
Influenza Myopericarditis and Pericarditis: A Literature Review

 ,
,  ,
,  ,
,  and
and
Abstract
1. Introduction
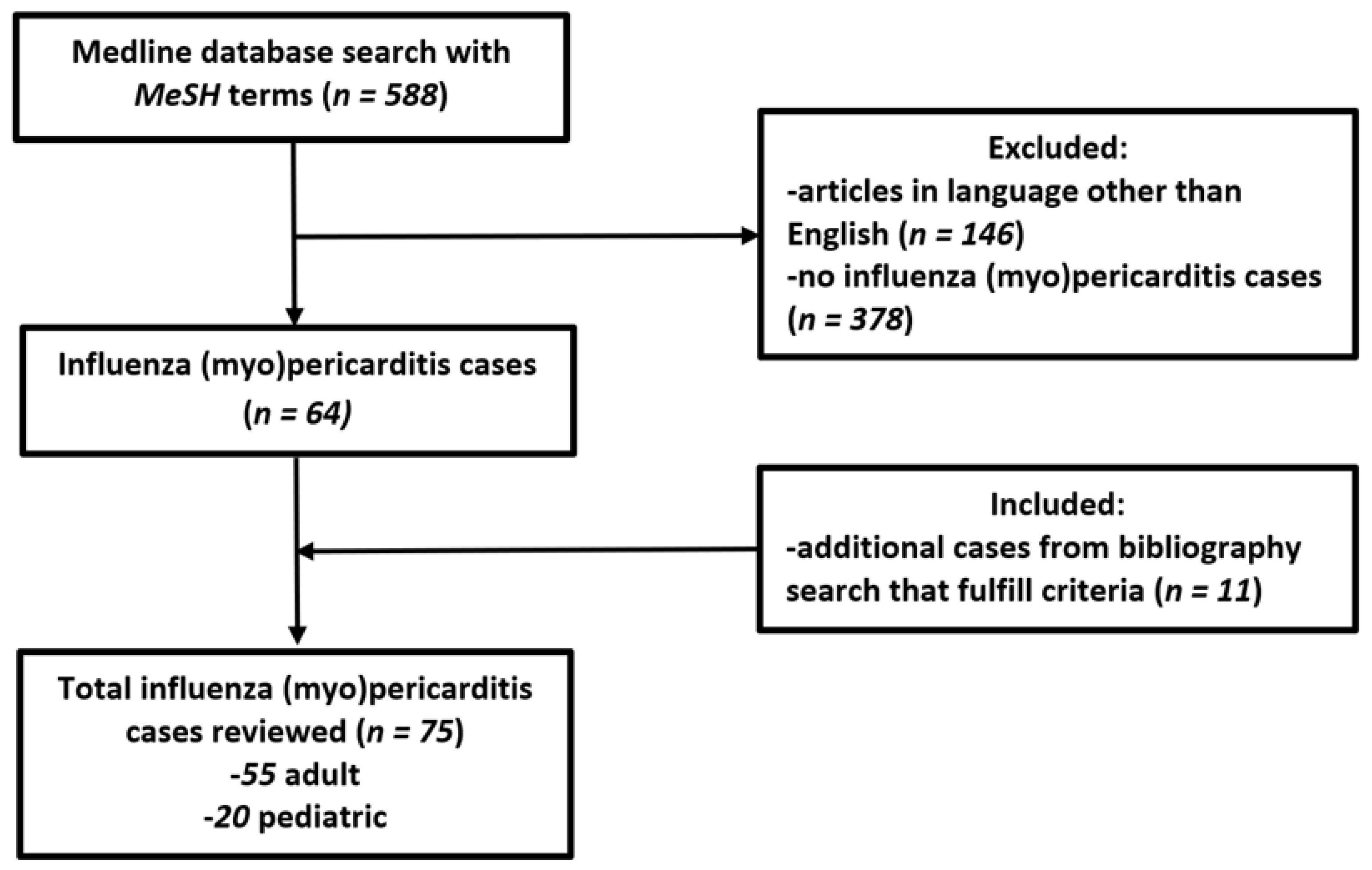
2. Materials and Methods
3. Results
3.1. Demographics
3.2. Presentation
3.3. Evaluation
3.4. Treatment and Interventions
3.5. Complications and Outcome
4. Discussion
4.1. Presentation and Diagnostics
4.2. Treatment and Prevention
4.3. Complications and Outcomes
5. Conclusions
6. Limitations of the Study
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Rezkalla, S.H.; Kloner, R.A. Viral myocarditis: 1917–2020: From the Influenza A to the COVID-19 pandemics. Trends Cardiovasc. Med. 2021, 31, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Lefeuvre, C.; Behillil, S.; Triau, S.; Monteiro-Rodrigues, A.; Templier, F.; Tran, C.T.; Le Guillou-Guillemette, H.; Lunel-Fabiani, F.; Enouf, V.; Ducancelle, A. Fatal Myopericarditis Following an Influenza A (H3N2) Infection. Am. J. Case. Rep. 2018, 19, 540–544. [Google Scholar] [CrossRef] [PubMed]
- Morens, D.M.; Taubenberger, J.K. Influenza Cataclysm, 1918. N. Engl. J. Med. 2018, 379, 2285–2287. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, T.; Mamahit, A.; Cox, N.J. 65 years of influenza surveillance by a World Health Organization-coordinated global network. Influenza Other Respir. Viruses 2018, 12, 558–565. [Google Scholar] [CrossRef] [PubMed]
- Cooper, L.T., Jr. Myocarditis. N. Engl. J. Med. 2009, 360, 1526–1538. [Google Scholar] [CrossRef]
- Imazio, M.; Trinchero, R. Myopericarditis: Etiology, management, and prognosis. Int. J. Cardiol. 2008, 127, 17–26. [Google Scholar] [CrossRef]
- Imazio, M.; Cooper, L.T. Management of myopericarditis. Expert Rev. Cardiovasc. Ther. 2013, 11, 193–201. [Google Scholar] [CrossRef]
- Manda, Y.R.; Baradhi, K.M. Myopericarditis. In StatPearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2022. [Google Scholar]
- Adler, Y.; Charron, P.; Imazio, M.; Badano, L.; Barón-Esquivias, G.; Bogaert, J.; Brucato, A.; Gueret, P.; Klingel, K.; Lionis, C.; et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC)Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2015, 36, 2921–2964. [Google Scholar]
- Dolader, P.; Balcells, J.; Gran, F. Influenza myocarditis in paediatric patients. Cardiol. Young 2021, 32, 1–3. [Google Scholar] [CrossRef]
- Mamas, M.A.; Fraser, D.; Neyses, L. Cardiovascular manifestations associated with influenza virus infection. Int. J. Cardiol. 2008, 130, 304–309. [Google Scholar] [CrossRef]
- Tseng, G.S.; Hsieh, C.Y.; Hsu, C.T.; Lin, J.C.; Chan, J.S. Myopericarditis and exertional rhabdomyolysis following an influenza A (H3N2) infection. BMC Infect. Dis. 2013, 13, 283. [Google Scholar] [CrossRef] [PubMed]
- Rezkalla, S.H.; Kloner, R.A. Influenza-related viral myocarditis. WMJ 2010, 109, 209–213. [Google Scholar] [PubMed]
- Baral, N.; Adhikari, P.; Adhikari, G.; Karki, S. Influenza Myocarditis: A Literature Review. Cureus 2020, 12, e12007. [Google Scholar] [CrossRef]
- Sellers, S.A.; Hagan, R.S.; Hayden, F.G.; Fischer, W.A., 2nd. The hidden burden of influenza: A review of the extra-pulmonary complications of influenza infection. Influenza Other Respir. Viruses 2017, 11, 372–393. [Google Scholar] [CrossRef]
- Silva, E.; Montenegro, J.S.; Estupiñán, M.C.; Arias, G.; Osorio, J.P.; Poveda, C.M.; Buitrago, R. Fulminant myocarditis due to the influenza B virus in adults: Report of two cases and literature review. Biomedica 2019, 39 (Suppl. S2), 11–19. [Google Scholar] [CrossRef] [PubMed]
- Ukimura, A.; Satomi, H.; Ooi, Y.; Kanzaki, Y. Myocarditis Associated with Influenza A H1N1pdm2009. Influenza Res. Treat. 2012, 2012, 351979. [Google Scholar] [CrossRef]
- Kumar, K.; Guirgis, M.; Zieroth, S.; Lo, E.; Menkis, A.H.; Arora, R.C.; Freed, D.H. Influenza myocarditis and myositis: Case presentation and review of the literature. Can. J. Cardiol. 2011, 27, 514–522. [Google Scholar] [CrossRef]
- Schroff, P.; Hovey, J.R.; Tharumia Jagadeesan, C.; Nagalapuram, V.; Chaucer, B. Cardiac Tamponade Secondary to Influenza B Infection. Cureus 2021, 13, e14888. [Google Scholar] [CrossRef]
- Ebert, D.; Mungard, N.; Mensch, A.; Homeister, L.; Willsch, J.; Ibe, R.; Baust, H.; Stiller, M.; Rebelo, A.; Ukkat, J.; et al. Cardiogenic shock with highly complicated course after influenza A virus infection treated with vva-ECMO and Impella CP (ECMELLA): A case report. BMC Cardiovasc. Disord. 2021, 21, 528. [Google Scholar] [CrossRef]
