
The Optimal Strategy of Dual Antiplatelet Therapy after Percutaneous Coronary Intervention with Drug-Eluting Stent


Abstract
:1. Introduction
2. Methods
2.1. Search Strategy and Eligibility Criteria
2.2. Outcomes
2.3. Statistical Analysis
3. Results
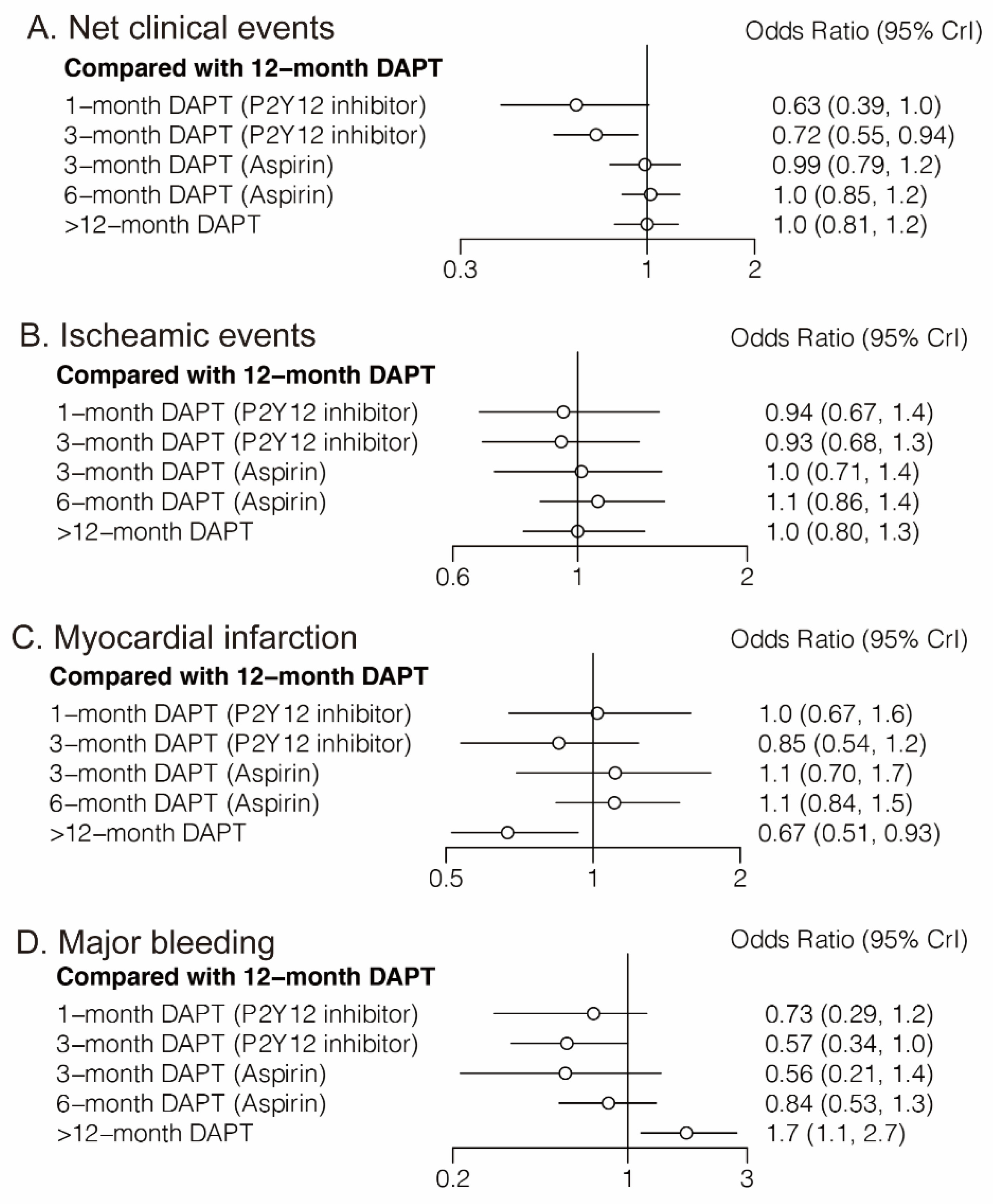
3.1. Primary Outcomes
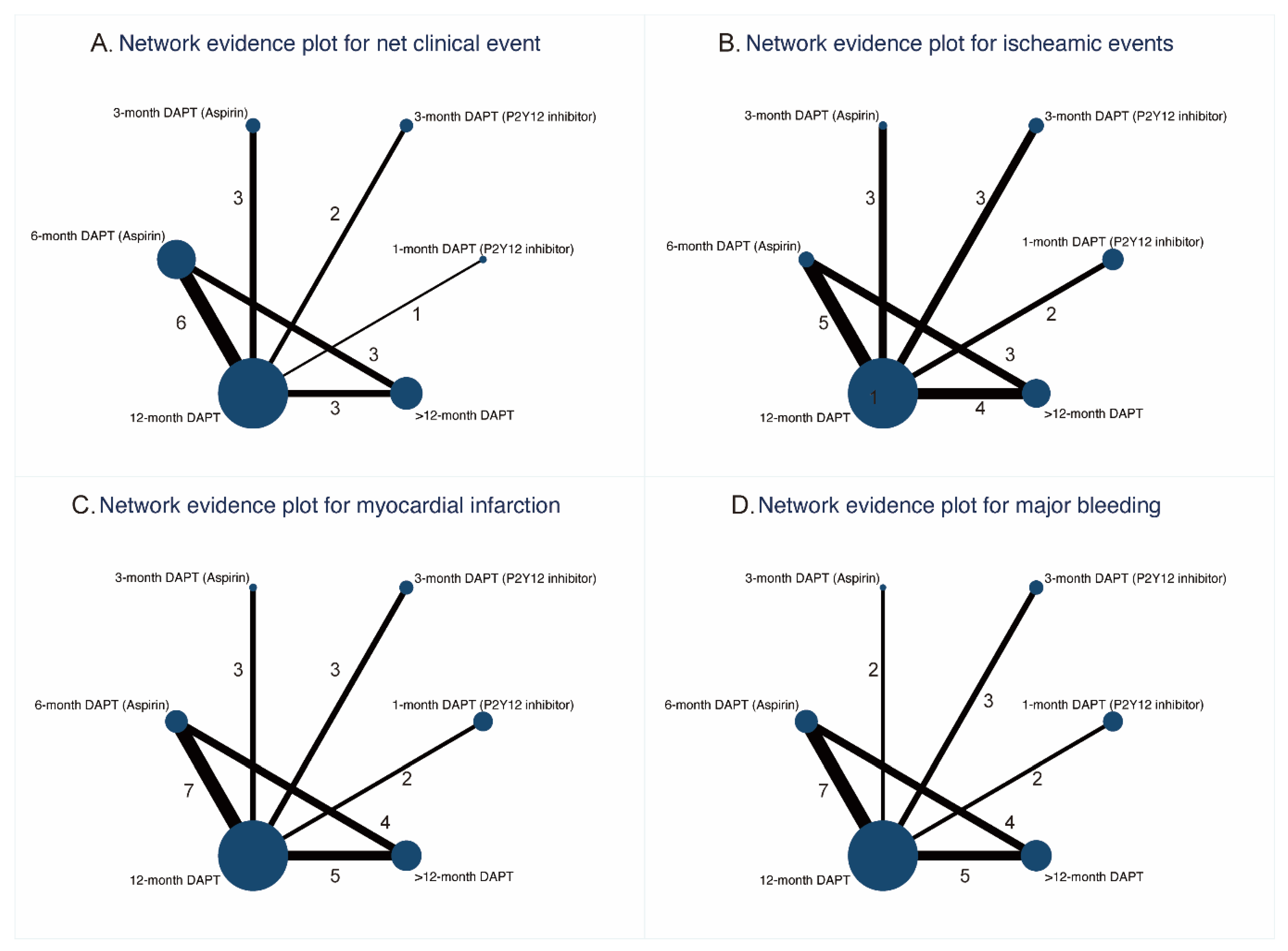
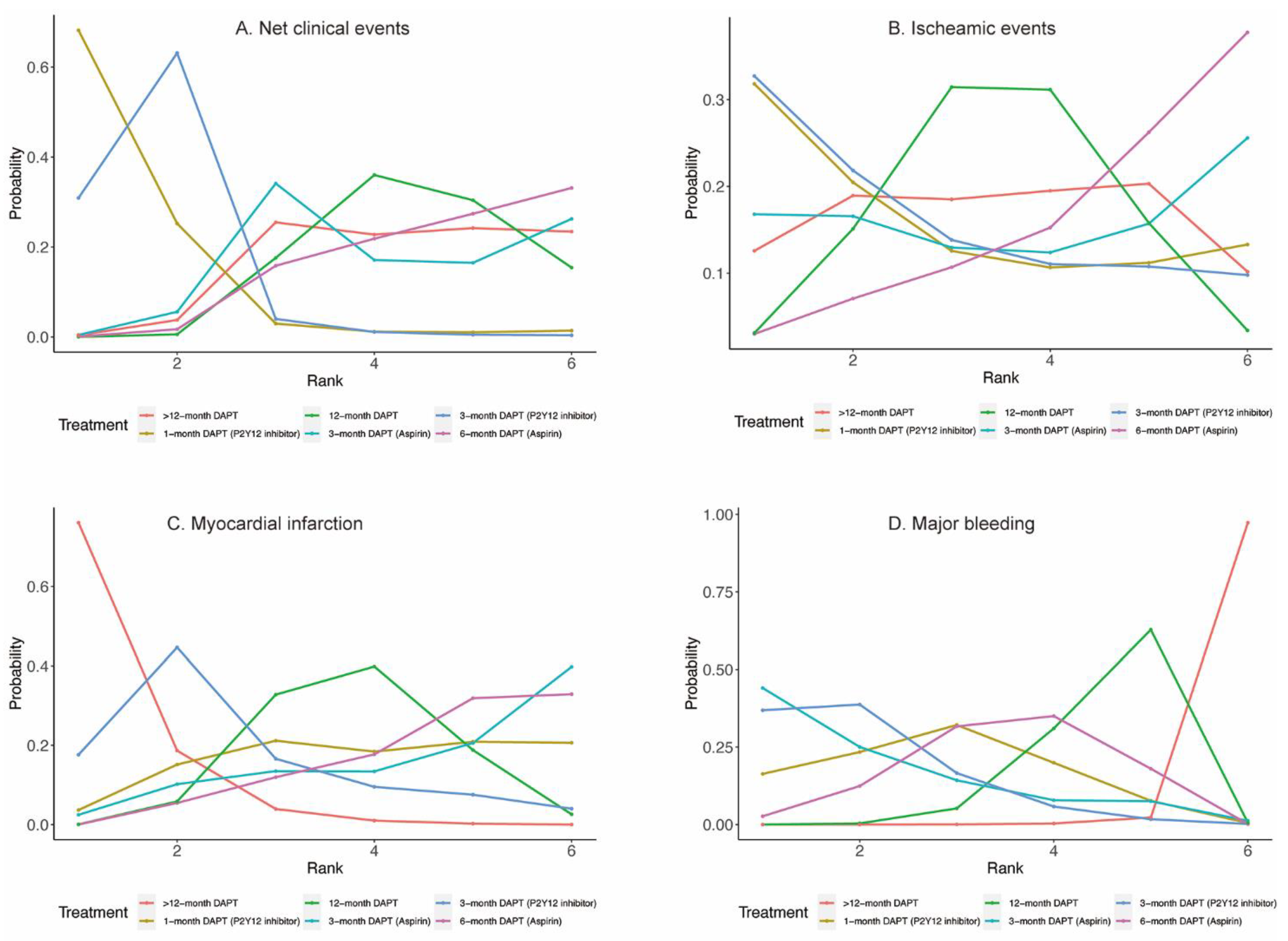
3.1.1. Net Clinical Events
3.1.2. Ischemic Events
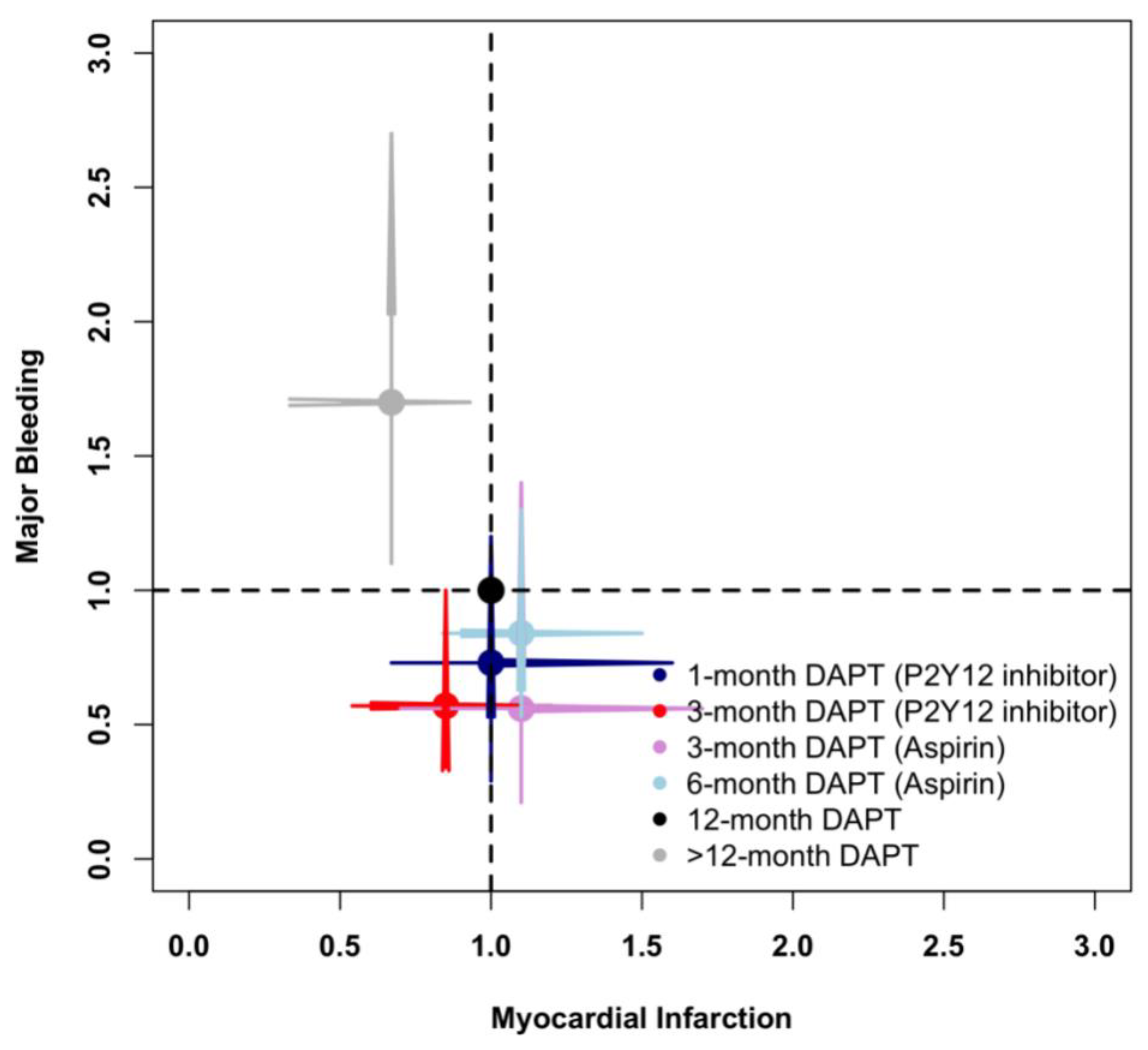
3.1.3. Myocardial Infarction
3.1.4. Major Bleeding
3.2. Secondary Outcomes
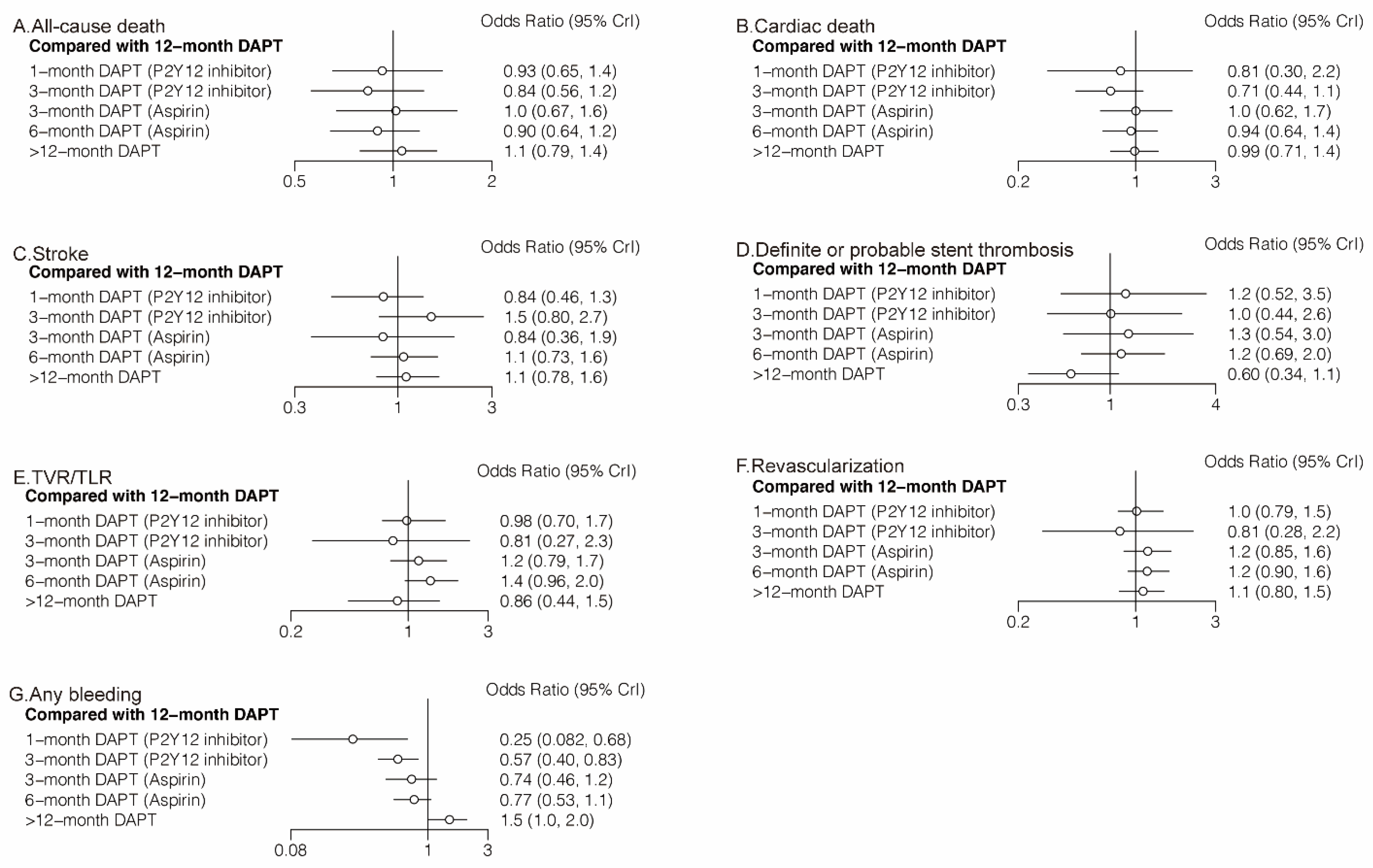
3.2.1. All-Cause Death and Cardiac Death
3.2.2. Stroke and Definite or Probable Stent Thrombosis
3.2.3. TVR/TLR and Revascularization
3.2.4. Any Bleeding
3.3. Network Coherence
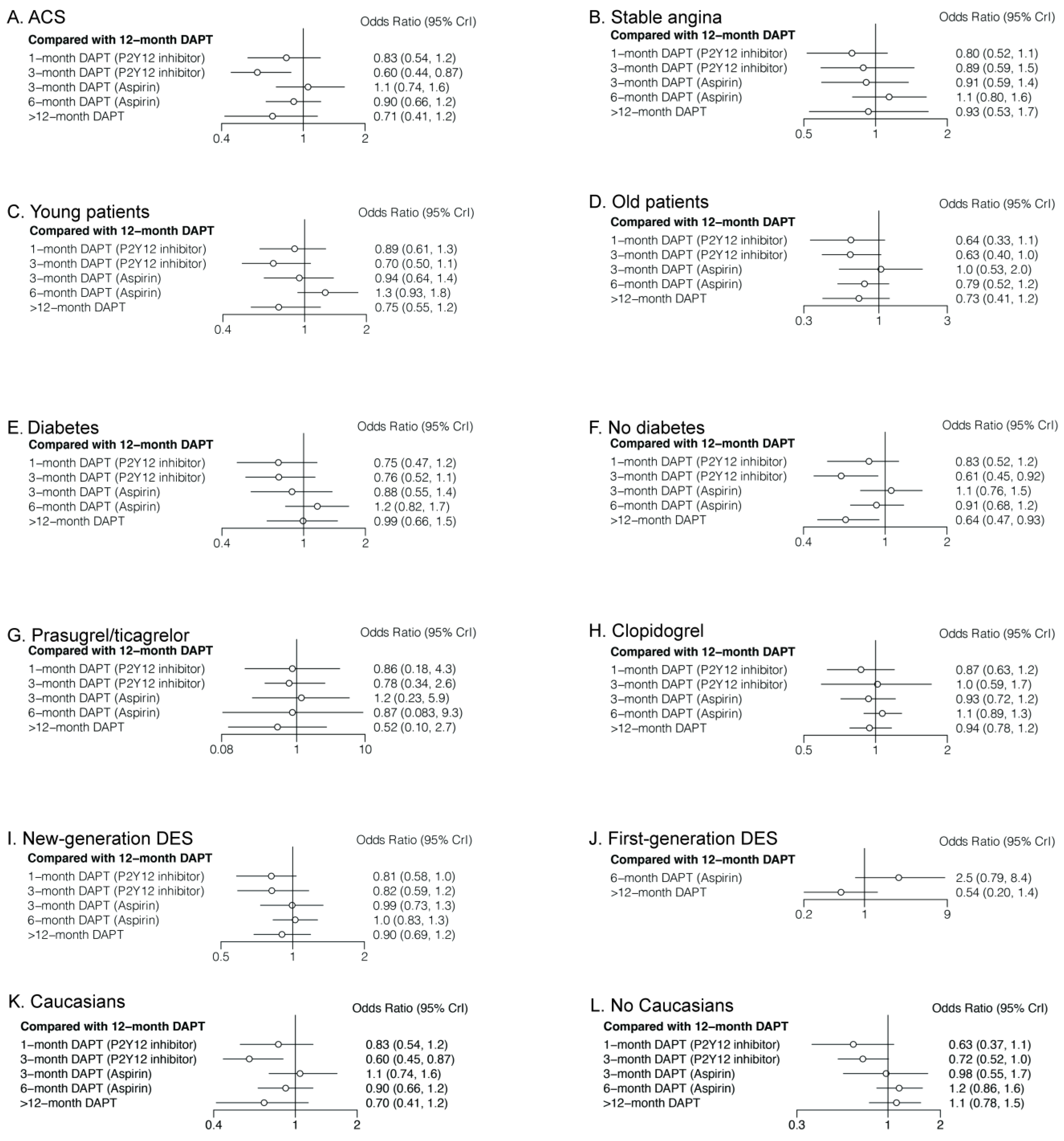
3.4. Subgroup Analyses of Primary Outcomes
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Williams, D.O.; Abbott, J.D.; Kip, K.E. Outcomes of 6906 patients undergoing percutaneous coronary intervention in the era of drug-eluting stents: Report of the DEScover Registry. Circulation 2006, 114, 2154–2162. [Google Scholar] [CrossRef] [PubMed]
- Capodanno, D.; Alfonso, F.; Levine, G.N.; Valgimigli, M.; Angiolillo, D.J. ACC/AHA Versus ESC Guidelines on Dual Antiplatelet Therapy: JACC Guideline Comparison. J. Am. Coll. Cardiol. 2018, 72, 2915–2931. [Google Scholar] [CrossRef] [PubMed]
- Mauri, L.; Hsieh, W.H.; Massaro, J.M.; Ho, K.K.; D’Agostino, R.; Cutlip, D.E. Stent thrombosis in randomized clinical trials of drug-eluting stents. N. Engl. J. Med. 2007, 356, 1020–1029. [Google Scholar] [CrossRef] [PubMed]
- Levine, G.N.; Bates, E.R.; Blankenship, J.C.; Bailey, S.R.; Bittl, J.A.; Cercek, B.; Chambers, C.E.; Ellis, S.G.; Guyton, R.A.; Hollenberg, S.M.; et al. 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention: Executive summary: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Circulation 2011, 124, 2574–2609. [Google Scholar] [PubMed]
- Yusuf, S.; Zhao, F.; Mehta, S.R.; Chrolavicius, S.; Tognoni, G.; Fox, K.K. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N. Engl. J. Med. 2001, 345, 494–502. [Google Scholar]
- Généreux, P.; Giustino, G.; Witzenbichler, B.; Weisz, G.; Stuckey, T.D.; Rinaldi, M.J.; Neumann, F.J.; Metzger, D.C.; Henry, T.D.; Cox, D.A.; et al. Incidence, Predictors, and Impact of Post-Discharge Bleeding After Percutaneous Coronary Intervention. J. Am. Coll. Cardiol. 2015, 66, 1036–1045. [Google Scholar] [CrossRef] [Green Version]
- Vranckx, P.; Valgimigli, M.; Jüni, P.; Hamm, C.; Steg, P.G.; Heg, D.; van Es, G.A.; McFadden, E.P.; Onuma, Y.; van Meijeren, C.; et al. Ticagrelor plus aspirin for 1 month, followed by ticagrelor monotherapy for 23 months vs aspirin plus clopidogrel or ticagrelor for 12 months, followed by aspirin monotherapy for 12 months after implantation of a drug-eluting stent: A multicentre, open-label, randomised superiority trial. Lancet 2018, 392, 940–949. [Google Scholar]
- Helft, G.; Steg, P.G.; Le Feuvre, C.; Georges, J.L.; Carrie, D.; Dreyfus, X.; Furber, A.; Leclercq, F.; Eltchaninoff, H.; Falquier, J.F.; et al. Stopping or continuing clopidogrel 12 months after drug-eluting stent placement: The OPTIDUAL randomized trial. Eur. Heart J. 2016, 37, 365–374. [Google Scholar] [CrossRef] [Green Version]
- Mehran, R.; Baber, U.; Sharma, S.K.; Cohen, D.J.; Angiolillo, D.J.; Briguori, C.; Cha, J.Y.; Collier, T.; Dangas, G.; Dudek, D.; et al. Ticagrelor with or without Aspirin in High-Risk Patients after PCI. N. Engl. J. Med. 2019, 381, 2032–2042. [Google Scholar] [CrossRef]
