
Indicators of the Right Ventricle Systolic and Diastolic Function 18 Months after Coronary Bypass Surgery


Abstract
1. Introduction
2. Subjects, Materials, and Methods
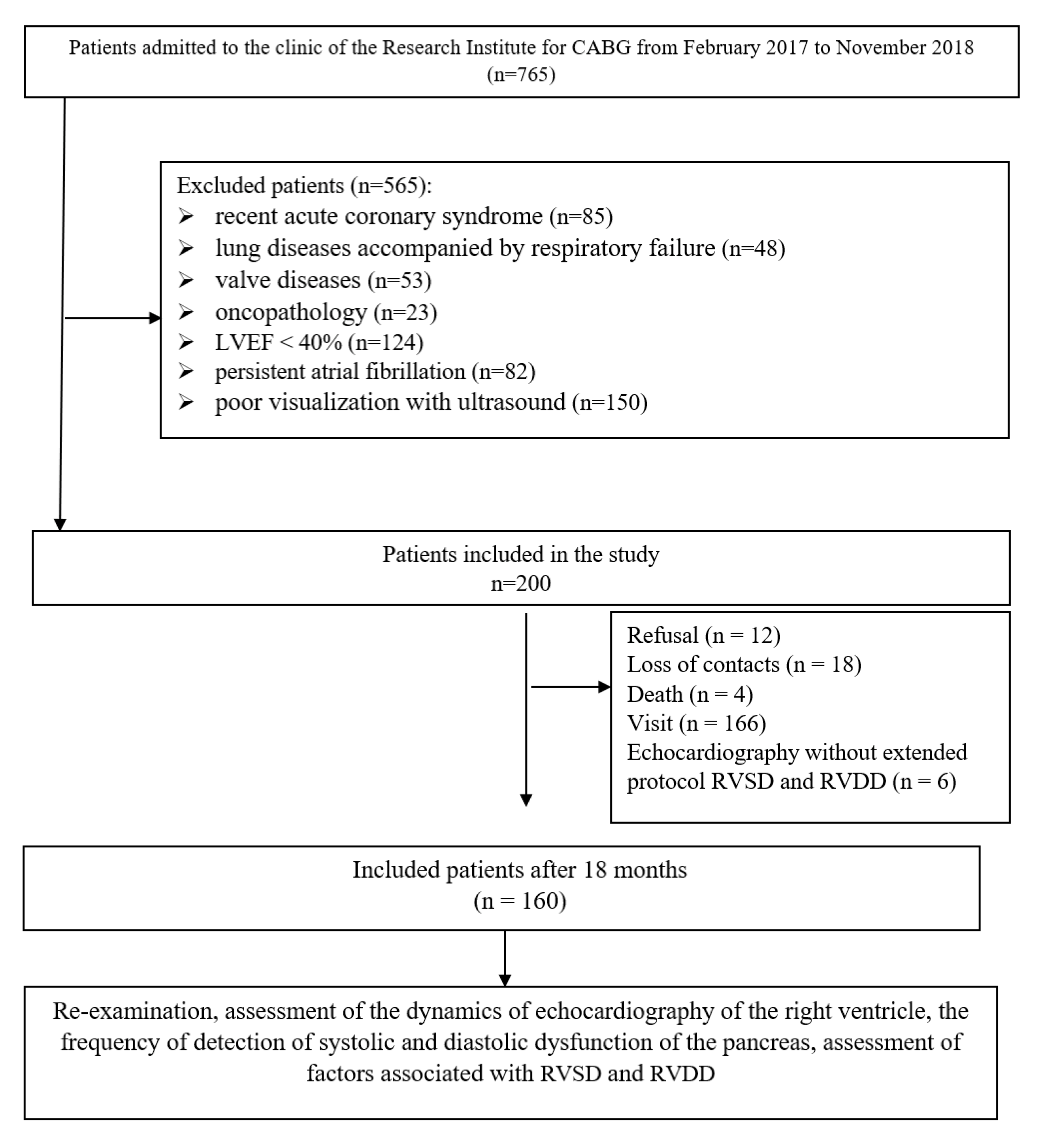
2.1. Study Population
2.2. Data Collection and Study Outcomes
2.3. Echocardiographic Examination
2.4. Ethics Statement
2.5. Statistical Analyses
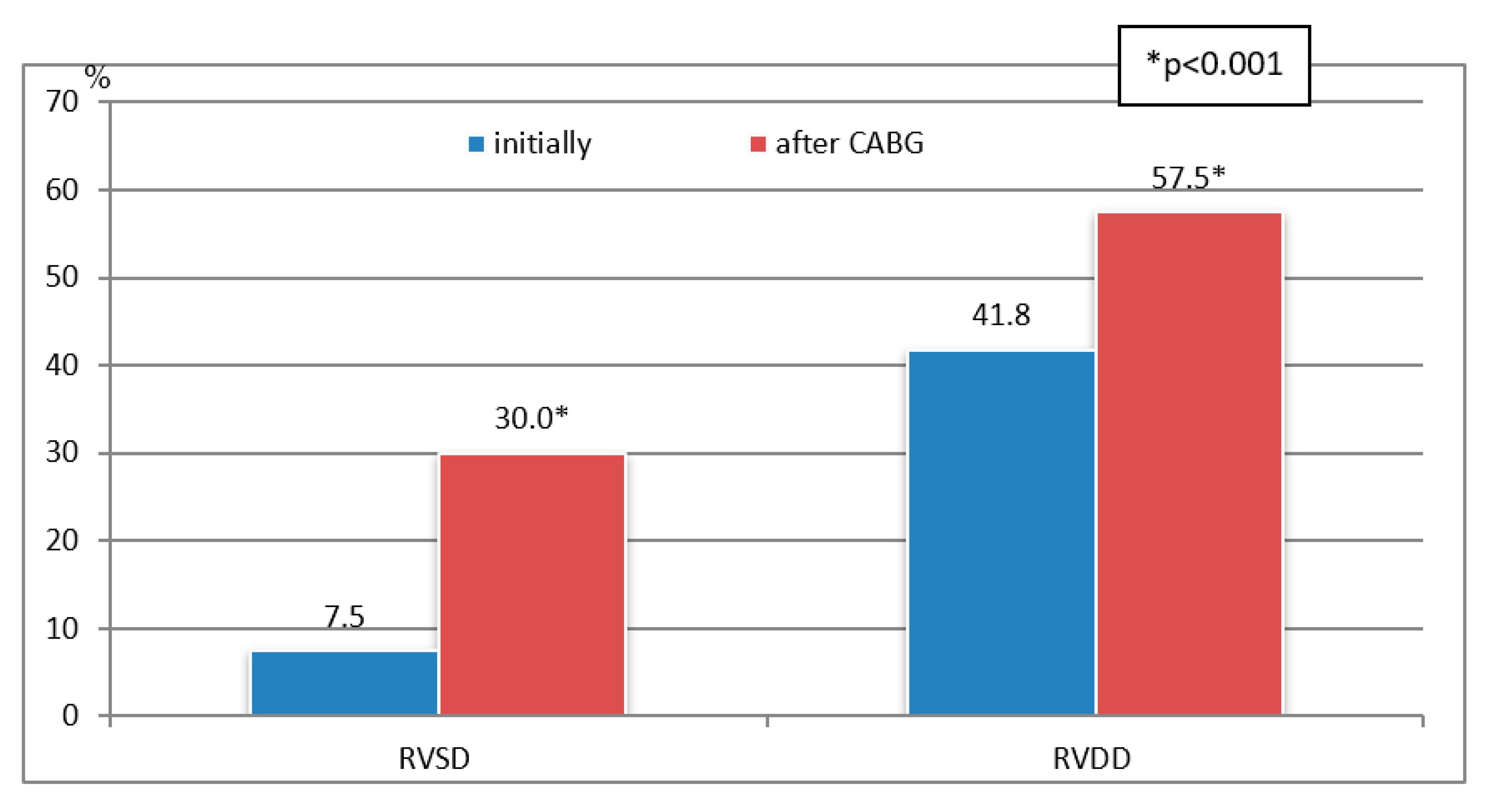
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef] [PubMed]
- Guinot, P.G.; Abou-Arab, O.; Longrois, D.; Dupont, H. Right ventricular systolic dysfunction and vena cava dilatation precede alteration of renal function in adult patients undergoing cardiac surgery: An observational study. Eur. J. Anaesthesiol. 2015, 32, 535–542. [Google Scholar] [CrossRef] [PubMed]
- Pouleur, A.C.; Rousseau, M.F.; Ahn, S.A.; Amzulescu, M.; Demeure, F.; de Meester, C.; Vancraeynest, D.; Pasquet, A.; Vanoverschelde, J.P.; Gerber, B.L. Right ventricular systolic dysfunction assessed by cardiac magnetic resonance is a strong predictor of cardiovascular death after coronary bypass grafting. Ann. Thorac. Surg. 2016, 101, 2176–2184. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Chowdhury, M.A.; Cook, J.M.; Moukarbel, G.V.; Ashtiani, S.; Schwann, T.A.; Bonnell, M.R.; Cooper, C.J.; Khouri, S.J. Pre-operative right ventricular echocardiographic parameters associated with short-term outcomes and long-term mortality after CABG. Echo Res. Pract. 2018, 5, 155–166. [Google Scholar] [CrossRef] [PubMed]
- Levy, D.; Laghlam, D.; Estagnasie, P.; Brusset, A.; Squara, P.; Nguyen, L.S. Post-operative Right Ventricular Failure After Cardiac Surgery: A Cohort Study. Front. Cardiovasc. Med. 2021, 8, 667328. [Google Scholar] [CrossRef]
- Itagaki, S.; Hosseinian, L.; Varghese, R. Right ventricular failure after cardiac surgery: Management strategies. Semin. Thorac. Cardiovasc. Surg. 2012, 24, 188–194. [Google Scholar] [CrossRef]
- Zochios, V.; Protopapas, A.D.; Parhar, K. Markers of Right Ventricular Dysfunction in Adult Cardiac Surgical Patients. J. Cardiothorac. Vasc. Anesth. 2017, 31, 1570–1574. [Google Scholar] [CrossRef]
- Grønlykke, L.; Ravn, H.B.; Gustafsson, F.; Hassager, C.; Kjaergaard, J.; Nilsson, J.C. Right ventricular dysfunction after cardiac surgery—Diagnostic options. Scand. Cardiovasc. J. 2017, 51, 114–121. [Google Scholar] [CrossRef]
