
Catheter-Associated Urinary Infections and Consequences of Using Coated versus Non-Coated Urethral Catheters—Outcomes of a Systematic Review and Meta-Analysis of Randomized Trials

 ,
,  ,
,  , , , ,
, , , ,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Aim of This Review
2.2. Literature Search
2.3. Selection Criteria
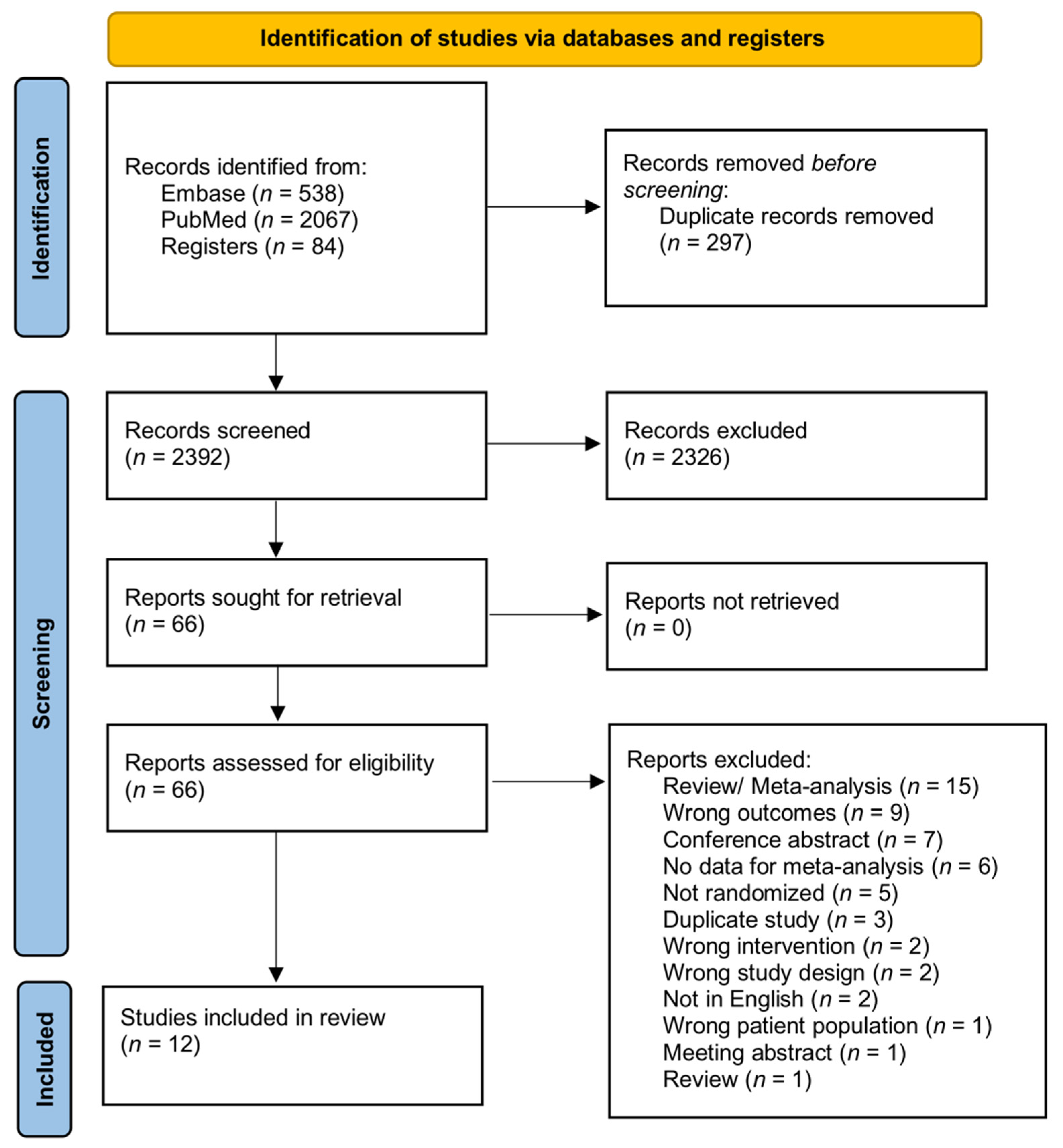
2.4. Study Screening and Selection
2.5. Statistical Analysis
3. Results
3.1. Study Characteristics and Quality Assessment
3.2. Meta-Analysis of CAUTI
3.3. Meta-Analysis of Need for Catheter Removal or Catheter Exchange
3.4. Meta-Analysis of Lower Urinary Tract Symptoms at Follow-Up after Removal of Catheter
3.5. Meta-Analysis of Hematuria Incidence
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Feneley, R.C.L.; Hopley, I.B.; Wells, P.N.T. Urinary Catheters: History, Current Status, Adverse Events and Research Agenda. J. Med. Eng. Technol. 2015, 39, 459–470. [Google Scholar] [CrossRef] [PubMed]
- Andersen, M.J.; Flores-Mireles, A.L. Urinary Catheter Coating Modifications: The Race against Catheter-Associated Infections. Coatings 2020, 10, 23. [Google Scholar] [CrossRef]
- Henly, E.L.; Dowling, J.A.R.; Maingay, J.B.; Lacey, M.M.; Smith, T.J.; Forbes, S. Biocide Exposure Induces Changes in Susceptibility, Pathogenicity, and Biofilm Formation in Uropathogenic Escherichia Coli. Antimicrob. Agents Chemother. 2019, 63, e01892-18. [Google Scholar] [CrossRef]