- Hahn, J.Y.; Song, Y.B.; Oh, J.H.; Chun, W.J.; Park, Y.H.; Jang, W.J.; Im, E.S.; Jeong, J.O.; Cho, B.R.; Oh, S.K.; et al. Effect of P2Y12 Inhibitor Monotherapy vs Dual Antiplatelet Therapy on Cardiovascular Events in Patients Undergoing Percutaneous Coronary Intervention: The SMART-CHOICE Randomized Clinical Trial. JAMA 2019, 321, 2428–2437. [Google Scholar] [CrossRef] [Green Version]
- Kim, B.K.; Hong, S.J.; Cho, Y.H.; Yun, K.H.; Kim, Y.H.; Suh, Y.; Cho, J.Y.; Her, A.Y.; Cho, S.; Jeon, D.W.; et al. Effect of Ticagrelor Monotherapy vs Ticagrelor with Aspirin on Major Bleeding and Cardiovascular Events in Patients with Acute Coronary Syndrome: The TICO Randomized Clinical Trial. JAMA 2020, 323, 2407–2416. [Google Scholar] [CrossRef] [PubMed]
- Chiarito, M.; Sanz-Sánchez, J.; Cannata, F.; Cao, D.; Sturla, M.; Panico, C.; Godino, C.; Regazzoli, D.; Reimers, B.; De Caterina, R.; et al. Monotherapy with a P2Y(12) inhibitor or aspirin for secondary prevention in patients with established atherosclerosis: A systematic review and meta-analysis. Lancet 2020, 395, 1487–1495. [Google Scholar] [CrossRef]
- Giacoppo, D.; Matsuda, Y.; Fovino, L.N.; D’Amico, G.; Gargiulo, G.; Byrne, R.A.; Capodanno, D.; Valgimigli, M.; Mehran, R.; Tarantini, G. Short dual antiplatelet therapy followed by P2Y12 inhibitor monotherapy vs. prolonged dual antiplatelet therapy after percutaneous coronary intervention with second-generation drug-eluting stents: A systematic review and meta-analysis of randomized clinical trials. Eur. Heart J. 2021, 42, 308–319. [Google Scholar] [PubMed]
- O’Donoghue, M.L.; Murphy, S.A.; Sabatine, M.S. The Safety and Efficacy of Aspirin Discontinuation on a Background of a P2Y(12) Inhibitor in Patients After Percutaneous Coronary Intervention: A Systematic Review and Meta-Analysis. Circulation 2020, 142, 538–545. [Google Scholar] [CrossRef]
- Yin, S.H.; Xu, P.; Wang, B.; Lu, Y.; Wu, Q.Y.; Zhou, M.L.; Wu, J.R.; Cai, J.J.; Sun, X.; Yuan, H. Duration of dual antiplatelet therapy after percutaneous coronary intervention with drug-eluting stent: Systematic review and network meta-analysis. BMJ 2019, 365, l2222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawton, J.S.; Tamis-Holland, J.E.; Bangalore, S.; Bates, E.R.; Beckie, T.M.; Bischoff, J.M.; Bittl, J.A.; Cohen, M.G.; DiMaio, J.M.; Don, C.W.; et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e18–e114. [Google Scholar] [CrossRef] [PubMed]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef] [Green Version]
- Salanti, G.; Ades, A.E.; Ioannidis, J.P. Graphical methods and numerical summaries for presenting results from multiple-treatment meta-analysis: An overview and tutorial. J. Clin. Epidemiol. 2011, 64, 163–171. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, H.; Domei, T.; Morimoto, T.; Natsuaki, M.; Shiomi, H.; Toyota, T.; Ohya, M.; Suwa, S.; Takagi, K.; Nanasato, M.; et al. Effect of 1-Month Dual Antiplatelet Therapy Followed by Clopidogrel vs 12-Month Dual Antiplatelet Therapy on Cardiovascular and Bleeding Events in Patients Receiving PCI: The STOPDAPT-2 Randomized Clinical Trial. JAMA 2019, 321, 2414–2427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feres, F.; Costa, R.A.; Abizaid, A.; Leon, M.B.; Marin-Neto, J.A.; Botelho, R.V.; King, S.B.; Negoita, M.; Liu, M.; de Paula, J.E.; et al. Three vs twelve months of dual antiplatelet therapy after zotarolimus-eluting stents: The OPTIMIZE randomized trial. JAMA 2013, 310, 2510–2522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, B.K.; Hong, M.K.; Shin, D.H.; Nam, C.M.; Kim, J.S.; Ko, Y.G.; Choi, D.; Kang, T.S.; Park, B.E.; Kang, W.C.; et al. A new strategy for discontinuation of dual antiplatelet therapy: The RESET Trial (REal Safety and Efficacy of 3-month dual antiplatelet Therapy following Endeavor zotarolimus-eluting stent implantation). J. Am. Coll. Cardiol. 