- Denault, A.; Haddad, F.; Lamarche, Y.; Bouabdallaoui, N.; Deschamps, A.; Desjardins, G. Postoperative right ventricular dysfunction-Integrating right heart profiles beyond long-axis function. J. Thorac. Cardiovasc. Surg. 2020, 159, e315–e317. [Google Scholar] [CrossRef] [PubMed]
- Kukulski, T.; She, L.; Racine, N.; Gradinac, S.; Panza, J.A.; Velazquez, E.J.; Chan, K.; Petrie, M.C.; Lee, K.L.; Pellikka, P.A.; et al. Surgical Treatment for Ischemic Heart Failure Investigators. Implication of right ventricular dysfunction on long-term outcome in patients with ischemic cardiomyopathy undergoing coronary artery bypass grafting with or without surgical ventricular reconstruction. J. Thorac. Cardiovasc. Surg. 2015, 149, 1312–1321. [Google Scholar] [CrossRef]
- Bootsma, I.T.; Scheeren, T.W.L.; de Lange, F.; Haenen, J.; Boonstra, P.W.; Boerma, E.C. Impaired right ventricular ejection fraction after cardiac surgery is associated with a complicated ICU stay. J. Intensive Care 2018, 6, 85. [Google Scholar] [CrossRef] [PubMed]
- Krishna, S.N.; Hasija, S.; Chauhan, S.; Kaushal, B.; Chowdhury, U.K.; Bisoi, A.K.; Khan, M.A. Can Echocardiographic Right Ventricular Function Parameters Predict Vasoactive Support Requirement After Tetralogy of Fallot Repair? J. Cardiothorac. Vasc. Anesth. 2019, 33, 2404–2413. [Google Scholar] [CrossRef] [PubMed]
- Magne, J.; Serena, C.; Salerno, B.; Mohty, D.; Marsaud, J.P.; Blossier, J.D.; Piccardo, A.; Cornu, E.; Le Guyader, A.; Aboyans, V. Which echocardiographic parameters improve the risk prediction for peri-operative outcomes in patients undergoing coronary bypass surgery: A prospective study. Eur. Heart J. Acute Cardiovasc. Care. 2020, 9, 504–512. [Google Scholar] [CrossRef] [PubMed]
- Murch, S.D.; La Gerche, A.; Roberts, T.J.; Prior, D.L.; MacIsaac, A.I.; Burns, A.T. Abnormal right ventricular relaxation in pulmonary hypertension. Pulm Circ. 2015, 5, 370–375. [Google Scholar] [CrossRef] [PubMed]
- Sumin, A.N.; Korok, E.V.; Sergeeva, T.Y. Impaired right ventricular filling in patients with a chronic coronary syndrome. Med Ultrason. 2021, 23, 311–318. [Google Scholar] [CrossRef]
