
Autoimmune Disease Classification Based on PubMed Text Mining

 , and
, and 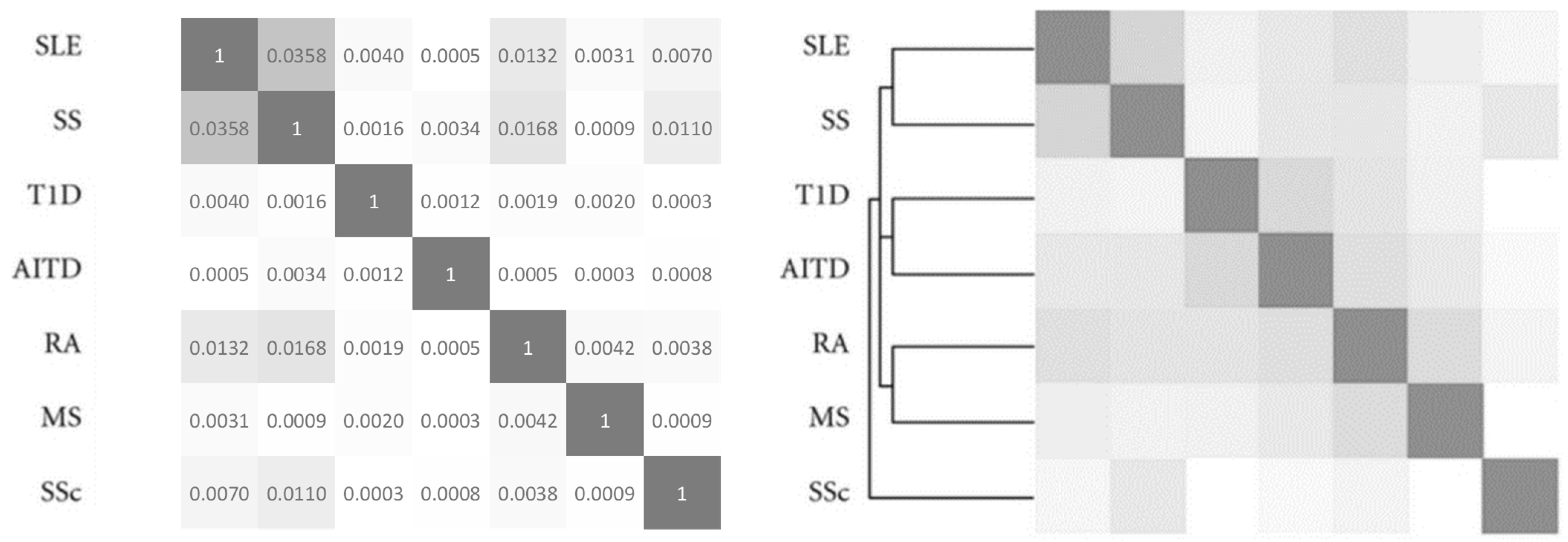{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
2.1. PubMed Count
2.2. List of Autoimmune Diseases
2.3. Clustering
3. Results and Discussion
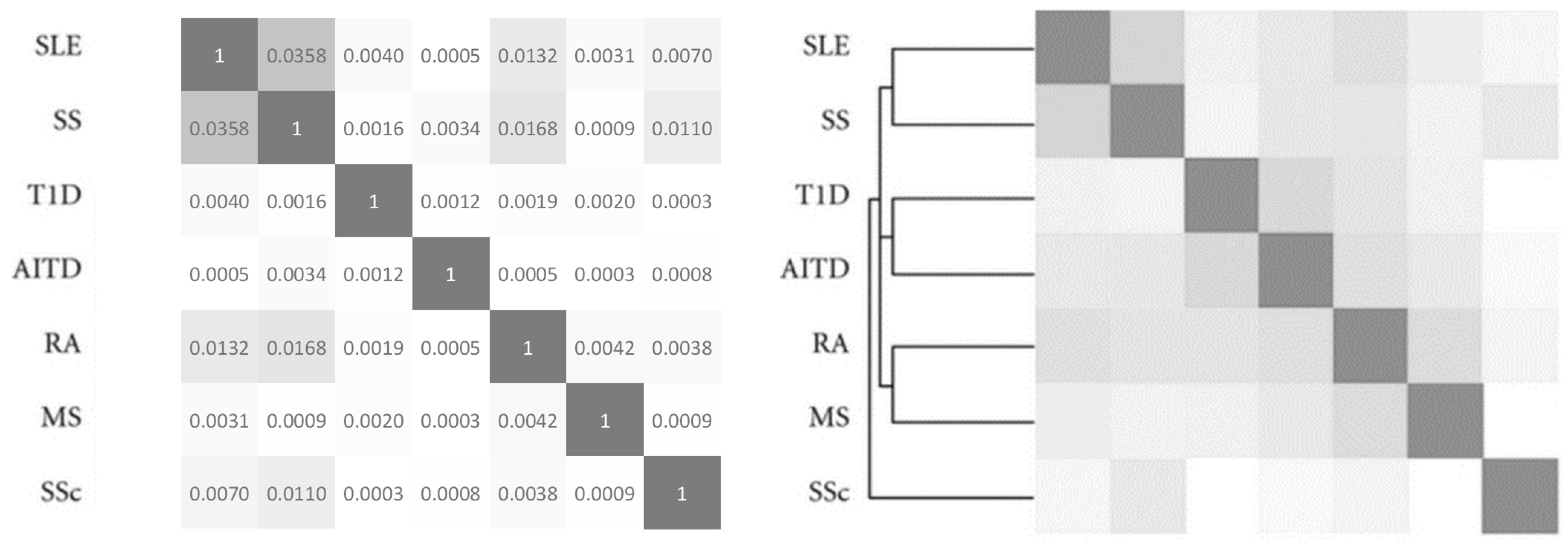
3.1. Validation
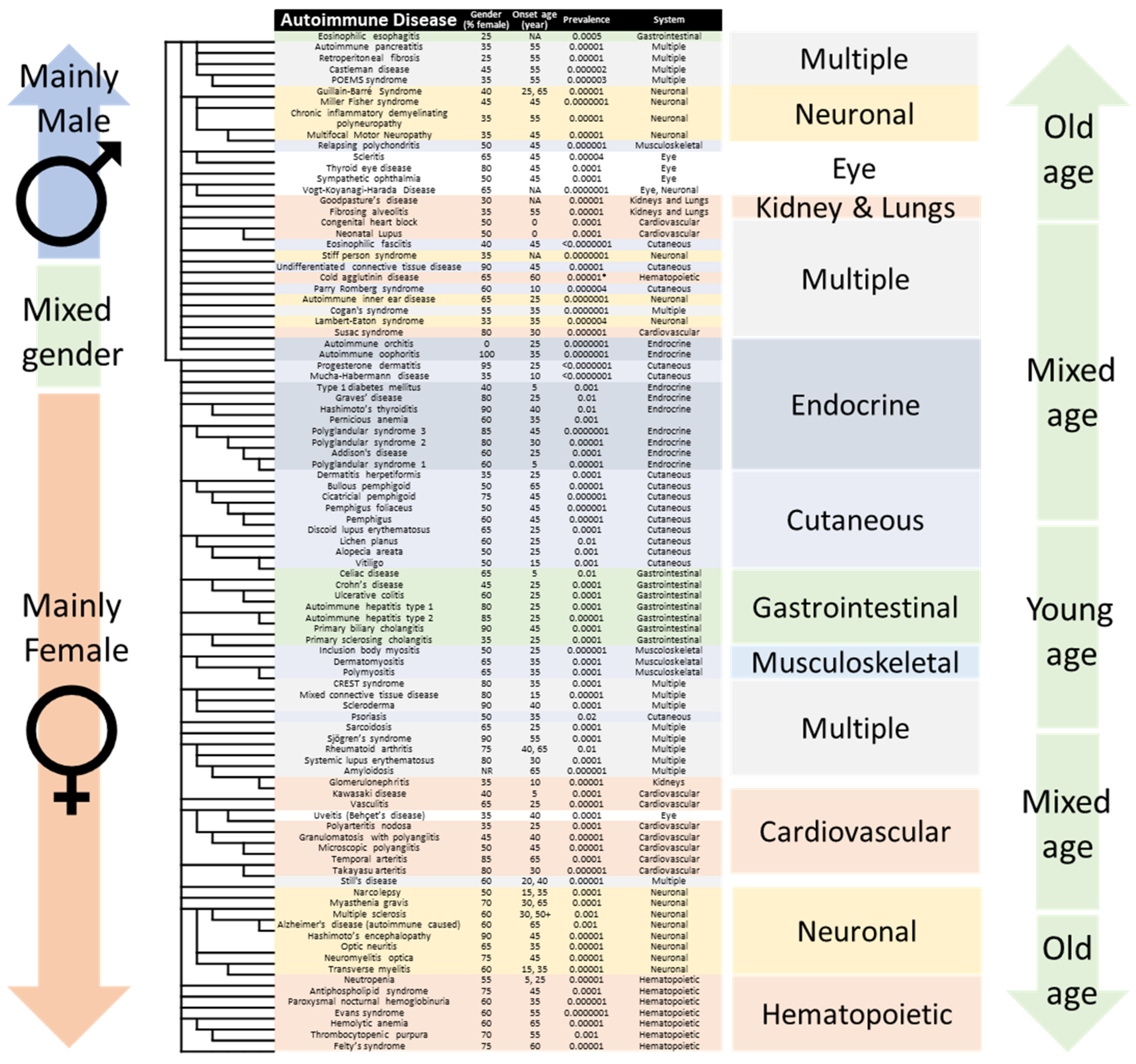
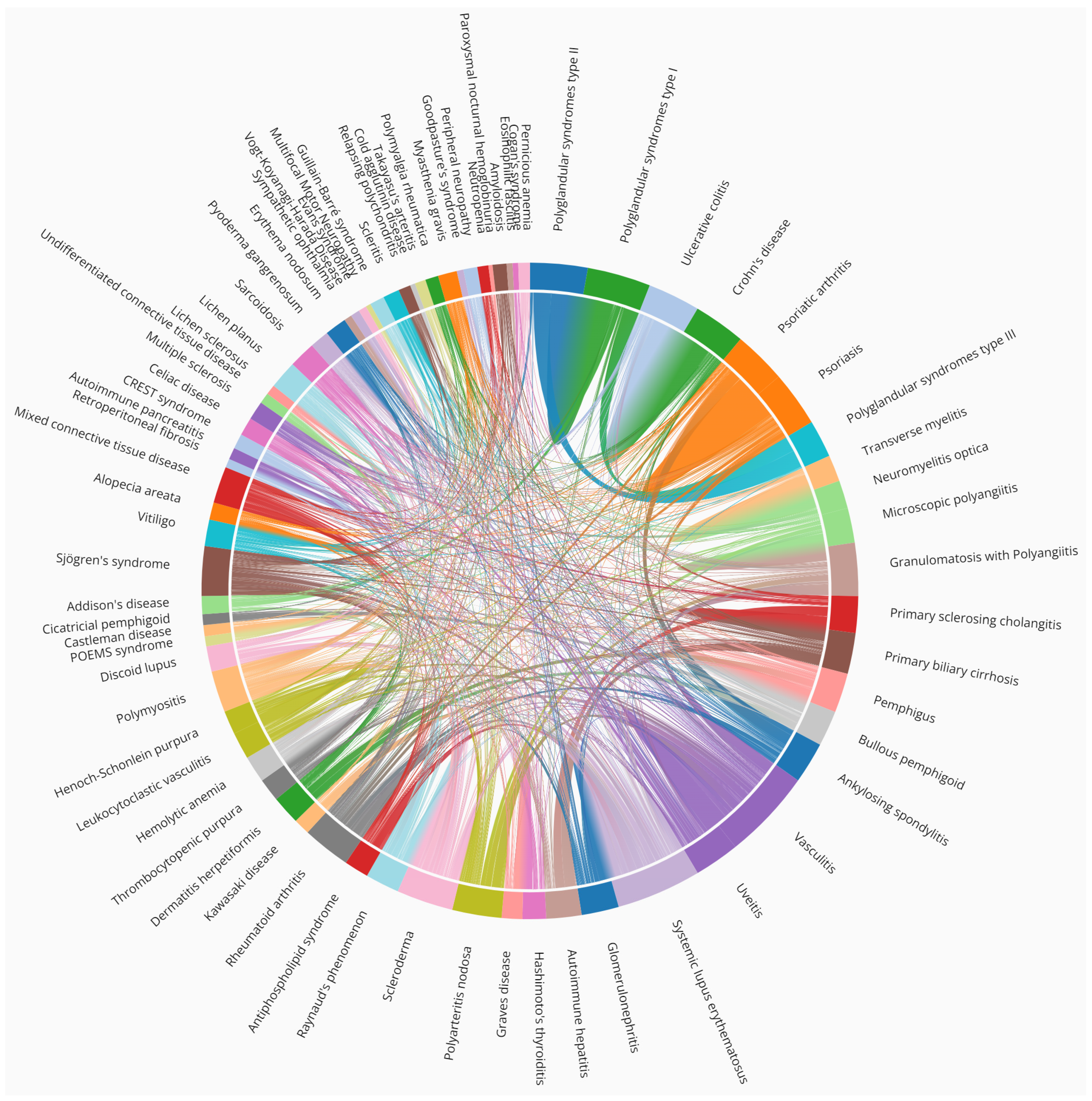
3.2. Association of Autoimmune Diseases
3.3. Misfit AIDs
3.4. Pathogen-Induced Diseases
3.5. Tumor-Induced Diseases
3.6. Toxicity-Induced Diseases
3.7. Injury-Induced Diseases
3.8. Alzheimer’s Disease Spectrum Includes Autoimmunization
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
References
- Wang, L.; Wang, F.-S.; Gershwin, M.E. Human autoimmune diseases: A comprehensive update. J. Intern. Med. 2015, 278, 369–395. [Google Scholar] [CrossRef]
- Matzinger, P. Tolerance, Danger, and the Extended Family. Ann. Rev. Immunol. 1994, 12, 991–1045. [Google Scholar] [CrossRef]
- Cifuentes, R.A.; Restrepo-Montoya, D.; Anaya, J.-M. The Autoimmune Tautology: An In Silico Approach. Autoimmune Dis. 2012, 2012, 792106. [Google Scholar] [CrossRef] [Green Version]
- Mitratza, M.; Klijs, B.; Hak, A.E.; Kardaun, J.W.P.F.; Kunst, A.E. Systemic autoimmune disease as a cause of death: Mortality burden and comorbidities. Rheumatology 2021, 60, 1321–1330. [Google Scholar] [CrossRef]
- Eaton, W.W.; Rose, N.R.; Kalaydjian, A.; Pedersen, M.G.; Mortensen, P.B. Epidemiology of autoimmune diseases in Denmark. J. Autoimmun. 2017, 29, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sardu, C.; Cocco, E.; Mereu, A.; Massa, R.; Cuccu, A.; Marrosu, M.G.; Contu, P. Population Based Study of 12 Autoimmune Diseases in Sardinia, Italy: Prevalence and Comorbidity. PLoS ONE 2012, 7, e32487. [Google Scholar] [CrossRef] [Green Version]
- Turner, M.R.; Goldacre, R.; Ramagopalan, S.; Talbot, K.; Goldacre, M.J. Autoimmune disease preceding amyotrophic lateral sclerosis: An epidemiologic study. Neurology 2013, 81, 1222–1225. [Google Scholar] [CrossRef] [Green Version]
- Hayter, S.M.; Cook, M.C. Updated assessment of the prevalence, spectrum and case definition of autoimmune disease. Autoimmun. Rev. 2012, 11, 754–765. [Google Scholar] [CrossRef] [PubMed]
- McGonagle, D.; McDermott, M.F. A Proposed Classification of the Immunological Diseases. PLoS Med. 2006, 3, e297. [Google Scholar] [CrossRef] [Green Version]
- Rose, N.R.; Bona, C. Defining criteria for autoimmune diseases (Witebsky’s postulates revisited). Immunol. Today 1993, 14, 426–430. [Google Scholar] [CrossRef]
- Sirota, M.; Schaub, M.A.; Batzoglou, S.; Robinson, W.H.; Butte, A.J. Autoimmune Disease Classification by Inverse Association with SNP Alleles. PLoS Genet. 2009, 5, e1000792. [Google Scholar] [CrossRef] [Green Version]
- Miller, F.W.; Pollard, K.M.; Parks, C.G.; Germolec, D.R.; Leung, P.S.C.; Selmi, C.; Humble, M.C.; Rose, N.R. Criteria for environmentally associated autoimmune diseases. J. Autoimmun. 2012, 39, 253–258. [Google Scholar] [CrossRef] [Green Version]