2012, 60, 1340–1348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Luca, G.; Damen, S.A.; Camaro, C.; Benit, E.; Verdoia, M.; Rasoul, S.; Liew, H.B.; Polad, J.; Ahmad, W.A.; Zambahari, R.; et al. Final results of the randomised evaluation of short-term dual antiplatelet therapy in patients with acute coronary syndrome treated with a new-generation stent (REDUCE trial). EuroIntervention 2019, 15, e990–e998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, B.K.; Kim, J.S.; Lee, O.H.; Min, P.K.; Yoon, Y.W.; Hong, B.K.; Shin, D.H.; Kang, T.S.; Kim, B.O.; Cho, D.K.; et al. Safety of six-month dual antiplatelet therapy after second-generation drug-eluting stent implantation: OPTIMA-C Randomised Clinical Trial and OCT Substudy. EuroIntervention 2018, 13, 1923–1930. [Google Scholar] [CrossRef]
- Han, Y.; Xu, B.; Xu, K.; Guan, C.; Jing, Q.; Zheng, Q.; Li, X.; Zhao, X.; Wang, H.; Zhao, X.; et al. Six Versus 12 Months of Dual Antiplatelet Therapy After Implantation of Biodegradable Polymer Sirolimus-Eluting Stent: Randomized Substudy of the I-LOVE-IT 2 Trial. Circ. Cardiovasc. Interv. 2016, 9, e003145. [Google Scholar] [CrossRef] [Green Version]
- Hong, S.J.; Shin, D.H.; Kim, J.S.; Kim, B.K.; Ko, Y.G.; Choi, D.; Her, A.Y.; Kim, Y.H.; Jang, Y.; Hong, M.K. 6-Month Versus 12-Month Dual-Antiplatelet Therapy Following Long Everolimus-Eluting Stent Implantation: The IVUS-XPL Randomized Clinical Trial. JACC Cardiovasc. Interv. 2016, 9, 1438–1446. [Google Scholar] [CrossRef] [PubMed]
- Schulz-Schüpke, S.; Byrne, R.A.; Ten Berg, J.M.; Neumann, F.J.; Han, Y.; Adriaenssens, T.; Tölg, R.; Seyfarth, M.; Maeng, M.; Zrenner, B.; et al. ISAR-SAFE: A randomized, double-blind, placebo-controlled trial of 6 vs. 12 months of clopidogrel therapy after drug-eluting stenting. Eur. Heart J. 2015, 36, 1252–1263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colombo, A.; Chieffo, A.; Frasheri, A.; Garbo, R.; Masotti-Centol, M.; Salvatella, N.; Oteo Dominguez, J.F.; Steffanon, L.; Tarantini, G.; Presbitero, P.; et al. Second-generation drug-eluting stent implantation followed by 6- versus 12-month dual antiplatelet therapy: The SECURITY randomized clinical trial. J. Am. Coll. Cardiol. 2014, 64, 2086–2097. [Google Scholar] [CrossRef]
- Gwon, H.C.; Hahn, J.Y.; Park, K.W.; Song, Y.B.; Chae, I.H.; Lim, D.S.; Han, K.R.; Choi, J.H.; Choi, S.H.; Kang, H.J.; et al. Six-month versus 12-month dual antiplatelet therapy after implantation of drug-eluting stents: The Efficacy of Xience/Promus Versus Cypher to Reduce Late Loss After Stenting (EXCELLENT) randomized, multicenter study. Circulation 2012, 125, 505–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kedhi, E.; Fabris, E.; van der Ent, M.; Buszman, P.; von Birgelen, C.; Roolvink, V.; Zurakowski, A.; Schotborgh, C.E.; Hoorntje, J.C.A.; Eek, C.H.; et al. Six months versus 12 months dual antiplatelet therapy after drug-eluting stent implantation in ST-elevation myocardial infarction (DAPT-STEMI): Randomised, multicentre, non-inferiority trial. BMJ 2018, 363, k3793. [Google Scholar] [CrossRef] [Green Version]
- Hahn, J.Y.; Song, Y.B.; Oh, J.H.; Cho, D.K.; Lee, J.B.; Doh, J.H.; Kim, S.H.; Jeong, J.O.; Bae, J.H.; Kim, B.O.; et al. 6-month versus 12-month or longer dual antiplatelet therapy after percutaneous coronary intervention in patients with acute coronary syndrome (SMART-DATE): A randomised, open-label, non-inferiority trial. Lancet 2018, 391, 1274–1284. [Google Scholar] [CrossRef]