- Sumin, A.N.; Korok, E.V.; Sergeeva, T.J. Preexisting Right Ventricular Diastolic Dysfunction and Postoperative Cardiac Complications in Patients Undergoing Nonemergency Coronary Artery Bypass Surgery. J. Cardiothorac. Vasc. Anesth. 2021, 35, 799–806. [Google Scholar] [CrossRef]
- Zanobini, M.; Loardi, C.; Poggio, P.; Tamborini, G.; Veglia, F.; Di Minno, A.; Myasoedova, V.; Mammana, L.F.; Biondi, R.; Pepi, M.; et al. The impact of pericardial approach and myocardial protection onto postoperative right ventricle function reduction. J. Cardiothorac. Surg. 2018, 13, 55. [Google Scholar] [CrossRef]
- Chinikar, M.; Rafiee, M.; Aghajankhah, M.; Gholipour, M.; Hasandokht, T.; Imantalab, V.; Mirmansouri, A.; Mohammadzadeh, A.; Nassiri-Sheikhani, N.; Naghshbandi, M.; et al. Right ventricular dysfunction and associated factors in patients after coronary artery bypass grafting. ARYA Atheroscler. 2019, 15, 99–105. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–270. [Google Scholar] [CrossRef]
- Mukhaini, M.; Prashanth, P.; Abdulrehman, S.; Zadjali, M. Assessment of right ventricular diastolic function by tissue Doppler imaging in patients with acute right ventricular myocardial infarction. Echocardiography 2010, 27, 539–543. [Google Scholar] [CrossRef]
- Roshanali, F.; Yousefnia, M.A.; Mandegar, M.H.; Rayatzadeh, H.; Alinejad, S. Decreased right ventricular function after coronary artery bypass grafting. Tex. Heart Inst. J. 2008, 35, 250–255. [Google Scholar] [PubMed]
- Labus, J.; Winata, J.; Schmidt, T.; Nicolai, J.; Tomko, M.; Sveric, K.; Wilbring, M.; Fassl, J. Perioperative Course of Three-Dimensional-Derived Right Ventricular Strain in Coronary Artery Bypass Surgery: A Prospective, Observational, Pilot Trial. J. Cardiothorac. Vasc. Anesth. 2021, 35, 1628–1637. [Google Scholar] [CrossRef] [PubMed]
- Borde, D.; Joshi, P.; Joshi, S.; Asegaonkar, B.; Apsingekar, P.; Khade, S.; Pande, S.; Agrawal, A.; Puranik, M. Changes in Right Ventricular Function After Off-Pump Coronary Artery Bypass Grafting. J. Cardiothorac. Vasc. Anesth. 2021, 35, 811–819. [Google Scholar] [CrossRef]
- Steffen, H.J.; Kalverkamp, S.; Zayat, R.; Autschbach, R.; Spillner, J.W.; Hagendorff, A.; Hatam, N. Is Systolic Right Ventricular Function Reduced after Thoracic Non-Cardiac Surgery? A Propensity Matched Echocardiographic Analysis. Ann. Thorac. Cardiovasc. Surg. 2018, 24, 238–246. [Google Scholar] [CrossRef]
