
Two Patterns of White Matter Connection in Multiple Gliomas: Evidence from Probabilistic Fiber Tracking


Abstract
:1. Introduction
2. Materials and Methods
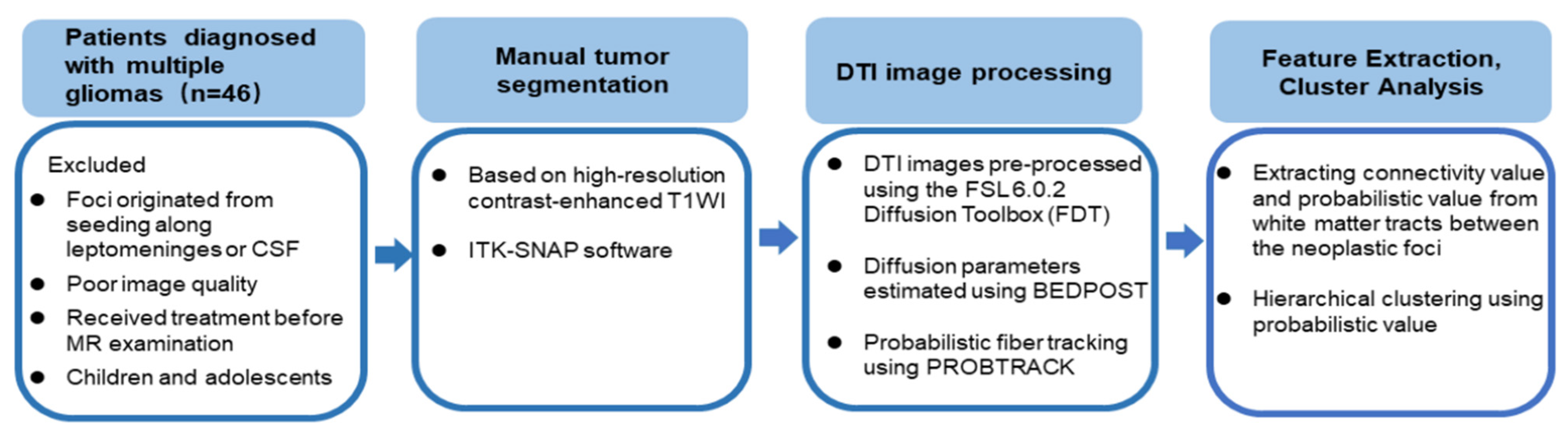
2.1. Subjects
2.2. Molecular Analyses
2.3. MRI Acquisition
2.4. Image Processing
2.4.1. DTI
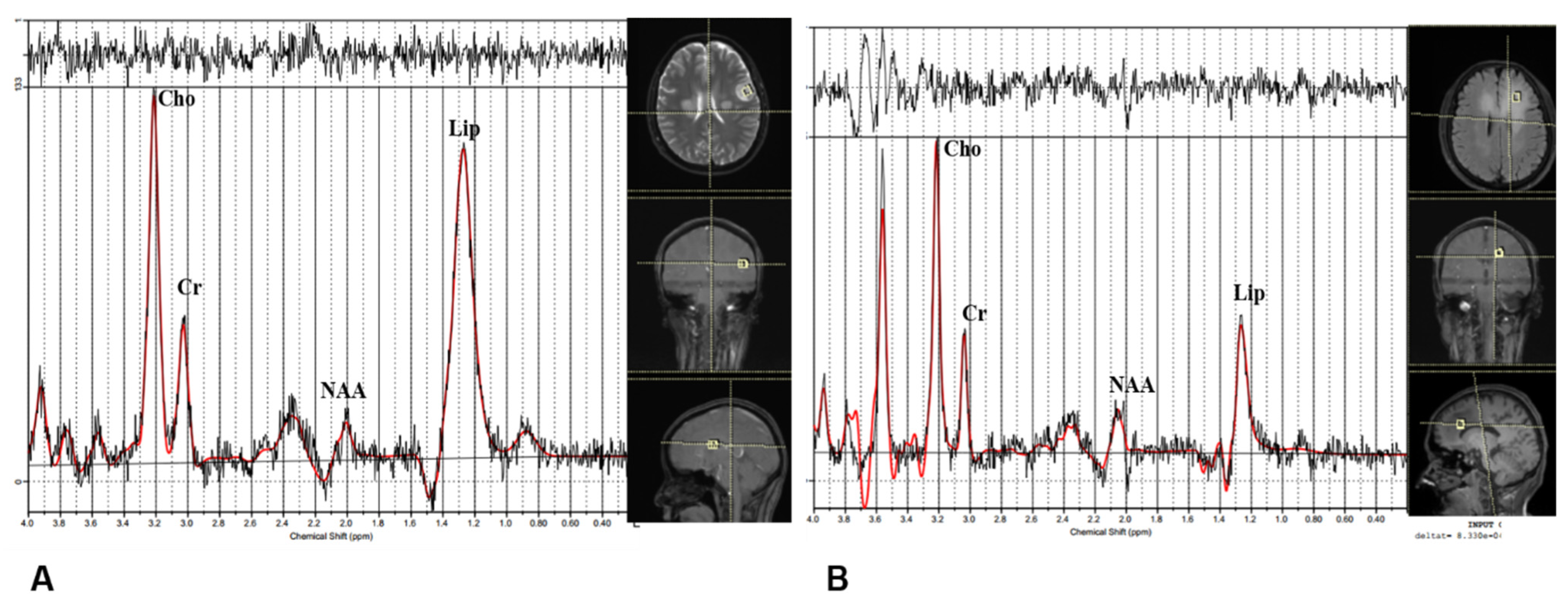
2.4.2. Other Advanced MR Imaging Modalities
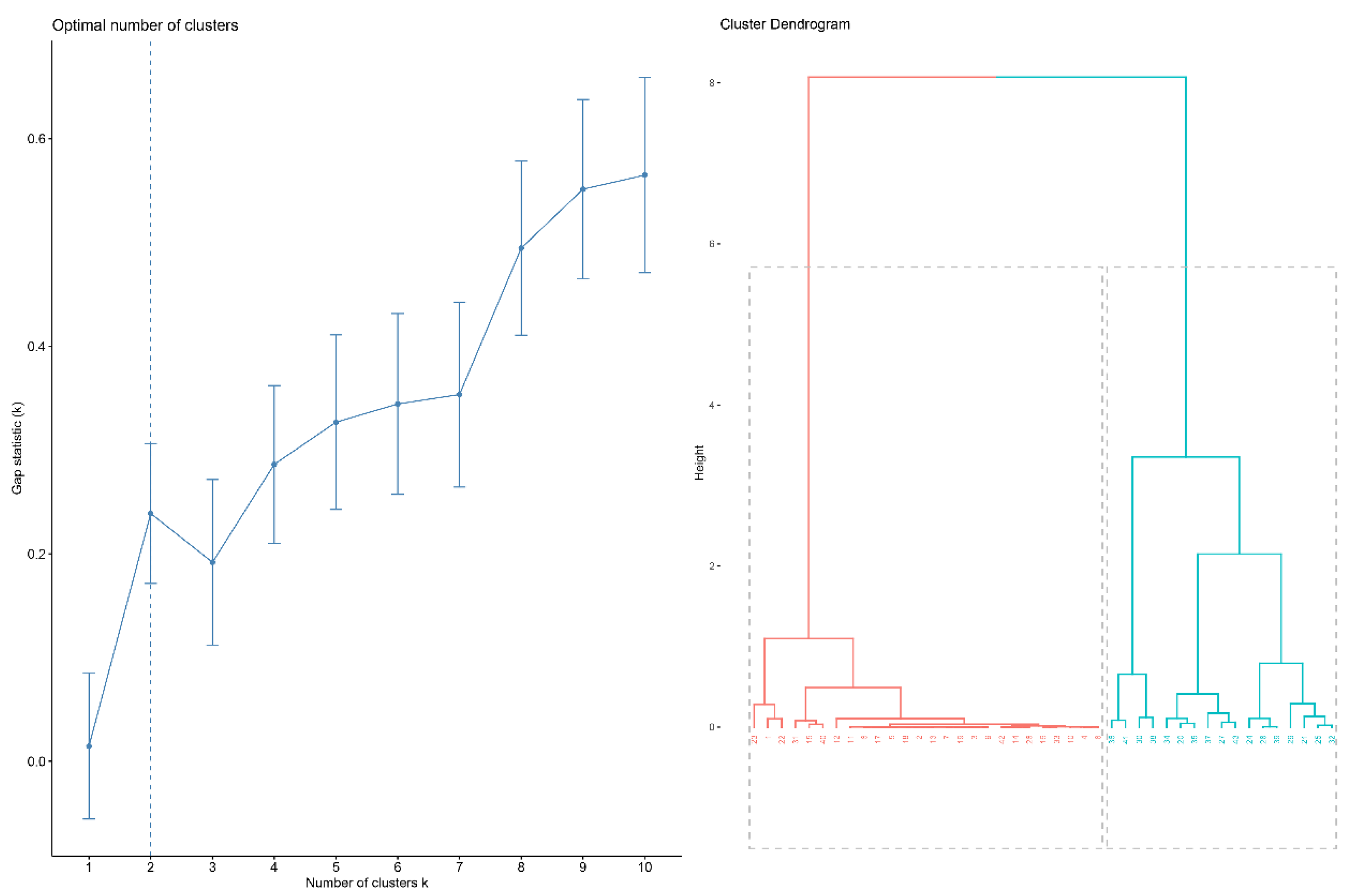
2.5. Cluster Analysis
2.6. Inter-Subgroup Comparison
3. Results
3.1. Demographic and Clinical Characteristics of the Patients
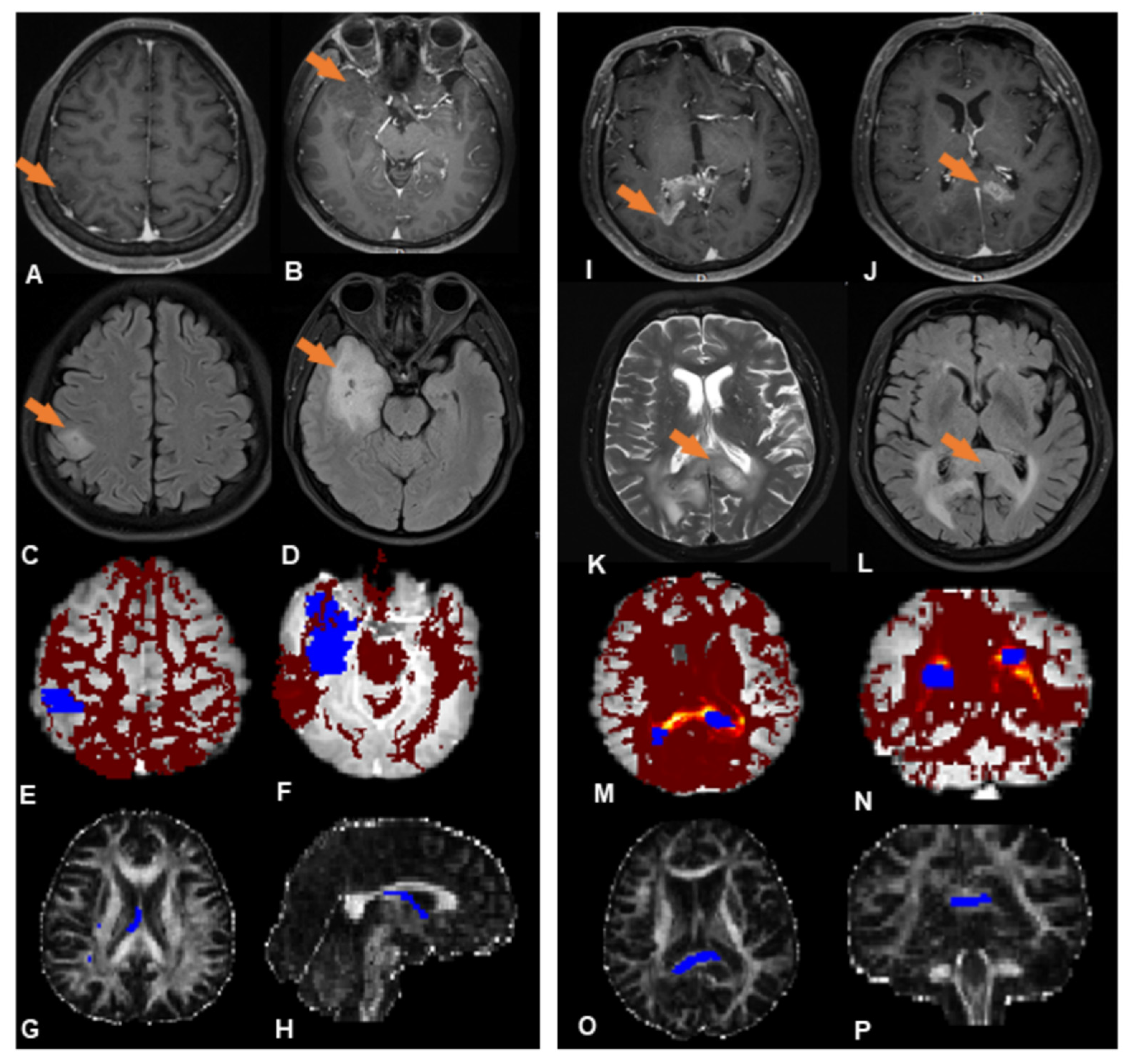
3.2. Probabilistic Fiber Tracking
3.3. Hierarchical Clustering
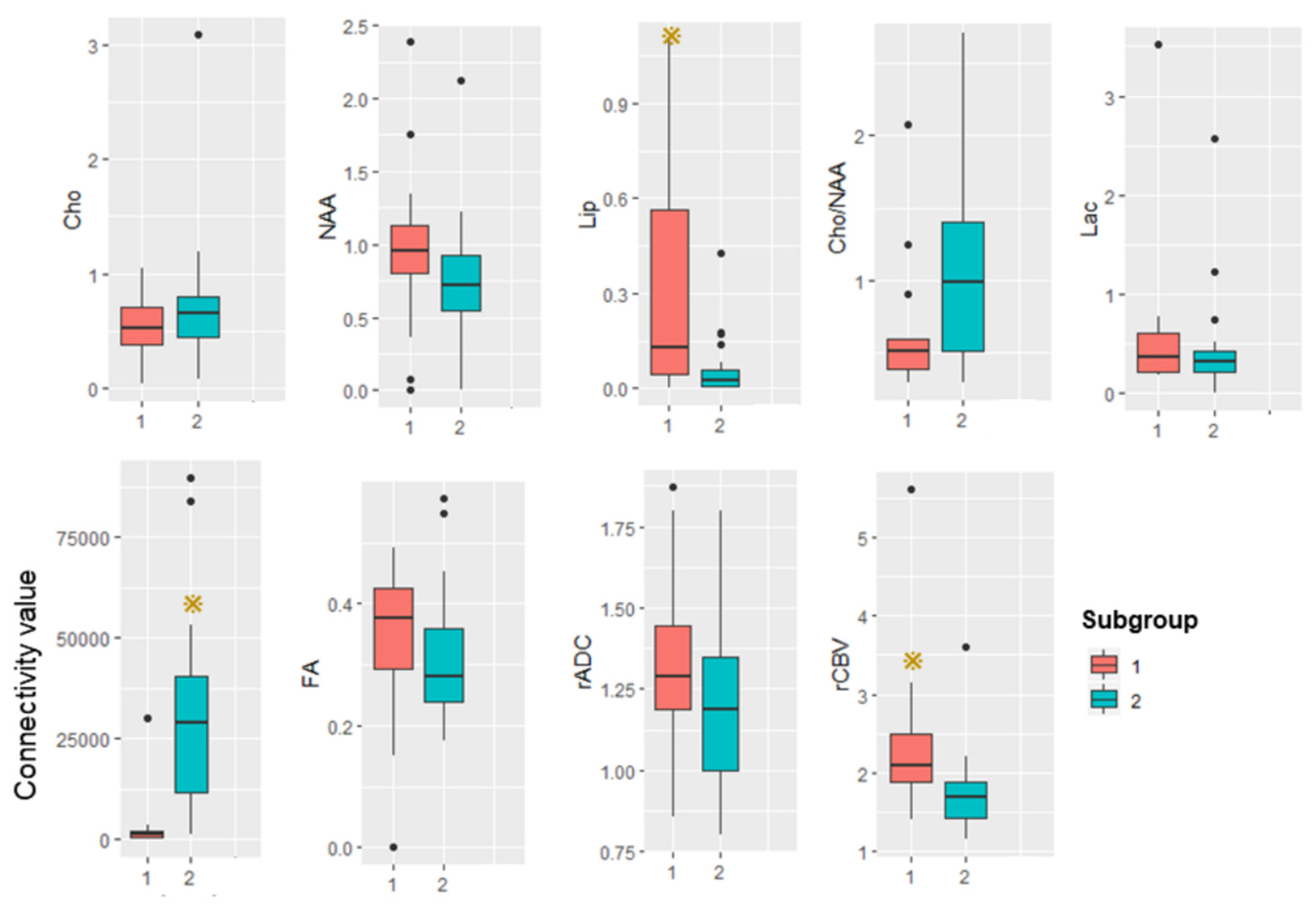
3.4. Subgroup Differences
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barnard, R.O.; Geddes, J.F. The incidence of multifocal cerebral gliomas. A histologic study of large hemisphere sections. Cancer 1987, 60, 1519–1531. [Google Scholar] [CrossRef]
- Batzdorf, U.; Malamud, N. the problem of multicentric gliomas. J. Neurosurg. 1963, 20, 122–136. [Google Scholar] [CrossRef] [PubMed]
- Djalilian, H.R.; Shah, M.V.; Hall, W.A. Radiographic incidence of multicentric malignant gliomas. Surg. Neurol. 1999, 51, 554–557; discussion 557–558. [Google Scholar] [CrossRef]