- Nakamura, M.; Iijima, R.; Ako, J.; Shinke, T.; Okada, H.; Ito, Y.; Ando, K.; Anzai, H.; Tanaka, H.; Ueda, Y.; et al. Dual Antiplatelet Therapy for 6 Versus 18 Months After Biodegradable Polymer Drug-Eluting Stent Implantation. JACC Cardiovasc. Interv. 2017, 10, 1189–1198. [Google Scholar] [CrossRef] [PubMed]
- Didier, R.; Morice, M.C.; Barragan, P.; Noryani, A.A.L.; Noor, H.A.; Majwal, T.; Hovasse, T.; Castellant, P.; Schneeberger, M.; Maillard, L.; et al. 6-Versus 24-Month Dual Antiplatelet Therapy After Implantation of Drug-Eluting Stents in Patients Nonresistant to Aspirin: Final Results of the ITALIC Trial (Is There a Life for DES After Discontinuation of Clopidogrel). JACC Cardiovasc. Interv. 2017, 10, 1202–1210. [Google Scholar] [CrossRef] [PubMed]
- Valgimigli, M.; Campo, G.; Monti, M.; Vranckx, P.; Percoco, G.; Tumscitz, C.; Castriota, F.; Colombo, F.; Tebaldi, M.; Fucà, G.; et al. Short- versus long-term duration of dual-antiplatelet therapy after coronary stenting: A randomized multicenter trial. Circulation 2012, 125, 2015–2026. [Google Scholar] [CrossRef] [Green Version]
- Collet, J.P.; Silvain, J.; Barthélémy, O.; Rangé, G.; Cayla, G.; Van Belle, E.; Cuisset, T.; Elhadad, S.; Schiele, F.; Lhoest, N.; et al. Dual-antiplatelet treatment beyond 1 year after drug-eluting stent implantation (ARCTIC-Interruption): A randomised trial. Lancet 2014, 384, 1577–1585. [Google Scholar] [CrossRef]
- Mauri, L.; Kereiakes, D.J.; Yeh, R.W.; Driscoll-Shempp, P.; Cutlip, D.E.; Steg, P.G.; Normand, S.L.; Braunwald, E.; Wiviott, S.D.; Cohen, D.J.; et al. Twelve or 30 months of dual antiplatelet therapy after drug-eluting stents. N. Engl. J. Med. 2014, 371, 2155–2166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, C.W.; Ahn, J.M.; Park, D.W.; Kang, S.J.; Lee, S.W.; Kim, Y.H.; Park, S.W.; Han, S.; Lee, S.G.; Seong, I.W.; et al. Optimal duration of dual antiplatelet therapy after drug-eluting stent implantation: A randomized, controlled trial. Circulation 2014, 129, 304–312. [Google Scholar] [CrossRef] [Green Version]
- Park, S.J.; Park, D.W.; Kim, Y.H.; Kang, S.J.; Lee, S.W.; Lee, C.W.; Han, K.H.; Park, S.W.; Yun, S.C.; Lee, S.G.; et al. Duration of dual antiplatelet therapy after implantation of drug-eluting stents. N. Engl. J. Med. 2010, 362, 1374–1382. [Google Scholar] [CrossRef] [Green Version]
- Capodanno, D.; Mehran, R.; Valgimigli, M.; Baber, U.; Windecker, S.; Vranckx, P.; Dangas, G.; Rollini, F.; Kimura, T.; Collet, J.P.; et al. Aspirin-free strategies in cardiovascular disease and cardioembolic stroke prevention. Nat. Rev. Cardiol. 2018, 15, 480–496. [Google Scholar] [CrossRef]
- Palmerini, T.; Benedetto, U.; Bacchi-Reggiani, L.; Della Riva, D.; Biondi-Zoccai, G.; Feres, F.; Abizaid, A.; Hong, M.K.; Kim, B.K.; Jang, Y.; et al. Mortality in patients treated with extended duration dual antiplatelet therapy after drug-eluting stent implantation: A pairwise and Bayesian network meta-analysis of randomised trials. Lancet 2015, 385, 2371–2382. [Google Scholar] [CrossRef]
- Traby, L.; Kollars, M.; Kaider, A.; Eichinger, S.; Wolzt, M.; Kyrle, P.A. Effects of P2Y12 receptor inhibition with or without aspirin on hemostatic system activation: A randomized trial in healthy subjects. J. Thromb. Haemost. 2016, 14, 273–281. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, P.C.; Leadbeater, P.D.; Chan, M.V.; Kirkby, N.S.; Jakubowski, J.A.; Mitchell, J.A.; Warner, T.D. In the presence of strong P2Y12 receptor blockade, aspirin provides little additional inhibition of platelet aggregation. J. Thromb. Haemost. 