
A Telehealth Intervention for Nutritional Counseling in Amyotrophic Lateral Sclerosis Patients

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Standard Protocol Approval, Registrations, and Patient Consents
2.2. Study Design and Aim
- (1)
- Is dietary monitoring through a Chatbot feasible with ALS patients?
- (2)
- Is the Chatbot approach with a more intensive dietary control effective in stabilizing the body weight of ALS patients?
- (3)
- (1)
- neurological and functional evaluation (ALSFRS-R), monitoring of intercurrent events;
- (2)
- dietary evaluation by diet monitoring (e.g., collection of weight, body mass index (BMI), caloric intake, and diet consistency);
- (3)
- evaluation of the quality of life by collecting ALSAQ-40?
2.3. Participants
- (1)
- (2)
- resident in Italy;
- (3)
- age > 18 years;
- (4)
- who were able to understand the study protocol and able to provide informed consent;
- (5)
- with the presence of caregiver if necessary;
- (6)
- who were able to manage personal computers or smartphones, and internet connection for data sharing.
2.4. Interventions
2.5. Outcome Measures
2.6. Statistical Analysis
3. Results
3.1. Study Population
3.2. Feasibility and Compliance with Counseling
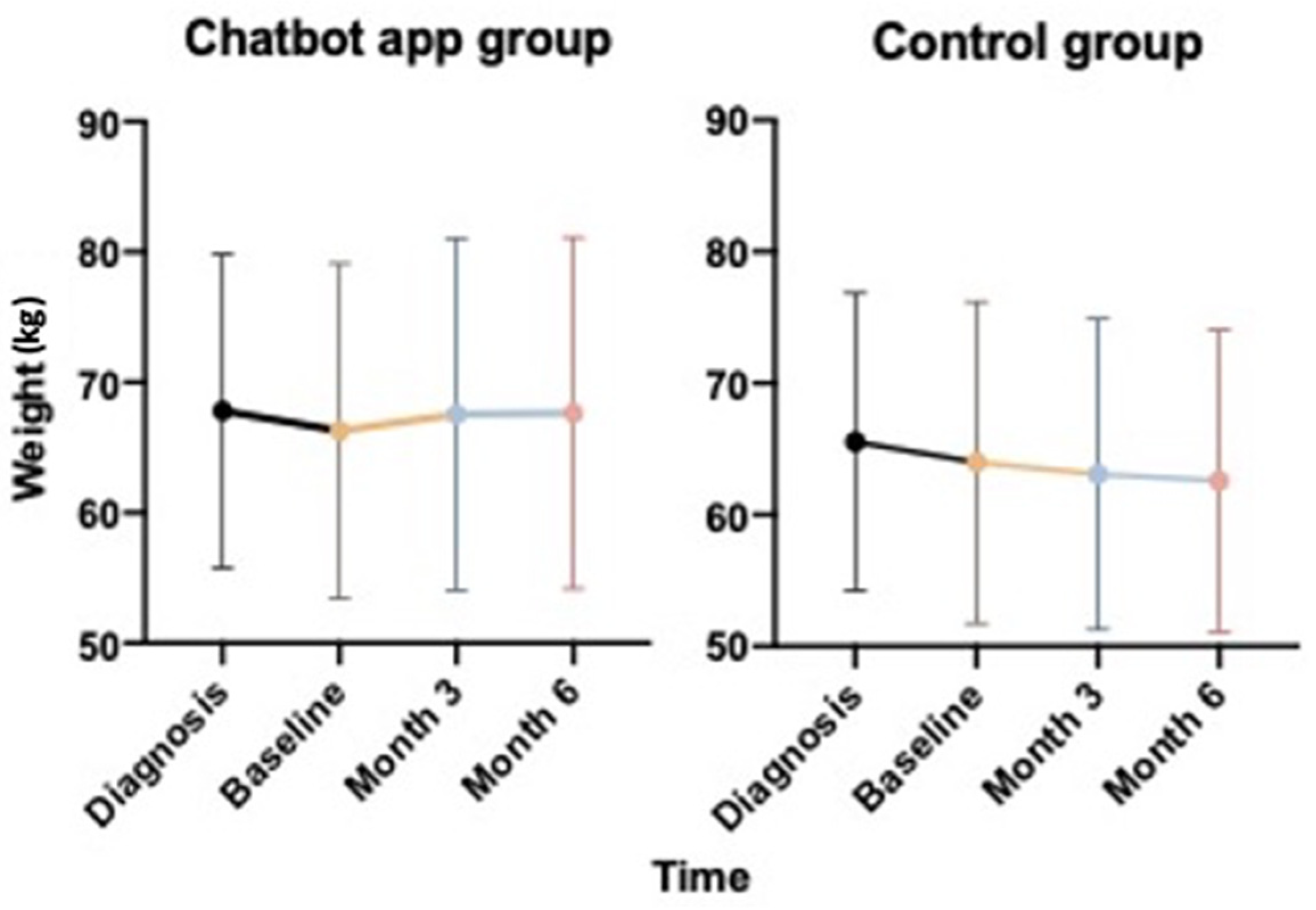
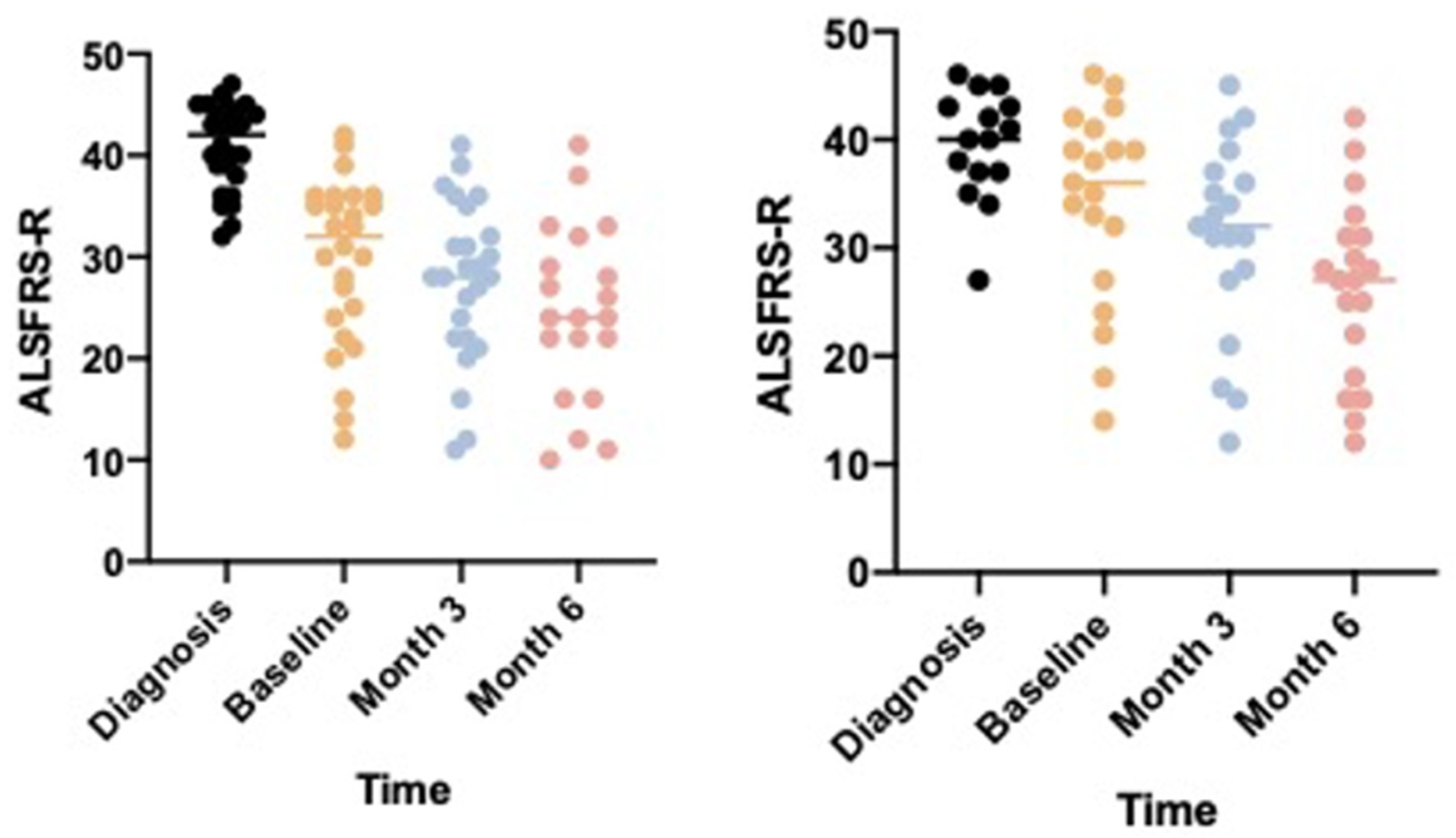
3.3. Efficacy
3.4. Secondary Outcomes
4. Discussion
5. Conclusions
6. Take Home Points
- -
- Weight loss and malnutrition are major obstacles in ALS management and course. Regular nutritional assessment and appropriate interventions are crucial within a multidisciplinary management.