- Arfaras-Melainis, A.; Cordero, H.; Goyal, A.; Benes, L.; Salgunan, R. Acute Influenza B Infection Presenting as Cardiac Tamponade: A Case Report. Cureus 2020, 12, e11799. [Google Scholar] [CrossRef]
- Giafaglione, J.R.; Morrison, A.K.; Nandi, D. A case report of myocarditis masquerading as hypertrophic cardiomyopathy. Ann. Pediatr. Cardiol. 2020, 13, 340–342. [Google Scholar] [CrossRef] [PubMed]
- Spoto, S.; Valeriani, E.; Locorriere, L.; Anguissola, G.B.; Pantano, A.L.; Terracciani, F.; Riva, E.; Ciccozzi, M.; Costantino, S.; Angeletti, S. Influenza B virus infection complicated by life-threatening pericarditis: A unique case-report and literature review. BMC Infect. Dis. 2019, 19, 40. [Google Scholar] [CrossRef] [PubMed]
- Pandey, Y.; Hasan, R.; Joshi, K.P.; Habash, F.J.; Jagana, R. Acute Influenza Infection Presenting with Cardiac Tamponade: A Case Report and Review of Literature. Perm. J. 2019, 23, 18–104. [Google Scholar] [CrossRef] [PubMed]
- Hollowed, J.; Nsair, A. Influenza A (H3N2) Induced Fulminant Myocarditis Requiring Mechanical Circulatory Support. JACC Case Rep 2019, 1, 133–137. [Google Scholar] [CrossRef]
- Jiménez-Méndez, C.; Díez-Villanueva, P.; Bastante, T.; Cuerda, F.; Segovia, J.; Alfonso, F. Venoarterial extracorporeal membrane oxygenation as a bridge to recovery in refractory cardiogenic shock secondary to fulminant influenza A myocarditis complicated with cardiac tamponade. Arch. Cardiol. Mex. 2020, 90, 216–218. [Google Scholar] [CrossRef]
- Thomas, T.P.; Kumar, S.; Anand, A.; Kiran, R.; Sabu, V.; Gaffoor, A. A Rare Presentation of Fulminant Viral Myocarditis Associated with H1N1: A Series of Four Cases. Indian J. Crit. Care Med. 2019, 23, 538–541. [Google Scholar] [CrossRef]
- Mazzitelli, M.; Garofalo, E.; Bruni, A.; Barreca, G.S.; Quirino, A.; Giancotti, A.; Serapide, F.; Indolfi, C.; Matera, G.; Navalesi, P.; et al. Severe myocarditis due to influenza A(H1N1)pdm09 viral infection in a young woman successfully treated with intravenous zanamivir: A case report. Clin. Case Rep. 2019, 7, 2336–2340. [Google Scholar] [CrossRef]
- Ciabatti, M.; Vignini, E.; Mattesini, A.; Di Mario, C.; Valente, S. Why can flu be so deadly? An unusual case of cardiogenic shock. Intern. Emerg. Med. 2020, 15, 679–684. [Google Scholar] [CrossRef]
- Hashmi, A.T.; Yousuf, M.S.; Waseem, H.; Ambesh, P.; Rodriguez, D.; Adzic, A. Cardiogenic Shock: A Rare Complication of Influenza. Cureus 2018, 10, e2549. [Google Scholar] [CrossRef]
- Roto, D.; Malnoske, M.L.; Winters, S.; Georas, S.N. A Fatal Case of Influenza B Myocarditis with Cardiac Tamponade. Case Rep. Crit. Care 2018, 2018, 8026314. [Google Scholar] [CrossRef]
- Hékimian, G.; Jovanovic, T.; Bréchot, N.; Lebreton, G.; Leprince, P.; Trouillet, J.L.; Schmidt, M.; Nieszkowska, A.; Besset, S.; Chastre, J.; et al. When the heart gets the flu: Fulminant influenza B myocarditis: A case-series report and review of the literature. J. Crit. Care 2018, 47, 61–64. [Google Scholar] [CrossRef] [PubMed]
- Piccininni, J.A.; Richmond, M.E.; Cheung, E.W.; Lee, T.M.; Law, S.P.; Addonizio, L.J.; Zuckerman, W.A. Influenza Myocarditis Treated With Antithymocyte Globulin. Pediatrics 2018, 142, e20180884. [Google Scholar] [CrossRef] [PubMed]
- Siskin, M.; Rao, S.; Rapkiewicz, A.; Bangalore, S.; Garshick, M. A Case of Cardiogenic Shock Secondary to Complement-Mediated Myopericarditis From Influenza B Infection. Can. J. Cardiol. 2017, 33, 1335.e1–1335.e3. [Google Scholar] [CrossRef] [PubMed]
- Allyn, J.; Brottet, E.; Antok, E.; Dangers, L.; Persichini, R.; Coolen-Allou, N.; Roquebert, B.; Allou, N.; Vandroux, D. Case Report: Severe Imported Influenza Infections Developed during Travel in Reunion Island. Am. J. Trop. Med. Hyg. 2017, 97, 1943–1944. [Google Scholar] [CrossRef] [PubMed][Green Version]
- McCormick, A.D.; Censoplano, N.; Schumacher, K.R. Fulminant Influenza B Myocarditis in a Pediatric Patient. J. Pediatr. Intensive Care 2017, 6, 209–213. [Google Scholar]
- Cárdenes León, A.; Gallardo Santos, E.; Prada Osorio, R.; López Pérez, M.; Martín Lorenzo, P.L. Cardiogenic Shock and Cardiac Tamponade in the Context of Influenza A Myopericarditis. Rev. Esp. Cardiol. Engl. Ed. 2017, 70, 1149–1151. [Google Scholar] [CrossRef]
- Sidhu, R.S.; Sharma, A.; Paterson, I.D.; Bainey, K.R. Influenza H1N1 Infection Leading To Cardiac Tamponade in a Previously Healthy Patient: A Case Report. Res. Cardiovasc. Med. 2016, 5, e31546. [Google Scholar] [CrossRef]