2011, 9, 552–561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valgimigli, M.; Costa, F.; Lokhnygina, Y.; Clare, R.M.; Wallentin, L.; Moliterno, D.J.; Armstrong, P.W.; White, H.D.; Held, C.; Aylward, P.E.; et al. Trade-off of myocardial infarction vs. bleeding types on mortality after acute coronary syndrome: Lessons from the Thrombin Receptor Antagonist for Clinical Event Reduction in Acute Coronary Syndrome (TRACER) randomized trial. Eur. Heart J. 2017, 38, 804–810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stefanini, G.G.; Byrne, R.A.; Serruys, P.W.; de Waha, A.; Meier, B.; Massberg, S.; Jüni, P.; Schömig, A.; Windecker, S.; Kastrati, A. Biodegradable polymer drug-eluting stents reduce the risk of stent thrombosis at 4 years in patients undergoing percutaneous coronary intervention: A pooled analysis of individual patient data from the ISAR-TEST 3, ISAR-TEST 4, and LEADERS randomized trials. Eur. Heart J. 2012, 33, 1214–1222. [Google Scholar] [PubMed] [Green Version]
- Stefanini, G.G.; Baber, U.; Windecker, S.; Morice, M.C.; Sartori, S.; Leon, M.B.; Stone, G.W.; Serruys, P.W.; Wijns, W.; Weisz, G.; et al. Safety and efficacy of drug-eluting stents in women: A patient-level pooled analysis of randomised trials. Lancet 2013, 382, 1879–1888. [Google Scholar] [CrossRef]
- Loh, J.P.; Pendyala, L.K.; Kitabata, H.; Torguson, R.; Omar, A.; Minha, S.; Chen, F.; Satler, L.F.; Pichard, A.D.; Waksman, R. Comparison of outcomes after percutaneous coronary intervention among different coronary subsets (stable and unstable angina pectoris and ST-segment and non-ST-segment myocardial infarction). Am. J. Cardiol. 2014, 113, 1794–1801. [Google Scholar] [CrossRef]
- Levine, G.N.; Bates, E.R.; Bittl, J.A.; Brindis, R.G.; Fihn, S.D.; Fleisher, L.A.; Granger, C.B.; Lange, R.A.; Mack, M.J.; Mauri, L.; et al. 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients with Coronary Artery Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines: An Update of the 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention, 2011 ACCF/AHA Guideline for Coronary Artery Bypass Graft Surgery, 2012 ACC/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease, 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction, 2014 AHA/ACC Guideline for the Management of Patients With Non-ST-Elevation Acute Coronary Syndromes, and 2014 ACC/AHA Guideline on Perioperative Cardiovascular Evaluation and Management of Patients Undergoing Noncardiac Surgery. Circulation 2016, 134, e123–e155. [Google Scholar] [PubMed] [Green Version]
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef]
- Kubo, T.; Maehara, A.; Mintz, G.S.; Doi, H.; Tsujita, K.; Choi, S.Y.; Katoh, O.; Nasu, K.; Koenig, A.; Pieper, M.; et al. The dynamic nature of coronary artery lesion morphology assessed by serial virtual histology intravascular ultrasound tissue characterization. J. Am. Coll. Cardiol. 2010, 55, 1590–1597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Capodanno, D.; Gargiulo, G.; Buccheri, S.; Giacoppo, D.; Capranzano, P.; Tamburino, C. Meta-Analyses of Dual Antiplatelet Therapy Following Drug-Eluting Stent Implantation: Do Bleeding and Stent Thrombosis Weigh Similar on Mortality? J. Am. Coll. Cardiol. 2015, 66, 1639–1640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, S.U.; Singh, M.; Valavoor, S.; Khan, M.U.; Lone, A.N.; Khan, M.Z.; Khan, M.S.; Mani, P.; Kapadia, S.R.; Michos, E.D.; et al. Dual Antiplatelet Therapy After Percutaneous Coronary Intervention and Drug-Eluting Stents: A Systematic Review and Network Meta-Analysis. Circulation 2020, 142, 1425–1436. [Google Scholar] [CrossRef] [PubMed]
