
Optimal Arterial Blood Gas Tensions for the Prognosis of Favorable Neurological Outcomes in Survivors after Extracorporeal Cardiopulmonary Resuscitation


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Variables
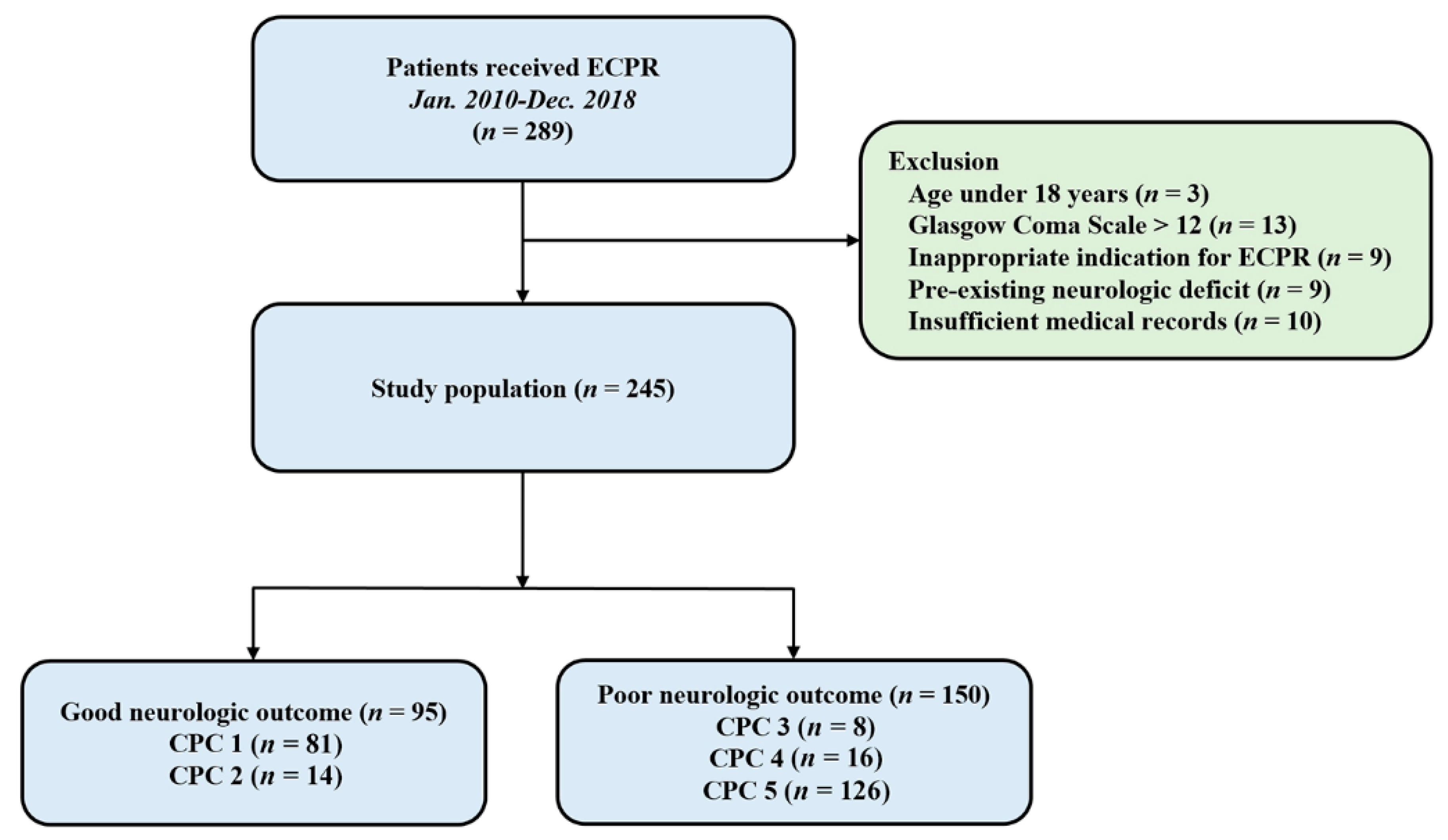
2.2. Study Population
2.3. Data Collection Process
2.4. Statistical Analyses
3. Results
3.1. Baseline Characteristics and Clinical Outcomes
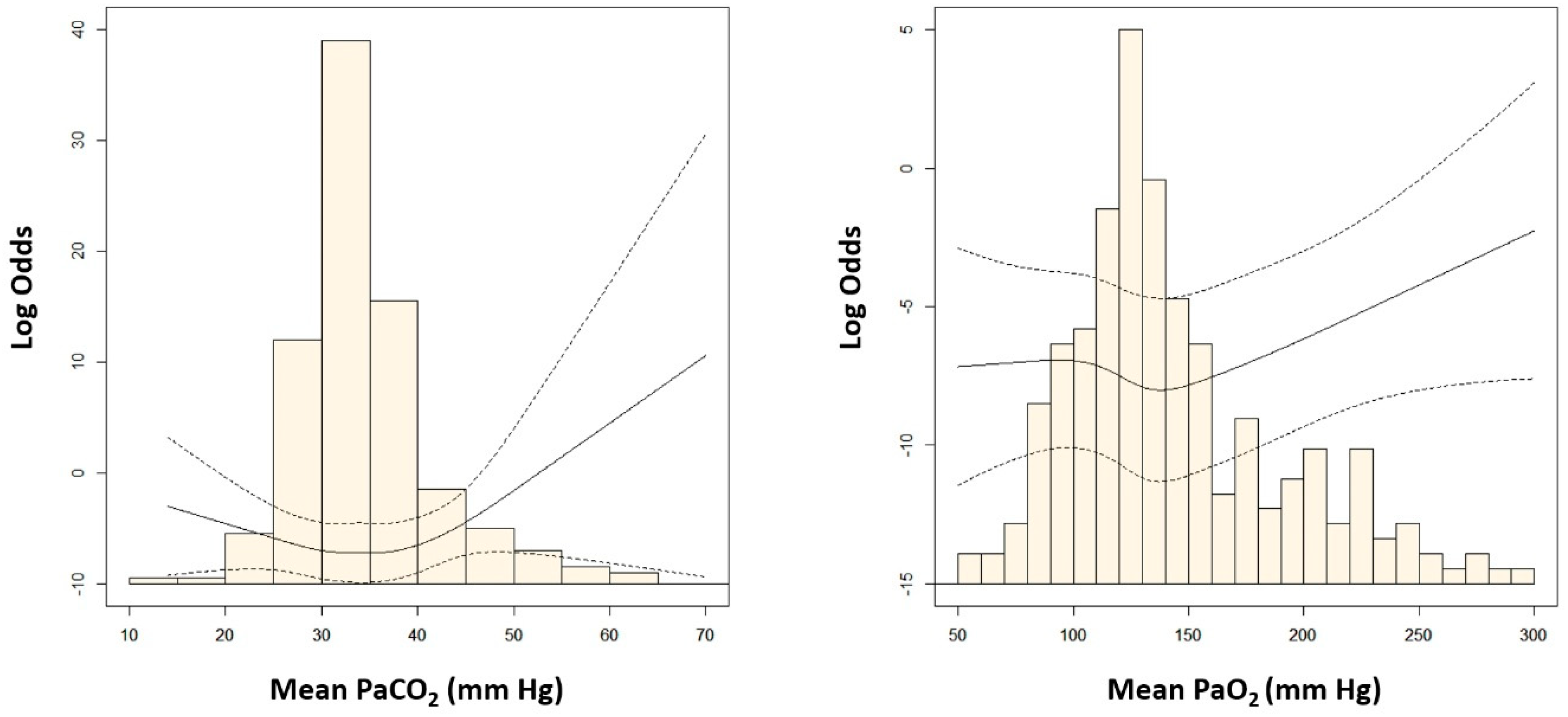
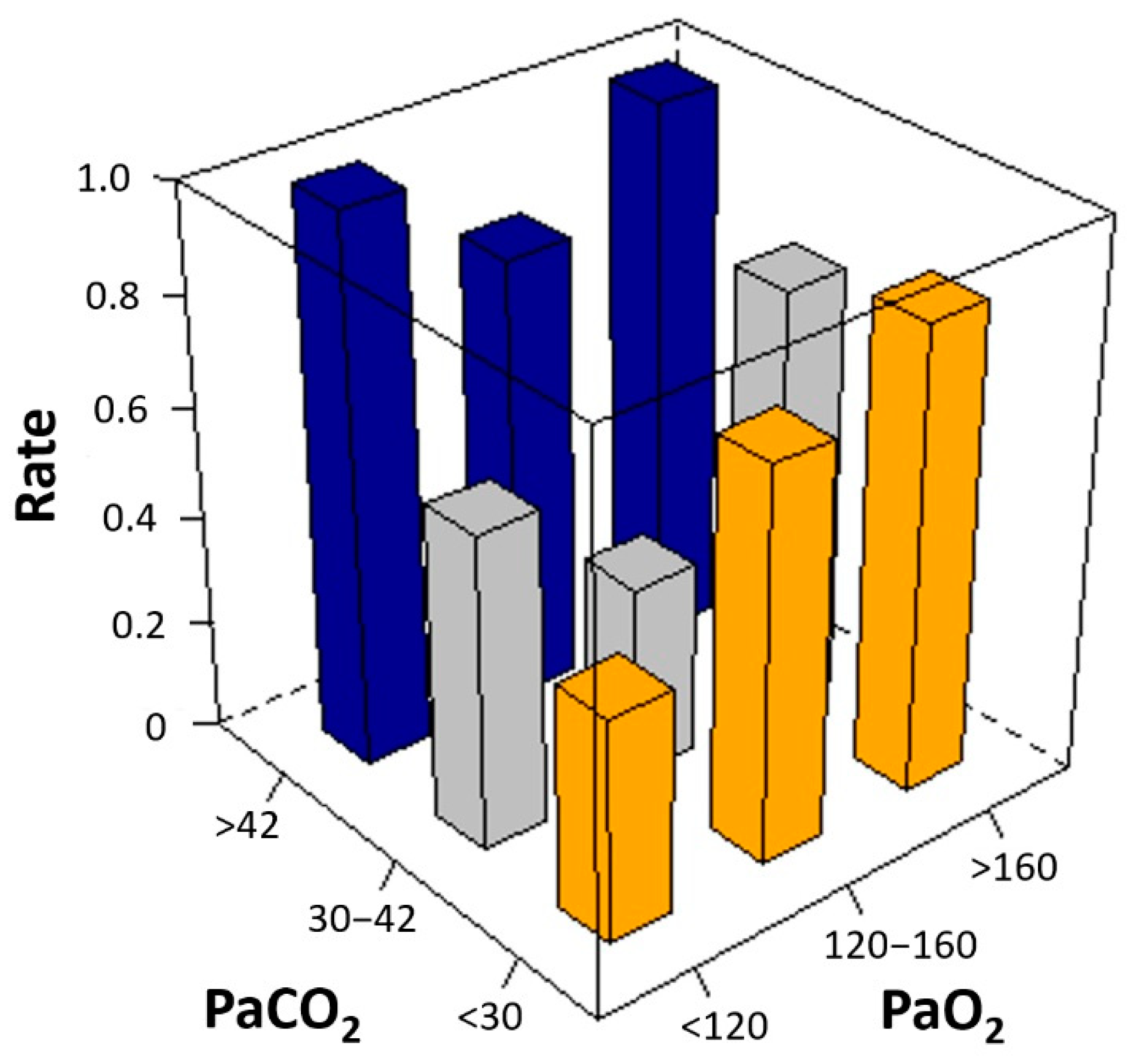
3.2. The Relationship between Mean Arterial Blood Gas Tensions and Neurologic Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Ryu, J.A.; Chung, C.R.; Cho, Y.H.; Sung, K.; Jeon, K.; Suh, G.Y.; Park, T.K.; Lee, J.M.; Song, Y.B.; Hahn, J.Y.; et al. Neurologic Outcomes in Patients Who Undergo Extracorporeal Cardiopulmonary Resuscitation. Ann. Thorac. Surg. 2019, 108, 749–755. [Google Scholar] [CrossRef] [PubMed]
- Panchal, A.R.; Bartos, J.A.; Cabañas, J.G.; Donnino, M.W.; Drennan, I.R.; Hirsch, K.G.; Kudenchuk, P.J.; Kurz, M.C.; Lavonas, E.J.; Morley, P.T.; et al. Part 3: Adult Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2020, 142, S366–S468. [Google Scholar] [CrossRef] [PubMed]
- Nolan, J.P.; Sandroni, C.; Böttiger, B.W.; Cariou, A.; Cronberg, T.; Friberg, H.; Genbrugge, C.; Haywood, K.; Lilja, G.; Moulaert, V.R.M.; et al. European Resuscitation Council and European Society of Intensive Care Medicine guidelines 2021: Post-resuscitation care. Intensive Care Med. 2021, 47, 369–421. [Google Scholar] [CrossRef] [PubMed]
- Nolan, J.P.; Soar, J.; Zideman, D.A.; Biarent, D.; Bossaert, L.L.; Deakin, C.; Koster, R.W.; Wyllie, J.; Böttiger, B. European Resuscitation Council Guidelines for Resuscitation 2010 Section 1. Executive summary. Resuscitation 2010, 81, 1219–1276. [Google Scholar] [CrossRef]
- Hazinski, M.F.; Nolan, J.P.; Billi, J.E.; Böttiger, B.W.; Bossaert, L.; de Caen, A.R.; Deakin, C.D.; Drajer, S.; Eigel, B.; Hickey, R.W.; et al. Part 1: Executive summary: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation 2010, 122, S250–S275. [Google Scholar] [CrossRef] [Green Version]