- Bening, C.; Sales, V.L.; Alhussini, K.; Radakovic, D.; Benitez, R.C.; Madrahimov, N.; Keller, D.; Leyh, R. Clinically inapparent right heart dysfunction is associated with reduced myofilament force development in coronary artery disease. BMC Cardiovasc. Disord. 2021, 21, 125. [Google Scholar] [CrossRef] [PubMed]
- Sumin, A.N.; Korok, E.V.; Sergeeva, T.Y. Moderate right ventricular systolic dysfunction in patients with chronic coronary syndrome—What determines it? Complex Issues Cardiovasc. Dis. 2019, 8 (Suppl. S4), 51–61. [Google Scholar] [CrossRef]
- Lella, L.K.; Sales, V.L.; Goldsmith, Y.; Chan, J.; Iskandir, M.; Gulkarov, I.; Tortolani, A.; Brener, S.J.; Sacchi, T.J.; Heitner, J.F. Reduced Right Ventricular Function Predicts Long-Term Cardiac Re-Hospitalization after Cardiac Surgery. PLoS ONE 2015, 10, e0132808. [Google Scholar] [CrossRef]
- Jin, Y.; Wang, H.; Wang, Z.; Jiang, H.; Tao, D.; Wu, H. The evaluation of preoperative right ventricular diastolic dysfunction on coronary artery disease patients with left ventricular dysfunction. Echocardiography 2014, 31, 1259–1264. [Google Scholar] [CrossRef]
- Mandoli, G.E.; Cameli, M.; Novo, G.; Righini, F.M.; Santoro, C.; D’Ascenzi, F.; Ancona, F.; Sorrentino, R.; D’Andrea, A.; Galderisi, M.; et al. Right ventricular function after cardiac surgery: The diagnostic and prognostic role of echocardiography. Heart Fail. Rev. 2019, 24, 625–635. [Google Scholar] [CrossRef]
- Schneider, M.; Aschauer, S.; Mascherbauer, J.; Ran, H.; Binder, C.; Lang, I.; Goliasch, G.; Binder, T. Echocardiographic assessment of right ventricular function: Current clinical practice. Int. J. Cardiovasc. Imaging 2019, 35, 49–56. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | p |
|---|---|
| Clinical and anamnestic data | |
| Male, n (%) | 120 (75.0) |
| Age, ME [LQ; UQ], (y) | 64.0 [60.0; 68.0] |
| Body mass index, ME [LQ; UQ], (kg/m2) | 28.7 [26.0; 30.7] |
| Smoking, n (%) | 48 (30.2) |
| Smoking experience, ME [LQ; UQ], (y) | 40.0 [20.0; 40.0] |
| Hypertension, n (%) | 151 (94.3) |
| Angina pectoris, n (%) | 138 (86.3) |
| Myocardial infarction history, n (%) | 99 (62.3) |
| CHF NYHA IIA cт., n (%) | 31(19.4) |
| Rhythm disturbances, n (%) | 26 (16.3) |
| Diabetes mellitus, n (%) | 43 (26.8) |
| Stroke history, n (%) | 13 (8.2) |