- Davidović, G.; Simović, S.; Mitrović, S.; Irić-Ćupić, V.; Miloradović, V. Fulminant myocarditis as a primary manifestation of H1N1 infection: A first reported case from Serbia. Hellenic J. Cardiol. 2016, 57, 181–184. [Google Scholar] [CrossRef][Green Version]
- Van Diepen, K.M.; de Almeida, C.L.; Kam, A.J. An Interesting Case of Viral Pericarditis. Pediatr. Emerg. Care 2016, 32, 323–325. [Google Scholar] [CrossRef]
- Ito, N.; Sato, M.; Momoi, N.; Aoyagi, Y.; Endo, K.; Chishiki, M.; Kawasaki, Y.; Hosoya, M. Influenza A H1N1 pdm09-associated myocarditis during zanamivir therapy. Pediatr. Int. 2015, 57, 1172–1174. [Google Scholar] [CrossRef]
- Hawwa, N.; Popovic, Z.B.; Isma’eel, H.A. Discordant Electrocardiogram Left Ventricular Wall Thickness and Strain Findings in Influenza Myocarditis. Echocardiography 2015, 32, 1880–1884. [Google Scholar] [CrossRef] [PubMed]
- Martín-Lázaro, J.F.; Homs, C.; Benito, R.; Pedro, A.S.; Suárez, M.A. Chronic pericardial effusion secondary to a influenza virus A (H1N1)/2009 infection. Türk Kardiyol. Derneği Arşivi 2013, 41, 157–160. [Google Scholar]
- Knežević Praveček, M.; Hadžibegović, I.; Coha, B.; Samardžić, P.; Mišić, B.; Jandrić Balen, M. Pericardial effusion complicating swine origin influenzae A (H1N1) infection in a 50-year-old woman. Med. Glas 2013, 10, 173–176. [Google Scholar]
- Levenson, J.E.; Kaul, D.R.; Saint, S.; Nallamothu, B.K.; Gurm, H.S. Clinical problem-solving. A shocking development. N. Engl. J. Med. 2013, 369, 2253–2258. [Google Scholar] [CrossRef]
- Yoshimizu, N.; Tominaga, T.; Ito, T.; Nishida, Y.; Wada, Y.; Sohmiya, K.; Tanaka, S.; Shibata, K.; Kanzaki, Y.; Ukimura, A.; et al. Repetitive fulminant influenza myocarditis requiring the use of circulatory assist devices. Intern. Med. 2014, 53, 109–114. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Babamahmoodi, F.; Davoodi, A.R.; Ghasemian, R.; Delavarian, L. Report of two rare complications of pandemic influenza A (H1N1). J. Infect. Dev. Ctries. 2012, 6, 204–207. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.F.; Chiasson, D.A.; Smythe, J.F.; Sanatani, S. Recurrent congestive heart failure in a child due to probable myocarditis. Pediatr. Cardiol. 2012, 33, 176–181. [Google Scholar] [CrossRef]
- Davoudi, A.R.; Maleki, A.R.; Beykmohammadi, A.R.; Tayebi, A. Fulminant myopericarditis in an immunocompetent adult due to pandemic 2009 (H1N1) influenza A virus infection. Scand. J. Infect. Dis. 2012, 44, 470–472. [Google Scholar] [CrossRef]
- Khouzam, R.N.; Parizianu, C.; Hafiz, A.M.; Chawla, S.; Schwartz, R. Fulminant myocarditis associated with novel H1N1 influenza A. Heart Lung 2011, 40, 566–568. [Google Scholar] [CrossRef]
- Quandt, D.; Buechel, E.R.V.; Knirsch, W. Pericarditis constrictiva in a 10-year-old boy after influenza A virus infection. Pediatr. Cardiol. 2011, 32, 525–526. [Google Scholar] [CrossRef][Green Version]
- Koranyi, K.; Yontz, D.; Rohrer, Z.; Leber, A.; Ramilo, O. Pericardial effusion complicating novel influenza A (H1N1) infection in an infant. Pediatr. Infect. Dis. J. 2010, 29, 782–783. [Google Scholar] [CrossRef] [PubMed]
- Gross, E.R.; Gander, J.W.; Reichstein, A.; Cowles, R.A.; Stolar, C.J.; Middlesworth, W. Fulminant pH1N1-09 influenza-associated myocarditis in pediatric patients. Pediatr. Crit. Care Med. 2011, 12, e99–e101. [Google Scholar] [CrossRef] [PubMed]
- Frank, H.; Wittekind, C.; Liebert, U.G.; Siekmeyer, M.; Siekmeyer, W.; Schuster, V.; Kiess, W. Lethal influenza B myocarditis in a child and review of the literature for pediatric age groups. Infection 2010, 38, 231–235. [Google Scholar] [CrossRef] [PubMed]
- Jang, J.Y.; Chang, H.J.; Jang, Y.; Han, S.H.; Bang, W.D.; Cho, S.S.; Oh, C.M.; Yu, H.T.; Shim, C.Y.; Ha, J.W.; et al. Constrictive Pericarditis Accompanied by Swine-Origin Influenza A (H1N1) Infection. Korean Circ. J. 2010, 40, 539–542. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Puzelli, S.; Buonaguro, F.M.; Facchini, M.; Palmieri, A.; Calzoletti, L.; De Marco, M.A.; Arace, P.; de Campora, E.; Esposito, C.; Cassone, A.; et al. Cardiac tamponade and heart failure due to myopericarditis as a presentation of infection with the pandemic H1N1 2009 influenza A virus. J. Clin. Microbiol. 2010, 48, 2298–2300. [Google Scholar] [CrossRef]
- Al-Amoodi, M.; Rao, K.; Rao, S.; Brewer, J.H.; Magalski, A.; Chhatriwalla, A.K. Fulminant myocarditis due to H1N1 influenza. Circ. Heart Fail. 2010, 3, e7–e9. [Google Scholar] [CrossRef][Green Version]
- Bramante, R.M.; Cirilli, A.; Raio, C.C. Point-of-care sonography in the emergency department diagnosis of acute H1N1 influenza myocarditis. J. Ultrasound Med. 2010, 29, 1361–1364. [Google Scholar] [CrossRef]