- Showalter, T.N.; Andrel, J.; Andrews, D.W.; Curran, W.J., Jr.; Daskalakis, C.; Werner-Wasik, M. Multifocal glioblastoma multiforme: Prognostic factors and patterns of progression. Int. J. Radiat. Oncol. Biol. Phys. 2007, 69, 820–824. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.P.; Xu, L.W.; Lober, R.M.; Li, G.; Nagpal, S. The incidence and significance of multiple lesions in glioblastoma. J. Neurooncol. 2013, 112, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Patil, C.G.; Yi, A.; Elramsisy, A.; Hu, J.; Mukherjee, D.; Irvin, D.K.; Yu, J.S.; Bannykh, S.I.; Black, K.L.; Nuno, M. Prognosis of patients with multifocal glioblastoma: A case-control study. J. Neurosurg. 2012, 117, 705–711. [Google Scholar] [CrossRef]
- Liu, Q.; Liu, Y.; Li, W.; Wang, X.; Sawaya, R.; Lang, F.F.; Yung WK, A.; Chen, K.; Fuller, G.N.; Zhang, W. Genetic, epigenetic, and molecular landscapes of multifocal and multicentric glioblastoma. Acta Neuropathol. 2015, 130, 587–597. [Google Scholar] [CrossRef] [Green Version]
- Abou-El-Ardat, K.; Seifert, M.; Becker, K.; Eisenreich, S.; Lehmann, M.; Hackmann, K.; Rump, A.; Meijer, G.; Carvalho, B.; Temme, A.; et al. Comprehensive molecular characterization of multifocal glioblastoma proves its monoclonal origin and reveals novel insights into clonal evolution and heterogeneity of glioblastomas. Neuro-Oncol. 2017, 19, 546–557. [Google Scholar] [CrossRef] [Green Version]
- Krex, D.; Mohr, B.; Appelt, H.; Schackert, H.K.; Schackert, G. Genetic analysis of a multifocal glioblastoma multiforme: A suitable tool to gain new aspects in glioma development. Neurosurgery 2003, 53, 1377–1384. [Google Scholar] [CrossRef]