- Stafford, I.S.; Kellermann, M.; Mossotto, E.; Beattie, R.M.; MacArthur, B.D.; Ennis, S. A systematic review of the applications of artificial intelligence and machine learning in autoimmune diseases. NPJ Digit. Med. 2020, 3, 30. [Google Scholar] [CrossRef]
- Zhou, J.; Fu, B. The research on gene-disease association based on text-mining of PubMed. BMC Bioinform. 2018, 19, 37. [Google Scholar] [CrossRef]
- Kuhn, M.; Campillos, M.; Letunic, I.; Jensen, L.J.; Bork, P. A side effect resource to capture phenotypic effects of drugs. Mol. Syst. Biol. 2010, 6, 343. [Google Scholar] [CrossRef]
- Pletscher-Frankild, S.; Pallejà, A.; Tsafou, K.; Binder, J.X.; Jensen, L.J. DISEASES: Text mining and data integration of disease–gene associations. Methods 2015, 74, 83–89. [Google Scholar] [CrossRef]
- Dabour, R.; Meirson, T.; Samson, A.O. Global antibiotic resistance is mostly periodic. J. Glob. Antimicrob. Resist. 2016, 7, 132–134. [Google Scholar] [CrossRef]
- Weitzman, R.; Calfon-Peretz, O.; Saha, T.; Bloch, N.; Ben Zaken, K.; Rosenfeld, A.; Amitay, M.; Samson, A.O. Resistance to Antimalarial Monotherapy Is Cyclic. J. Clin. Med. 2022, 11, 781. [Google Scholar] [CrossRef]
- Avitan, I.; Halperin, Y.; Saha, T.; Bloch, N.; Atrahimovich, D.; Polis, B.; Samson, A.O.; Braitbard, O. Towards a Consensus on Alzheimer’s Disease Comorbidity? J. Clin. Med. 2021, 10, 4360. [Google Scholar] [CrossRef]
- Metsalu, T.; Vilo, J. ClustVis: A web tool for visualizing clustering of multivariate data using Principal Component Analysis and heatmap. Nucleic Acids Res. 2015, 43, W566–W570. [Google Scholar] [CrossRef]
- Bender, M.; Christiansen, J.; Quick, M. Autoimmune Disease, by the Numbers. Sci. Am. 2021, 325, 31–33. [Google Scholar]
- Krzywinski, M.; Schein, J.; Birol, İ.; Connors, J.; Gascoyne, R.; Horsman, D.; Jones, S.J.; Marra, M.A. Circos: An information aesthetic for comparative genomics. Genome Res. 2009, 19, 1639–1645. [Google Scholar] [CrossRef] [Green Version]
- Nurko, S.; Rosen, R.; Furuta, G.T. Esophageal Dysmotility in Children with Eosinophilic Esophagitis. Am. J. Gastroenterol. 2009, 104, 3050–3057. [Google Scholar] [CrossRef]
- Blanchard, C.; Rothenberg, M.E. Basic Pathogenesis of Eosinophilic Esophagitis. Gastrointest. Endosc. Clin. N. Am. 2008, 18, 133–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Runowska, M.; Majewski, D.; Puszczewicz, M. Retroperitoneal fibrosis—The state-of-the-art. Rheumatology 2016, 5, 256–263. [Google Scholar] [CrossRef] [PubMed]
- Ulas, S.T.; Dasdelen, S. Multizentrische Castleman-Erkrankung in Kombination mit Polyserositis und POEMS-Syndrom—Fallbericht und Übersichtsbeitrag. Internist 2021, 62, 777–785. [Google Scholar] [CrossRef]
- Florian, I.A.; Lupan, I.; Sur, L.; Samasca, G.; Timiș, T.L. To be, or not to be… Guillain-Barré Syndrome. Autoimmun. Rev. 2021, 20, 102983. [Google Scholar] [CrossRef]