- Kazmierska, K.A.; Thompson, R.; Morris, N.; Long, A.; Ciach, T. In Vitro Multicompartmental Bladder Model for Assessing Blockage of Urinary Catheters: Effect of Hydrogel Coating on Dynamics of Proteus Mirabilis Growth. Urology 2010, 76, 515.e15–515.e20. [Google Scholar] [CrossRef] [PubMed]
- Desai, D.G.; Liao, K.S.; Cevallos, M.E.; Trautner, B.W. Silver or Nitrofurazone Impregnation of Urinary Catheters Has a Minimal Effect on Uropathogen Adherence. J. Urol. 2010, 184, 2565–2571. [Google Scholar] [CrossRef] [PubMed]
- Lam, T.B.L.; Omar, M.I.; Fisher, E.; Gillies, K.; MacLennan, S. Types of Indwelling Urethral Catheters for Short-Term Catheterisation in Hospitalised Adults. Cochrane Database Syst. Rev. 2014, 9, CD004013. [Google Scholar] [CrossRef] [PubMed]
- Pickard, R.; Lam, T.; MacLennan, G.; Starr, K.; Kilonzo, M.; McPherson, G.; Gillies, K.; McDonald, A.; Walton, K.; Buckley, B.; et al. Antimicrobial Catheters for Reduction of Symptomatic Urinary Tract Infection in Adults Requiring Short-Term Catheterisation in Hospital: A Multicentre Randomised Controlled Trial. Lancet 2012, 380, 1927–1935. [Google Scholar] [CrossRef]
- Higgins, J.P.; Eldridge, S.; Tianjing, L. How to Include Multiple Groups from One Study. Available online: https://training.cochrane.org/handbook/current/chapter-23#section-23-3 (accessed on 15 May 2022).
