
One-Year Follow-Up of Patients Admitted for Emergency Coronary Angiography after Resuscitated Cardiac Arrest

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
3. Results
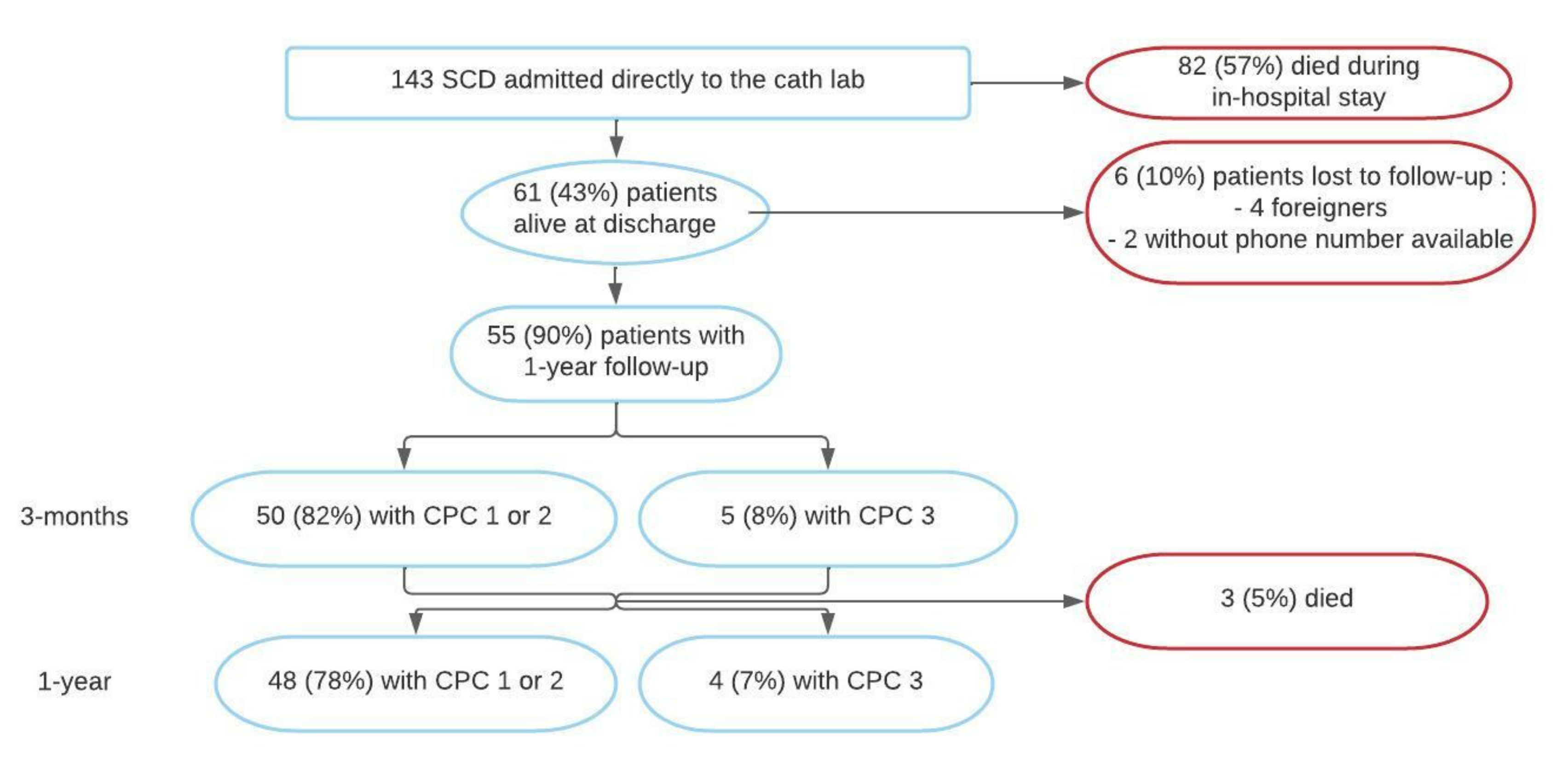
3.1. Study Population
3.2. Primary End Point
3.3. Secondary End Points
3.4. Quality of Life
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Answer (n = 36) | Satisfaction | Health Problems | ||||||
|---|---|---|---|---|---|---|---|---|
| Cognition | Self | Daily Life | Social Relationships | Total | Emotion | Physical Problems | Total | |
| “Not at all” no. (%) | 3 (8.3) | 0 (0) | 4 (11.1) | 1 (2.8) | 2 (5.6) | 18 (50) | 18 (50) | 20 (55.6) |
| “Slightly” no. (%) | 7 (19.4) | 15 (41.7) | 9 (25) | 8 (22.2) | 10 (27.8) | 5 (13.9) | 9 (25) | 5 (13.9) |
| “Quite” no. (%) | 16 (44.4) | 16 (44.4) | 5 (13.9) | 22 (61.1) | 18 (50) | 11 (30.6) | 9 (25) | 11 (30.6) |
| “Very” no. (%) | 10 (27.8) | 5 (13.9) | 18 (50) | 5 (13.9) | 6 (16.7) | 2 (5.6) | 0 (0) | 0 (0) |
References
- Luc, G.; Baert, V.; Escutnaire, J.; Genin, M.; Vilhelm, C.; Di Pompéo, C.; El Khoury, C.; Segal, N.; Wiel, E.; Adnet, F.; et al. Epidemiology of out-of-hospital cardiac arrest: A French national incidence and mid-term survival rate study. Anaesth. Crit. Care Pain Med. 2019, 38, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Chugh, S.S.; Reinier, K.; Teodorescu, C.; Evanado, A.; Kehr, E.; Al Samara, M.; Mariani, R.; Gunson, K.; Jui, J. Epidemiology of Sudden Cardiac Death: Clinical and Research Implications. Prog. Cardiovasc. Dis. 2008, 51, 213–228. [Google Scholar] [CrossRef] [PubMed]
- Kuriachan, V.P.; Sumner, G.L.; Mitchell, L.B. Sudden Cardiac Death. Curr. Probl. Cardiol. 2015, 40, 133–200. [Google Scholar] [CrossRef] [PubMed]
- Spaulding, C.M.; Joly, L.-M.; Rosenberg, A.; Monchi, M.; Weber, S.N.; Dhainaut, J.-F.A.; Carli, P. Immediate Coronary Angiography in Survivors of Out-of-Hospital Cardiac Arrest. N. Engl. J. Med. 1997, 336, 1629–1633. [Google Scholar] [CrossRef]
- Leclercq, F.; Lonjon, C.; Marin, G.; Akodad, M.; Roubille, F.; Macia, J.-C.; Cornillet, L.; Gervasoni, R.; Schmutz, L.; Ledermann, B.; et al. Post resuscitation electrocardiogram for coronary angiography indication after out-of-hospital cardiac arrest. Int. J. Cardiol. 2020, 310, 73–79. [Google Scholar] [CrossRef]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [CrossRef]
- Moulaert, V.R.; Verbunt, J.A.; van Heugten, C.M.; Wade, D.T. Cognitive impairments in survivors of out-of-hospital cardiac arrest: A systematic review. Resuscitation 2009, 80, 297–305. [Google Scholar] [CrossRef]