- Helmerhorst, H.J.; Roos-Blom, M.J.; van Westerloo, D.J.; Abu-Hanna, A.; de Keizer, N.F.; de Jonge, E. Associations of arterial carbon dioxide and arterial oxygen concentrations with hospital mortality after resuscitation from cardiac arrest. Crit. Care 2015, 19, 348. [Google Scholar] [CrossRef] [Green Version]
- Schneider, A.G.; Eastwood, G.M.; Bellomo, R.; Bailey, M.; Lipcsey, M.; Pilcher, D.; Young, P.; Stow, P.; Santamaria, J.; Stachowski, E.; et al. Arterial carbon dioxide tension and outcome in patients admitted to the intensive care unit after cardiac arrest. Resuscitation 2013, 84, 927–934. [Google Scholar] [CrossRef]
- Balan, I.S.; Fiskum, G.; Hazelton, J.; Cotto-Cumba, C.; Rosenthal, R.E. Oximetry-guided reoxygenation improves neurological outcome after experimental cardiac arrest. Stroke 2006, 37, 3008–3013. [Google Scholar] [CrossRef] [Green Version]
- Kety, S.S.; Schmidt, C.F. The effects of altered arterial tensions of carbon dioxide and oxygen on cerebral blood flow and cerebral oxygen consumption of normal young men. J. Clin. Investig. 1948, 27, 484–492. [Google Scholar] [CrossRef]
- Sundgreen, C.; Larsen, F.S.; Herzog, T.M.; Knudsen, G.M.; Boesgaard, S.; Aldershvile, J. Autoregulation of cerebral blood flow in patients resuscitated from cardiac arrest. Stroke 2001, 32, 128–132. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.I.; Ko, R.E.; Yang, J.H.; Cho, Y.H.; Ahn, J.; Ryu, J.A. Optimal Mean Arterial Pressure for Favorable Neurological Outcomes in Survivors after Extracorporeal Cardiopulmonary Resuscitation. J. Clin. Med. 2022, 11, 290. [Google Scholar] [CrossRef]
- Ryu, J.A.; Chung, C.R.; Cho, Y.H.; Sung, K.; Suh, G.Y.; Park, T.K.; Song, Y.B.; Hahn, J.Y.; Choi, J.H.; Gwon, H.C.; et al. The association of findings on brain computed tomography with neurologic outcomes following extracorporeal cardiopulmonary resuscitation. Crit. Care 2017, 21, 15. [Google Scholar] [CrossRef] [Green Version]