- Köller, H.; Kieseier, B.C.; Jander, S.; Hartung, H.-P. Chronic Inflammatory Demyelinating Polyneuropathy. N. Engl. J. Med. 2005, 352, 1343–1356. [Google Scholar] [CrossRef] [Green Version]
- López-Medina, C.; Molto, A.; Sieper, J.; Duruöz, T.; Kiltz, U.; Elzorkany, B.; Hajjaj-Hassouni, N.; Burgos-Vargas, R.; Maldonado-Cocco, J.; Ziade, N.; et al. Prevalence and distribution of peripheral musculoskeletal manifestations in spondyloarthritis including psoriatic arthritis: Results of the worldwide, cross-sectional ASAS-PerSpA study. RMD Open 2021, 7, e001450. [Google Scholar] [CrossRef]
- Fukuda, K.; Mizobuchi, T.; Nakajima, I.; Kishimoto, T.; Miura, Y.; Taniguchi, Y. Ocular Involvement in Relapsing Polychondritis. J. Clin. Med. 2021, 10, 4970. [Google Scholar] [CrossRef]
- Meel, R.; Das, D.; Bhadu, D.; Sen, S.; Kishor, K.; Pushker, N. Bilateral Nodular Episcleritis: A Rare Presentation of Relapsing Polychondritis. Ophthalmic Plast. Reconstr. Surg. 2021, 37, e103–e105. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Chan, C.-C. Gender Differences in Vogt-Koyanagi-Harada Disease and Sympathetic Ophthalmia. J. Ophthalmol. 2014, 2014, 157803. [Google Scholar] [CrossRef] [Green Version]
- Pedchenko, V.; Kitching, A.R.; Hudson, B.G. Goodpasture’s autoimmune disease—A collagen IV disorder. Matrix Biol. 2018, 71, 240–249. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, L. Congenital Heart Block. Card. Electrophysiol. Clin. 2021, 13, 691–702. [Google Scholar] [CrossRef]
- Marijianowski, M.M.H.; van der Loos, C.M.; Mohrschladt, M.F.; Becker, A.E. The neonatal heart has a relatively high content of total collagen and type I collagen, a condition that may explain the less compliant state. J. Am. Coll. Cardiol. 1994, 23, 1204–1208. [Google Scholar] [CrossRef] [Green Version]
- Friedman, D.M.; Rupel, A.; Glickstein, J.; Buyon, J.P. Congenital heart block in neonatal lupus: The pediatric cardiologist’s perspective. Indian J. Pediatr. 2002, 69, 517–522. [Google Scholar] [CrossRef]
- Liao, H.; Tang, C.; Qiao, L.; Zhou, K.; Hua, Y.; Wang, C.; Li, Y. Prenatal Management Strategy for Immune-Associated Congenital Heart Block in Fetuses. Front. Cardiovasc. Med. 2021, 8, 644122. [Google Scholar] [CrossRef]
- Ihn, H. Eosinophilic fasciitis: From pathophysiology to treatment. Allergol. Int. 2019, 68, 437–439. [Google Scholar] [CrossRef]
- Sciascia, S.; Roccatello, D.; Radin, M.; Parodis, I.; Yazdany, J.; Pons-Estel, G.; Mosca, M. Differentiating between UCTD and early-stage SLE: From definitions to clinical approach. Nat. Rev. Rheumatol. 2022, 18, 9–21. [Google Scholar] [CrossRef]
- Hansen, O.P.; Sørensen, C.H.; Astrup, L. Evans’ Syndrome in IgA Deficiency Episodic Autoimmune Haemolytic Anaemia and Thrombocytopenia during a 10 Years Observation Period. Scand. J. Haematol. 2009, 29, 265–270. [Google Scholar] [CrossRef]