- -
- Nutritional intervention should include a flexible dietary plan, adjustable in accordance with disease complications (dysphagia) and clinical needs (energy and protein requirements).
- -
- A telehealth approach is a feasible and useful tool in ALS population in order to provide effective nutritional monitoring and advice, early detecting swallowing disorders and weight loss and adjusting nutritional strategy.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kiernan, M.C.; Vucic, S.; Cheah, B.C.; Turner, M.R.; Eisen, A.; Hardiman, O.; Burrell, J.R.; Zoing, M.C. Amyotrophic lateral sclerosis. Lancet 2011, 377, 942–955. [Google Scholar] [CrossRef] [Green Version]
- Pinto, S.; Quintarelli, S.; Silani, V. New technologies and amyotrophic lateral sclerosis–which step forward rushed by the COVID-19 pandemic? J. Neurol. Sci. 2020, 418, 117081. [Google Scholar] [CrossRef]
- Van den Berg, J.P.; Kalmijn, S.; Lindeman, E.; Veldink, J.H.; de Visser, M.; van der Graaff, M.M.; Wokke, J.H.J.; van den Berg, L.H. Multidisciplinary ALS care improves quality of life in patients with ALS. Neurology 2005, 65, 1264–1267. [Google Scholar] [CrossRef] [PubMed]
- Marin, B.; Desport, J.-C.; Kajeu, P.; Jesus, P.; Nicolaud, B.; Nicol, M.; Preux, P.M.; Couratier, P. Alteration of nutritional status at diagnosis is a prognostic factor for survival of amyotrophic lateral sclerosis patients. J. Neurol. Neurosurg. Psychiatry 2011, 82, 628–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roubeau, V.; Blasco, H.; Maillot, F.; Corcia, P.; Praline, J. Nutritional assessment of amyotrophic lateral sclerosis in routine practice: Value of weighing and bioelectrical impedance analysis. Muscle Nerv. 2015, 51, 479–484. [Google Scholar] [CrossRef]
- Heffernan, C.; Jenkinson, C.; Holmes, T.; Feder, G.; Kupfer, R.; Leigh, P.N. Nutritional management in MND/ALS patients: An evidence based review. Amyotroph. Lateral Scler Other Mot. Neuron Disord. 2004, 5, 72–83. [Google Scholar] [CrossRef]
- De Marchi, F.; Munitic, I.; Amedei, A.; Berry, J.D.; Feldman, E.L.; Aronica, E.; Nardo, G.; Van Weehaeghe, D.; Niccolai, E.; Prtenjaca, N.; et al. Interplay between immunity and amyotrophic lateral sclerosis: Clinical impact. Neurosci. Biobehav. Rev. 2021, 127, 958–978. [Google Scholar] [CrossRef]
- Bouteloup, C.; Desport, J.-C.; Clavelou, P.; Guy, N.; Detrumeaux-Burel, H.; Ferrier, A.; Couratier, P. Hypermetabolism in ALS patients: An early and persistent phenomenon. J. Neurol. 2009, 256, 1236–1242. [Google Scholar] [CrossRef]
- Mazzini, L.; de Marchi, F.; Niccolai, E.; Mandrioli, J.; Amedei, A. Gastrointestinal Status and Microbiota Shaping in Amyotrophic Lateral Sclerosis: A New Frontier for Targeting? In Amyotrophic Lateral Sclerosis; Exon Publications: Brisbane, Australia, 2021. [Google Scholar]
- Burgos, R.; Bretón, I.; Cereda, E.; Desport, J.C.; Dziewas, R.; Genton, L.; Gomes, F.; Jésus, P.; Leischker, A.; Muscaritoli, M.; et al. ESPEN guideline clinical nutrition in neurology. Clin. Nutr. 2018, 37, 354–396. [Google Scholar] [CrossRef] [Green Version]