- Akimoto, J.; Sasaki, H.; Haraoka, R.; Nakajima, N.; Fukami, S.; Kohno, M. Case of radiologically multicentric but genetically identical multiple glioblastomas. Brain Tumor Pathol. 2014, 31, 113–117. [Google Scholar] [CrossRef]
- Kim, J.; Lee, I.-H.; Cho, H.J.; Park, C.-K.; Jung, Y.-S.; Kim, Y.; Nam, S.H.; Kim, B.S.; Johnson, M.D.; Kong, D.-S. Spatiotemporal Evolution of the Primary Glioblastoma Genome. Cancer Cell 2015, 28, 318–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fares, Y.; Younes, M.; Kanj, A.; Barnes, P.R.; Muñiz, J. Multicentric glioma: Problems & interpretations [corrected]. P R Health Sci. J. 2009, 28, 75–79. [Google Scholar] [PubMed]
- Lombardi, G.; Della Puppa, A.; Gardiman, M.P.; Rossi, S.; Candiotto, C.; Zanatta, L.; Bertorelle, R.; De Rossi, A.; Fassan, M.; Zagonel, V. Discordance of IDH mutational status between lesions in an adult patient with multifocal glioma. Neuro-Oncol. 2018, 20, 1142–1143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arcos, A.; Romero, L.; Serramito, R.; Santin, J.M.; Prieto, A.; Gelabert, M.; Arraez, M.A. Multicentric glioblastoma multiforme. Report of 3 cases, clinical and pathological study and literature review. Neurocirugia 2012, 23, 211–215. [Google Scholar] [CrossRef]
- Van Tassel, P.; Lee, Y.Y.; Bruner, J.M. Synchronous and metachronous malignant gliomas: CT findings. AJNR Am. J. Neuroradiol. 1988, 9, 725–732. [Google Scholar]