- Sasson, C.; Rogers, M.A.; Dahl, J.; Kellermann, A.L. Predictors of Survival From Out-of-Hospital Cardiac Arrest: A Systematic Review and Meta-Analysis. Circ. Cardiovasc. Qual. Outcomes 2010, 3, 63–81. [Google Scholar] [CrossRef]
- Patel, N.; Patel, N.J.; Macon, C.J.; Thakkar, B.; Desai, M.; Rengifo-Moreno, P.; Alfonso, C.E.; Myerburg, R.J.; Bhatt, D.L.; Cohen, M. Trends and Outcomes of Coronary Angiography and Percutaneous Coronary Intervention After Out-of-Hospital Cardiac Arrest Associated With Ventricular Fibrillation or Pulseless Ventricular Tachycardia. JAMA Cardiol. 2016, 1, 890–899. [Google Scholar] [CrossRef]
- Daubin, C.; Quentin, C.; Allouche, S.; Etard, O.; Gaillard, C.; Seguin, A.; Valette, X.; Parienti, J.-J.; Prevost, F.; Ramakers, M.; et al. Serum neuron-specific enolase as predictor of outcome in comatose cardiac-arrest survivors: A prospective cohort study. BMC Cardiovasc. Disord. 2011, 11, 48. [Google Scholar] [CrossRef]
- Haydon, G.; Van Der Riet, P.; Inder, K. A systematic review and meta-synthesis of the qualitative literature exploring the experiences and quality of life of survivors of a cardiac arrest. Eur. J. Cardiovasc. Nurs. J. Work Group Cardiovasc. Nurs. Eur. Soc. Cardiol. 2017, 16, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Cummins, R.O.; Chamberlain, D.A.; Abramson, N.S.; Allen, M.; Baskett, P.J.; Becker, L.; Bossaert, L.; Delooz, H.H.; Dick, W.F.; Eisenberg, M.S. Recommended guidelines for uniform reporting of data from out-of-hospital cardiac arrest: The Utstein Style. A statement for health professionals from a task force of the American Heart Association, the European Resuscitation Council, the Heart and Stroke Foundation of Canada, and the Australian Resuscitation Council. Circulation 1991, 84, 960–975. [Google Scholar] [CrossRef] [PubMed]
- Phelps, R.J.; Rea, T.; Maynard, C.; Dumas, F. Cerebral Performance Category and Long-Term Prognosis in Cardiac Arrest Survivors. Circulation 2011, 124 (Suppl. S21), A179. [Google Scholar] [CrossRef]
- Edgren, E.; Hedstrand, U.; Kelsey, S.; Sutton-Tyrrell, K.; Safar, P. BRCTI Study Group Assessment of neurological prognosis in comatose survivors of cardiac arrest. Lancet 1994, 343, 1055–1059. [Google Scholar] [CrossRef]
- Martinell, L.; Nielsen, N.; Herlitz, J.; Karlsson, T.; Horn, J.; Wise, M.P.; Undén, J.; Rylander, C. Early predictors of poor outcome after out-of-hospital cardiac arrest. Crit. Care 2017, 21, 96. [Google Scholar] [CrossRef]