- Garcia-de la Torre, I.; Castello-Sendra, J.; Esgleyes-Ribot, T.; Martinez-Bonilla, G.; Guerrerosantos, J.; Fritzler, M.J. Autoantibodies in Parry-Romberg syndrome: A serologic study of 14 patients. J. Rheumatol. 1995, 22, 73–77. [Google Scholar]
- Shah, S.S.; Chhabra, M. Parry Romberg Syndrome. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Greco, A.; Gallo, A.; Fusconi, M.; Magliulo, G.; Turchetta, R.; Marinelli, C.; Macri, G.F.; de Virgilio, A.; de Vincentiis, M. Cogan’s syndrome: An autoimmune inner ear disease. Autoimmun. Rev. 2013, 12, 396–400. [Google Scholar] [CrossRef]
- Guidon, A.C. Lambert-Eaton Myasthenic Syndrome, Botulism, and Immune Checkpoint Inhibitor–Related Myasthenia Gravis. CONTIN. Lifelong Learn. Neurol. 2019, 25, 1785–1806. [Google Scholar] [CrossRef]
- Lee, J.D.; Woodruff, T.M. The emerging role of complement in neuromuscular disorders. Semin. Immunopathol. 2021, 43, 817–828. [Google Scholar] [CrossRef]
- Pereira, S.; Vieira, B.; Maio, T.; Moreira, J.; Sampaio, F. Susac’s Syndrome: An Updated Review. Neuro-Ophthalmology 2020, 44, 355–360. [Google Scholar] [PubMed]
- Tung, K. Mechanisms of autoimmune disease in the testis and ovary. Hum. Reprod. Update 1995, 1, 35–50. [Google Scholar] [CrossRef]
- Fernandes, N.F.; Rozdeba, P.J.; Schwartz, R.A.; Kihiczak, G.; Lambert, W.C. Pityriasis lichenoides et varioliformis acuta: A disease spectrum. Int. J. Dermatol. 2010, 49, 257–261. [Google Scholar] [CrossRef]
- Li, R.-C.; Buchheit, K.M.; Bernstein, J.A. Progestogen Hypersensitivity. Curr. Allergy Asthma Rep. 2018, 18, 1. [Google Scholar] [CrossRef]
- Dasari, S.; Naha, K.; Hande, M.; Vivek, G. Hot and cold: Coexistent Graves’ disease and Hashimoto’s thyroiditis in a patient with Schmidt’s syndrome. Case Rep. 2014, 2014, bcr2013010432. [Google Scholar]
- Htut, T.W.; Thein, K.Z.; Oo, T.H. Pernicious anemia: Pathophysiology and diagnostic difficulties. J. Evid.-Based Med. 2021, 14, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Perniola, R.; Fierabracci, A.; Falorni, A. Autoimmune Addison’s Disease as Part of the Autoimmune Polyglandular Syndrome Type 1: Historical Overview and Current Evidence. Front. Immunol. 2021, 12, 606860. [Google Scholar] [CrossRef] [PubMed]
- Pham-Dobor, G.; Hanák, L.; Hegyi, P.; Márta, K.; Párniczky, A.; Gergics, M.; Sarlós, P.; Erőss, B.; Mezősi, E. Prevalence of other autoimmune diseases in polyglandular autoimmune syndromes type II and III. J. Endocrinol. Investig. 2020, 43, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joly, P. Maladies bulleuses auto-immunes. Rev. Méd. Interne 1999, 20, 26–38. [Google Scholar] [CrossRef]
- Cifuentes-González, C.; Amaris-Martínez, S.; Reyes-Guanes, J.; Uribe-Reina, P.; de-la-Torre, A. Ocular Cicatricial Pemphigoid, Sjögren’s Syndrome, and Hashimoto’s Thyroiditis as a Multiple Autoimmune Syndrome: A case report. Eur. J. Ophthalmol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Bech, R.; Kibsgaard, L.; Vestergaard, C. Comorbidities and Treatment Strategies in Bullous Pemphigoid: An Appraisal of the Existing Litterature. Front. Med. 2018, 5, 238. [Google Scholar] [CrossRef]