- Painter, K.J.; Hillen, T. Mathematical modelling of glioma growth: The use of Diffusion Tensor Imaging (DTI) data to predict the anisotropic pathways of cancer invasion. J. Theor. Biol. 2013, 323, 25–39. [Google Scholar] [CrossRef]
- Mohan, S.; Wang, S.; Coban, G.; Kural, F.; Chawla, S.; O’Rourke, D.M.; Poptani, H. Detection of occult neoplastic infiltration in the corpus callosum and prediction of overall survival in patients with glioblastoma using diffusion tensor imaging. Eur. J. Radiol. 2019, 112, 106–111. [Google Scholar] [CrossRef]
- Price, S.J.; Peña, A.; Burnet, N.G.; Pickard, J.D.; Gillard, J.H. Detecting glioma invasion of the corpus callosum using diffusion tensor imaging. Br. J. Neurosurg. 2004, 18, 391–395. [Google Scholar] [CrossRef]
- Johansen-Berg, H.; Behrens, T.E. Just pretty pictures? What diffusion tractography can add in clinical neuroscience. Curr. Opin. Neurol. 2006, 19, 379–385. [Google Scholar] [CrossRef] [Green Version]
- Shakur, S.F.; Bit-Ivan, E.; Watkin, W.G.; Merrell, R.T.; Farhat, H.I. Multifocal and multicentric glioblastoma with leptomeningeal gliomatosis: A case report and review of the literature. Case Rep. Med. 2013, 2013, 132679. [Google Scholar] [CrossRef] [Green Version]
- Setty, P.; Hammes, J.; Rothämel, T.; Vladimirova, V.; Kramm, C.M.; Pietsch, T.; Waha, A. A pyrosequencing-based assay for the rapid detection of IDH1 mutations in clinical samples. J. Mol. Diagn. 2010, 12, 750–756. [Google Scholar] [CrossRef] [PubMed]