- Von Steinbuechel, N.; Wilson, L.; Gibbons, H.; Hawthorne, G.; Höfer, S.; Schmidt, S.; Bullinger, M.; Maas, A.I.; Neugebauer, E.; Powell, J.; et al. Quality of Life after Brain Injury (QOLIBRI): Scale Validity and Correlates of Quality of Life. J. Neurotrauma 2010, 27, 1157–1165. [Google Scholar] [CrossRef]
- Von Steinbüchel, N.; Wilson, L.; Gibbons, H.; Hawthorne, G.; Hofer, S.; Schmidt, S.; Bullinger, M.; Maas, A.I.; Neugebauer, E.; Powell, J.; et al. Quality of Life after Brain Injury (QOLIBRI): Scale Development and Metric Properties. J. Neurotrauma 2010, 27, 1167–1185. [Google Scholar] [CrossRef]
- Middelkamp, W.; Moulaert, V.R.; Verbunt, J.A.; Van Heugten, C.M.; Bakx, W.G.; Wade, D.T. Life after survival: Long-term daily life functioning and quality of life of patients with hypoxic brain injury as a result of a cardiac arrest. Clin. Rehabil. 2007, 21, 425–431. [Google Scholar] [CrossRef]
- Andersen, L.W.; Holmberg, M.J.; Berg, K.M.; Donnino, M.W.; Granfeldt, A. In-Hospital Cardiac Arrest: A Review. JAMA 2019, 321, 1200–1210. [Google Scholar] [CrossRef]
- Nolan, J.P.; Soar, J.; Smith, G.B.; Gwinnutt, C.; Parrott, F.; Power, S.; Harrison, D.; Nixon, E.; Rowan, K. Incidence and outcome of in-hospital cardiac arrest in the United Kingdom National Cardiac Arrest Audit. Resuscitation 2014, 85, 987–992. [Google Scholar] [CrossRef]
- Pasupula, D.K.; Bhat, A.G.; Meera, S.J.; Malleshappa, S.K.S. Influence of comorbidity on survival after out-of-hospital cardiac arrest in the United States. Resuscitation 2019, 145, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Bunch, T.J.; White, R.D.; Gersh, B.J.; Meverden, R.A.; Hodge, D.O.; Ballman, K.V.; Hammill, S.C.; Shen, W.-K.; Packer, D.L. Long-Term Outcomes of Out-of-Hospital Cardiac Arrest after Successful Early Defibrillation. N. Engl. J. Med. 2003, 348, 2626–2633. [Google Scholar] [CrossRef] [PubMed]
- Kalbag, A.; Kotyra, Z.; Richards, M.; Spearpoint, K.; Brett, S. Long-term survival and residual hazard after in-hospital cardiac arrest. Resuscitation 2006, 68, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Pleskot, M.; Hazukova, R.; Parizek, P.; Cermakova, E.; Tacheci, I. A seven-year follow-up of discharged patients after out-of-hospital cardiac arrest with respect to ST-segment elevation myocardial infarction. Signa Vitae J. Intesive Care Emerg. Med. 2012, 7, 33–39. [Google Scholar]
- Lemkes, J.S.; Janssens, G.N.; van der Hoeven, N.W.; Jewbali, L.S.; Dubois, E.A.; Meuwissen, M.; Rijpstra, T.A.; Bosker, H.A.; Blans, M.J.; Bleeker, G.B.; et al. Coronary Angiography after Cardiac Arrest without ST-Segment Elevation. N. Engl. J. Med. 2019, 380, 1397–1407. [Google Scholar] [CrossRef]