| PCI history, n (%) | 28 (17.6) |
| Chronic lung disease, n (%) | 25 (15.6) |
| Carotid atherosclerosis >50%, n (%) | 31 (19.4) |
| Atherosclerosis of the legs >50%, n (%) | 7 (4.4) |
| Hyperlipidemia, n (%) | 105 (65.6) |
| Right coronary artery stenosis >70%, n (%) | 141(88.1) |
| Biochemical markers | |
| NT-proBNP, ME [LQ; UQ], pg/mL | 66.7 [32.4; 150.0] |
| Creatinine, ME [LQ; UQ], mmol/L | 84.5 [74.5; 97.0] |
| Glucose, ME [LQ; UQ], mmol/L | 5.7 [5.2; 6.5] |
| Total cholesterol, ME [LQ; UQ], mmol/L | 4.6 [3.7; 5.3] |
| Low-density lipoprotein, ME [LQ; UQ], mmol/L | 2.73 [2.08; 3.54] |
| High-density lipoproteins, ME [LQ; UQ], mmol/L | 1.13 [0.92; 1.33] |
| Triglycerides, ME [LQ; UQ], mmol/L | 1.43 [1.16; 2.17] |
| Therapy before surgery | |
| Betablocker, n (%) | 152 (95.0) |
| Statins, n (%) | 152 (95.0) |
| ACE-I, n (%) | 121 (75.6) |
| Aspirin, n (%) | 148 (92.5) |
| Surgical procedure | |
| Cardiopulmonary bypass, n (%) | 184 (92.0) |
| Bypass graft number | 3 (2–3) |
| Cardiopulmonary bypass duration, ME [LQ; UQ] (min) | 77.0 [65.0; 95.0] |
| Aortic cross-clamp time, ME [LQ; UQ] (min) | 51.0 [40.0; 61.0] |
| Ventriculoplasty, n (%) | 17 (8.5) |
| Thrombectomy, n (%) | 9 (4.5) |
| Radiofrequency ablation, n (%) | 6 (3.0) |
| Carotid endarterectomy, n (%) | 23 (11.5) |
| Perioperative complications | |
| Congestive heart failure, n (%) | 13 (8.1) |
| Myocardial infarction, nonfatal, n (%) | 2 (1.3) |
| Stroke, nonfatal, n (%) | 5 (3.1) |
| Cardiovascular death, n (%) | - |
| Acute renal failure, n (%) | 5 (3.1) |
| Therapy after surgery | |
| Betablocker, n (%) | 139 (86.9) |
| Statins, n (%) | 137 (85.6) |
| ACE-I, n (%) | 96 (60.0) |
| Aspirin, n (%) | 130 (81.3) |
| Characteristics | Group 1 Control (n = 36) | Group 2 before Surgery(n = 160) | Group 3 18 Months after CABG (n = 160) | H | p |
|---|---|---|---|---|---|
| Structural indicators and systolic function | |||||
| LA, ME [LQ; UQ] mm | 4.15 [3.7; 4.55] | 4.4 [4.1; 4.8] * | 4.6 [4.2; 4.95] **# | 15.98 | 0.0003 |
| EDD, ME [LQ; UQ] mm | 5.2 [4.95; 5.5] | 5.5 [5.3; 6.1] * | 5.5 [5.1; 6.0] # | 18.3 | 0.0001 |
| ESD LV, ME [LQ; UQ] mm | 3.3 [3.05; 3.5] | 3.6 [3.3; 4.0] * | 3.7 [3.4; 4.2] # | 23.04 | <0.001 |
| EDVI, ME [LQ;UQ] мл | 130.0 [115.5; 147.0] | 147.0 [135.0; 187.0] * | 147.0 [124.0; 180.0] # | 18.21 | 0.0001 |
