
NICU Admission for Term Neonates in a Large Single-Center Population: A Comprehensive Assessment of Risk Factors Using a Tandem Analysis Approach

 , , ,
, , , 
Abstract
:1. Introduction
2. Methods
2.1. Study Population and Data Collection
2.2. Data Collection and Variables
2.3. Data Analysis
2.3.1. Statistical Analyses
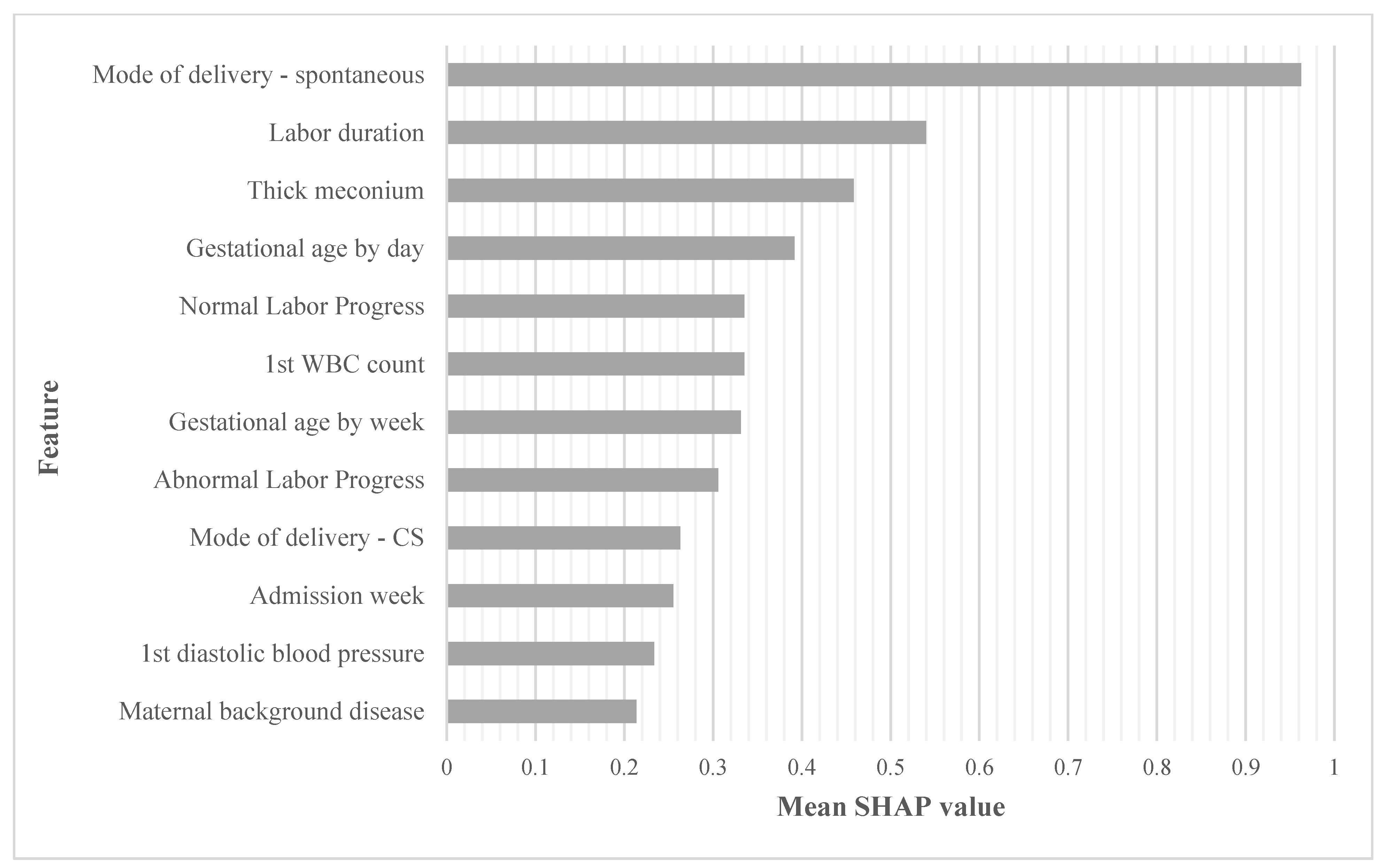
2.3.2. Machine Learning and Gradient Boosting Model
3. Results
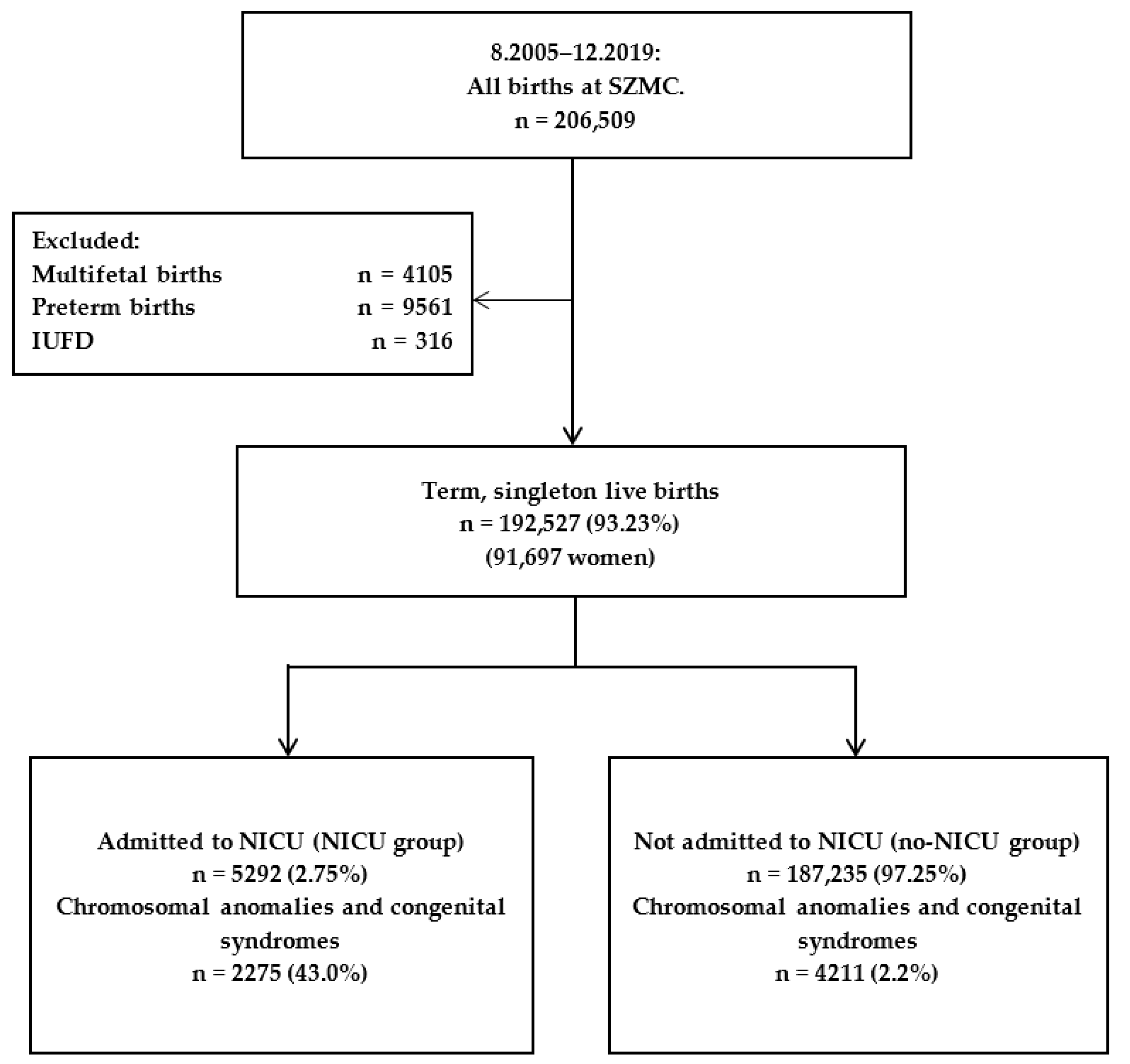
3.1. Study Population
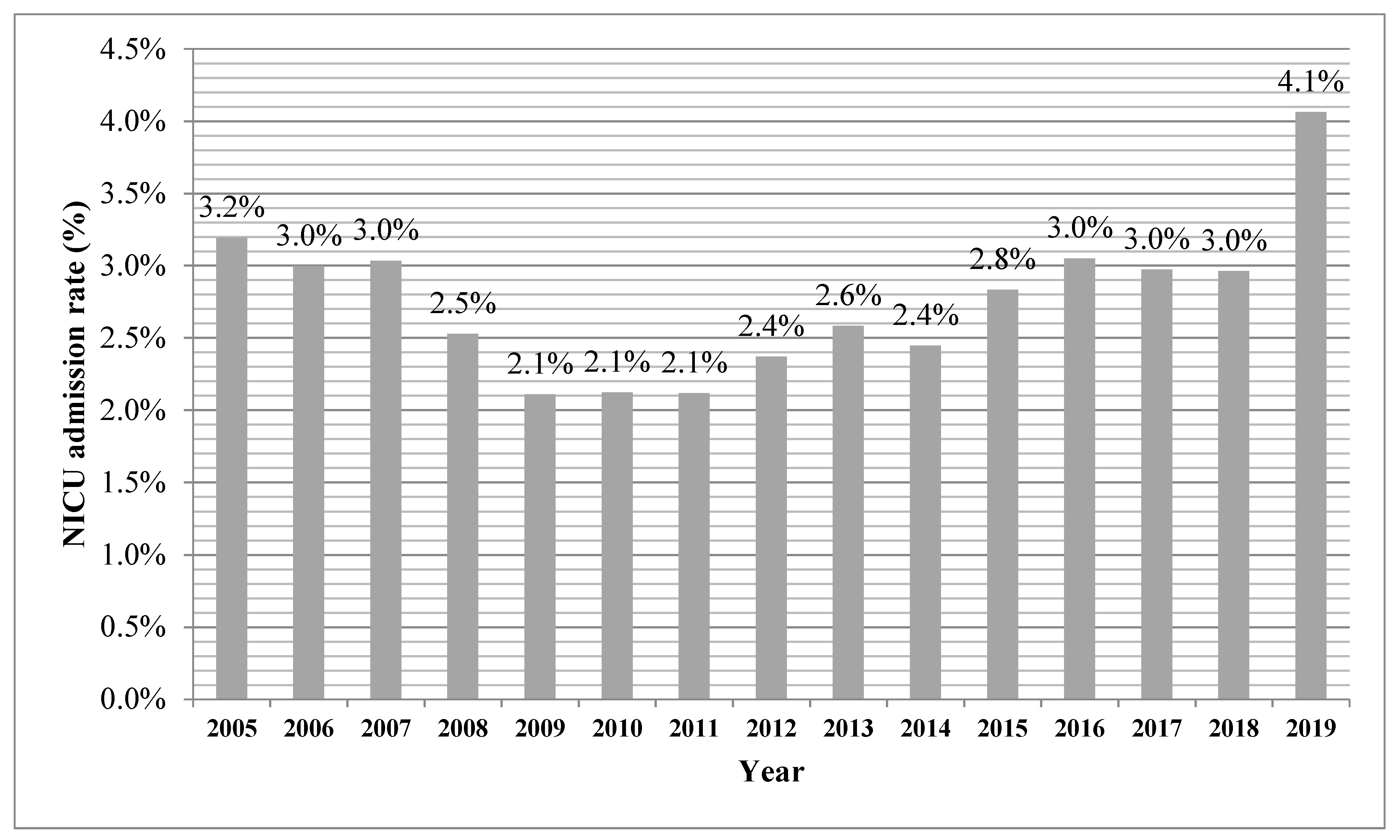
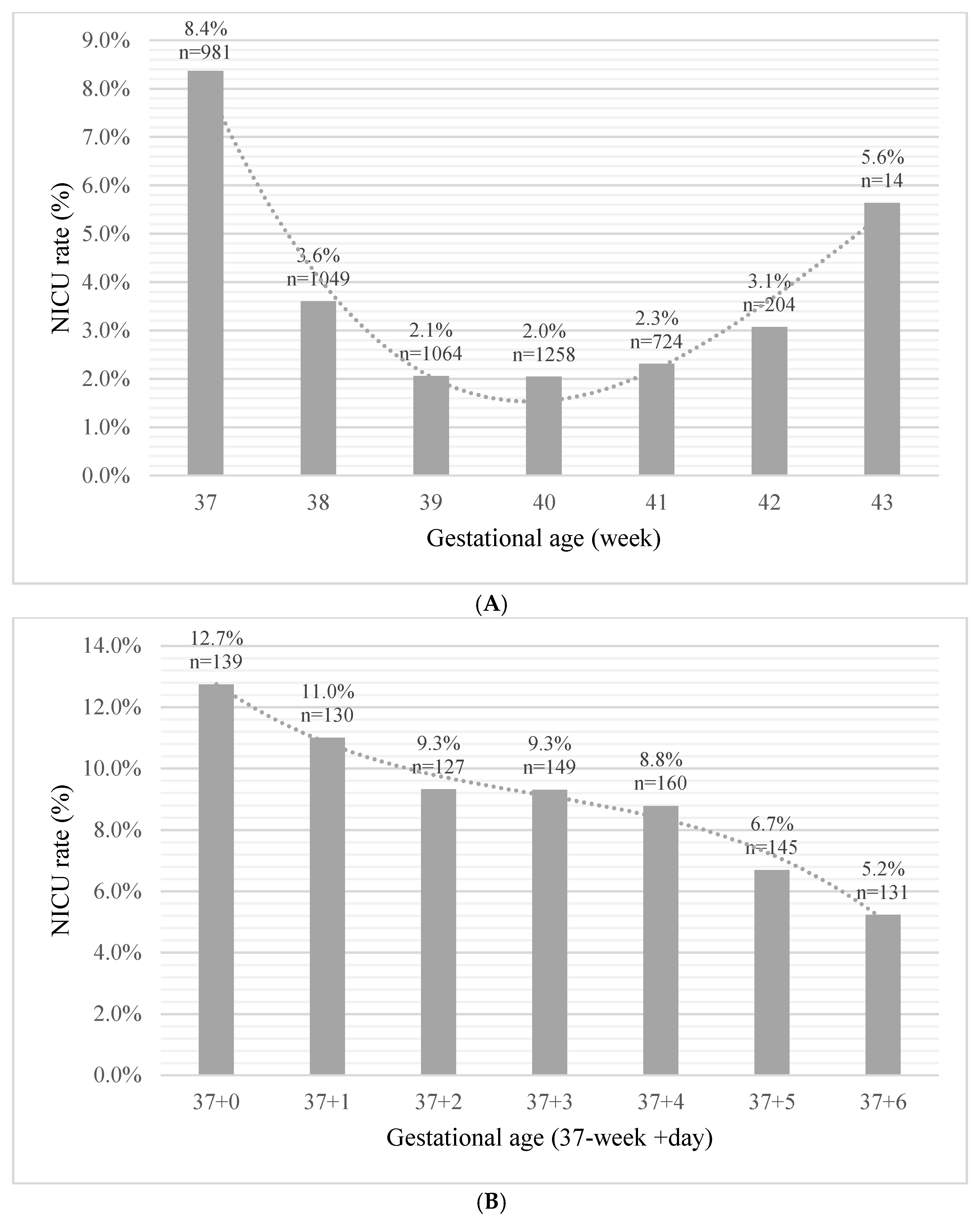
3.2. Neonatal Admission to NICU
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- Tubbs-Cooley, H.L.; Mara, C.A.; Carle, A.C.; Mark, B.A.; Pickler, R.H. Association of Nurse Workload with Missed Nursing Care in the Neonatal Intensive Care Unit. JAMA Pediatr. 2019, 173, 44–51. [Google Scholar] [CrossRef]
- Tawfik, D.S.; Thomas, E.J.; Vogus, T.J.; Liu, J.B.; Sharek, P.J.; Nisbet, C.C.; Lee, H.C.; Sexton, J.B.; Profit, J. Safety climate, safety climate strength, and length of stay in the NICU. BMC Health Serv. Res. 2019, 19, 738. [Google Scholar] [CrossRef] [Green Version]
- Harrison, W.; Goodman, D. Epidemiologic trends in neonatal intensive care, 2007–2012. JAMA Pediatr. 2015, 169, 855–862. [Google Scholar] [CrossRef] [Green Version]
- Olusanya, B.O. Full-term newborns with normal birth weight requiring special care in a resource-constrained setting. Pan Afr. Med. J. 2013, 15, 1–10. [Google Scholar] [CrossRef]
- Demisse, A.G.; Alemu, F.; Gizaw, M.A.; Tigabu, Z. Patterns of admission and factors associated with neonatal mortality among neonates admitted to the neonatal intensive care unit of University of Gondar Hospital, Northwest Ethiopia. Pediatr. Health Med. Ther. 2017, 8, 57–64. [Google Scholar] [CrossRef] [Green Version]
- Clapp, M.A.; James, K.E.; Bates, S.V.; Kaimal, A.J. Unexpected term NICU admissions: A marker of obstetrical care quality? Am. J. Obstet. Gynecol. 2019, 220, 395.e1–395.e12. [Google Scholar] [CrossRef]