- Antonelli, D.; Koren, O.; Nahir, M.; Rozner, E.; Freedberg, N.A.; Turgeman, Y. Long-Term Survival of Discharged Patients Admitted to Intensive Coronary Care Unit after Out-of-Hospital Cardiac Arres. Isr. Med. Assoc. J. 2017, 19, 751–755. [Google Scholar]
- Lilja, G.; Nielsen, N.; Bro-Jeppesen, J.; Dunford, H.; Friberg, H.; Hofgren, C.; Horn, J.; Insorsi, A.; Kjaergaard, J.; Nilsson, F.; et al. Return to Work and Participation in Society After Out-of-Hospital Cardiac Arrest. Circ. Cardiovasc. Qual. Outcomes 2018, 11, e003566. [Google Scholar] [CrossRef]
- Van Wijnen, H.G.; Mc Rasquin, S.; Van Heugten, C.M.; Verbunt, J.A.; Moulaert, V.R. The impact of cardiac arrest on the long-term wellbeing and caregiver burden of family caregivers: A prospective cohort study. Clin. Rehabil. 2017, 31, 1267–1275. [Google Scholar] [CrossRef]
- Lilja, G. Follow-Up of Cardiac Arrest Survivors: Why, How, and When? A Practical Approach. Semin Neurol. 2017, 37, 88–93. [Google Scholar] [CrossRef]
- Schaaf, K.P.W.; Artman, L.K.; Peberdy, M.A.; Walker, W.C.; Ornato, J.P.; Gossip, M.R.; Kreutzer, J.S. Anxiety, depression, and PTSD following cardiac arrest: A systematic review of the literature. Resuscitation 2013, 84, 873–877. [Google Scholar] [CrossRef]
- Boyce, L.W.; Goossens, P.H.; Moulaert, V.R.; Pound, G.; Van Heugten, C.M. Out-of-hospital cardiac arrest survivors need both cardiological and neurological rehabilitation! Curr. Opin. Crit. Care 2019, 25, 240–243. [Google Scholar] [CrossRef] [PubMed]
- Joshi, V.L.; Tang, L.H.; Borregaard, B.; Zinckernagel, L.; Mikkelsen, T.B.; Taylor, R.S.; Christiansen, S.R.; Nielsen, J.F.; Zwisler, A.D. Long-term physical and psychological outcomes after out-of-hospital cardiac arrest—protocol for a national cross-sectional survey of survivors and their relatives (the DANCAS survey). BMJ Open 2021, 11, e045668. [Google Scholar] [CrossRef] [PubMed]
- Sakr, Y.; Alhussami, I.; Nanchal, R.; Wunderink, R.G.; Pellis, T.; Wittebole, X.; Martin-Loeches, I.; François, B.; Leone, M.; Vincent, J.-L. Being Overweight Is Associated With Greater Survival in ICU Patients: Results From the Intensive Care Over Nations Audit. Crit. Care Med. 2015, 43, 2623–2632. [Google Scholar] [CrossRef] [PubMed]
- Bunch, T.J.; White, R.D.; Lopez-Jimenez, F.; Thomas, R. Association of body weight with total mortality and with ICD shocks among survivors of ventricular fibrillation in out-of-hospital cardiac arrest. Resuscitation 2008, 77, 351–355. [Google Scholar] [CrossRef]