- Tukenmez Demirci, G.; Altunay, I.K.; Sarikaya, S.; Sakiz, D. Lupus erythematosus and lichen planus overlap syndrome: A case report with a rapid response to topical corticosteroid therapy. Dermatol. Rep. 2011, 3, e48. [Google Scholar] [CrossRef]
- Marques, L.C.; Santos, L.R.; da Silva, N.C.; Cunha, K.S.; Junior, A.S.; Conde, D.C. Oral Lichen Planus Associated with Lichen Planus Pigmentosus and Lichen Sclerosus in Monozygotic Twins. Am. J. Dermatopathol. 2021, 43, 368–372. [Google Scholar] [CrossRef]
- Dahir, A.M.; Thomsen, S.F. Comorbidities in vitiligo: Comprehensive review. Int. J. Dermatol. 2018, 57, 1157–1164. [Google Scholar] [CrossRef]
- Suchonwanit, P.; Kositkuljorn, C.; Pomsoong, C. Alopecia Areata: An Autoimmune Disease of Multiple Players. ImmunoTarg. Ther. 2021, 10, 299–312. [Google Scholar] [CrossRef]
- Podolsky, D.K. Inflammatory Bowel Disease. N. Engl. J. Med. 2002, 347, 417–429. [Google Scholar] [CrossRef]
- Feakins, R.M. Ulcerative colitis or Crohn’s disease? Pitfalls and problems. Histopathology 2014, 64, 317–335. [Google Scholar] [CrossRef]
- Ayaki, M.; Manabe, N.; Fujita, M.; Katsumata, R.; Nakamura, J.; Kamada, T.; Murota, M.; Inoue, K.; Haruma, K. Prevalence of Autoimmune Disease in Patients with Eosinophilic Esophagitis: A Cross-Sectional Study of Three Hospitals in Japan. Intern. Med. 2021, 60, 7321–7389. [Google Scholar] [CrossRef] [PubMed]
- Pullen, R. A Clinical Review of Primary Biliary Cholangitis. Gastroenterol. Nurs. 2020, 43, E48–E55. [Google Scholar] [CrossRef] [PubMed]
- Dalakas, M.C.; Hohlfeld, R. Polymyositis and dermatomyositis. Lancet 2003, 362, 971–982. [Google Scholar] [CrossRef]
- Betteridge, Z.; McHugh, N. Myositis-specific autoantibodies: An important tool to support diagnosis of myositis. J. Intern. Med. 2016, 280, 8–23. [Google Scholar] [CrossRef]
- Adigun, R.; Goyal, A.; Bansal, P.; Hariz, A. Systemic Sclerosis; StatPearls Publishing: Tampa, FL, USA, 2021. [Google Scholar]
- Zheng, B.; Vincent, C.; Fritzler, M.J.; Senécal, J.-L.; Koenig, M.; Joyal, F. Prevalence of Systemic Sclerosis in Primary Biliary Cholangitis Using the New ACR/EULAR Classification Criteria. J. Rheumatol. 2017, 44, 33–39. [Google Scholar] [CrossRef]
- Gottlieb, A.B.; Merola, J.F. A clinical perspective on risk factors and signs of subclinical and early psoriatic arthritis among patients with psoriasis. J. Dermatol. Treat. 2021, 33, 1–9. [Google Scholar] [CrossRef]
- Song, M.; Manansala, M.; Parmar, P.J.; Ascoli, C.; Rubinstein, I.; Sweiss, N.J. Sarcoidosis and autoimmunity. Curr. Opin. Pulm. Med. 2021, 27, 448–454. [Google Scholar] [CrossRef]
- Seror, R.; Nocturne, G.; Mariette, X. Current and future therapies for primary Sjögren syndrome. Nat. Rev. Rheumatol. 2021, 17, 475–486. [Google Scholar] [CrossRef]
- Sokolova, M.V.; Schett, G.; Steffen, U. Autoantibodies in Rheumatoid Arthritis: Historical Background and Novel Findings. Clin. Rev. Allergy Immunol. 2021. [Google Scholar] [CrossRef]
