
Negative-Pressure Wound Therapy for Prevention of Sternal Wound Infection after Adult Cardiac Surgery: Systematic Review and Meta-Analysis

 ,
, 
Abstract
:1. Introduction
2. Material and Methods
2.1. Literature Search Strategy
2.2. Treatment Definition and Inclusion/Exclusion Criteria
2.3. Data Extraction
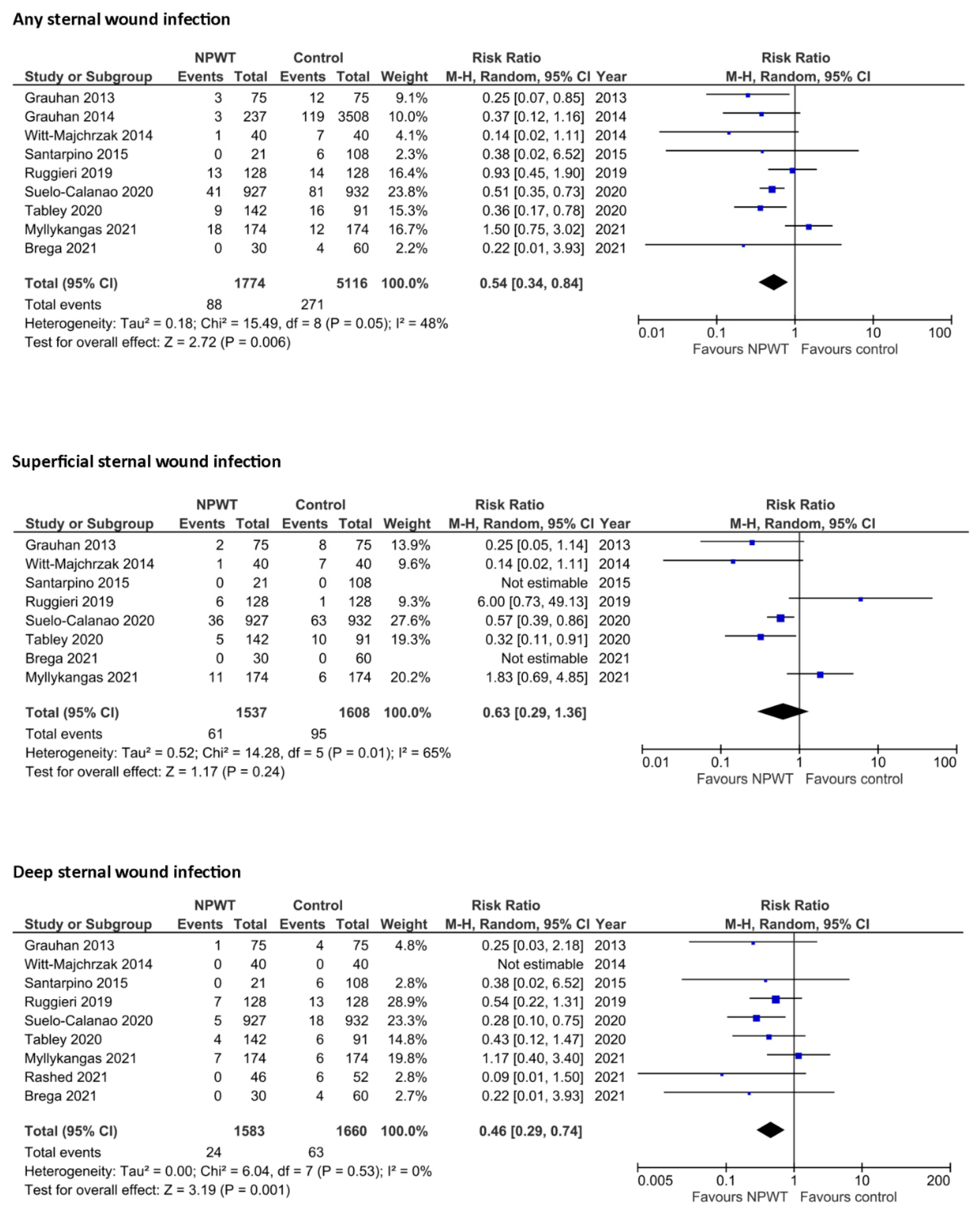
2.4. Outcome Measures
2.5. Statistical Analysis
3. Results
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gaudino, M.; Audisio, K.; Rahouma, M.; Robinson, N.B.; Soletti, G.J.; Cancelli, G.; Masterson Creber, R.M.M.; Gray, A.; Lees, B.; Gerry, S.; et al. Association between sternal wound complications and 10-year mortality following coronary artery bypass grafting. J. Thorac. Cardiovasc. Surg. 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Coskun, D.; Aytac, J.; Aydinli, A.; Bayer, A. Mortality rate, length of stay and extra cost of sternal surgical site infections following coronary artery bypass grafting in a private medical centre in Turkey. J. Hosp. Infect. 2005, 60, 176–179. [Google Scholar] [CrossRef] [PubMed]
- Hirahara, N.; Miyata, H.; Motomura, N.; Kohsaka, S.; Nishimura, T.; Takamoto, S. Procedure- and hospital-level variation of deep sternal wound infection from all-Japan registry. Ann. Thorac. Surg. 2020, 109, 547–554. [Google Scholar] [CrossRef] [PubMed]
- Dai, C.; Lu, Z.; Zhu, H.; Xue, S.; Lian, F. Bilateral internal mammary artery grafting and risk of sternal wound infection: Evidence from observational studies. Ann. Thorac. Surg. 2013, 95, 1938–1945. [Google Scholar] [CrossRef]
- Schwann, T.A.; Gaudino, M.F.; Engelman, D.T.; Sedrakyan, A.; Li, D.; Tranbaugh, R.F.; Habib, R.H. Effect of skeletonization of bilateral internal thoracic arteries on deep sternal wound infections. Ann. Thorac. Surg. 2021, 111, 600–606. [Google Scholar] [CrossRef]
- Lazar, H.L.; Salm, T.V.; Engelman, R.; Orgill, D.; Gordon, S. Prevention and management of sternal wound infections. J. Thorac. Cardiovasc. Surg. 2016, 152, 962–972. [Google Scholar] [CrossRef] [Green Version]
- Zwanenburg, P.R.; Tol, B.T.; Obdeijn, M.C.; Lapid, O.; Gans, S.L.; Boermeester, M.A. Meta-analysis, meta-regression, and GRADE assessment of randomized and nonrandomized studies of incisional negative pressure wound therapy versus control dressings for the prevention of postoperative wound complications. Ann. Surg. 2020, 272, 81–91. [Google Scholar] [CrossRef]
- Biancari, F.; Gatti, G.; Rosato, S.; Mariscalco, G.; Pappalardo, A.; Onorati, F.; Faggian, G.; Salsano, A.; Santini, F.; Ruggieri, V.G.; et al. Preoperative risk stratification of deep sternal wound infection after coronary surgery. Infect. Control Hosp. Epidemiol. 2020, 41, 444–451. [Google Scholar] [CrossRef]
- Norman, G.; Goh, E.L.; Dumville, J.C.; Shi, C.; Liu, Z.; Chiverton, L.; Stankiewicz, M.; Dumville, J.C. Negative pressure wound therapy for surgical wounds healing by primary closure. Cochrane Database Syst. Rev. 2020, 6, CD009261. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. J. Clin. Epidemiol. 2021, 134, 178–189. [Google Scholar] [CrossRef]