- Lange, A.P.; Secher, N.J.; Westergaard, J.G.; Skovgård, I.; Stat, C. Prelabor evaluation of inducibility. Obstet. Gynecol. 1982, 60, 137–147. [Google Scholar] [PubMed]
- Dollberg, S.; Haklai, Z.; Mimouni, F.B.; Gorfein, I.; Gordon, E.S. Birthweight standards in the live-born population in Israel. Isr. Med. Assoc. J. 2005, 7, 311–314. [Google Scholar]
- Guedalia, J.; Lipschuetz, M.; Novoselsky-Persky, M.; Cohen, S.M.; Rottenstreich, A.; Levin, G.; Yagel, S.; Unger, R.; Sompolinsky, Y. Real-time data analysis using a machine learning model significantly improves prediction of successful vaginal deliveries. Am. J. Obstet. Gynecol. 2020, 223, 437.e1–437.e15. [Google Scholar] [CrossRef]
- Sun, X.; Xu, W. Fast implementation of DeLong’s algorithm for comparing the areas under correlated receiver operating characteristic curves. IEEE Signal Process. Lett. 2014, 21, 1389–1393. [Google Scholar] [CrossRef]
- Lundberg, S.M.; Erion, G.; Chen, H.; DeGrave, A.; Prutkin, J.M.; Nair, B.; Katz, R.; Himmelfarb, J.; Bansal, N.; Lee, S.-I. From local explanations to global understanding with explainable AI for trees. Nat. Mach. Intell. 2020, 2, 56–67. [Google Scholar] [CrossRef] [PubMed]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- Kennedy, E.B.; Hacker, M.R.; Miedema, D.; Pursley, D.W.M.; Modest, A.M.; Golen, T.H.; Burris, H.H. NICU Admissions After a Policy to Eliminate Elective Early Term Deliveries Before 39 Weeks’ Gestation. Hosp. Pediatr. 2018, 8, 686–692. [Google Scholar] [CrossRef] [Green Version]
- Tracy, S.K.; Tracy, M.B.; Sullivan, E. Admission of term infants to neonatal intensive care: A population-based study. Birth 2007, 34, 301–307. [Google Scholar] [CrossRef]
- Gray, J.E.; McCormick, M.C.; Richardson, D.K.; Ringer, S. Normal birth weight intensive care unit survivors: Outcome assessment. Pediatrics 1996, 97, 832–838. [Google Scholar] [CrossRef]
- Kalafat, E.; Morales-Rosello, J.; Thilaganathan, B.; Dhother, J.; Khalil, A. Risk of neonatal care unit admission in small for gestational age fetuses at term: A prediction model and internal validation. J. Matern. Neonatal Med. 2019, 32, 2361–2368. [Google Scholar] [CrossRef]