- De Marchi, F.; Cantello, R.; Ambrosini, S.; Mazzini, L.; on behalf of the CANPALS Study Group. Telemedicine and technological devices for amyotrophic lateral sclerosis in the era of COVID-19. Neurol. Sci. 2020, 41, 1365–1367. [Google Scholar] [CrossRef]
- De Marchi, F.; Sarnelli, M.F.; Serioli, M.; De Marchi, I.; Zani, E.; Bottone, N.; Ambrosini, S.; Garone, R.; Cantello, R.; Mazzini, L.; et al. Telehealth approach for amyotrophic lateral sclerosis patients: The experience during COVID-19 pandemic. Acta Neurol. Scand. 2021, 143, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Cedarbaum, J.M.; Stambler, N.; Malta, E.; Fuller, C.; Hilt, D.; Thurmond, B.; Nakanishi, A. The ALSFRS-R: A revised ALS functional rating scale that incorporates assessments of respiratory function. J. Neurol. Sci. 1999, 169, 13–21. [Google Scholar] [CrossRef]
- Gordon, P.H.; Miller, R.G.; Moore, D.H. ALSFRS-R. Amyotroph. Lateral Scler Other Mot. Neuron Disord. 2004, 5 (Suppl. 1), 90–93. [Google Scholar] [CrossRef] [PubMed]
- Kollewe, K.; Mauss, U.; Krampfl, K.; Petri, S.; Dengler, R.; Mohammadi, B. ALSFRS-R score and its ratio: A useful predictor for ALS-progression. J. Neurol. Sci. 2008, 275, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Palmieri, A.; Sorarù, G.; Lombardi, L.; D’Ascenzo, C.; Baggio, L.; Ermani, M.; Pegoraro, E.; Angelini, C. Quality of life and motor impairment in ALS: Italian validation of ALSAQ. Neurol. Res. 2010, 32, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Brooks, B.R.; Miller, R.G.; Swash, M.; Munsat, T.L.; World Federation of Neurology Research Group on Motor Neuron Diseases. El Escorial revisited: Revised criteria for the diagnosis of amyotrophic lateral sclerosis. Amyotroph. Lateral Scler Other Mot. Neuron Disord. 2000, 1, 293–299. [Google Scholar] [CrossRef]
- Agosta, F.; Al-Chalabi, A.; Filippi, M.; Hardiman, O.; Kaji, R.; Meininger, V.; Nakano, I.; Shaw, P.; Shefner, J.; van den Berg, L.H.; et al. The El Escorial criteria: Strengths and weaknesses. Amyotroph. Lateral Scler Front. Degener. 2015, 16, 1–7. [Google Scholar] [CrossRef]
- Reich-Slotky, R.; Andrews, J.; Cheng, B.; Buchsbaum, R.; Levy, D.; Kaufmann, P.; Thompson, J.L.P. Body mass index (BMI) as predictor of ALSFRS-R score decline in ALS patients. Amyotroph. Lateral Scler Front. Degener. 2013, 14, 212–216. [Google Scholar] [CrossRef]
- Gallo, V.; Wark, P.A.; Jenab, M.; Pearce, N.; Brayne, C.; Vermeulen, R.; Andersen, P.M.; Hallmans, G.; Kyrozis, A.; Vanacore, N.; et al. Prediagnostic body fat and risk of death from amyotrophic lateral sclerosis: The EPIC cohort. Neurology 2013, 80, 829–838. [Google Scholar] [CrossRef] [Green Version]
- Desport, J.C.; Preux, P.M.; Truong, T.C.; Vallat, J.M.; Sautereau, D.; Couratier, P. Nutritional status is a prognostic factor for survival in ALS patients. Neurology 1999, 53, 1059–1063. [Google Scholar] [CrossRef]