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Akcam, F.Z.; Kaya, O.; Temel, E.N.; Buyuktuna, S.A.; Unal, O.; Yurekli, V.A. An Investigation of the Effectiveness against Bacteriuria of Silver-Coated Catheters in Short-Term Urinary Catheter Applications: A Randomized Controlled Study. J. Infect. Chemother. 2019, 25, 797–800. [Google Scholar] [CrossRef]
- Menezes, F.G.; Corrêa, L.; Medina-Pestana, J.O.; Aguiar, W.F.; Camargo, L.F.A. A Randomized Clinical Trial Comparing Nitrofurazone-Coated and Uncoated Urinary Catheters in Kidney Transplant Recipients: Results from a Pilot Study. Transpl. Infect. Dis. 2019, 21, e13031. [Google Scholar] [CrossRef] [PubMed]
- Karchmer, T.B.; Giannetta, E.T.; Muto, C.A.; Strain, B.A.; Farr, B.M. A Randomized Crossover Study of Silver-Coated Urinary Catheters in Hospitalized Patients. Arch. Intern. Med. 2000, 160, 3294–3298. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.R.; Roberts, P.L.; Olsen, R.J.; Moyer, K.A.; Stamm, W.E. Prevention of Catheter-Associated Urinary Tract Infection with a Silver Oxide-Coated Urinary Catheter: Clinical and Microbiologic Correlates. J. Infect. Dis. 1990, 162, 1145–1150. [Google Scholar] [CrossRef] [PubMed]
- Stenzelius, K.; Persson, S.; Olsson, U.-B.; Stjärneblad, M. Noble Metal Alloy-Coated Latex versus Silicone Foley Catheter in Short-Term Catheterization: A Randomized Controlled Study. Scand. J. Urol. Nephrol. 2011, 45, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Stensballe, J.; Tvede, M.; Looms, D.; Lippert, F.K.; Dahl, B.; Tønnesen, E.; Rasmussen, L.S. Infection Risk with Nitrofurazone-Impregnated Urinary Catheters in Trauma Patients: A Randomized Trial. Ann. Intern. Med. 2007, 147, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Erickson, B.A.; Navai, N.; Patil, M.; Chang, A.; Gonzalez, C.M. A Prospective, Randomized Trial Evaluating the Use of Hydrogel Coated Latex versus All Silicone Urethral Catheters after Urethral Reconstructive Surgery. J. Urol. 2008, 179, 203–206. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-J.; Kim, S.W.; Cho, Y.-H.; Shin, W.-S.; Lee, S.E.; Kim, C.-S.; Hong, S.J.; Chung, B.H.; Kim, J.J.; Yoon, M.S. A Comparative Multicentre Study on the Incidence of Catheter-Associated Urinary Tract Infection between Nitrofurazone-Coated and Silicone Catheters. Int. J. Antimicrob. Agents 2004, 24 (Suppl. S1), S65–S659. [Google Scholar] [CrossRef]
- Bonfill, X.; Rigau, D.; Esteban-Fuertes, M.; Barrera-Chacón, J.M.; Jáuregui-Abrisqueta, M.L.; Salvador, S.; Alemán-Sánchez, C.M.; Borau, A.; Bea-Muñoz, M.; Hidalgo, B.; et al. Efficacy and Safety of Urinary Catheters with Silver Alloy Coating in Patients with Spinal Cord Injury: A Multicentric Pragmatic Randomized Controlled Trial. The ESCALE Trial. Spine J. 2017, 17, 1650–1657. [Google Scholar] [CrossRef]
- Thibon, P.; Le Coutour, X.; Leroyer, R.; Fabry, J. Randomized Multi-Centre Trial of the Effects of a Catheter Coated with Hydrogel and Silver Salts on the Incidence of Hospital-Acquired Urinary Tract Infections. J. Hosp. Infect. 2000, 45, 117–124. [Google Scholar] [CrossRef]
- Tae, B.S.; Oh, J.J.; Jeong, B.C.; Ku, J.H. Catheter-Associated Urinary Tract Infections in Patients Who Have Undergone Radical Cystectomy for Bladder Cancer: A Prospective Randomized Clinical Study of Two Silicone Catheters (Clinical Benefit of Antibiotic Silicone Material). Investig. Clin. Urol. 2022, 63, 334–340. [Google Scholar] [CrossRef] [PubMed]