- Haessler, S.; Paez, A.; Rothberg, M.; Higgins, T. 2009 pandemic H1N1-associated myocarditis in a previously healthy adult. Clin. Microbiol. Infect. 2011, 17, 572–574. [Google Scholar] [CrossRef]
- Cobas, M.; Abbo, L.; Santos, M.; Baccini-Jauregui, C.; Pham, S. Successful management of fulminant influenza A subtype H1N1 myocarditis. BMJ Case Rep. 2010, 2010, bcr0220102763. [Google Scholar] [CrossRef]
- Horai, Y.; Miyamura, T.; Takahama, S.; Sonomoto, K.; Nakamura, M.; Ando, H.; Minami, R.; Yamamoto, M.; Suematsu, E. Influenza virus B-associated hemophagocytic syndrome and recurrent pericarditis in a patient with systemic lupus erythematosus. Mod. Rheumatol. 2010, 20, 178–182. [Google Scholar] [CrossRef]
- Mamas, M.A.; Nair, S.; Fraser, D. Cardiac tamponade and heart failure as a presentation of influenza. Exp. Clin. Cardiol. 2007, 12, 214–216. [Google Scholar] [PubMed]
- Laurila, J.J.; Ala-Kokko, T.I.; Tuokko, H.; Syrjälä, H. Cardiac tamponade and septic shock caused by viral infection in a previously healthy woman. Acta Anaesthesiol. Scand. 2005, 49, 1384–1386. [Google Scholar] [CrossRef] [PubMed]
- Gerberding, J.L.; Morgan, J.G.; Shepard, J.A.; Kradin, R.L. Case records of the Massachusetts General Hospital. Weekly clinicopathological exercises. Case 9-2004. An 18-year-old man with respiratory symptoms and shock. N. Engl. J. Med. 2004, 350, 1236–1247. [Google Scholar] [CrossRef] [PubMed]
- Tabbutt, S.; Leonard, M.; Godinez, R.I.; Sebert, M.; Cullen, J.; Spray, T.L.; Friedman, D. Severe influenza B myocarditis and myositis. Pediatr. Crit. Care Med. 2004, 5, 403–406. [Google Scholar] [CrossRef]
- Takehana, H.; Inomata, T.; Kuwao, S.; Nakahata, J.; Sasaki, T.; Nishii, M.; Kurokawa, S.; Izumi, T. Recurrent fulminant viral myocarditis with a short clinical course. Circ. J. 2003, 67, 646–648. [Google Scholar] [CrossRef]
- Agnino, A.; Schena, S.; Ferlan, G.; De Luca Tupputi Schinosa, L. Left ventricular pseudoaneurysm after acute influenza A myocardiopericarditis. J. Cardiovasc. Surg. 2002, 43, 203–205. [Google Scholar]
- McGovern, P.C.; Chambers, S.; Blumberg, E.A.; Acker, M.A.; Tiwari, S.; Taubenberger, J.K.; Carboni, A.; Twomey, C.; Loh, E. Successful explantation of a ventricular assist device following fulminant influenza type A-associated myocarditis. J. Heart Lung Transplant. 2002, 21, 290–293. [Google Scholar] [CrossRef]
- Nolte, K.B.; Alakija, P.; Oty, G.; Shaw, M.W.; Subbarao, K.; Guarner, J.; Shieh, W.J.; Dawson, J.E.; Morken, T.; Cox, N.J.; et al. Influenza A virus infection complicated by fatal myocarditis. Am. J. Forensic Med. Pathol. 2000, 21, 375–379. [Google Scholar] [CrossRef]
- McGregor, D.; Henderson, S. Myocarditis, rhabdomyolysis and myoglobinuric renal failure complicating influenza in a young adult. N. Z. Med. J. 1997, 110, 237. [Google Scholar]
- Voets, A.J.; Netten, P.M.; Aengevaeren, W.R.; Berden, J.H. Cardiac tamponade caused by influenza B. Neth. J. Med. 1988, 32, 243–246. [Google Scholar]
- Proby, C.M.; Hackett, D.; Gupta, S.; Cox, T.M. Acute myopericarditis in influenza A infection. Q. J. Med. 1986, 60, 887–892. [Google Scholar] [PubMed]
- Osanloo, E.; Shalhoub, R.J.; Cioffi, R.F.; Parker, R.H. Viral pericarditis in patients receiving hemodialysis. Arch. Intern. Med. 1979, 139, 301–303. [Google Scholar] [CrossRef] [PubMed]
- Macon, R.C.; Miller, G.W.; Katz, S. Type A Asian influenzal pericarditis. Report of a case. Med. Ann. Dist. Columbia 1964, 33, 570–571. [Google Scholar]
- Hildebrandt, H.M.; Maassab, H.F.; Willis, P.W., 3rd. Influenza virus pericarditis. Report of a case with isolation of Asian influenza virus from the pericardial fluid. Am. J. Dis. Child. 1962, 104, 579–582. [Google Scholar] [CrossRef]
- Adams, C.W. Postviral myopericarditis associated with the influenza virus; report of eight cases. Am. J. Cardiol. 1959, 4, 56–67. [Google Scholar] [CrossRef]
- Onitsuka, H.; Imamura, T.; Miyamoto, N.; Shibata, Y.; Kashiwagi, T.; Ayabe, T.; Kawagoe, J.; Matsuda, J.; Ishikawa, T.; Unoki, T.; et al. Clinical manifestations of influenza a myocarditis during the influenza epidemic of winter 1998-1999. J. Cardiol. 2001, 37, 315–323. [Google Scholar]
- Baughman, K.L. Diagnosis of myocarditis: Death of Dallas criteria. Circulation 2006, 113, 593–595. [Google Scholar] [CrossRef]