- Frittoli, R.B.; Vivaldo, J.F.; Costallat, L.T.L.; Appenzeller, S. Gastrointestinal involvement in systemic lupus erythematosus: A systematic review. J. Transl. Autoimmun. 2021, 4, 100106. [Google Scholar] [CrossRef] [PubMed]
- Senthelal, S.; Li, J.; Goyal, A.; Bansal, P.; Thomas, M. Arthritis; StatPearls Publishing: Tampa, FL, USA, 2020. [Google Scholar]
- Ali, M.; Riad, M.; Adhikari, P.; Bhattarai, S.; Gupta, A.; Ali, E.; Mostafa, J.A. Association between Myasthenia Gravis and Systemic Lupus Erythematosus as a Comorbid State. Cureus 2021, 13, e14719. [Google Scholar] [CrossRef] [PubMed]
- McCarty-Farid, G.A. Antiphospholipid antibodies in systemic lupus erythematosus and Sjögren’s syndrome. Curr. Opin. Rheumatol. 1993, 5, 596–603. [Google Scholar] [CrossRef] [PubMed]
- Pillebout, E.; Sunderkötter, C. IgA vasculitis. Semin. Immunopathol. 2021, 43, 729–738. [Google Scholar] [CrossRef]
- Nussenblatt, R.B. Uveitis in Behçet’s Disease. Int. Rev. Immunol. 1997, 14, 67–79. [Google Scholar] [CrossRef]
- González-López, J.J.; García-Aparicio, Á.M.; Sánchez-Ponce, D.; Muñoz-Sanz, N.; Fernandez-Ledo, N.; Beneyto, P.; Westcott, M.C. Development and validation of a Bayesian network for the differential diagnosis of anterior uveitis. Eye 2016, 30, 865–872. [Google Scholar] [CrossRef] [Green Version]
- Sunderkötter, C.; Bonsmann, G.; Sindrilaru, A.; Luger, T. Management of leukocytoclastic vasculitis. J. Dermatol. Treat. 2005, 16, 193–206. [Google Scholar] [CrossRef]
- Gori, T. Coronary Vasculitis. Biomedicines 2021, 9, 622. [Google Scholar] [CrossRef]
- Leung, A.K.C.; Leong, K.F.; Lam, J.M. Erythema nodosum. World J. Pediatr. 2018, 14, 548–554. [Google Scholar] [CrossRef]
- Marzano, A.V.; Borghi, A.; Meroni, P.L.; Cugno, M. Pyoderma gangrenosum and its syndromic forms: Evidence for a link with autoinflammation. Br. J. Dermatol. 2016, 175, 882–891. [Google Scholar] [CrossRef] [Green Version]
- Plazzi, G.; Ferri, R.; Antelmi, E.; Bayard, S.; Franceschini, C.; Cosentino, F.I.I.; Abril, B.; Spruyt, K.; Provini, F.; Montagna, P.; et al. Restless Legs Syndrome is Frequent in Narcolepsy with Cataplexy Patients. Sleep 2010, 33, 689–694. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.J. Neuromuscular junction disorders beyond myasthenia gravis. Curr. Opin. Neurol. 2021, 34, 648–657. [Google Scholar] [CrossRef] [PubMed]
- Bachhuber, A. Entzündliche Erkrankungen des zentralen Nervensystems. Radiologe 2021, 61, 575–585. [Google Scholar] [CrossRef] [PubMed]
- Thvilum, M.; Brandt, F.; Lillevang-Johansen, M.; Folkestad, L.; Brix, T.H.; Hegedüs, L. Increased risk of dementia in hypothyroidism: A Danish nationwide register-based study. Clin. Endocrinol. 2021, 94, 1017–1024. [Google Scholar] [CrossRef]
- Nie, L.-L.; Wang, X.-K.; Su, G.-F. Longitudinal extensive transverse myelitis and optic neuritis: The elements for the diagnosis of neuromyelitis optica. Neurol. Sci. 2013, 34, 579–580. [Google Scholar] [CrossRef]