- Wiviott, S.D.; Braunwald, E.; McCabe, C.H.; Montalescot, G.; Ruzyllo, W.; Gottlieb, S.; Neumann, F.J.; Ardissino, D.; De Servi, S.; Murphy, S.A.; et al. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N. Engl. J. Med. 2007, 357, 2001–2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallentin, L.; Becker, R.C.; Budaj, A.; Cannon, C.P.; Emanuelsson, H.; Held, C.; Horrow, J.; Husted, S.; James, S.; Katus, H.; et al. Ticagrelor versus clopidogrel in patients with acute coronary syndromes. N. Engl. J. Med. 2009, 361, 1045–1057. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Net Clinical Events | ||||||
| Ischemic events | 1-month DAPT (P2Y12 inhibitor) | 1.13 (0.66, 1.99) | 1.56 (0.93, 2.67) | 1.62 (0.98, 2.72) | 1.58 (0.99, 2.57) | 1.58 (0.94, 2.65) |
| 1.01 (0.64, 1.68) | 3-month DAPT (P2Y12 inhibitor) | 1.38 (0.97, 1.96) | 1.42 (1.03, 1.98) | 1.39 (1.06, 1.82) | 1.39 (0.99, 1.94) | |
| 0.93 (0.58, 1.61) | 0.92 (0.58, 1.48) | 3-month DAPT (aspirin) | 1.04 (0.77, 1.38) | 1.01 (0.81, 1.27) | 1.01 (0.75, 1.37) | |
| 0.87 (0.56, 1.36) | 0.86 (0.56, 1.27) | 0.93 (0.59, 1.39) | 6-month DAPT (aspirin) | 0.98 (0.81, 1.18) | 0.98 (0.79, 1.19) | |
| 0.94 (0.67, 1.39) | 0.93 (0.68, 1.29) | 1.01 (0.71, 1.41) | 1.09 (0.86, 1.43) | 12-month DAPT | 1.00 (0.81, 1.22) | |
| 0.95 (0.60, 1.44) | 0.94 (0.61, 1.36) | 1.01 (0.64, 1.49) | 1.09 (0.83, 1.39) | 1 (0.76, 1.25) | >12-month DAPT | |
| Myocardial Infarction | ||||||
| Major bleeding | 1-month DAPT (P2Y12 inhibitor) | 0.84 (0.43, 1.43) | 1.09 (0.57, 1.97) | 1.08 (0.65, 1.85) | 0.98 (0.63, 1.49) | 0.65 (0.40, 1.14) |
| 1.27 (0.42, 2.49) | 3-month DAPT (P2Y12 inhibitor) | 1.31 (0.73, 2.45) | 1.30 (0.82, 2.31) | 1.18 (0.81, 1.86) | 0.78 (0.50, 1.43) | |
| 1.27 (0.36, 3.60) | 1.02 (0.37, 3.16) | 3-month DAPT (aspirin) | 1.00 (0.59, 1.77) | 0.90 (0.58, 1.43) | 0.60 (0.36, 1.09) | |
| 0.86 (0.32, 1.68) | 0.68 (0.35, 1.43) | 0.67 (0.23, 1.80) | 6-month DAPT (aspirin) | 0.90 (0.67, 1.19) | 0.61 (0.44, 0.86) | |
| 0.73 (0.29, 1.19) | 0.57 (0.34, 1.00) | 0.56 (0.21, 1.36) | 0.84 (0.53, 1.30) | 12-month DAPT | 0.67 (0.51, 0.93) | |
| 0.42 (0.14, 0.78) | 0.33 (0.17, 0.66) | 0.33 (0.11, 0.87) | 0.49 (0.29, 0.78) | 0.58 (0.37, 0.89) | >12-month DAPT | |
| All-Cause Death | ||||||
| Cardiac death | 1-month DAPT (P2Y12 inhibitor) | 0.90 (0.51, 1.52) | 1.10 (0.61, 1.91) | 0.97 (0.55, 1.49) | 1.08 (0.71, 1.53) | 1.15 (0.67, 1.72) |
| 1.15 (0.40, 3.44) | 3-month DAPT (P2Y12 inhibitor) | 1.22 (0.69, 2.20) | 1.07 (0.63, 1.73) | 1.19 (0.81, 1.78) | 1.28 (0.77, 2.00) | |
| 0.81 (0.27, 2.45) | 0.70 (0.36, 1.37) | 3-month DAPT (aspirin) | 0.88 (0.50, 1.48) | 0.98 (0.64, 1.49) | 1.04 (0.61, 1.68) | |
| 0.87 (0.30, 2.50) | 0.76 (0.42, 1.37) | 1.07 (0.58, 2.02) | 6-month DAPT (aspirin) | 1.12 (0.83, 1.56) | 1.18 (0.90, 1.57) | |
| 0.81 (0.30, 2.18) | 0.71 (0.44, 1.11) | 1.00 (0.62, 1.66) | 0.94 (0.64, 1.35) | 12-month DAPT | 1.06 (0.79, 1.36) | |
| 0.83 (0.29, 2.34) | 0.72 (0.41, 1.27) | 1.02 (0.57, 1.87) | 0.95 (0.68, 1.34) | 1.01 (0.73, 1.41) | >12-month DAPT | |
| Stroke | ||||||
| Definite or probable stent thrombosis | 1-month DAPT (P2Y12 inhibitor) | 1.75 (0.82, 4.10) | 1.00 (0.38, 2.75) | 1.27 (0.69, 2.59) | 1.18 (0.74, 2.17) | 1.31 (0.74, 2.72) |
| 1.22 (0.36, 4.58) | 3-month DAPT (P2Y12 inhibitor) | 0.57 (0.20, 1.56) | 0.73 (0.35, 1.49) | 0.68 (0.37, 1.24) | 0.75 (0.37, 1.53) | |
| 0.97 (0.30, 3.86) | 0.80 (0.25, 2.86) | 3-month DAPT (aspirin) | 1.27 (0.52, 3.20) | 1.19 (0.52, 2.74) | 1.32 (0.55, 3.27) | |
| 1.07 (0.38, 3.36) | 0.88 (0.31, 2.46) | 1.10 (0.38, 2.97) | 6-month DAPT (aspirin) | 0.94 (0.63, 1.37) | 1.03 (0.69, 1.56) | |