- Van Schaik, G.W.W.; van Schaik, K.D.; Murphy, M.C. Point-of-Care Ultrasonography (POCUS) in a Community Emergency Department: An Analysis of Decision Making and Cost Savings Associated With POCUS. J. Ultrasound Med. 2019, 38, 2133–2140. [Google Scholar] [CrossRef]
- Appleton, C.; Gillam, L.; Koulogiannis, K. Cardiac Tamponade. Cardiol. Clin. 2017, 35, 525–537. [Google Scholar] [CrossRef]
- Cooper, L.T.; Baughman, K.L.; Feldman, A.M.; Frustaci, A.; Jessup, M.; Kuhl, U.; Levine, G.N.; Narula, J.; Starling, R.C.; Towbin, J.; et al. The role of endomyocardial biopsy in the management of cardiovascular disease: A scientific statement from the American Heart Association, the American College of Cardiology, and the European Society of Cardiology. Circulation 2007, 116, 2216–2233. [Google Scholar] [CrossRef]
- Ukimura, A.; Izumi, T.; Matsumori, A. A national survey on myocarditis associated with the 2009 influenza A (H1N1) pandemic in Japan. Circ. J. 2010, 74, 2193–2199. [Google Scholar] [CrossRef] [PubMed]
- Kotaka, M.; Kitaura, Y.; Deguchi, H.; Kawamura, K. Experimental influenza A virus myocarditis in mice. Light and electron microscopic, virologic, and hemodynamic study. Am. J. Pathol. 1990, 136, 409–419. [Google Scholar] [PubMed]
- Mahrholdt, H.; Goedecke, C.; Wagner, A.; Meinhardt, G.; Athanasiadis, A.; Vogelsberg, H.; Fritz, P.; Klingel, K.; Kandolf, R.; Sechtem, U. Cardiovascular magnetic resonance assessment of human myocarditis: A comparison to histology and molecular pathology. Circulation 2004, 109, 1250–1258. [Google Scholar] [CrossRef] [PubMed]
- Cooper, L.T., Jr.; Berry, G.J.; Shabetai, R.; Multicenter Giant Cell Myocarditis Study Group Investigators. Idiopathic giant-cell myocarditis—Natural history and treatment. N. Engl. J. Med. 1997, 336, 1860–1866. [Google Scholar] [CrossRef] [PubMed]
- Kadoglou, N.P.E.; Bracke, F.; Simmers, T.; Tsiodras, S.; Parissis, J. Influenza infection and heart failure-vaccination may change heart failure prognosis? Heart Fail. Rev. 2017, 22, 329–336. [Google Scholar] [CrossRef]
- Kwong, J.C.; Schwartz, K.L.; Campitelli, M.A. Acute Myocardial Infarction after Laboratory-Confirmed Influenza Infection. N. Engl. J. Med. 2018, 378, 2540–2541. [Google Scholar] [CrossRef]
- Kalil, A.C.; Thomas, P.G. Influenza virus-related critical illness: Pathophysiology and epidemiology. Crit. Care 2019, 23, 258. [Google Scholar] [CrossRef]
- Smith, S.C., Jr.; Allen, J.; Blair, S.N.; Bonow, R.O.; Brass, L.M.; Fonarow, G.C.; Grundy, S.M.; Hiratzka, L.; Jones, D.; Krumholz, H.M.; et al. AHA/ACC guidelines for secondary prevention for patients with coronary and other atherosclerotic vascular disease: 2006 update endorsed by the National Heart, Lung, and Blood Institute. J. Am. Coll. Cardiol. 2006, 47, 2130–2139. [Google Scholar] [CrossRef]
- Wieruszewski, P.M.; Linn, D.D. Contemporary management of severe influenza disease in the intensive care unit. J. Crit. Care 2018, 48, 48–55. [Google Scholar] [CrossRef]
- Dobson, J.; Whitley, R.J.; Pocock, S.; Monto, A.S. Oseltamivir treatment for influenza in adults: A meta-analysis of randomised controlled trials. Lancet 2015, 385, 1729–1737. [Google Scholar] [CrossRef]
- Chaves, S.S.; Pérez, A.; Miller, L.; Bennett, N.M.; Bandyopadhyay, A.; Farley, M.M.; Fowler, B.; Hancock, E.B.; Kirley, P.D.; Lynfield, R.; et al. Impact of Prompt Influenza Antiviral Treatment on Extended Care Needs After Influenza Hospitalization Among Community-Dwelling Older Adults. Clin. Infect. Dis. 2015, 61, 1807–1814. [Google Scholar] [CrossRef] [PubMed]
- Jefferson, T.; Jones, M.A.; Doshi, P.; Del Mar, C.B.; Hama, R.; Thompson, M.J.; Spencer, E.A.; Onakpoya, I.; Mahtani, K.R.; Nunan, D.; et al. Neuraminidase inhibitors for preventing and treating influenza in adults and children. Cochrane Database Syst. Rev. 2014, 2014, Cd008965. [Google Scholar]
- Baik, S.H.; Jeong, H.S.; Kim, S.J.; Yoon, Y.K.; Sohn, J.W.; Kim, M.J. A Case of Influenza Associated Fulminant Myocarditis Successfully Treated with Intravenous Peramivir. Infect. Chemother. 2015, 47, 272–277. [Google Scholar] [CrossRef]
- Jahns, F.P.; Ben-Hamouda, N.; Kirsch, M.; Roumy, A.; Liaudet, L. Intravenous zanamivir for influenza myocarditis and enteral malabsorption. Crit. Care 2018, 22, 332. [Google Scholar] [CrossRef] [PubMed]
- Yu, D.Q.; Wang, Y.; Ma, G.Z.; Xu, R.H.; Cai, Z.X.; Ni, C.M.; Chen, P.; Zhu, Z.D. Intravenous immunoglobulin in the therapy of adult acute fulminant myocarditis: A retrospective study. Exp. Ther. Med. 2014, 7, 97–102. [Google Scholar] [CrossRef]