- Yang, X.; Meng, T. Admission of full-term infants to the neonatal intensive care unit: A 9.5-year review in a tertiary teaching hospital. J. Matern. Neonatal Med. 2020, 33, 3003–3009. [Google Scholar] [CrossRef]
- Evers, A.C.C.; Brouwers, H.A.A.; Hukkelhoven, C.W.P.M.; Nikkels, P.G.J.; Boon, J.; Van Egmond-Linden, A.; Hillegersberg, J.; Snuif, Y.S.; Sterken-Hooisma, S.; Bruinse, H.W.; et al. Perinatal mortality and severe morbidity in low and high risk term pregnancies in the Netherlands: Prospective cohort study. BMJ 2010, 341, c5639. [Google Scholar] [CrossRef] [Green Version]
- Horowitz, K.; Feldman, D.; Stuart, B.; Borgida, A.; Ming Victor Fang, Y.; Herson, V. Full-term neonatal intenstive care unit admission in an urban community hospital: The role of respiratory morbidity. J. Matern. Neonatal Med. 2011, 24, 1407–1410. [Google Scholar] [CrossRef]
- Alkiaat, A.; Hutchinson, M.; Jacques, A.; Sharp, M.J.; Dickinson, J.E. Evaluation of the frequency and obstetric risk factors associated with term neonatal admissions to special care units. Aust. N. Z. J. Obstet. Gynaecol. 2013, 53, 277–282. [Google Scholar] [CrossRef]
- Ziegler, K.A.; Paul, D.A.; Hoffman, M.; Locke, R. Variation in NICU Admission Rates Without Identifiable Cause. Hosp. Pediatr. 2016, 6, 255–260. [Google Scholar] [CrossRef] [Green Version]
- Craighead, D.V.; Elswick, R.K. The Influence of Early-Term Birth on NICU Admission, Length of Stay, and Breastfeeding Initiation and Duration. JOGNN J. Obstet. Gynecol. Neonatal Nurs. 2014, 43, 409–421. [Google Scholar] [CrossRef]
- Al-Wassia, H.; Saber, M. Admission of term infants to the neonatal intensive care unit in a Saudi tertiary teaching hospital: Cumulative incidence and risk factors. Ann. Saudi Med. 2017, 37, 420–424. [Google Scholar] [CrossRef] [Green Version]
- Aagaard, H.; Uhrenfeldt, L.; Spliid, M.; Fegran, L. Parents’ experiences of transition when their infants are discharged from the Neonatal Intensive Care Unit: A systematic review protocol. JBI Evid. Synth. 2015, 13, 123–132. [Google Scholar] [CrossRef]