- Mak, K.-H.; Bhatt, D.L.; Shao, M.; Haffner, S.M.; Hamm, C.W.; Hankey, G.; Johnston, S.C.; Montalescot, G.; Steg, P.G.; Steinhubl, S.R.; et al. The influence of body mass index on mortality and bleeding among patients with or at high-risk of atherothrombotic disease. Eur. Heart J. 2009, 30, 857–865. [Google Scholar] [CrossRef]
- Matinrazm, S.; Ladejobi, A.; Pasupula, D.K.; Javed, A.; Durrani, A.; Ahmad, S.; Munir, M.B.; Adelstein, E.; Jain, S.K.; Saba, S. Effect of body mass index on survival after sudden cardiac arrest. Clin. Cardiol. 2018, 41, 46–50. [Google Scholar] [CrossRef]
- Lee, H.; Oh, J.; Kang, H.; Lim, T.H.; Ko, B.S.; Choi, H.J.; Park, S.M.; Jo, Y.H.; Lee, J.S.; Park, Y.S.; et al. Association between the body mass index and outcomes of patients resuscitated from out-of-hospital cardiac arrest: A prospective multicentre registry study. Scand. J. Trauma Resusc. Emerg. Med. 2021, 29, 24. [Google Scholar] [CrossRef]
- Witt, B.J.; Jacobsen, S.; Weston, S.A.; Killian, J.M.; Meverden, R.A.; Allison, T.G.; Reeder, G.S.; Roger, V.L. Cardiac rehabilitation after myocardial infarction in the community. J. Am. Coll. Cardiol. 2004, 44, 988–996. [Google Scholar] [CrossRef]
- González-Salvado, V.; Rodríguez-Núñez, A.; González-Juanatey, J.R. From Prevention to Rehabilitation: Toward a Comprehensive Approach to Tackling Cardiac Arrest. Rev. Espanola Cardiol. 2019, 72, 3–6. [Google Scholar] [CrossRef]
- Kim, C.; Jung, H.; Choi, H.E.; Kang, S.H. Cardiac Rehabilitation After Acute Myocardial Infarction Resuscitated From Cardiac Arrest. Ann. Rehabil. Med. 2014, 38, 799–804. [Google Scholar] [CrossRef][Green Version]
- Kubota, T.; Komukai, K.; Miyanaga, S.; Shirasaki, K.; Oki, Y.; Yoshida, R.; Fukushima, K.; Kamba, T.; Okuyama, T.; Maehara, T.; et al. Out-of-Hospital Cardiac Arrest Does Not Affect Post-Discharge Survival in Patients With Acute Myocardial Infarction. Circ. Rep. 2021, 3, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Moulaert, V.R.; Verbunt, J.A.; Van Heugten, C.M.; Bakx, W.G.; Gorgels, A.P.; Bekkers, S.C.; De Krom, M.C.; Wade, D.T. Activity and Life After Survival of a Cardiac Arrest (ALASCA) and the effectiveness of an early intervention service: Design of a randomised controlled trial. BMC Cardiovasc. Disord. 2007, 7, 26. [Google Scholar] [CrossRef] [PubMed]




| Characteristics n (%) | n = 61 |
|---|---|
| Age (yo) | 59.4 ± 14.1 |
| Male sex | 47 (77.0) |
| Current smoking | 19 (31.1) |
| Hypertension | 25 (41.0) |
| Diabetes | 5 (8.2) |
| Dyslipidemia | 11 (18.0) |
| Body mass index, kg/m2 | 25.9 ± 4.9 |