- Myllykangas, H.M.; Halonen, J.; Husso, A.; Väänänen, H.; Berg, L.T. Does incisional negative pressure wound therapy prevent sternal wound infections? Thorac. Cardiovasc. Surg. 2022, 70, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Rashed, A.; Csiszar, M.; Beledi, A.; Gombocz, K. The impact of incisional negative pressure wound therapy on the wound healing process after midline sternotomy. Int. Wound J. 2021, 18, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Ruggieri, V.G.; Olivier, M.E.; Aludaat, C.; Rosato, S.; Marticho, P.; Saade, Y.A.; Lefebvre, A.; Poncet, A.; Rubin, S.; Biancari, F. Negative pressure versus conventional sternal wound dressing in coronary surgery using bilateral internal mammary artery grafts. Heart Surg. Forum 2019, 22, 92–96. [Google Scholar] [CrossRef] [PubMed]
- Grauhan, O.; Navasardyan, A.; Hofmann, M.; Muller, P.; Stein, J.; Hetzer, R. Prevention of poststernotomy wound infections in obese patients by negative pressure wound therapy. J. Thorac. Cardiovasc. Surg. 2013, 145, 1387–1392. [Google Scholar] [CrossRef] [Green Version]
- Brega, C.; Calvi, S.; Albertini, A. Use of negative pressure wound therapy system over closed incisions option in preventing post-sternotomy wound complications. Wound Rep. Reg. 2021, 29, 848–852. [Google Scholar] [CrossRef]
- Suelo-Calanao, R.L.; Thomson, R.; Read, M.; Matheson, E.; Isaac, E.; Chaudhry, M.; Loubani, M. The impact of incision negative pressure therapy on prevention of median sternotomy infection for high risk cases: A single centre retrospective study. J. Cardiothorac. Surg. 2020, 15, 222. [Google Scholar] [CrossRef]
- Grauhan, O.; Navasardyan, A.; Tutkun, B.; Hennig, F.; Müller, P.; Hummel, M.; Hetzer, R. Effect of surgical incision management on wound infections in a poststernotomy patient population. Int. Wound J. 2014, 11 (Suppl. S1), 6–9. [Google Scholar] [CrossRef]
- Witt-Majchrzak, A.; Żelazny, P.; Snarska, J. Preliminary outcome of treatment of postoperative primarily closed sternotomy wounds treated using negative pressure wound therapy. Pol. Przegl. Chir. 2015, 86, 456–465. [Google Scholar] [CrossRef]
- Santarpino, G.; Gazdag, L.; Sirch, J.; Vogt, F.; Ledwon, M.; Fischlein, T.; Pfeiffer, S. A retrospective study to evaluate use of negative pressure wound therapy in patients undergoing bilateral internal thoracic artery grafting. Ostomy Wound Manag. 2015, 61, 26–30. [Google Scholar]
- Tabley, A.; Aludaat, C.; Le Guillou, V.; Gay, A.; Nafeh-Bizet, C.; Scherrer, V.; Bouchart, F.; Doguet, F. A survey of cardiac surgery infections with PICO negative pressure therapy in high-risk patients. Ann. Thorac. Surg. 2020, 110, 2034–2040. [Google Scholar] [CrossRef]