- Haviv, H.R.; Said, J.; Mol, B.W. The place of antenatal corticosteroids in late preterm and early term births. Semin. Fetal Neonatal Med. 2019, 24, 37–42. [Google Scholar] [CrossRef] [Green Version]
- American College of Obstetricians and Gynecologists. ACOG Committee opinion no 579: Definition of term pregnancy. Obstet. Gynecol. 2013, 122, 1139–1140. [Google Scholar] [CrossRef]
- Spong, C.Y. Defining “term” pregnancy: Recommendations from the defining “term” pregnancy workgroup. JAMA J. Am. Med. Assoc. 2013, 309, 2445–2446. [Google Scholar] [CrossRef]
- Torbenson, V.E.; Tolcher, M.C.; Nesbitt, K.M.; Colby, C.E.; El-Nashar, S.A.; Gostout, B.S.; Weaver, A.L.; Gree, M.E.M.; Famuyide, A.O. Intrapartum factors associated with neonatal hypoxic ischemic encephalopathy: A case-controlled study. BMC Pregnancy Childbirth 2017, 17, 415. [Google Scholar] [CrossRef] [Green Version]
- Michaeli, J.; Srebnik, N.; Zilberstein, Z.; Rotem, R.; Bin-Nun, A.; Grisaru-Granovsky, S. Intrapartum fetal monitoring and perinatal risk factors of neonatal hypoxic-ischemic encephalopathy. Arch. Gynecol. Obstet. 2021, 303, 409–417. [Google Scholar] [CrossRef]
- Braun, D.; Braun, E.; Chiu, V.; Burgos, A.E.; Gupta, M.; Volodarskiy, M.; Getahun, D. Trends in Neonatal Intensive Care Unit Utilization in a Large Integrated Health Care System. JAMA Netw. Open 2020, 3, e205239. [Google Scholar] [CrossRef]
- Mani, S.; Ozdas, A.; Aliferis, C.; Varol, H.A.; Chen, Q.; Carnevale, R.; Chen, Y.; Romano-Keeler, J.; Nian, H.; Weitkamp, J.-H. Medical decision support using machine learning for early detection of late-onset neonatal sepsis. J. Am. Med. Inform. Assoc. 2014, 21, 326–336. [Google Scholar] [CrossRef] [Green Version]
- Van Laere, D.; Meeus, M.; Beirnaert, C.; Sonck, V.; Laukens, K.; Mahieu, L.; Mulder, A. Machine Learning to Support Hemodynamic Intervention in the Neonatal Intensive Care Unit. Clin. Perinatol. 2020, 47, 435–448. [Google Scholar] [CrossRef]