- Tavor, Y.; Herskovitz, M.; Ronen, G.; Balbir-Gurman, A. Longitudinally Extensive Transverse Myelitis in a Lupus–Neuromyelitis Optica Overlap. Rambam Maimonides Med. J. 2021, 12, e0006. [Google Scholar] [CrossRef] [PubMed]
- Greenbaum, H.; Weil, C.; Chodick, G.; Shalev, V.; Eisenberg, V.H. Evidence for an association between endometriosis, fibromyalgia, and autoimmune diseases. Am. J. Reprod. Immunol. 2019, 81, e13095. [Google Scholar] [CrossRef]
- Van Moerkercke, W.; Verhamme, M.; Meeus, G.; Oyen, R.; van Steenbergen, W. A Case of IgG4-Related Sclerosing Disease with Retroperitoneal Fibrosis, Autoimmune Pancreatitis and Bilateral Focal Nephritis. Pancreas 2009, 38, 825–832. [Google Scholar] [CrossRef]
- Shin, L.; Gardner, J.T.; Dao, H. Updates in the Diagnosis and Management of Linear IgA Disease: A Systematic Review. Medicina 2021, 57, 818. [Google Scholar] [CrossRef]
- Priyadarshini, S.R.; Behera, H.S.; Sahu, S.; Dutta, A. Turicella otitidis: A rare agent causing microbial keratitis. BMJ Case Rep. 2021, 14, e241371. [Google Scholar] [CrossRef]
- Ng, H.Y.; Guttman, O.R.; Tucker, L.B. Chronic recurrent multifocal osteomyelitis and primary sclerosing cholangitis with type 1 autoimmune hepatitis in a child with ulcerative colitis: A case report. BMC Rheumatol. 2021, 5, 16. [Google Scholar] [CrossRef] [PubMed]
- Pérez, C.A.; Evangelista, M. Evaluation and Management of Tolosa–Hunt Syndrome in Children: A Clinical Update. Pediatr. Neurol. 2016, 62, 18–26. [Google Scholar] [CrossRef]
- Tocut, M.; Rozman, Z.; Biro, A.; Winder, A.; Tanay, A.; Zandman-Goddard, G. The complexity of an overlap type resistant cryoglobulinemia: A case report and review of the literature. Clin. Rheumatol. 2019, 38, 1257–1262. [Google Scholar] [CrossRef] [PubMed]
- Carey, B.; Setterfield, J. Mucous membrane pemphigoid and oral blistering diseases. Clin. Exp. Dermatol. 2019, 44, 732–739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stepp, M.A.; Menko, A.S. Immune responses to injury and their links to eye disease. Transl. Res. 2021, 236, 52–71. [Google Scholar] [CrossRef]
- Lehto, J.; Kiviniemi, T. Postpericardiotomy syndrome after cardiac surgery. Ann. Med. 2020, 52, 243–264. [Google Scholar] [CrossRef]
- Kandolin, R.; Lehtonen, J.; Salmenkivi, K.; Räisänen-Sokolowski, A.; Lommi, J.; Kupari, M. Diagnosis, Treatment, and Outcome of Giant-Cell Myocarditis in the Era of Combined Immunosuppression. Circ. Heart Fail. 2013, 6, 15–22. [Google Scholar] [CrossRef] [Green Version]
- Farr, E.; D’Andrea, D.; Franz, C.K. Phrenic Nerve Involvement in Neuralgic Amyotrophy (Parsonage-Turner Syndrome). Sleep Med. Clin. 2020, 15, 539–543. [Google Scholar] [CrossRef] [PubMed]
- Polis, B.; Karasik, D.; Samson, A.O. Alzheimer’s disease as a chronic maladaptive polyamine stress response. Aging 2021, 13, 10770. [Google Scholar] [CrossRef]