- Akiyama, H.; Okamoto, S. Prophylaxis of Indwelling Urethral Catheter Infection: Clinical Experience with a Modified Foley Catheter and Drainage System. J. Urol. 1979, 121, 40–42. [Google Scholar] [CrossRef]
- Liedberg, H.; Lundeberg, T. Silver Alloy Coated Catheters Reduce Catheter-Associated Bacteriuria. Br. J. Urol. 1990, 65, 379–381. [Google Scholar] [CrossRef]
- Liedberg, H.; Lundeberg, T.; Ekman, P. Refinements in the Coating of Urethral Catheters Reduces the Incidence of Catheter-Associated Bacteriuria. An Experimental and Clinical Study. Eur. Urol. 1990, 17, 236–240. [Google Scholar] [CrossRef] [PubMed]
- Cooper, F.P.M.; Alexander, C.E.; Sinha, S.; Omar, M.I. Policies for Replacing Long-Term Indwelling Urinary Catheters in Adults. Cochrane Database Syst. Rev. 2016, 7, CD011115. [Google Scholar] [CrossRef] [PubMed]
- Priefer, B.A.; Duthie, E.H.J.; Gambert, S.R. Frequency of Urinary Catheter Change and Clinical Urinary Tract Infection. Study in Hospital-Based, Skilled Nursing Home. Urology 1982, 20, 141–142. [Google Scholar] [CrossRef]
- White, M.C.; Ragland, K.E. Urinary Catheter-Related Infections among Home Care Patients. J. Wound Ostomy Cont. Nurs. 1995, 22, 286–290. [Google Scholar] [CrossRef] [PubMed]
- Bologna, R.A.; Tu, L.M.; Polansky, M.; Fraimow, H.D.; Gordon, D.A.; Whitmore, K.E. Hydrogel/Silver Ion-Coated Urinary Catheter Reduces Nosocomial Urinary Tract Infection Rates in Intensive Care Unit Patients: A Multicenter Study. Urology 1999, 54, 982–987. [Google Scholar] [CrossRef]
- Chung, P.H.; Wong, C.W.; Lai, C.K.; Siu, H.K.; Tsang, D.N.; Yeung, K.Y.; Ip, D.K.; Tam, P.K. A Prospective Interventional Study to Examine the Effect of a Silver Alloy and Hydrogel-Coated Catheter on the Incidence of Catheter-Associated Urinary Tract Infection. Hong Kong Med. J. 2017, 23, 239–245. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Srinivasan, A.; Karchmer, T.; Richards, A.; Song, X.; Perl, T.M. A Prospective Trial of a Novel, Silicone-Based, Silver-Coated Foley Catheter for the Prevention of Nosocomial Urinary Tract Infections. Infect. Control Hosp. Epidemiol. 2006, 27, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Pickard, R.; Lam, T.; Maclennan, G.; Starr, K.; Kilonzo, M.; McPherson, G.; Gillies, K.; McDonald, A.; Walton, K.; Buckley, B.; et al. Types of Urethral Catheter for Reducing Symptomatic Urinary Tract Infections in Hospitalised Adults Requiring Short-Term Catheterisation: Multicentre Randomised Controlled Trial and Economic Evaluation of Antimicrobial- and Antiseptic-Impregnated Urethra. Health Technol. Assess. 2012, 16, 1–197. [Google Scholar] [CrossRef] [PubMed]
- Kinnear, N.; Barnett, D.; O’Callaghan, M.; Horsell, K.; Gani, J.; Hennessey, D. The Impact of Catheter-Based Bladder Drainage Method on Urinary Tract Infection Risk in Spinal Cord Injury and Neurogenic Bladder: A Systematic Review. Neurourol. Urodyn. 2020, 39, 854–862. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria | Length of Follow Up | Type of Coated Catheter | Number of Patients Included in Coated Catheter | Mean Age (Standard Deviation) in Coated Group | Type of Non-Coated Catheter | Number of Patients Included in Non-Coated Catheter | Mean Age (Standard Deviation) in Non-Coated Group | Catheter Duration (Days) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Akcam 2019 [10] | Patients admitted to the intensive care unit and anticipated to require long-term urinary catheterization | Patients with any infectious disease on admission or with pyuria/bacteriuria in the first urine specimen collected following catheter placement | Until discharge of patients | Silver-coated silicone catheters | 28 | 70.61 (NA) | silicone catheters | 26 | 69.23 (NA) | NA |