- Deo, R.C. Machine Learning in Medicine. Circulation 2015, 132, 1920–1930. [Google Scholar] [CrossRef] [Green Version]
- Williams, J.B.; Ghosh, D.; Wetzel, R.C. Applying Machine Learning to Pediatric Critical Care Data. Pediatr. Crit. Care Med. 2018, 19, 599–608. [Google Scholar] [CrossRef]
- Altman, R.B. Artificial intelligence (AI) systems for interpreting complex medical datasets. Clin. Pharmacol. Ther. 2017, 101, 585–586. [Google Scholar] [CrossRef]
- Keskinbora, K.H. Medical ethics considerations on artificial intelligence. J. Clin. Neurosci. 2019, 64, 277–282. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | NICU (n = 5292) | No-NICU (n = 187,235) | p | |
|---|---|---|---|---|
| Demographics and clinical history | Maternal age, mean (SD), Y | 29.3 (6.2) | 28.9 (5.7) | <0.001 |
| Maternal age > 35, n (%) | 988 (18.7) | 28,139 (15.0) | <0.001 | |
| Arab population group, n (%) | 590 (11.1) | 14,514 (7.8) | <0.001 | |
| Ethiopian ethnicity, n (%) | 101 (1.9) | 2045 (1.1) | <0.001 | |
| Education > 12 years, n (%) | 4884 (96.3) | 175,329 (97.8) | <0.001 | |
| GDM/DM, n (%) | 544 (10.3) | 6127 (3.3) | <0.001 | |
| Hypertensive disorder, n (%) | 246 (4.6) | 3500 (1.9) | <0.001 | |
| Maternal background disease, n (%) | 1441 (27.2) | 28,253 (15.1) | <0.001 | |
| Obstetrical history | Gestational age at birth, mean (SD), W | 39.1 (1.4) | 39.5 (1.2) | <0.001 |
| Parity, mean (SD), N | 3.3 (2.6) | 3.5 (2.4) | <0.001 | |
| ART, n (%) | 249 (4.7) | 5390 (2.9) | <0.001 | |
| Prior CS, n (%) | 1047 (19.8) | 21,439 (11.5) | <0.001 | |
| Prior miscarriage, n (%) | 1581 (29.9) | 54,562 (29.1) | 0.25 | |
| High risk hospitalization in pregnancy, n (%) | 327 (8.1) | 6977 (4.7) | <0.001 | |
| Inter-pregnancy interval, mean (SD), W | 94.7 (73.9) | 85.1 (61.2) | <0.001 | |
| Past neonatal death, n (%) | 46 (0.9) | 877 (0.5) | <0.001 | |
| Antenatal care, n (%) | 4282 (80.9) | 154,673 (82.6) | <0.001 | |
| Obstetrical data | Mode of delivery, n (%) | <0.001 | ||
| Spontaneous | 2959 (55.9) | 159,730 (85.3) | ||