| ESV, ME [LQ;UQ] mL | 44.0 [36.5; 51.0] | 52.0 [44.0; 70.0] * | 58.0 [46.0; 79.0] # | 22.19 | <0.001 |
| LVEF, ME [LQ;UQ] % | 62.0 [60.0; 64.0] | 61.0 [55.5; 65.5] | 56.0 [51.0; 61.0] **# | 34.6 | <0.001 |
| LVM, ME [LQ;UQ] (g) | 206.0 [172.0; 254.0] | 303.5 [258.8; 360.4] * | 242.0 [201.5; 286.5] **# | 49.65 | <0.001 |
| LVMI, ME [LQ; UQ] | 101.5 [89.0; 136.0] | 136.2 [87.0; 173.4] | 138.0 [112.0; 159.0] | 0.85 | 0.654 |
| Indicators of LV diastolic function | |||||
| IVRT, ME[LQ;UQ] m/s | 90.0 [90.0; 90.0] | 92.0 [90.0; 98.0] * | 90.0 [88.0; 92.0] # | 46.8 | <0.001 |
| E, ME [LQ; UQ] cм/ceк | 56.5 [48.0; 65.0] | 58.0 [46.0; 68.0] | 56.0 [47.0; 65.0] | 0.73 | 0.691 |
| A, ME [LQ; UQ] cm/s | 66.0 [56.0; 74.0] | 67.0 [58.5; 78.0] | 63.0 [54.0; 71.5] | 7.93 | 0.189 |
| E/A | 0.83 [0.69; 1.2] | 0.79 [0.68; 1.1] | 0.81 [0.7; 1.24] | 2.28 | 0.319 |
| e’, ME [LQ; UQ] cm/s | 9.4 [8.5; 11.0] | 9.3 [7.5; 11.0] | 10.6 [9.0; 12.3] **# | 16.39 | 0.0003 |
| a’, ME [LQ;UQ] cm/s | 11.95 [10.5; 13.3] | 10.0 [8.6; 11.6] * | 9.4 [7.7; 11.0] **# | 21.07 | <0.001 |
| e’/a’, ME [LQ;UQ] | 0.77 [0.66; 1.14] | 0.91 [0.68; 1.29] | 1.24 [0.83; 1.48] **# | 25.66 | <0.001 |
| s’, ME [LQ; UQ] cm/s | 10.0 [9.5; 10.7] | 9.2 [8.2; 10.35] * | 9.8 [8.6; 10.8] ** | 14.18 | 0.0008 |
| E/e’, ME [LQ;UQ] | 5.9 [5.13; 6.73] | 6.1 [4.75; 7.6] | 5.1 [4.17; 6.38] **# | 15.82 | 0.0004 |
| Tei LV [LQ;UQ] | 0.29 [0.26; 0.34] | 0.33 [0.25; 0.43] * | 0.26 [0.22; 0.31] **# | 37.47 | <0.001 |
| Characteristics | Group 1 Control(n = 36) | Group 2 before Surgery(n = 160) | Group 3 18 Months after CABG (n = 160) | H | p |
|---|---|---|---|---|---|
| Structural indicators and systolic function | |||||
| RV, [LQ; UQ] mm | 2.0 [1.8; 2.4] | 2.0 [1.9; 2.2] | 2.1 [2.0; 2.3] | 2.39 | 0.302 |
| RVth, [LQ; UQ] mm | 0.3 [0.3; 0.3] | 0.4 [0.3; 0.4] * | 0.4 [0.3; 0.4] # | 20.5 | <0.001 |
| TAPSE, [LQ; UQ] mm | 26.0 [24.0; 28.0] | 23.0 [21.0; 26.0] * | 20.0 [18.0; 21.0] **# | 107 | <0.001 |
| RVEF, ME [LQ; UQ] % | 55.0 [54.0; 59.5] | 55.0 [53.0; 57.0] | 54.5 [52.0; 55.0] **# | 15.0 | 0.0006 |
| RA, ME [LQ; UQ] mm | 44.0 [33.0; 55.0] | 40.0 [33.0; 49.0] | 53.0 [43.0; 63.0] **# | 53.9 | <0.001 |
| mPAP. [LQ; UQ] mmhg | 11.0 [11.0; 11.5] | 12.0 [24.0; 29.0] * | 11.0 [11.0; 13.0] # | 9.6 | 0.008 |