- Ryu, J.A.; Park, T.K.; Chung, C.R.; Cho, Y.H.; Sung, K.; Suh, G.Y.; Lee, T.R.; Sim, M.S.; Yang, J.H. Association between Body Temperature Patterns and Neurological Outcomes after Extracorporeal Cardiopulmonary Resuscitation. PLoS ONE 2017, 12, e0170711. [Google Scholar] [CrossRef] [Green Version]
- Vaahersalo, J.; Bendel, S.; Reinikainen, M.; Kurola, J.; Tiainen, M.; Raj, R.; Pettila, V.; Varpula, T.; Skrifvars, M.B.; Group, F.S. Arterial blood gas tensions after resuscitation from out-of-hospital cardiac arrest: Associations with long-term neurologic outcome. Crit. Care Med. 2014, 42, 1463–1470. [Google Scholar] [CrossRef]
- Roberts, B.W.; Kilgannon, J.H.; Chansky, M.E.; Mittal, N.; Wooden, J.; Trzeciak, S. Association between postresuscitation partial pressure of arterial carbon dioxide and neurological outcome in patients with post-cardiac arrest syndrome. Circulation 2013, 127, 2107–2113. [Google Scholar] [CrossRef] [Green Version]
- Peluso, L.; Belloni, I.; Calabro, L.; Dell’Anna, A.M.; Nobile, L.; Creteur, J.; Vincent, J.L.; Taccone, F.S. Oxygen and carbon dioxide levels in patients after cardiac arrest. Resuscitation 2020, 150, 1–7. [Google Scholar] [CrossRef]
- Wang, H.E.; Prince, D.K.; Drennan, I.R.; Grunau, B.; Carlbom, D.J.; Johnson, N.; Hansen, M.; Elmer, J.; Christenson, J.; Kudenchuk, P.; et al. Post-resuscitation arterial oxygen and carbon dioxide and outcomes after out-of-hospital cardiac arrest. Resuscitation 2017, 120, 113–118. [Google Scholar] [CrossRef]
- Muizelaar, J.P.; Marmarou, A.; Ward, J.D.; Kontos, H.A.; Choi, S.C.; Becker, D.P.; Gruemer, H.; Young, H.F. Adverse effects of prolonged hyperventilation in patients with severe head injury: A randomized clinical trial. J. Neurosurg. 1991, 75, 731–739. [Google Scholar] [CrossRef]