| Instrumental | 674 (12.7) | 10,735 (5.7) | ||
| CS | 1659 (31.3) | 16,770 (9.0) | ||
| Mode of labor initiation, n (%) | <0.001 | |||
| Spontaneous | 3363 (63.5) | 159,696 (85.3) | ||
| Induction | 997 (18.8) | 17,165 (9.2) | ||
| Elective CS | 932 (17.6) | 10,374 (5.5) | ||
| TOLAC, n (%) | 479 (9.1) | 14,661 (7.8) | 0.001 | |
| Thick meconium, n (%) | 578 (10.9) | 9030 (4.8) | <0.001 | |
| Head presentation, n (%) | 5034 (95.4) | 183,112 (98.0) | <0.001 | |
| Labor duration, mean (SD), Min | 442.1 (563.0) | 271.5 (344.5) | <0.001 | |
| Stage II duration, mean (SD), Min | 50.5 (63.6) | 33.0 (49.2) | <0.001 | |
| Stage III duration, mean (SD), Min | 11.6 (9.2) | 10.7 (26.3) | <0.001 | |
| On-call hours at births, n (%) | 3532 (66.7) | 134,621 (71.9) | <0.001 | |
| Neonatal characteristics and outcomes | Female sex, n (%) | 2273 (43.0) | 91,595 (48.9) | <0.001 |
| Birth weight, mean (SD), Gr | 3222.6 (576.4) | 3333.6 (424.5) | <0.001 | |
| 5’-Apgar ≤ 7, n (%) | 794 (15.0) | 2015 (1.1) | <0.001 | |
| Macrosomia, n (%) | 422 (8.2) | 11,751 (6.3) | <0.001 | |
| SGA, n (%) | 844 (15.9) | 11,224 (6.0) | <0.001 | |
| Pediatrician present at birth, n (%) | 1492 (28.2) | 14,154 (7.6) | <0.001 |
| OR [95%CI] | p | |
|---|---|---|
| Maternal age >35 years | 1.06 [0.94, 1.21] | 0.32 |
| Arab population group | 1.13 [0.98, 1.31] | 0.081 |
| Ethiopian ethnicity | 1.01 [0.69, 1.46] | 0.96 |
| GDM/DM | 2.52 [2.09, 3.03] | <0.001 * |
| Hypertensive disorder | 1.28 [1.02, 1.60] | 0.035 * |
| ART | 0.88 [0.70, 1.11] | 0.29 |
| Maternal background disease | 1.15 [1.02, 1.31] | 0.022 * |
| Antenatal care | 0.89 [0.80, 1.01] | 0.079 |
| Nulliparity | 1.19 [1.07, 1.33] | 0.002 * |
| Prior CS | 1.08 [0.93, 1.26] | 0.32 |
| High risk hospitalization | 1.42 [1.21, 1.66] | <0.001 * |
| Head presentation | 0.91 [0.57, 1.44] | 0.69 |
| On-call hours at birth | 0.95 [0.86, 1.04] | 0.29 |
| Gestational age at birth = 37 W | 2.99 [2.63, 3.41] | <0.001 * |
| Gestational age at birth 42–43 W | 0.98 [0.80, 1.22] | 0.91 |
| Induction | 1.28 [1.12, 1.46] | <0.001 * |