- Robinson, J.; Hartling, L.; Vandermeer, B.; Sebastianski, M.; Klassen, T.P. Intravenous immunoglobulin for presumed viral myocarditis in children and adults. Cochrane Database Syst. Rev. 2020, 8, Cd004370. [Google Scholar]
- Imazio, M.; Gaita, F.; LeWinter, M. Evaluation and Treatment of Pericarditis: A Systematic Review. JAMA 2015, 314, 1498–1506. [Google Scholar] [CrossRef]
- Imazio, M.; Brucato, A.; Cumetti, D.; Brambilla, G.; Demichelis, B.; Ferro, S.; Maestroni, S.; Cecchi, E.; Belli, R.; Palmieri, G.; et al. Corticosteroids for recurrent pericarditis: High versus low doses: A nonrandomized observation. Circulation 2008, 118, 667–671. [Google Scholar] [CrossRef]
- Lotrionte, M.; Biondi-Zoccai, G.; Imazio, M.; Castagno, D.; Moretti, C.; Abbate, A.; Agostoni, P.; Brucato, A.L.; Di Pasquale, P.; Raatikka, M.; et al. International collaborative systematic review of controlled clinical trials on pharmacologic treatments for acute pericarditis and its recurrences. Am. Heart J. 2010, 160, 662–670. [Google Scholar] [CrossRef]
- Estabragh, Z.R.; Mamas, M.A. The cardiovascular manifestations of influenza: A systematic review. Int. J. Cardiol. 2013, 167, 2397–2403. [Google Scholar] [CrossRef]
- McCarthy, R.E., 3rd; Boehmer, J.P.; Hruban, R.H.; Hutchins, G.M.; Kasper, E.K.; Hare, J.M.; Baughman, K.L. Long-term outcome of fulminant myocarditis as compared with acute (nonfulminant) myocarditis. N. Engl. J. Med. 2000, 342, 690–695. [Google Scholar] [CrossRef] [PubMed]
- Morparia, K.; Peshkovsky, C.; Kalyanaraman, M. Purulent pericarditis secondary to influenza and community-acquired methicillin-resistant Staphylococcus aureus co-infection. Cardiol. Young 2018, 28, 1481–1483. [Google Scholar] [CrossRef]
- Harre, B.; Nashelsky, M.; Douvoyiannis, M.; Shulman, S.T. Fatal group A streptococcal myopericarditis during influenza A infection. Pediatr. Infect. Dis. J. 2006, 25, 660–661. [Google Scholar] [CrossRef]
- Houlihan, E.; McLoughlin, R.; Waldron, R. Streptococcus pneumoniae purulent pericarditis secondary to influenza A infection and pneumococcal pneumonia in an immunocompetent woman. BMJ Case Rep. 2021, 14, e240763. [Google Scholar] [CrossRef] [PubMed]
- Radovanovic, M.; Petrovic, M.; Hanna, R.D.; Nordstrom, C.W.; Calvin, A.D.; Barsoum, M.K.; Milosavljevic, N.; Jevtic, D.; Sokanovic, M.; Dumic, I. Clinical Presentation and Management of Methicillin-Resistant Staphylococcus aureus Pericarditis—Systematic Review. J. Cardiovasc. Dev. Dis. 2022, 9, 103. [Google Scholar] [CrossRef]
- Manna, S.; Baindara, P.; Mandal, S.M. Molecular pathogenesis of secondary bacterial infection associated to viral infections including SARS-CoV-2. J. Infect. Public Health 2020, 13, 1397–1404. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Demographic Characteristics | n | M to F Ratio | Age Range (Years) | Mean Age (Years) |
| Adult | 55 (73.3%) | 28:27 | 18–75 | 40.5 ± 14.8 |
| Pediatric | 20 (26.7%) | 3:17 | 0.25–17 | 9.7 ± 4.9 |
| Total | 75 (100%) | 31:44 | 0.25–75 | 32.3 ± 18.8 |
| Co-morbidities | ||||
| Adult | ||||
| Not present | 26 (47.3%) | |||
| Present | 29 (52.7%) | |||
| Hypertension and alcohol use | each in 4 (7.3%) | |||
| CAD (previous MI), advanced CKD/ESRD, asthma, tobacco dependence | each in 3 (5.4%) | |||
| Obesity and hyperlipidemia | each in 2 (3.6%) | |||
| Previous Influenza B myocarditis (16 years prior), DMT2, hypothyroidism, primary biliary cirrhosis, diverticulitis, breast cancer, SLE, MS, TBI, Down syndrome, schizophrenia, marijuana and cocaine use, previous infection with TB, syphilis, gonorrhea | each in 1 (3.6%) | |||
| Pediatric | ||||
| Not present | 17 (85%) | |||
| Present | 3 (15%) | |||
| Viral myocarditis | 1 (5%) | |||
| Asthma | 1 (5%) | |||
| Rheumatic fever | 1 (5%) | |||
| Clinical presentation | Symptom duration | Range (days) | Mean (days) | |
| Febrile (“flu-like”) illness | 71 (94.7%) | Reported–66 (88%) | 1–42 | 6.9 ± 6.4 |
| Tachycardia | 62 (82.7%) | Not reported–9 (12%) | ||
| Hypotension/Shock | 54 (72%) | |||
| Chest pain | 36 (48%) | |||
| Dyspnea | 34 (45.3%) | |||
| Pericardial friction rub | 15 (20%) | |||
| Elevated JVP | 10 (13.3%) | |||
| Abdominal pain | 8 (10.7%) | |||
| Muffled heart sound | 8 (10.7%) | |||
| Nausea/vomiting | 8 (10.7%) | |||
| Collapse/syncope | 6 (8%) | |||
| Pulsus paradoxus | 5 (6.7%) | |||
| Altered mental status/lethargy | 5 (6.7%) | |||
| ECG findings | ||||
| Normal or not reported | 14 (18.7%) | |||
| Abnormal | ||||
| ST elevation and/or PR depression | 26 (42.6%) | |||
| Low voltage QRS complexes | 22 (36.1%) | |||