| Bonfill 2017 [18] | Patients with traumatic or medical SCI requiring an indwelling urinary catheter for at least 7 days | Patients with demonstrable UTI at the time of inclusion; taking antibiotic treatment at the time of inclusion for any infectious condition or within 7 days before inclusion | 12 months | Silver alloy catheters | 243 | 55.30 (16.35) | silicone catheters | 246 | 57.25 (16.32) | 27 in coated 28 in non-coated |
| Erickson 2008 [16] | Men undergoing urethral reconstruction | None | 20 months | Hydrogel-coated latex foley | 42 | 40 (NA) | silicone catheters | 43 | 43 (NA) | 14–21 |
| Johnson 1990 [13] | Patients with a steady catheter that was expected to remain indwelling for at least 24 h | UTI at enrollment | 16 months | Silicone catheter coated with a layer of silicone elastomer containing micronized silver oxide | 207 | 50 (NA) | silicone catheters | 208 | 47 (NA) | 3 in coated 4 in non-coated |
| Karchmer 2000 [12] | Hospitalized patients with vesical catheters | Pediatric, obstetrics, gynecology, and psychiatry wards excluded | 12 months | Silver-alloy, hydrogel-coated latex catheters | 13,945 | NA | silicone catheters | 13,933 | NA | >7 days |
| Lee 2004 [17] | Patients who were catheterized for more than 24 h | conditions such as silicone sensitivity, nitrofurazone or nitrofurantoin sensitivity, pregnancy, lactating, hospitalization for more than 7 days, and having urinary diseases; positive urine culture result before catheter insertion or when the catheter was removed within 24 h of insertion | 7 days | Release nitrofurazone foley catheter | 92 | 55.3 | silicone catheters | 85 | 54.1 | 3.9–4.4 |
| Menezes 2019 [11] | urethral catheterization for kidney transplantation with a living donor | asymptomatic bacteriuria or urinary tract infection at baseline, deceased kidney transplant donors, hypersensitivity to nitrofurantoin, pregnancy | 22 months | Nitrofural-impregnated silicone catheter | 88 | 38.4 (NA) | silicone catheters | 88 | 39.6 (NA) | 5.1 |
| Pickard 2012 [7] | Adults undergoing urethral catheterization for an anticipated duration of up to 14 days (including people with diabetes and individuals treated with immunosuppressive drugs) | Symptomatic urinary tract infection at baseline, urological procedures in the previous 7 days, or allergies to catheter materials | 39 months | (1) Silver alloy-coated latex catheter (2) Nitrofural-impregnated silicone catheter | (1) 2097 (2) 2153 | (1) 59 (16) (2) 59 (16) | standard polytetrafluoroethylene (PTFE)-coated latex catheter | 2144 | 59 (16) | 2 (1–3) |
| Stensballe 2007 [15] | trauma patients who needed a urinary catheter and were admitted directly from the accident scene to the Trauma Center | HIV infection; preinjury treatment with corticosteroids; pregnancy; primary burn injury; and unattainable signed informed consent | 24 months | Nitrofurazone-impregnated catheter | 106 | 41 (NA) | silicone catheters | 106 | 43 (NA) | 2 (0–7) |
| Stenzelius 2011 [14] | patients undergoing elective orthopedic surgery | recent (within 3 weeks) use of a urinary catheter or a recent history of UTI, previous radiation therapy over the lower pelvis, latex allergy, cognitive impairment, or difficulties in understanding the Swedish language | 2–7 days | Noble metal alloy-coated latex catheter | 222 | 67.6 (12) | silicone catheters | 217 | 66.7 (12.8) | 2 |