| 1.23 (0.52, 3.54) | 1.01 (0.44, 2.56) | 1.27 (0.54, 2.97) | 1.16 (0.69, 2.04) | 12-month DAPT | 1.10 (0.78, 1.61) | |
| 2.08 (0.72, 6.55) | 1.69 (0.60, 4.87) | 2.13 (0.72, 5.87) | 1.92 (1.03, 3.71) | 1.67 (0.89, 2.92) | >12-month DAPT | |
| TVR/TLR | ||||||
| Revascularization | 1-month DAPT (P2Y12 inhibitor) | 0.81 (0.24, 2.38) | 1.17 (0.60, 1.93) | 1.37 (0.75, 2.23) | 1.02 (0.60, 1.42) | 0.87 (0.36, 1.66) |
| 1.28 (0.45, 3.94) | 3-month DAPT (P2Y12 inhibitor) | 1.43 (0.46, 4.58) | 1.69 (0.56, 5.42) | 1.23 (0.43, 3.71) | 1.07 (0.31, 3.58) | |
| 0.86 (0.58, 1.42) | 0.68 (0.23, 1.97) | 3-month DAPT (aspirin) | 1.17 (0.71, 2.04) | 0.87 (0.59, 1.27) | 0.75 (0.34, 1.47) | |
| 0.87 (0.58, 1.33) | 0.68 (0.22, 1.93) | 1.01 (0.64, 1.52) | 6-month DAPT (aspirin) | 0.74 (0.51, 1.04) | 0.64 (0.30, 1.20) | |
| 1.01 (0.79, 1.46) | 0.81 (0.28, 2.21) | 1.18 (0.85, 1.63) | 1.17 (0.90, 1.59) | 12-month DAPT | 0.86 (0.44, 1.54) | |
| 0.92 (0.63, 1.55) | 0.73 (0.24, 2.10) | 1.07 (0.70, 1.70) | 1.06 (0.74, 1.66) | 0.90 (0.68, 1.25) | >12-month DAPT | |
| Any bleeding | ||||||
| 1-month DAPT (P2Y12 inhibitor) | 2.3 (0.80, 7.48) | 2.96 (0.99, 9.85) | 3.09 (1.07, 9.82) | 3.99 (1.46, 12.23) | 5.94 (2.00, 18.66) | |
| 3-month DAPT (P2Y12 inhibitor) | 1.29 (0.71, 2.28) | 1.35 (0.79, 2.14) | 1.74 (1.20, 2.49) | 2.59 (1.47, 4.05) | ||
| 3-month DAPT (aspirin) | 1.05 (0.59, 1.82) | 1.35 (0.86, 2.17) | 2.01 (1.10, 3.47) | |||
| 6-month DAPT (aspirin) | 1.29 (0.95, 1.87) | 1.91 (1.32, 2.71) | ||||
| 12-month DAPT | 1.48 (1.00, 2.04) | |||||
| >12-month DAPT | ||||||
| ACS | ||||||
| Stable angina | 1-month DAPT (P2Y12 inhibitor) | 0.72 (0.45, 1.30) | 1.27 (0.77, 2.35) | 1.09 (0.66, 1.85) | 1.21 (0.83, 1.86) | 0.85 (0.44, 1.65) |
| 0.90 (0.45, 1.51) | 3-month DAPT (P2Y12 inhibitor) | 1.76 (1.05, 2.87) | 1.50 (0.92, 2.27) | 1.67 (1.15, 2.25) | 1.18 (0.60, 2.09) | |
| 0.87 (0.48, 1.50) | 0.97 (0.55, 1.89) | 3-month DAPT (aspirin) | 0.85 (0.51, 1.36) | 0.95 (0.63, 1.35) | 0.67 (0.33, 1.23) | |
| 0.70 (0.39, 1.13) | 0.78 (0.45, 1.42) | 0.80 (0.46, 1.38) | 6-month DAPT (aspirin) | 1.11 (0.82, 1.52) | 0.79 (0.49, 1.21) | |
| 0.80 (0.52, 1.12) | 0.89 (0.59, 1.45) | 0.91 (0.59, 1.37) | 1.14 (0.80, 1.63) | 12-month DAPT | 0.71 (0.41, 1.17) | |
| 0.85 (0.41, 1.63) | 0.95 (0.47, 2.05) | 0.98 (0.48, 1.96) | 1.22 (0.68, 2.16) | 1.07 (0.60, 1.90) | >12-month DAPT | |
| Young Patients | ||||||
| Old patients | 1-month DAPT (P2Y12 inhibitor) | 0.79 (0.49, 1.44) | 1.05 (0.63, 1.86) | 1.41 (0.91, 2.49) | 1.12 (0.79, 1.65) | 0.84 (0.54, 1.59) |
| 1.01 (0.43, 2.02) | 3-month DAPT (P2Y12 inhibitor) | 1.33 (0.75, 2.22) | 1.78 (1.09, 2.93) | 1.42 (0.94, 2.01) | 1.07 (0.65, 1.84) | |
| 0.62 (0.24, 1.44) | 0.62 (0.28, 1.42) | 3-month DAPT (aspirin) | 1.34 (0.83, 2.30) | 1.06 (0.72, 1.57) | 0.80 (0.50, 1.45) | |
| 0.80 (0.38, 1.60) | 0.79 (0.44, 1.55) | 1.30 (0.61, 2.90) | 6-month DAPT (aspirin) | 0.79 (0.55, 1.08) | 0.60 (0.41, 0.90) | |
| 0.64 (0.33, 1.10) | 0.63 (0.40, 1.03) | 1.03 (0.53, 2.01) | 0.79 (0.52, 1.17) | 12-month DAPT | 0.75 (0.55, 1.20) | |
| 0.87 (0.39, 1.94) | 0.87 (0.46, 1.91) | 1.42 (0.64, 3.47) | 1.09 (0.67, 1.92) | 1.38 (0.84, 2.46) | >12-month DAPT | |
| Diabetes | ||||||
| No diabetes | 1-month DAPT (P2Y12 inhibitor) | 1.00 (0.57, 1.87) | 1.17 (0.62, 2.21) | 1.54 (0.88, 2.75) | 1.33 (0.86, 2.11) | 1.32 (0.74, 2.40) |
| 1.37 (0.70, 2.10) | 3-month DAPT (P2Y12 inhibitor) | 1.16 (0.63, 2.06) | 1.54 (0.89, 2.57) | 1.32 (0.88, 1.92) | 1.31 (0.74, 2.23) | |
| 0.78 (0.44, 1.24) | 0.57 (0.37, 0.98) | 3-month DAPT (aspirin) | 1.33 (0.75, 2.38) | 1.14 (0.73, 1.80) | 1.13 (0.62, 2.08) | |