| Electrical alternans | 2 (3.3%) | |||
| Echocardiography findings | ||||
| Performed | 62 (82.7%) | |||
| Decreased EF or diffuse hypokinesis | 42 (67.7%) | |||
| Pericardial effusion | ||||
| Without tamponade physiology | 38 (61.3%) | |||
| With tamponade physiology | 24 (38.7%) | |||
| Not reported, although authors reported pericardial effusion in all 13 cases with tamponade in 3 cases | 13 (17.3%) | |||
| Treatment | ||||
| Antivirals (Oseltamivir/Peramivir/Zanamivir) | 33 (44%)/6 (8%)/3 (5%) | |||
| NSAIDs | 13 (17.3%) | |||
| Corticosteroids | 12 (16%) | |||
| Colchicine | 8 (10.7%) | |||
| IVIG | 8 (10.7%) | |||
| Circulatory support | ||||
| Inotropes/vasopressors | 44 (58.7%) | |||
| Mechanical | ||||
| ECMO | 18 (24%) | |||
| Intra-aortic balloon pump | 9 (12%) | |||
| Ventricular assist device | 7 (9.3%) | |||
| Pericardiocentesis | 28 (37.3%) | |||
| Pericardiectomy/Pericardial window | 4 (5.3%)/3 (4%) | |||
| Outcome and complications | ||||
| Recovered | 63 (84%) | |||
| Long-term complications | ||||
| No | 55 (87.3%) | |||
| Yes | 8 (12.7%) | |||
| Chronic (constrictive) pericarditis | 3 (4.8%) | |||
| Recurrent pericardial effusions | 2 (3.2%) | |||
| Mild LV dysfunction | 2 (3.2%) | |||
| LV pseudoaneurysm | 1 (1.6%) | |||
| Awaiting transplant | 1 (1.3%) | |||
| Deceased | 11 (14.7%) |
| Myopericarditis | vs. | Pericarditis | |
|---|---|---|---|
| Number of cases | 58 (77.3%) | 17 (22.7%) | |
| Shock type | Cardiogenic (n = 25, 43.1%) | Obstructive (tamponade) (n = 7, 41.2%) | |
| Combined (n = 12, 20.7%) | |||
| Obstructive (tamponade) (n = 8, 13.8%) | |||
| Gender predominance | Female | Male (p = 0.008) | |
| Age | Younger patients (30 ± 19 years) | Older patients (39 ± 19 years; p = 0.091) | |
| Co-morbidities | No impact (p > 0.05) | No impact (p > 0.05) | |
| Initial physical exam | Tachycardia and hypotension (shock) (p < 0.001) | Pericardial friction rub (p < 0.001) | |
| Circulatory support (CS) | 44 (75.7%) | 1 (5.9%) | |
| Mechanical CS | 24 (41.4%) | None | |
| Deceased | 11 (p = 0.05) | None |
| Reference | Age/Sex | Influenza Type | Sampling | Histopathology |
|---|---|---|---|---|
| Jiménez-Méndez et al. (2019) [26] | 35 M | Influenza A | EMB | Minimal inflammatory infiltrate, CD3-positive cells |
| Lefeuvre et al. (2018) [2] | 14 F | Influenza A (H3N2) | Autopsy | Myocardial necrosis with contraction bands and interstitial edema with an abundant mononuclear inflammatory infiltrate |
| Roto et al. (2018) [31] | 57 F | Influenza B | Autopsy | Myocardial necrosis with infiltration of CD3-positive lymphocytes |
| Siskin et al. (2017) [34] | 22 F | Influenza B | EMB | Myocardial necrosis through complement-mediated cellular injury without evidence of interstitial infiltrates |
| Davidovic et al (2016) [39] | 19 M | Influenza A (H1N1) | Autopsy | Extensive zones of necrosis with degenerative cardiomyocytes and inflammatory neutrophilic and lymphocytic infiltrate |
| Lee et al. (2012) [48] | 8 F | Influenza A (H1N1) | Autopsy | Widespread contraction band myofiber necrosis with increased interstitial cellularity (mostly CD68-positive monocytes and CD8-positive T lymphocytes and no eosinophils) |
| Kumar et al. (2011) [18] | 17 F | Influenza A (H1N1) | Tissue sampling at the time of VAD placement | Extensive myocyte necrosis with the confirmation of viral particles by electron microscopy |
| Khouzam et al (2011) [50] | 36 M | Influenza A (H1N1) | Autopsy | Myocardial interstitium exhibited edema and an inflammatory infiltrate, rich in lymphocytes and macrophages |
| Frank et al. (2010) [54] | 5 F | Influenza B | Autopsy | Moderate interstitial infiltration of lymphocytes, as well as neutrophils and eosinophils, were found. Influenza B RNA was detected in cardiac tissue |
| Puzelli et al. (2010) [56]. | 11 F | Influenza A (H1N1) | Autopsy | Mild inflammation, modest infiltration of histiocytes (CD68-positive), and myocellular necrosis |
| Gerberding et al. (2004) [64] | 18 M | Influenza A | Autopsy | Cardiac myocyte hypertrophy and a patchy lymphohistiocytic infiltrate in perivascular areas associated with interstitial edema. Focal contraction-band myocyte necrosis and scattered intravascular fibrin thrombi |
| Tabbutt et al (2004) [65] | 4 F | Influenza B | EMB | Mildly congested myocardium, with interstitial fibrosis and rare lymphocytes. Electron microscopy showed mildly pleomorphic mitochondria and the absence of viral inclusions |