| History of ischemic cardiopathy | 13 (21.3) |
| Chronic kidney disease | 5 (8.2) |
| Cardiopulmonary resuscitation: | |
| >Witness | |
| Bystander no. (%) | 21 (34.4) |
| Fireman no. (%) | 11 (18.0) |
| Doctor no. (%) | 18 (29.5) |
| Family no. (%) | 11 (18.0) |
| >Location of SCD | |
| Outdoor no. (%) | 25 (41.0) |
| Home no. (%) | 25 (41.0) |
| Emergency department no. (%) | 11 (18.0) |
| >Timeline | |
| No-Flow (min) | 1.9 ± 2.4 |
| Low-Flow (min) | 16.5 ± 10.4 |
| Total (m) | 18.3 ± 11.6 |
| Initial shockable rhythm no. (%) | 57 (93.4) |
| Dose of adrenaline (mg) | 1.31 ± 2.08 |
| STEMI on ECG after ROSC no. (%) | 36 (59.0) |
| LVEF after ROSC (%) | 35.4 ± 16.1 |
| >Main coronary lesion | |
| Left main coronary no. (%) | 1 (1.6) |
| Left anterior descending no. (%) | 25 (41.0) |
| Left circumflex no. (%) | 7 (11.5) |
| Right coronary no. (%) | 13 (21.3) |
| None | 15 (24.6) |
| >Biology | |
| hs-cTNT (ng/L) | 4818 ± 7342 |
| Creatinin peak (µmol/L) | 131 ± 109 |
| K+ (mmol/L) | 4.1 ± 0.66 |
| ASAT (UI/L) | 280 ± 260 |
| pH | 7.34 ± 0.1 |
| Lactate peak (mmol/L) | ± 1.9 |
| >Evolution | |
| Length of ICU stay (d) | 7.16 ± 8.32 |
| Length of hospital stay (d) | 18.9 ± 11.6 |
| Presence of wall motion abnormalities at entry no. (%) | 51 (83.6) |
| Implantable cardioverter defibrillator no. (%) | 19 (31.1) |
| LVEF > 50% at discharge no. (%) | 29 (47.5) |
| Transfer to rehabilitation centre at discharge no. (%) | 18 (29.5) |
| Event | 3 Months | 1 Year |
|---|---|---|
| Total survival no. (%) | 55 (100) | 52 (94.5) |
| CPC no. (%) | n = 55 | n = 52 |
| 1 | 43 (78.2) | 42 (80.7) |
| 2 | 7 (12.7) | 6 (11.5) |
| 3 | 5 (9.1) | 4 (7.7) |
| Death from cardiac cause no. (%) | 0 (0) | 0 (0) |
| NYHA | ||
| 1 | 28 (50.9) | 36 (69.2) |
| 2 | 27 (49.1) | 14 (26.9) |
| 3 | 0 (0) | 1 (2) |
| 4 | 0 (0) | 1 (2) |
| LVEF (%) Mean ± SD | 49 ± 11 | 51.5 ± 9.2 |
| Characteristic | Good Outcome (n = 48) | Poor Outcome (n = 7) | p Value |
|---|---|---|---|
| Age (y) | 57.4 ± 13.6 | 69.3 ± 9.4 | 0.036 |
| Male sex no. (%) | 35 (72.9) | 7 (100) | 0.18 |
| Body mass index kg/m2 | 26.7 ± 5 | 22.4 ± 2.2 | 0.013 |
| Current smoking no. (%) | 14 (29.2) | 3 (42.9) | 0.66 |
| Hypertension no. (%) | 20 (41.7) | 4 (57.1) | 0.69 |
| Diabetes no. (%) | 5 (10.4) | 0 (0) | 1 |
| Dyslipidemia no. (%) | 10 (20.8) | 1 (14.3) | 1 |
| CKD no. (%) | 4 (8.3) | 1 (14.3) | 0.51 |
| Low flow (min) | 16.4 ± 10.7 | 17 ± 9.3 | 0.72 |
| No flow (min) | 1.9 ± 2.5 | 2 ± 2.2 | 0.68 |
| Total CPR (min) | 18.3 ± 11.8 | 19 ± 11 | 0.65 |
| LAD culprit no. (%) | 18 (37.5) | 4 (57.1) | 0.78 |