| sPAP. [LQ; UQ] mmhg | 22.5 [21.0; 24.0] | 27.0 [24.0; 29.0] * | 24.0 [23.0; 28.0] # | 9.81 | 0.007 |
| Diastolic function indicators | |||||
| Et, ME [LQ; UQ] cm/s | 50.0 [43.0; 55.5] | 44.0 [37.0; 49.5] * | 49.5 [44.0; 58.0] ** | 27.2 | <0.001 |
| At, ME [LQ; UQ] cm/s | 37.0 [33.0; 45.0] | 43.0 [35.0; 49.5] * | 34.5 [30.0; 41.5] ** | 35.7 | <0.001 |
| Et/At | 1.41 [1.12; 1.53] | 1.05 [0.76; 1.36] * | 1.46 [1.29; 1.62] ** | 61.1 | <0.001 |
| e’t, ME [LQ; UQ] cm/s | 10.7 [9.0; 12.5] | 9.6 [8.05; 11.3] * | 8.0 [7.0; 9.9] **# | 54.1 | <0.001 |
| a’t, ME [LQ; UQ] cm/s | 15.4 [12.85; 18.0] | 14.0 [12.1; 15.8] * | 9.4 [8.0; 11.0] **# | 151 | <0.001 |
| e’t/a’t, ME [LQ; UQ] | 0.7 [0.63; 0.78] | 0.69 [0.59; 0.8] | 0.78 [0.66; 1.19] **# | 33.7 | <0.001 |
| s’t, ME [LQ; UQ] cm/s | 14.0 [12.15; 15.9] | 13.2 [11.9; 14.7] | 11.8 [10.4; 12.95] **# | 48.4 | <0.001 |
| Et/e’t, ME [LQ; UQ] | 4.76 [3.58; 5.31] | 4.47 [3.6; 5.5] | 6.0 [4.77; 7.22] **# | 64.2 | <0.001 |
| Right ventricular Tei index [LQ; UQ] | 0.31 [0.26; 0.33] | 0.3 [0.24; 0.38] | 0.27 [0.21; 0.32] **# | 17.6 | 0.0001 |
| Variables in the Equation | |||||||
|---|---|---|---|---|---|---|---|
| B | SE | Wald | df | Significance | Exp(B) | ||
| Step 1 a | e’t | −0.212 | 0.089 | 5.686 | 1 | 0.017 | 0.809 |
| Constant | 1.318 | 0.875 | 2.266 | 1 | 0.132 | 3.736 | |
| Step 2 b | TAPSE | 0.117 | 0.052 | 5.055 | 1 | 0.025 | 1.124 |
| e’t | −0.302 | 0.102 | 8.717 | 1 | 0.003 | 0.740 | |
| Constant | −0.547 | 1.212 | 0.203 | 1 | 0.652 | 0.579 | |
| Step 3 c | TAPSE | 0.147 | 0.054 | 7.368 | 1 | 0.007 | 1.158 |
| e’t | −0.293 | 0.104 | 7.997 | 1 | 0.005 | 0.746 | |
| RVSD | 1.150 | 0.505 | 5.192 | 1 | 0.023 | 3.158 | |
| Constant | −1.529 | 1.297 | 1.390 | 1 | 0.238 | 0.217 | |
| Variables in the Equation | |||||||
|---|---|---|---|---|---|---|---|
| B | SE | Wald | df | Significance | Exp(B) | ||
| Step 1 a | At | 0.036 | 0.016 | 4.995 | 1 | 0.025 | 1.037 |
| Constant | −1.213 | 0.707 | 2.943 | 1 | 0.086 | 0.297 | |
| Step 2 b | Myocardial infarction history | 0.809 | 0.357 | 5.132 | 1 | 0.023 | 0.445 |
| At | 0.038 | 0.017 | 5.327 | 1 | 0.021 | 1.039 | |
| Constant | −0.798 | 0.744 | 1.151 | 1 | 0.283 | 0.450 | |
| Coefficients a | ||||||
|---|---|---|---|---|---|---|
| Model | Unstandardized Coefficients | Standardized Coefficients | t | Significance | ||