| Takehana et al. (2003) [66] | 75 M | Influenza A | Autopsy | Marked inflammatory cell infiltration, mainly composed of mononuclear cells, with myocardial degeneration and necrosis, and interstitial edema |
| McGovern et al. (2002) [68] | 30 F | Influenza A | Tissue sampling at the time of VAD placement | Focal interstitial fibrosis, diffuse lymphocytic infiltrate |
| Nolte et al. (2000) [69] | 11 F | Influenza A (H3N2) | Autopsy | Transmural, sparse, patchy infiltrates of lymphocytes and neutrophils associated with myocyte necrosis and nuclear debris |
| Reference | Age/Sex | Co-morbidities | Presenting Symptoms | Symptom Duration | Influenza Type | Cardiac Involvement | Cardiogenic Shock | Cardiac Tamponade | Pericardial Drainage | Medical Management | Circulatory Support | Time to Death |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Thomas et al. (2019) [27] | 23 F | None | AFI, dyspnea, | 3 days | Influenza A (H1N1) | Myopericarditis | Yes | No | No | Oseltamivir | Vasopressors/inotropes | 1 day |
| Lefeuvre et al. (2018) [2] | 14 F | None | AFI, dyspnea, collapse | not reported | Influenza A (H3N2) | Myopericarditis | Yes | Yes | No | None | Vasopressors/inotropes | 1 day |
| Roto et al. (2018) [31] | 57 F | None | AFI, dyspnea, AMS | 7 days | Influenza B | Myopericarditis | No | Yes | Pericardiocentesis (90 mL) | Not reported | Vasopressors/inotropes | not reported |
| Davidovic et al (2016) [39] | 19 M | None | AFI, chest pain | 2 days | Influenza A (H1N1) | Myopericarditis | Yes | No | No | NSAIDs | Vasopressors/inotropes | several hours |
| Lee et al. (2012) [48] | 8 F | Previous viral myocarditis | AFI, chest pain, vomiting | 2 days | Influenza A (H1N1) | Myopericarditis | Yes | No | No | Oseltamivir, IVIG | Vasopressors/inotropes | 2 days |
| Khouzam et al (2011) [50] | 36 M | childhood asthma | AFI, dyspnea, nausea, diarrhea | 21 days | Influenza A (H1N1) | Myopericarditis | Yes | No | Pericardiocentesis (700 mL) | Oseltamivir, peramivir | vasopressors/inotropes, catheter based VAD | 18 h |
| Frank et al. (2010) [54] | 5 F | None | AFI, abdominal pain | 7 days | Influenza B | Myopericarditis | Yes | No | No | Not reported | Vasopressors/inotropes | 1 day |
| Puzelli et al. (2010) [56] | 11 F | None | AFI, dyspnea | 3 days | Influenza A (H1N1) | Myopericarditis | No | Yes | Autopsy (150 mL) | None | No | not reported |
| Gerberding et al. (2004) [64] | 18 M | Obesity, HLD | AFI, pleuritic chest pain, mottled skin | 5 days | Influenza A | Myopericarditis | Yes | No | Autopsy (400 mL) | Not reported | Vasopressors/inotropes | 36 h |
| Takehana et al. (2003) [66] | 75 M | not reported | AFI | not reported | Influenza A | Myopericarditis | Yes | No | No | Not reported | IABP | 24 days |
| Nolte et al. (2000) [69] | 11 F | None | AFI, collapse | 7 days | Influenza A (H3N2) | Myopericarditis | No | Yes | Autopsy (40 mL) | None | No | Died before hospitalization |
| Univariate Regression Analysis | |||
|---|---|---|---|
| Variable | p Value | OR | 95% CI for OR |
| Sex | 0.564 | 1.806 | 0.243–13.444 |
| Age | 0.931 | 1.002 | 0.949–1.059 |
| Influenza type/subtype | 0.940 | 0.931 | 0.147–5.889 |
| Tamponade (recognized on presentation) | 0.570 | 0.570 | 0.082–3.965 |
| Cardiogenic shock | 0.157 | 4.983 | 0.538–46.180 |
| Mechanical circulatory support | 0.047 | 0.094 | 0.009–0.971 |
| Vasopressor support | 0.863 | 0.755 | 0.031–18.375 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Radovanovic, M.; Petrovic, M.; Barsoum, M.K.; Nordstrom, C.W.; Calvin, A.D.; Dumic, I.; Jevtic, D.; Hanna, R.D. Influenza Myopericarditis and Pericarditis: A Literature Review. J. Clin. Med. 2022, 11, 4123. https://doi.org/10.3390/jcm11144123
Radovanovic M, Petrovic M, Barsoum MK, Nordstrom CW, Calvin AD, Dumic I, Jevtic D, Hanna RD. Influenza Myopericarditis and Pericarditis: A Literature Review. Journal of Clinical Medicine. 2022; 11(14):4123. https://doi.org/10.3390/jcm11144123
Chicago/Turabian StyleRadovanovic, Milan, Marija Petrovic, Michel K. Barsoum, Charles W. Nordstrom, Andrew D. Calvin, Igor Dumic, Dorde Jevtic, and Richard D. Hanna. 2022. "Influenza Myopericarditis and Pericarditis: A Literature Review" Journal of Clinical Medicine 11, no. 14: 4123. https://doi.org/10.3390/jcm11144123
APA StyleRadovanovic, M., Petrovic, M., Barsoum, M. K., Nordstrom, C. W., Calvin, A. D., Dumic, I., Jevtic, D., & Hanna, R. D. (2022). Influenza Myopericarditis and Pericarditis: A Literature Review. Journal of Clinical Medicine, 11(14), 4123. https://doi.org/10.3390/jcm11144123