- Ikemura, M.; Shibahara, J.; Mukasa, A.; Takayanagi, S.; Aihara, K.; Saito, N.; Aburatani, H.; Fukayama, M. Utility of ATRX immunohistochemistry in diagnosis of adult diffuse gliomas. Histopathology 2016, 69, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Behrens, T.E.J.; Woolrich, M.W.; Jenkinson, M.; Johansen-Berg, H.; Nunes, R.G.; Clare, S.; Matthews, P.M.; Brady, J.M.; Smith, S.M. Characterization and propagation of uncertainty in diffusion-weighted MR imaging. Magn. Reson. Med. 2003, 50, 1077–1088. [Google Scholar] [CrossRef] [PubMed]
- Behrens, T.E.; Berg, H.J.; Jbabdi, S.; Rushworth, M.F.; Woolrich, M.W. Probabilistic diffusion tractography with multiple fibre orientations: What can we gain? Neuroimage 2007, 34, 144–155. [Google Scholar] [CrossRef]
- Shott, M.E.; Pryor, T.L.; Yang, T.T.; Frank, G.K.W. Greater Insula White Matter Fiber Connectivity in Women Recovered from Anorexia Nervosa. Neuropsychopharmacol. Off. Publ. Am. Coll. Neuropsychopharmacol. 2016, 41, 498–507. [Google Scholar] [CrossRef] [Green Version]
- Segobin, S.; Laniepce, A.; Ritz, L.; Lannuzel, C.; Boudehent, C.; Cabé, N.; Urso, L.; Vabret, F.; Eustache, F.; Beaunieux, H.; et al. Dissociating thalamic alterations in alcohol use disorder defines specificity of Korsakoff’s syndrome. Brain 2019, 142, 1458–1470. [Google Scholar] [CrossRef]
- Provencher, S.W. Estimation of metabolite concentrations from localized in vivo proton NMR spectra. Magn. Reson. Med. 1993, 30, 672–679. [Google Scholar] [CrossRef]