| B | SE | Beta | ||||
| 1 | (Constant) | 9.445 | 0.725 | 13.033 | 0.000 | |
| e’t | 0.231 | 0.070 | 0.257 | 3.301 | 0.001 | |
| 2 | (Constant) | 8.139 | 0.924 | 8.811 | 0.000 | |
| e’t | 0.178 | 0.073 | 0.198 | 2.435 | 0.016 | |
| s’t | 0.138 | 0.061 | 0.182 | 2.237 | 0.027 | |
| Model | Unstandardized Coefficients | Standardized Coefficients | t | Significance | ||
|---|---|---|---|---|---|---|
| B | SE | Beta | ||||
| 1 | (Constant) | 2.080 | 1.532 | 1.357 | 0.177 | |
| LA | 0.926 | 0.344 | 0.212 | 2.694 | 0.008 | |
| 2 | (Constant) | −1.671 | 2.077 | −0.804 | 0.422 | |
| LA | 0.902 | 0.338 | 0.207 | 2.672 | 0.008 | |
| age | 0.061 | 0.023 | 0.202 | 2.618 | 0.010 | |
| 3 | (Constant) | −2.953 | 2.157 | −1.369 | 0.173 | |
| LA | 0.936 | 0.335 | 0.214 | 2.796 | 0.006 | |
| age | 0.057 | 0.023 | 0.191 | 2.483 | 0.014 | |
| Et | 0.030 | 0.015 | 0.152 | 1.980 | 0.050 | |
| 4 | (Constant) | −3.331 | 2.143 | −1.554 | 0.122 | |
| LA | 0.986 | 0.332 | 0.226 | 2.967 | 0.004 | |
| age | 0.058 | 0.023 | 0.194 | 2.550 | 0.012 | |
| Et | 0.031 | 0.015 | 0.157 | 2.065 | 0.041 | |
| Stroke in the early postoperative period | 1.692 | 0.831 | 0.155 | 2.037 | 0.043 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sumin, A.N.; Shcheglova, A.V.; Korok, E.V.; Sergeeva, T.J. Indicators of the Right Ventricle Systolic and Diastolic Function 18 Months after Coronary Bypass Surgery. J. Clin. Med. 2022, 11, 3994. https://doi.org/10.3390/jcm11143994
Sumin AN, Shcheglova AV, Korok EV, Sergeeva TJ. Indicators of the Right Ventricle Systolic and Diastolic Function 18 Months after Coronary Bypass Surgery. Journal of Clinical Medicine. 2022; 11(14):3994. https://doi.org/10.3390/jcm11143994
Chicago/Turabian StyleSumin, Alexey N., Anna V. Shcheglova, Ekaterina V. Korok, and Tatjana Ju. Sergeeva. 2022. "Indicators of the Right Ventricle Systolic and Diastolic Function 18 Months after Coronary Bypass Surgery" Journal of Clinical Medicine 11, no. 14: 3994. https://doi.org/10.3390/jcm11143994
APA StyleSumin, A. N., Shcheglova, A. V., Korok, E. V., & Sergeeva, T. J. (2022). Indicators of the Right Ventricle Systolic and Diastolic Function 18 Months after Coronary Bypass Surgery. Journal of Clinical Medicine, 11(14), 3994. https://doi.org/10.3390/jcm11143994