- Polis, B.; Samson, A.O. A New Perspective on Alzheimer’s Disease as a Brain Expression of a Complex Metabolic Disorder. In Alzheimer’s Disease; Codon Publications: Singapore, 2019. [Google Scholar]
- Sardi, F.; Fassina, L.; Venturini, L.; Inguscio, M.; Guerriero, F.; Rolfo, E.; Ricevuti, G. Alzheimer’s disease, autoimmunity and inflammation. The good, the bad and the ugly. Autoimmun. Rev. 2011, 11, 149–153. [Google Scholar] [CrossRef]
- D’Andrea, M.R. Add Alzheimer’s disease to the list of autoimmune diseases. Med. Hypotheses 2005, 64, 458–463. [Google Scholar] [CrossRef] [PubMed]
- Lim, B.; Prassas, I.; Diamandis, E.P. Alzheimer Disease Pathogenesis: The Role of Autoimmunity. J. Appl. Lab. Med. 2021, 6, 756–764. [Google Scholar] [CrossRef] [PubMed]
- Dow, C.T. Warm, Sweetened Milk at the Twilight of Immunity—Alzheimer’s Disease—Inflammaging, Insulin Resistance, M. paratuberculosis and Immunosenescence. Front. Immunol. 2021, 12, 714179. [Google Scholar] [CrossRef] [PubMed]
- Itzhaki, R.F. Overwhelming Evidence for a Major Role for Herpes Simplex Virus Type 1 (HSV1) in Alzheimer’s Disease (AD); Underwhelming Evidence against. Vaccines 2021, 9, 679. [Google Scholar] [CrossRef]
- Wotton, C.J.; Goldacre, M.J. Associations between specific autoimmune diseases and subsequent dementia: Retrospective record-linkage cohort study, UK. J. Epidemiol. Community Health 2017, 71, 576–583. [Google Scholar] [CrossRef]
- Ciccocioppo, F.; Lanuti, P.; Pierdomenico, L.; Simeone, P.; Bologna, G.; Ercolino, E.; Buttari, F.; Fantozzi, R.; Thomas, A.; Onofrj, M.; et al. The Characterization of Regulatory T-Cell Profiles in Alzheimer’s Disease and Multiple Sclerosis. Sci. Rep. 2019, 9, 8788. [Google Scholar] [CrossRef] [Green Version]
- Chandra, A. Role of Amyloid from a Multiple Sclerosis Perspective: A Literature Review. Neuroimmunomodulation 2015, 22, 343–346. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Samuels, H.; Malov, M.; Saha Detroja, T.; Ben Zaken, K.; Bloch, N.; Gal-Tanamy, M.; Avni, O.; Polis, B.; Samson, A.O. Autoimmune Disease Classification Based on PubMed Text Mining. J. Clin. Med. 2022, 11, 4345. https://doi.org/10.3390/jcm11154345
Samuels H, Malov M, Saha Detroja T, Ben Zaken K, Bloch N, Gal-Tanamy M, Avni O, Polis B, Samson AO. Autoimmune Disease Classification Based on PubMed Text Mining. Journal of Clinical Medicine. 2022; 11(15):4345. https://doi.org/10.3390/jcm11154345
Chicago/Turabian StyleSamuels, Hadas, Malki Malov, Trishna Saha Detroja, Karin Ben Zaken, Naamah Bloch, Meital Gal-Tanamy, Orly Avni, Baruh Polis, and Abraham O. Samson. 2022. "Autoimmune Disease Classification Based on PubMed Text Mining" Journal of Clinical Medicine 11, no. 15: 4345. https://doi.org/10.3390/jcm11154345
APA StyleSamuels, H., Malov, M., Saha Detroja, T., Ben Zaken, K., Bloch, N., Gal-Tanamy, M., Avni, O., Polis, B., & Samson, A. O. (2022). Autoimmune Disease Classification Based on PubMed Text Mining. Journal of Clinical Medicine, 11(15), 4345. https://doi.org/10.3390/jcm11154345