| STEMI no. (%) | 28 (58.3) | 4 (57.1) | 0.5 |
| Occlusion no. (%) | 20 (41.7) | 3 (42.8) | 0.88 |
| Outdoor no. (%) | 19 (39.6) | 4 (57.1) | 0.22 |
| Home no. (%) | 22 (45.8) | 1 (14.3) | 0.22 |
| Witness no. (%) | 15 (31.3) | 4 (57.1) | 0.45 |
| Initial shockable no. (%) | 44 (91.7) | 7 (100) | 1 |
| Length of hospital stay (d) | 17.6 ± 12.5 | 31.7 ± 28.6 | 0.11 |
| Length of reanimation stay (d) | 7.5 ± 8.8 | 7.4 ± 7.7 | 0.93 |
| ASAT (UI/L) | 282 ± 240 | 356 ± 430 | 1 |
| K+ (mmol/L) | 4 ± 0.6 | 4.5 ± 0.7 | 0.16 |
| Lactate peak (mmol/L) | 2.8 ± 2 | 3.5 ± 2 | 0.23 |
| hs-cTNT (ng/L) | 4362 ± 6363 | 9417 ± 13,903 | 0.98 |
| Creatinin peak (µmol/L) | 140 ± 120 | 107 ± 29.3 | 0.88 |
| Initial LVEF (%) | 40.3 ± 12 | 32.1 ± 5.7 | 0.046 |
| LVEF at discharge (%) | 48.4 ± 11 | 41.4 ± 14.1 | 0.2 |
| LVEF at 3 months (%) | 50.1 ± 10.6 | 42.9 ± 12.5 | 0.13 |
| LVEF at 1 year (%) | 51.9 ± 9.3 | 46.3 ± 4.7 | 0.19 |
| Quality of Life (QOLIBRI) | Mean Score ± SD | Range of the Questionnaire |
|---|---|---|
| Part I: Satisfaction | 88.5 ± 20 | [20-140] |
| Cognition | 23.25 ± 6.3 | [5-35] |
| Self | 22.14 ± 5 | [5-35] |
| Daily life activities | 23.53 ± 7.2 | [5-35] |
| Social relationships | 19.56 ± 3.7 | [5-25] |
| Part II: Problems and complaints | 22.9 ± 8.3 | [10-40] |
| Emotion | 12 ± 4.6 | [5-20] |
| Physical problems | 10.9 ± 4 | [5-20] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Delbaere, Q.; Akodad, M.; Roubille, F.; Lattuca, B.; Cayla, G.; Leclercq, F. One-Year Follow-Up of Patients Admitted for Emergency Coronary Angiography after Resuscitated Cardiac Arrest. J. Clin. Med. 2022, 11, 3738. https://doi.org/10.3390/jcm11133738
Delbaere Q, Akodad M, Roubille F, Lattuca B, Cayla G, Leclercq F. One-Year Follow-Up of Patients Admitted for Emergency Coronary Angiography after Resuscitated Cardiac Arrest. Journal of Clinical Medicine. 2022; 11(13):3738. https://doi.org/10.3390/jcm11133738
Chicago/Turabian StyleDelbaere, Quentin, Myriam Akodad, François Roubille, Benoît Lattuca, Guillaume Cayla, and Florence Leclercq. 2022. "One-Year Follow-Up of Patients Admitted for Emergency Coronary Angiography after Resuscitated Cardiac Arrest" Journal of Clinical Medicine 11, no. 13: 3738. https://doi.org/10.3390/jcm11133738
APA StyleDelbaere, Q., Akodad, M., Roubille, F., Lattuca, B., Cayla, G., & Leclercq, F. (2022). One-Year Follow-Up of Patients Admitted for Emergency Coronary Angiography after Resuscitated Cardiac Arrest. Journal of Clinical Medicine, 11(13), 3738. https://doi.org/10.3390/jcm11133738