- Johnson, S.C. Hierarchical clustering schemes. Psychometrika 1967, 32, 241–254. [Google Scholar] [CrossRef]
- Tibshirani, R.; Walther, G.; Hastie, T. Estimating the Number of Clusters in a Data Set via the Gap Statistic. J. R. Statist. Soc. B 2002, 63, 411–423. [Google Scholar] [CrossRef]
- Di Carlo, D.T.; Cagnazzo, F.; Benedetto, N.; Morganti, R.; Perrini, P. Multiple high-grade gliomas: Epidemiology, management, and outcome. A systematic review and meta-analysis. Neurosurg. Rev. 2019, 42, 263–275. [Google Scholar] [CrossRef]
- di Russo, P.; Perrini, P.; Pasqualetti, F.; Meola, A.; Vannozzi, R. Management and outcome of high-grade multicentric gliomas: A contemporary single-institution series and review of the literature. Acta Neurochir. 2013, 155, 2245–2251. [Google Scholar] [CrossRef] [PubMed]
- Salvati, M.; Oppido, P.A.; Artizzu, S.; Fiorenza, F.; Puzzilli, F.; Orlando, E.R. Multicentric gliomas. Report of seven cases. Tumori 1991, 77, 518–522. [Google Scholar] [CrossRef] [PubMed]
- Budka, H.; Podreka, I.; Reisner, T.; Zeiler, K. Diagnostic and pathomorphological aspects of glioma multiplicity. Neurosurg. Rev. 1980, 3, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Giannopoulos, S.; Kyritsis, A.P. Diagnosis and management of multifocal gliomas. Oncology 2010, 79, 306–312. [Google Scholar] [CrossRef]