- Davierwala, P.M.; Mohr, F.W. Bilateral internal mammary artery grafting: Rationale and evidence. Int. J. Surg. 2015, 16, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Graf, K.; Ott, E.; Vonberg, R.P.; Kuehn, C.; Haverich, A.; Chaberny, I.F. Economic aspects of deep sternal wound infections. Eur. J. Cardiothorac. Surg. 2010, 37, 893–896. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, R.B.; Mehaffey, J.H.; Charles, E.J.; Krebs, E.D.; Smith, J.G.; Kern, J.A.; Wanchek, T.; Teman, N. Cost-effectiveness of negative pressure incision management system in cardiac surgery. J. Surg. Res. 2019, 240, 227–235. [Google Scholar] [CrossRef]
- Ariyaratnam, P.; Bland, M.; Loubani, M. Risk factors and mortality associated with deep sternal wound infections following coronary bypass surgery with or without concomitant procedures in a UK population: A basis for a new risk model? Interact. Cardiovasc. Thorac. Surg. 2010, 11, 543–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| PICO | Description |
|---|---|
| Population | Patients who underwent any adult cardiac surgery procedure |
| Intervention | Negative-pressure wound therapy with any commercially available device |
| Comparison | Standard wound therapy |
| Outcomes | Any sternal wound infection, superficial sternal wound infection, deep sternal wound infection |
| Variables | No. of Studies | NPWT Cohort | Control Cohort | p-Value |
|---|---|---|---|---|
| Age, mean in years | 9 | 66.1 | 66.2 | 0.975 |
| Female | 8 | 29.5% | 28.4% | 0.937 |
| BMI > 30 kg/m2 | 6 | 59.4% | 64.8% | 0.785 |
| Diabetes | 9 | 49.4% | 52.3% | 0.825 |
| Pulmonary disease | 9 | 15.9% | 17.3% | 0.992 |
| Any coronary surgery | 9 | 85.7% | 84.1% | 0.354 |
| Isolated coronary surgery | 8 | 75.8% | 76.1% | 0.862 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Biancari, F.; Santoro, G.; Provenzano, F.; Savarese, L.; Iorio, F.; Giordano, S.; Zebele, C.; Speziale, G. Negative-Pressure Wound Therapy for Prevention of Sternal Wound Infection after Adult Cardiac Surgery: Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 4268. https://doi.org/10.3390/jcm11154268
Biancari F, Santoro G, Provenzano F, Savarese L, Iorio F, Giordano S, Zebele C, Speziale G. Negative-Pressure Wound Therapy for Prevention of Sternal Wound Infection after Adult Cardiac Surgery: Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2022; 11(15):4268. https://doi.org/10.3390/jcm11154268
Chicago/Turabian StyleBiancari, Fausto, Grazia Santoro, Federica Provenzano, Leonardo Savarese, Francesco Iorio, Salvatore Giordano, Carlo Zebele, and Giuseppe Speziale. 2022. "Negative-Pressure Wound Therapy for Prevention of Sternal Wound Infection after Adult Cardiac Surgery: Systematic Review and Meta-Analysis" Journal of Clinical Medicine 11, no. 15: 4268. https://doi.org/10.3390/jcm11154268
APA StyleBiancari, F., Santoro, G., Provenzano, F., Savarese, L., Iorio, F., Giordano, S., Zebele, C., & Speziale, G. (2022). Negative-Pressure Wound Therapy for Prevention of Sternal Wound Infection after Adult Cardiac Surgery: Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 11(15), 4268. https://doi.org/10.3390/jcm11154268