (µmol/L) | 83.0 [70.0; 100.0] | 82.5 [72.0; 102.0] | 0.93 |
| Glucose (mmol/L) | 5.55 [5.1; 6.4] | 5.45 [5.0; 6.3] | 0.67 |
| Preoperative echocardiogram | |||
| LV EDD, cm | 5.5 [5.2; 6.0] | 5.5 [5.2; 6.1] | 0.98 |
| LV ESD, cm | 3.8 [3.4; 4.6] | 3.7 [3.5; 4.6] | 0.68 |
| LV EDV, mL | 153.0 [135.0; 180.0] | 147.0 [135.0; 188.0] | 0.95 |
| LV ESV, mL | 62.0 [47.0; 87.0] | 60.0 [49.0; 84.0] | 0.75 |
| LA, cm | 4.1 [3.8; 4.4] | 4.3 [3.9; 4.6] | 0.007 |
| RV, cm | 1.8 [1.8; 1.9] | 1.8 [1.8; 1.8] | 0.24 |
| RA, cm | 4.0 [3.8; 4.5] | 4.25 [3.9; 4.5] | 0.17 |
| LV EF, (%) | 60.0 [51.0; 64.0] | 60.0 [52.0; 63.0] | 0.32 |
| CIMT, mm | 1.1 [1.0; 1.2] | 1.1 [1.0; 1.2] | 0.32 |
| Atherosclerosis lesions of arterial basins | |||
| Carotid artery stenoses ≥ 30%, n(%) | 27 (16.56) | 20 (18.02) | 0.75 |
| Carotid artery stenoses ≥ 50%, n(%) | 18 (11.04) | 21 (18.92) | 0.06 |
| Carotid artery stenoses both sides ≥ 30%, n(%) | 19 (11.66) | 19 (17.21) | 0.19 |
| Multifocal atherosclerosis ≥ 30%, n(%) | 55 (33.74) | 55 (49.55) | 0.0008 |
| Multifocal atherosclerosis ≥ 50%, n(%) | 21 (12.88) | 30 (27.03) | 0.003 |
| Variables | Group 1 CAVI < 9.0 n = 163 | Group 2 CAVI ≥ 9.0 n = 111 | p | ||
|---|---|---|---|---|---|
| No. of Events | % | No. of Events | % | ||
| 1-coronary artery disease | 28 | 17.18 | 20 | 18.02 | 0.85 |
| 2-coronary artery disease | 56 | 34.36 | 34 | 30.63 | 0.51 |
| 3-coronary artery disease | 71 | 43.56 | 50 | 45.05 | 0.81 |
| LMCA ≥ 50% | 36 | 22.09 | 19 | 18.02 | 0.41 |
| Cardiopulmonary bypass | 140 | 85.89 | 93 | 83.78 | 0.63 |
| Ventriculoplasty | 9 | 5.52 | 5 | 4.5 | 0.7 |
| Thrombectomy | 6 | 3.68 | 2 | 1.8 | 0.36 |
| Carotid endarterectomy. | 3 | 1.84 | 2 | 1.8 | 0.98 |
| Radiofrequency ablation | 2 | 1.23 | 3 | 2.7 | 0.37 |
| Bypass graft number Me [LQ; UQ] | 3.0 [2.0; 3.0] | 3.0 [2.0; 3.0] | 0.71 | ||
| Cardiopulmonary bypass duration, Me [LQ; UQ] min | 98.0 [79.0; 110.0] | 94.0 [79.5; 107.5] | 0.59 | ||
| Operation duration Me [LQ; UQ] min | 240.0 [198.0; 300.0] | 240.0 [204.0; 270.0] | 0.82 | ||
| Death | ||||||
|---|---|---|---|---|---|---|
| B | S.E. | Wald | df | Sig. | Exp (B) | |
| Male gender | 1.032 | 0.448 | 5.313 | 1 | 0.021 | 2.807 |
| Diabetes mellitus | 0.838 | 0.426 | 3.874 | 1 | 0.049 | 2.312 |
| PAD | −1.737 | 0.813 | 4.567 | 1 | 0.033 | 0.176 |
| Multifocal atherosclerosis ≥ 30% | 1.030 | 0.360 | 8.169 | 1 | 0.004 | 2.800 |
| CAVI ≥ 9.0 | 0.646 | 0.348 | 3.445 | 1 | 0.063 | 1.907 |
| Constant | −2.716 | 0.498 | 29.724 | 1 | 0.000 | 0.066 |
| Combined endpoint | ||||||
| Multifocal atherosclerosis ≥ 30% | 0.705 | 0.292 | 5.843 | 1 | 0.016 | 2.025 |
| CAVI ≥ 9.0 | 0.589 | 0.286 | 4.250 | 1 | 0.039 | 1.802 |
| Constant | −0.480 | 0.204 | 5.543 | 1 | 0.019 | 0.619 |
| Combined endpoint + recurrent angina | ||||||
| Diabetes mellitus | 1.296 | 0.509 | 6.481 | 1 | 0.011 | 3.656 |
| Multifocal atherosclerosis ≥ 30% | 0.681 | 0.321 | 4.498 | 1 | 0.034 | 1.975 |
| Constant | 0.302 | 0.185 | 2.663 | 1 | 0.103 | 1.353 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sumin, A.N.; Shcheglova, A.V.; Ivanov, S.V.; Barbarash, O.L. Long-Term Prognosis after Coronary Artery Bypass Grafting: The Impact of Arterial Stiffness and Multifocal Atherosclerosis. J. Clin. Med. 2022, 11, 4585. https://doi.org/10.3390/jcm11154585
Sumin AN, Shcheglova AV, Ivanov SV, Barbarash OL. Long-Term Prognosis after Coronary Artery Bypass Grafting: The Impact of Arterial Stiffness and Multifocal Atherosclerosis. Journal of Clinical Medicine. 2022; 11(15):4585. https://doi.org/10.3390/jcm11154585
Chicago/Turabian StyleSumin, Alexey N., Anna V. Shcheglova, Sergey V. Ivanov, and Olga L. Barbarash. 2022. "Long-Term Prognosis after Coronary Artery Bypass Grafting: The Impact of Arterial Stiffness and Multifocal Atherosclerosis" Journal of Clinical Medicine 11, no. 15: 4585. https://doi.org/10.3390/jcm11154585
APA StyleSumin, A. N., Shcheglova, A. V., Ivanov, S. V., & Barbarash, O. L. (2022). Long-Term Prognosis after Coronary Artery Bypass Grafting: The Impact of Arterial Stiffness and Multifocal Atherosclerosis. Journal of Clinical Medicine, 11(15), 4585. https://doi.org/10.3390/jcm11154585