- Hutin, A.; Abu-Habsa, M.; Burns, B.; Bernard, S.; Bellezzo, J.; Shinar, Z.; Torres, E.C.; Gueugniaud, P.Y.; Carli, P.; Lamhaut, L. Early ECPR for out-of-hospital cardiac arrest: Best practice in 2018. Resuscitation 2018, 130, 44–48. [Google Scholar] [CrossRef]
- Douzinas, E.E.; Patsouris, E.; Kypriades, E.M.; Makris, D.J.; Andrianakis, I.; Korkolopoulou, P.; Boursinos, V.; Papalois, A.; Sotiropoulou, C.; Davaris, P.; et al. Hypoxaemic reperfusion ameliorates the histopathological changes in the pig brain after a severe global cerebral ischaemic insult. Intensive Care Med. 2001, 27, 905–910. [Google Scholar] [CrossRef]
- Becker, L.B. New concepts in reactive oxygen species and cardiovascular reperfusion physiology. Cardiovasc. Res. 2004, 61, 461–470. [Google Scholar] [CrossRef]
- Bonnemain, J.; Rusca, M.; Ltaief, Z.; Roumy, A.; Tozzi, P.; Oddo, M.; Kirsch, M.; Liaudet, L. Hyperoxia during extracorporeal cardiopulmonary resuscitation for refractory cardiac arrest is associated with severe circulatory failure and increased mortality. BMC Cardiovasc. Disord. 2021, 21, 542. [Google Scholar] [CrossRef]
- Chang, W.T.; Wang, C.H.; Lai, C.H.; Yu, H.Y.; Chou, N.K.; Wang, C.H.; Huang, S.C.; Tsai, P.R.; Chou, F.J.; Tsai, M.S.; et al. Optimal Arterial Blood Oxygen Tension in the Early Postresuscitation Phase of Extracorporeal Cardiopulmonary Resuscitation: A 15-Year Retrospective Observational Study. Crit. Care Med. 2019, 47, 1549–1556. [Google Scholar] [CrossRef]
- Halter, M.; Jouffroy, R.; Saade, A.; Philippe, P.; Carli, P.; Vivien, B. Association between hyperoxemia and mortality in patients treated by eCPR after out-of-hospital cardiac arrest. Am. J. Emerg. Med. 2020, 38, 900–905. [Google Scholar] [CrossRef]
- Eastwood, G.M.; Schneider, A.G.; Suzuki, S.; Peck, L.; Young, H.; Tanaka, A.; Martensson, J.; Warrillow, S.; McGuinness, S.; Parke, R.; et al. Targeted therapeutic mild hypercapnia after cardiac arrest: A phase II multi-centre randomised controlled trial (the CCC trial). Resuscitation 2016, 104, 83–90. [Google Scholar] [CrossRef]