| Tae 2022 [20] | Patients underwent radical cystectomy with neobladder cause of invasive bladder cancer | Malnutrition, active infection, immunodeficiency, allergy to components | NA | Carbon nanotube and ZnO-bonded CNT | 41 | 65.22 (10.25) | silicone catheters | 44 | 65.36 (8.56) | 14 + or − 1 |
| Thibon 2000 [19] | Patients in neurosurgery ICU required catheter during admission for more than three days and had to stay in hospital for at least10 days after the insertion of a urinary catheter | urinary tract infection or inflammation of the perineum or penis before catheter insertion, allergy to hydrogel or silver salts, contraindications for catheterization, urinary tract catheter insertion during the 48 h before inclusion, antibiotic treatment for urinary tractinfection and other types of urinary tract intervention (prostate, bladder) | 24 months | Hydrogel and silver salt-coated catheter | 90 | 59.8 (17.1) | silicone catheters | 109 | 60.5 (15.5) | 10 |
| Pathogen Species in Urine Culture | Difference in Urine Culture between Coated and Non-Coated Catheters | |
|---|---|---|
| Akcam 2019 [10] | The most commonly detected agent, at 11/25 (44%), was Escherichia coli (44%), Enterococcus spp. (20%), Klebsiella pneumonia (8%), Pseudomonas spp. (8%), Acinetobacter spp. (8%), Enterobacter cloacae (4%), Proteus mirabilis (4%) and Candida spp. (4%). Second species were grown in four of the specimens: Enterococcus spp. was isolated in three specimens, and E. cloacae in one | E. coli grew in 26.9% and microorganisms other than E. coli in 19.3% of the subjects using normal catheters, while E. coli grew in 14.3% and other microorganisms in 32.1% of the patients using silver-coated catheters |
| Bonfill 2017 [18] | Not reported in full | One patient, pertaining to the group with SAC urinary catheter, developed a urinary septic shock caused by Proteus mirabilis. Another patient, pertaining to the group of standard urinary catheter, developed a urinary sepsis caused by Escherichia coli and P. mirabilis |
| Erickson 2008 [16] | Not reported | Not reported |
| Johnson 1990 [13] | Coagulase-negative staphylococci, Enterococcus species, Escherichia coli, Proteus mirabilis, Pseudomonas species, Yeast other | No difference |
| Karchmer 2000 [12] | Escherichia coli (18.4%), Escherichia faecalis (16.9%), Candida albicans (13.4%), and Pseudomonas aeruginosa (11.7%), Yeast (26.2%), Gram-positive cocci, including Staphylococcus aureus, coagulase-negative staphylococci, and enterococci (28%) | There were no statistically significant differences in the proportion of infections attributed to different organisms following use of silver-coated and uncoated catheters |
| Lee 2004 [17] | Enterococcus species (22.5%), Staphylococcus (15%), Pseudomonas species (30%), StenotrophomonasMaltophilia (10%), others (Acinetobacter calcoaceticus–baumannii complex, A. lwoffi, Citrobacter freundii, Enterobacter cloacae, Nonfermenting Gram-negative Bacillus, Pasteurella multocida, Burkholderia cepacia, B. pseudomallei, Chryseobacterium meningosepticum 15%). Mixed infection was observed in five patients | StenotrophomonasMaltophilia was not isolated in patients with non-coated catheters |