- Paganoni, S.; Deng, J.; Jaffa, M.; Cudkowicz, M.E.; Wills, A.-M. Body mass index, not dyslipidemia, is an independent predictor of survival in amyotrophic lateral sclerosis. Muscle Nerv. 2011, 44, 20–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wills, A.M.; Garry, J.; Hubbard, J.; Mezoian, T.; Breen, C.T.; Ortiz-Miller, C.; Nalipinski, P.; Sullivan, S.; Berry, J.D.; Cudkowicz, M.; et al. Nutritional counseling with or without mobile health technology: A randomized open-label standard-of-care-controlled trial in ALS. BMC Neurol. 2019, 19, 104. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Chatbot Care | Standard of Care | p-Value | |
|---|---|---|---|
| Male/female (n, %) | 17/9 (65%/35%) | 10/10 (50%/50%) | 0.293 |
| Age at onset (years, SD) | 57.2 (13.6) | 59.8 (6.50) | 0.435 |
| Bulbar/spinal phenotype (n, %) | 5/21 (19%/81%) | 7/13 (35%/65%) | 0.227 |
| Educational level (age) | 11.5 (3.94) | 11.0 (4.00) | 0.674 |
| Disease duration (months, SD) | 10.5 (7.25) | 8.52 (7.80) | 0.379 |
| Total ALSFRS-R score at diagnosis (mean, SD); range | 40.90 (4.26) 32–47 | 39.53 (5.05) 27–46 | 0.233 |
| Total ALSFRS-R score at baseline (mean, SD); range | 35.04 (7.74) 13–48 | 34.05 (9.15) 14–46 | 0.693 |
| ALSFRS-R score (item 1–3) at baseline (mean, SD) | 10.04 (2.07) | 8.58 (3.65) | 0.093 |
| ALSFRS-R score (item 4–6) at baseline (mean, SD) | 7.52 (3.38) | 7.21 (3.94) | 0.776 |
| ALSFRS-R score (item 7–9) at baseline (mean, SD) | 6.80 (3.05) | 7.53 (3.69) | 0.466 |
| ALSFRS-R score (item 10–12) at baseline (mean, SD) | 10.56 (1.88) | 10.74 (2.24) | 0.768 |
| Weight at diagnosis (mean, SD) | 67.80 (12.00) | 65.55 (11.30) | 0.521 |
| BMI at diagnosis (mean, SD); range | 24.55 (3.80) 18.72–35.56 | 24.86 (4.74) 18.25–38.22 | 0.806 |
| Weight at baseline (mean, SD) | 66.27 (11.97) | 63.98 (11.97) | 0.523 |
| BMI at baseline (mean, SD); range | 23.72 (3.98) 17.82–36.44 | 24.54 (4.74) 16.75–38.22 | 0.527 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Marchi, F.; Serioli, M.; Collo, A.; Belotti, E.G.; Alloatti, F.; Biroli, G.; Bolioli, A.; Cantello, R.; Riso, S.; Mazzini, L. A Telehealth Intervention for Nutritional Counseling in Amyotrophic Lateral Sclerosis Patients. J. Clin. Med. 2022, 11, 4286. https://doi.org/10.3390/jcm11154286
De Marchi F, Serioli M, Collo A, Belotti EG, Alloatti F, Biroli G, Bolioli A, Cantello R, Riso S, Mazzini L. A Telehealth Intervention for Nutritional Counseling in Amyotrophic Lateral Sclerosis Patients. Journal of Clinical Medicine. 2022; 11(15):4286. https://doi.org/10.3390/jcm11154286
Chicago/Turabian StyleDe Marchi, Fabiola, Marcella Serioli, Alessandro Collo, Evelyn Gisell Belotti, Francesca Alloatti, Giampaolo Biroli, Andrea Bolioli, Roberto Cantello, Sergio Riso, and Letizia Mazzini. 2022. "A Telehealth Intervention for Nutritional Counseling in Amyotrophic Lateral Sclerosis Patients" Journal of Clinical Medicine 11, no. 15: 4286. https://doi.org/10.3390/jcm11154286
APA StyleDe Marchi, F., Serioli, M., Collo, A., Belotti, E. G., Alloatti, F., Biroli, G., Bolioli, A., Cantello, R., Riso, S., & Mazzini, L. (2022). A Telehealth Intervention for Nutritional Counseling in Amyotrophic Lateral Sclerosis Patients. Journal of Clinical Medicine, 11(15), 4286. https://doi.org/10.3390/jcm11154286