- Delgado, A.F.; Fahlstrom, M.; Nilsson, M.; Berntsson, S.G.; Zetterling, M.; Libard, S.; Alafuzoff, I.; van Westen, D.; Latt, J.; Smits, A.; et al. Diffusion Kurtosis Imaging of Gliomas Grades II and III—A Study of Perilesional Tumor Infiltration, Tumor Grades and Subtypes at Clinical Presentation. Radiol. Oncol. 2017, 51, 121–129. [Google Scholar] [CrossRef] [Green Version]
- Karlowee, V.; Amatya, V.J.; Hirano, H.; Takayasu, T.; Nosaka, R.; Kolakshyapati, M.; Yoshihiro, M.; Takeshima, Y.; Sugiyama, K.; Arita, K.; et al. Multicentric Glioma Develops via a Mutant IDH1-Independent Pathway: Immunohistochemical Study of Multicentric Glioma. Pathobiology 2017, 84, 99–107. [Google Scholar] [CrossRef]
- Jomin, M.; Lesoin, F.; Lozes, G.; Delandsheer, J.M.; Biondi, A.; Krivosic, I. Multifocal glioma. Apropos of 10 cases. Neuro-Chirurgie 1983, 29, 411–416. [Google Scholar]
- Oshiro, S.; Tsugu, H.; Komatsu, F.; Abe, H.; Onishi, H.; Ohmura, T.; Iwaasa, M.; Sakamoto, S.; Fukushima, T. Quantitative assessment of gliomas by proton magnetic resonance spectroscopy. Anticancer Res. 2007, 27, 3757–3763. [Google Scholar]
- Law, M.; Yang, S.; Babb, J.S.; Knopp, E.A.; Golfinos, J.G.; Zagzag, D.; Johnson, G. Comparison of cerebral blood volume and vascular permeability from dynamic susceptibility contrast-enhanced perfusion MR imaging with glioma grade. AJNR Am. J. Neuroradiol. 2004, 25, 746–755. [Google Scholar]