| Elective CS | 1.52 [1.05, 2.22] | 0.026 |
| Education > 12 years | 1.04 [0.77, 1.39] | 0.81 |
| Feature | OR [95%CI] | p-Value | Crude Numeric Results * | |
|---|---|---|---|---|
| Severe placental, uterine, and maternal bleeding complications | Uterine Dehiscence | 43.52 [26.65, 71.09] | <0.001 | [141,973, 50,275], [17, 262] |
| Uterine rupture | 23.13 [13.28, 40.29] | <0.001 | [141,976, 50,422], [14, 115] | |
| Placenta Accreta | 14.05 [5.38, 36.71] | <0.001 | [141,985, 50,512], [5, 25] | |
| Massive antenatal/intrapartum bleeding | 8.71 [5.32, 14.24] | <0.001 | [141,969, 50,472], [21, 65] | |
| PPH | 2.32 [2.24, 2.41] | <0.001 | [135,199, 45,254], [6791, 5283] | |
| Blood products transfusion | 3.74 [3.41, 4.11] | <0.001 | [141,203, 49,504], [787, 1033] | |
| Re Laparotomy | 2.14 [1.79, 2.55] | <0.001 | [141,703, 50,319], [287, 218] | |
| Uterine atony | 1.56 [1.21, 2.03] | 0.007 | [141,830, 50,448], [160, 89] | |
| NICU admission | 5.26 [4.96, 5.56] | <0.001 | [140,079, 47,156], [1911, 3381] | |
| Severe neonatal complications | Meconium aspiration | 7.59 [5.71, 10.09] | <0.001 | [141,925, 50,362], [65, 175] |
| Infection | 5.56 [4.20, 7.35] | <0.001 | [141,916, 50,391], [74, 146] | |
| Hypoxic ischemic encephalopathy (high grade) | 3.36 [2.76, 4.07] | <0.001 | [141,801, 50,312], [189, 225] | |
| Chromosomal anomaly | 3.14 [2.48, 3.99] | <0.001 | [141,862, 50,394], [128, 143] | |
| GIT complications | 2.41 [1.54, 3.76] | 0.001 | [141,948, 50,501], [42, 36] | |
| Electrolytes disorders | 2.81 [1.58, 5.01] | 0.005 | [141,967, 50,514], [23, 23] | |
| Congenital malformations | 1.28 [1.14, 1.45] | 0.001 | [141,142, 50,151], [848, 386] | |
| Apgar scores | 1′-Apgar1 ≤ 7 | 3.95 [3.75, 4.16] | <0.001 | [139,396, 47,076], [2594, 3461] |
| 5′-Apgar ≤ 7 | 1.84 [1.70, 1.99] | <0.001 | [140,286, 49,432], [1704, 1105] | |
| Congenital disorders | Chromosomal (numeric) | 3.26 [2.52, 4.21] | <0.001 | [141,882, 50,412], [108, 125] |
| Genetic (non-numeric chromosomal and others) | 2.91 [1.75, 4.84] | <0.001 | [141,961, 50,507], [29, 30] | |