- Sekhon, M.S.; Ainslie, P.N.; Griesdale, D.E. Clinical pathophysiology of hypoxic ischemic brain injury after cardiac arrest: A “two-hit” model. Crit. Care 2017, 21, 90. [Google Scholar] [CrossRef] [Green Version]
- Arlt, M.; Philipp, A.; Voelkel, S.; Schopka, S.; Husser, O.; Hengstenberg, C.; Schmid, C.; Hilker, M. Early experiences with miniaturized extracorporeal life-support in the catheterization laboratory. Eur. J. Cardiothorac. Surg. 2012, 42, 858–863. [Google Scholar] [CrossRef]
- Goyal, V. ECPR in the cath lab. Qatar. Med. J. 2017, 1, 28. [Google Scholar] [CrossRef]
- Ko, R.E.; Ryu, J.A.; Cho, Y.H.; Sung, K.; Jeon, K.; Suh, G.Y.; Park, T.K.; Lee, J.M.; Song, Y.B.; Hahn, J.Y.; et al. The differential neurologic prognosis of low-flow time according to the initial rhythm in patients who undergo extracorporeal cardiopulmonary resuscitation. Resuscitation 2020, 148, 121–127. [Google Scholar] [CrossRef]
- Kagawa, E.; Inoue, I.; Kawagoe, T.; Ishihara, M.; Shimatani, Y.; Kurisu, S.; Nakama, Y.; Dai, K.; Takayuki, O.; Ikenaga, H.; et al. Assessment of outcomes and differences between in- and out-of-hospital cardiac arrest patients treated with cardiopulmonary resuscitation using extracorporeal life support. Resuscitation 2010, 81, 968–973. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Favorable
Neurological Outcome (n = 95) | Poor
Neurological Outcome (n = 150) | p-Value | |
|---|---|---|---|
| Age (years) | 56.6 ± 15.4 | 60.1 ± 15.8 | 0.089 |
| Gender, male | 73 (76.8) | 103 (68.7) | 0.215 |
| Comorbidities | |||
| Hypertension | 45 (47.4) | 73 (48.7) | 0.947 |
| Diabetes mellitus | 32 (33.7) | 54 (36.0) | 0.816 |
| Previous myocardial infarction | 22 (23.2) | 34 (22.7) | 0.999 |
| Current smoker | 21 (22.1) | 24 (16.0) | 0.302 |
| Malignancy | 13 (13.7) | 30 (20.0) | 0.274 |
| Chronic kidney disease a | 8 (8.4) | 26 (17.3) | 0.076 |
| Dyslipidemia | 15 (15.8) | 17 (11.3) | 0.416 |