| Menezes 2019 [11] | Gram-negative bacilli (95.24%) and Escherichia coli was the most frequently isolated microorganism (47.62%). Among the isolates of E coli and Klebsiella pneumoniae, 25% had an extended spectrum beta-lactamase producing profile, and 12.5% of the K pneumonie strains were carbapenem resistant | No evidence of enhanced antimicrobial resistance with the employment of the Nitrofurazone-coated urinary catheter |
| Pickard 2012 [7] | Not reported | Not reported |
| Stensballe 2007 [15] | Enterococcus species, Escherichia coli, Candida species, Coagulase-negative staphylococci, Corynebacterium species, Pseudomonas aeruginosa, polymicrobial | Nitrofurantoin resistance was found in 3 isolates in the nitrofurazone group (1 with Pseudomonas aeruginosa and 2 with Candida species) compared with 7 in the silicone group (1 with Enterobacter species, 5 with Candida species, and 1 with Enterobacter species and Candida species) |
| Stenzelius 2011 [14] | Not reported | Not reported |
| Tae 2022 [20] | Enterococcus faecalis, Pseudomonas aeruginosa, Yeast, Streptococcus species, Klebsiella pneumoniae, methicillin-resistant Staphylococcus aureus | Coated: 19 positive cultures. Non-coated: 22 positive cultures Enterococcus faecalis: coated 8; non-coated 11 Pseudomonas aeruginosa: coated 4; non-coated 4 Yeast: coated 3; non-coated 2 Streptococcus species: coated 2; non-coated 4 Klebsiella pneumoniae: coated 1; non-coated 2 methicillin-resistant Staphylococcus aureus: coated 1; non-coated 1 |
| Thibon 2000 [19] | Escherichia coli, Proteus, Pseudomonas, Enterobacter cloacae, Yeasts, coagulase negative staphylococci, enterococci, others | There was no significant difference between the types of organism identified with the two types of catheter |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gauhar, V.; Castellani, D.; Teoh, J.Y.-C.; Nedbal, C.; Chiacchio, G.; Gabrielson, A.T.; Heldwein, F.L.; Wroclawski, M.L.; de la Rosette, J.; Donalisio da Silva, R.; et al. Catheter-Associated Urinary Infections and Consequences of Using Coated versus Non-Coated Urethral Catheters—Outcomes of a Systematic Review and Meta-Analysis of Randomized Trials. J. Clin. Med. 2022, 11, 4463. https://doi.org/10.3390/jcm11154463
Gauhar V, Castellani D, Teoh JY-C, Nedbal C, Chiacchio G, Gabrielson AT, Heldwein FL, Wroclawski ML, de la Rosette J, Donalisio da Silva R, et al. Catheter-Associated Urinary Infections and Consequences of Using Coated versus Non-Coated Urethral Catheters—Outcomes of a Systematic Review and Meta-Analysis of Randomized Trials. Journal of Clinical Medicine. 2022; 11(15):4463. https://doi.org/10.3390/jcm11154463
Chicago/Turabian StyleGauhar, Vineet, Daniele Castellani, Jeremy Yuen-Chun Teoh, Carlotta Nedbal, Giuseppe Chiacchio, Andrew T. Gabrielson, Flavio Lobo Heldwein, Marcelo Langer Wroclawski, Jean de la Rosette, Rodrigo Donalisio da Silva, and et al. 2022. "Catheter-Associated Urinary Infections and Consequences of Using Coated versus Non-Coated Urethral Catheters—Outcomes of a Systematic Review and Meta-Analysis of Randomized Trials" Journal of Clinical Medicine 11, no. 15: 4463. https://doi.org/10.3390/jcm11154463
APA StyleGauhar, V., Castellani, D., Teoh, J. Y.-C., Nedbal, C., Chiacchio, G., Gabrielson, A. T., Heldwein, F. L., Wroclawski, M. L., de la Rosette, J., Donalisio da Silva, R., Galosi, A. B., & Somani, B. K. (2022). Catheter-Associated Urinary Infections and Consequences of Using Coated versus Non-Coated Urethral Catheters—Outcomes of a Systematic Review and Meta-Analysis of Randomized Trials. Journal of Clinical Medicine, 11(15), 4463. https://doi.org/10.3390/jcm11154463