| SGA | 1.58 [1.52, 1.65] | <0.001 | [134,186, 46,273], [7804, 4264] | |
| Pediatric re-admission | ≤7 days | 2.31 [1.91, 2.78] | <0.001 | [141,747, 50,338], [243, 199] |
| ≤14 days | 2.43 [2.09, 2.82] | <0.001 | [141,615, 50,214], [375, 323] | |
| ≤21 days | 2.47 [2.14, 2.85] | <0.001 | [141,580, 50,178], [410, 359] | |
| ≤42 days | 2.34 [2.06, 2.67] | <0.001 | [141,494, 50,125], [496, 412] | |
| ≤90 days | 2.11 [1.87, 2.37] | <0.001 | [141,348, 50,058], [642, 479] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Talisman, S.; Guedalia, J.; Farkash, R.; Avitan, T.; Srebnik, N.; Kasirer, Y.; Schimmel, M.S.; Ghanem, D.; Unger, R.; Grisaru Granovsky, S. NICU Admission for Term Neonates in a Large Single-Center Population: A Comprehensive Assessment of Risk Factors Using a Tandem Analysis Approach. J. Clin. Med. 2022, 11, 4258. https://doi.org/10.3390/jcm11154258
Talisman S, Guedalia J, Farkash R, Avitan T, Srebnik N, Kasirer Y, Schimmel MS, Ghanem D, Unger R, Grisaru Granovsky S. NICU Admission for Term Neonates in a Large Single-Center Population: A Comprehensive Assessment of Risk Factors Using a Tandem Analysis Approach. Journal of Clinical Medicine. 2022; 11(15):4258. https://doi.org/10.3390/jcm11154258
Chicago/Turabian StyleTalisman, Shahar, Joshua Guedalia, Rivka Farkash, Tehila Avitan, Naama Srebnik, Yair Kasirer, Michael S. Schimmel, Dunia Ghanem, Ron Unger, and Sorina Grisaru Granovsky. 2022. "NICU Admission for Term Neonates in a Large Single-Center Population: A Comprehensive Assessment of Risk Factors Using a Tandem Analysis Approach" Journal of Clinical Medicine 11, no. 15: 4258. https://doi.org/10.3390/jcm11154258
APA StyleTalisman, S., Guedalia, J., Farkash, R., Avitan, T., Srebnik, N., Kasirer, Y., Schimmel, M. S., Ghanem, D., Unger, R., & Grisaru Granovsky, S. (2022). NICU Admission for Term Neonates in a Large Single-Center Population: A Comprehensive Assessment of Risk Factors Using a Tandem Analysis Approach. Journal of Clinical Medicine, 11(15), 4258. https://doi.org/10.3390/jcm11154258