| CPR details | |||
| Type of cardiac arrest | 0.033 | ||
| Out of hospital cardiac arrest | 9 (9.5) | 31 (20.7) | |
| In-hospital cardiac arrest | 86 (90.5) | 119 (79.3) | |
| First monitored rhythm | 0.006 | ||
| Asystole | 6 (6.3) | 30 (20.0) | |
| Pulseless electrical activity | 47 (49.5) | 74 (49.3) | |
| Shockable rhythm (VT or VF) | 42 (44.2) | 46 (30.7) | |
| CPR duration (min) | 16.63 ± 14.42 | 33.13 ± 21.37 | <0.001 |
| Cardiac cause of arrest | 0.015 | ||
| Ischemic | 54 (56.8) | 58 (38.7) | |
| Non-ischemic | 17 (17.9) | 31 (20.7) | |
| Management in the intensive care unit | |||
| Targeted temperature management | 18 (18.9) | 30 (20.0) | 0.970 |
| Arctic Sun | 10 (10.5) | 24 (16.0) | |
| Cooling pad | 8 (8.4) | 6 (4.0) | |
| Intra-aortic balloon pump | 10 (10.5) | 8 (5.3) | 0.205 |
| Renal replacement therapy | 26 (27.4) | 83 (55.3) | <0.001 |
| Location of ECPR | <0.001 | ||
| Cardiac catheterization lab | 39 (41.1) | 24 (16.0) | |
| Intensive care unit | 29 (30.5) | 74 (49.3) | |
| Emergency department | 22 (23.2) | 45 (30.0) | |
| Others (operation room, general wards, etc.) | 5 (5.3) | 7 (4.7) |
| Mean Blood Gas Tension (mm Hg) | Favorable Neurological Outcome (n = 95) | Poor Neurological Outcome (n = 150) | p-Value |
|---|---|---|---|
| PaCO2 | 33.19 ± 4.06 | 36.71 ± 14.41 | 0.005 |
| Tertile of mean PaCO2 | <0.001 | ||
| First tertile (<30) | 18 (18.9) | 37 (24.7) | |
| Second tertile (30–42) | 75 (78.9) | 84 (56.0) | |
| Third tertile (>42) | 2 (2.1) | 29 (19.3) | |
| PaO2 | 131.68 ± 30.91 | 148.40 ± 55.19 | 0.003 |
| Tertile of mean PaO2 | <0.001 | ||
| First tertile (<120) | 32 (33.7) | 49 (32.7) | |
| Second tertile (120–160) | 52 (54.7) | 47 (31.3) | |
| Third tertile (>160) | 11 (11.6) | 54 (36.0) |
| Adjusted OR (95% CI) | p-Value | |
|---|---|---|
| Tertile of mean PaCO2 | ||
| First tertile (<30 mm Hg) | 1 | Reference |
| Second tertile (30–42 mm Hg) | 0.51 (0.205–1.283) | 0.148 |