| 0.92 (0.53, 1.42) | 0.68 (0.44, 1.11) | 1.18 (0.74, 1.87) | 6-month DAPT (aspirin) | 0.86 (0.60, 1.23) | 0.85 (0.56, 1.31) | |
| 0.83 (0.52, 1.16) | 0.61 (0.45, 0.92) | 1.07 (0.76, 1.52) | 0.91 (0.68, 1.23) | 12-month DAPT | 0.99 (0.66, 1.46) | |
| 1.30 (0.70, 2.04) | 0.95 (0.60, 1.58) | 1.67 (1.00, 2.65) | 1.41 (0.97, 2.01) | 1.56 (1.07, 2.13) | >12-month DAPT | |
| Prasugrel/Ticagrelor | ||||||
| Clopidogrel | 1-month DAPT (P2Y12 inhibitor) | 0.88 (0.17, 7.07) | 1.36 (0.14, 12.95) | 1.02 (0.06, 17.86) | 1.16 (0.23, 5.68) | 0.61 (0.06, 6.02) |
| 0.85 (0.46, 1.60) | 3-month DAPT (P2Y12 inhibitor) | 1.52 (0.18, 8.20) | 1.10 (0.07, 12.21) | 1.29 (0.39, 2.90) | 0.69 (0.09, 3.80) | |
| 0.93 (0.62, 1.42) | 1.09 (0.60, 1.98) | 3-month DAPT (aspirin) | 0.75 (0.05, 13.66) | 0.85 (0.17, 4.43) | 0.45 (0.05, 4.64) | |
| 0.81 (0.56, 1.18) | 0.95 (0.53, 1.66) | 0.88 (0.63, 1.20) | 6-month DAPT (aspirin) | 1.15 (0.11, 12.04) | 0.60 (0.11, 3.52) | |
| 0.87 (0.63, 1.20) | 1.02 (0.59, 1.71) | 0.93 (0.72, 1.21) | 1.07 (0.89, 1.29) | 12-month DAPT | 0.52 (0.10, 2.73) | |
| 0.92 (0.62, 1.33) | 1.08 (0.60, 1.86) | 0.99 (0.70, 1.35) | 1.13 (0.88, 1.45) | 1.06 (0.86, 1.28) | >12-month DAPT | |
| New-Generation DESs | ||||||
| First-generation DESs | 1-month DAPT (P2Y12 inhibitor) | 1.01 (0.67, 1.66) | 1.22 (0.84, 1.94) | 1.26 (0.92, 1.87) | 1.23 (0.97, 1.72) | 1.12 (0.78, 1.70) |
| - | 3-month DAPT (P2Y12 inhibitor) | 1.22 (0.76, 1.90) | 1.25 (0.83, 1.87) | 1.22 (0.86, 1.70) | 1.11 (0.70, 1.69) | |
| - | - | 3-month DAPT (aspirin) | 1.03 (0.71, 1.51) | 1.01 (0.75, 1.37) | 0.91 (0.60, 1.38) | |
| - | - | - | 6-month DAPT (aspirin) | 0.98 (0.79, 1.21) | 0.88 (0.68, 1.14) | |
| - | - | - | 2.48 (0.79, 8.43) | 12-month DAPT | 0.90 (0.69, 1.19) | |
| - | - | - | 4.63 (1.05, 21.99) | 1.87 (0.71, 4.97) | >12-month DAPT | |
| Caucasians | ||||||
| No Caucasian | 1-month DAPT (P2Y12 inhibitor) | 0.72 (0.45, 1.32) | 1.27 (0.77, 2.36) | 1.09 (0.66, 1.83) | 1.21 (0.82, 1.86) | 0.85 (0.44, 1.62) |
| 0.88 (0.47, 1.66) | 3-month DAPT (P2Y12 inhibitor) | 1.76 (1.05, 2.89) | 1.5 (0.92, 2.3) | 1.68 (1.15, 2.25) | 1.18 (0.59, 2.09) | |
| 0.65 (0.3, 1.41) | 0.74 (0.38, 1.42) | 3-month DAPT (aspirin) | 0.85 (0.5, 1.36) | 0.95 (0.63, 1.34) | 0.67 (0.33, 1.22) | |
| 0.55 (0.29, 1.02) | 0.62 (0.39, 0.97) | 0.84 (0.44, 1.59) | 6-month DAPT (aspirin) | 1.12 (0.82, 1.52) | 0.79 (0.49, 1.2) | |
| 0.63 (0.37, 1.08) | 0.72 (0.52, 1.01) | 0.98 (0.55, 1.69) | 1.16 (0.86, 1.58) | 12-month DAPT | 0.7 (0.41, 1.16) | |
| 0.56 (0.3, 1.07) | 0.64 (0.41, 1.06) | 0.87 (0.46, 1.68) | 1.04 (0.78, 1.43) | 0.89 (0.65, 1.28) | >12-month DAPT | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, M.; Gao, X.; Yang, J.; Yang, Y. The Optimal Strategy of Dual Antiplatelet Therapy after Percutaneous Coronary Intervention with Drug-Eluting Stent. J. Clin. Med. 2022, 11, 4465. https://doi.org/10.3390/jcm11154465
Hu M, Gao X, Yang J, Yang Y. The Optimal Strategy of Dual Antiplatelet Therapy after Percutaneous Coronary Intervention with Drug-Eluting Stent. Journal of Clinical Medicine. 2022; 11(15):4465. https://doi.org/10.3390/jcm11154465
Chicago/Turabian StyleHu, Mengjin, Xiaojin Gao, Jingang Yang, and Yuejin Yang. 2022. "The Optimal Strategy of Dual Antiplatelet Therapy after Percutaneous Coronary Intervention with Drug-Eluting Stent" Journal of Clinical Medicine 11, no. 15: 4465. https://doi.org/10.3390/jcm11154465
APA StyleHu, M., Gao, X., Yang, J., & Yang, Y. (2022). The Optimal Strategy of Dual Antiplatelet Therapy after Percutaneous Coronary Intervention with Drug-Eluting Stent. Journal of Clinical Medicine, 11(15), 4465. https://doi.org/10.3390/jcm11154465