| Third tertile (>42 mm Hg) | 12.02 (1.703–84.760) | 0.012 |
| Tertile of mean PaO2 | ||
| First tertile (<120 mm Hg) | 1 | Reference |
| Second tertile (120–160 mm Hg) | 0.50 (0.223–1.107) | 0.083 |
| Third tertile (>160 mm Hg) | 2.85 (1.043–7.804) | 0.039 |
| Age (years) | 1.05 (1.021–1.076) | <0.001 |
| First monitored rhythm | ||
| Asystole | 1 | Reference |
| Pulseless electrical activity | 0.31 (0.092–1.056) | 0.058 |
| Shockable rhythm (VT or VF) | 0.16 (0.047–0.555) | 0.003 |
| Out of hospital cardiac arrest | 3.13 (1.074–9.133) | 0.034 |
| CPR duration a | 3.57 (2.263–5.616) | <0.001 |
| ECMO insertion in cardiac catheterization lab | 0.17 (0.069–0.409) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hong, S.; Jang, J.H.; Yang, J.H.; Cho, Y.H.; Ahn, J.; Ryu, J.-A. Optimal Arterial Blood Gas Tensions for the Prognosis of Favorable Neurological Outcomes in Survivors after Extracorporeal Cardiopulmonary Resuscitation. J. Clin. Med. 2022, 11, 4211. https://doi.org/10.3390/jcm11144211
Hong S, Jang JH, Yang JH, Cho YH, Ahn J, Ryu J-A. Optimal Arterial Blood Gas Tensions for the Prognosis of Favorable Neurological Outcomes in Survivors after Extracorporeal Cardiopulmonary Resuscitation. Journal of Clinical Medicine. 2022; 11(14):4211. https://doi.org/10.3390/jcm11144211
Chicago/Turabian StyleHong, SungMin, Ji Hoon Jang, Jeong Hoon Yang, Yang Hyun Cho, Joonghyun Ahn, and Jeong-Am Ryu. 2022. "Optimal Arterial Blood Gas Tensions for the Prognosis of Favorable Neurological Outcomes in Survivors after Extracorporeal Cardiopulmonary Resuscitation" Journal of Clinical Medicine 11, no. 14: 4211. https://doi.org/10.3390/jcm11144211
APA StyleHong, S., Jang, J. H., Yang, J. H., Cho, Y. H., Ahn, J., & Ryu, J.-A. (2022). Optimal Arterial Blood Gas Tensions for the Prognosis of Favorable Neurological Outcomes in Survivors after Extracorporeal Cardiopulmonary Resuscitation. Journal of Clinical Medicine, 11(14), 4211. https://doi.org/10.3390/jcm11144211