- Hassaneen, W.; Levine, N.B.; Suki, D.; Salaskar, A.L.; de Moura Lima, A.; McCutcheon, I.E.; Prabhu, S.S.; Lang, F.F.; DeMonte, F.; Rao, G.; et al. Multiple craniotomies in the management of multifocal and multicentric glioblastoma. J. Neurosurg. 2011, 114, 576–584. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | MPRAGE (3D T1WI) | Enhanced 3D T1WI | T2WI | FLAIR | DWI | DSC-PWI | 1H-MRS |
|---|---|---|---|---|---|---|---|
| Repetition time (ms) | 1630 | 1630 | 4500 | 6000 | 6000 | 1640 | 2000 |
| Echo time (ms) | 2.3 | 2.3 | 105 | 81 | 93 | 30 | 135 |
| Flip angle | 8° | 8° | 150° | 90° | 90° | 90° | 150° |
| Slice thickness (mm) | 1 | 1 | 5 | 5 | 3 | 5 | 5 |
| In-plane resolution (mm) | 0.5 × 1 | 0.5 × 1 | 0.5 × 0.5 | 0.7 × 0.7 | 1.8 × 1.8 | 1.7 × 1.3 | 0.5 × 0.5 |
| Acquisition time (s) | 187 | 200 | 58 | 62 | 206 | 105 | 394 |
| Directions | - | - | - | - | 30 | - | - |
| Characteristic | Subgroup | Statistical Analysis | ||
|---|---|---|---|---|
| 1 | 2 | Statistic | p | |
| Demographics | ||||
| Age (y) | 42.3 ± 14.2 | 41.8 ± 13.2 | 0.027 | 0.98 |
| Sex (male/female) | 8/11 | 17/10 | 1.96 | 0.16 |
| Histopathology | ||||
| Low grade (II) | 7 (37%) | 13 (48%) | 0.58 | 0.45 |
| High grade (III + IV) | 12 (63%) | 14 (52%) | - | - |
| IDHmut (with/without) | 10/9 | 11/16 | 0.64 | 0.44 |
| MGMTmet (with/without) | 12/7 | 10/17 | 3.05 | 0.081 |
| ATRX loss (with/without) | 9/10 | 12/15 | 0.038 | 0.85 |
| Ki-67 proliferation index | 0.15 ± 0.12 | 0.20 ± 0.16 | −1.07 | 0.29 |
| MR imaging | ||||
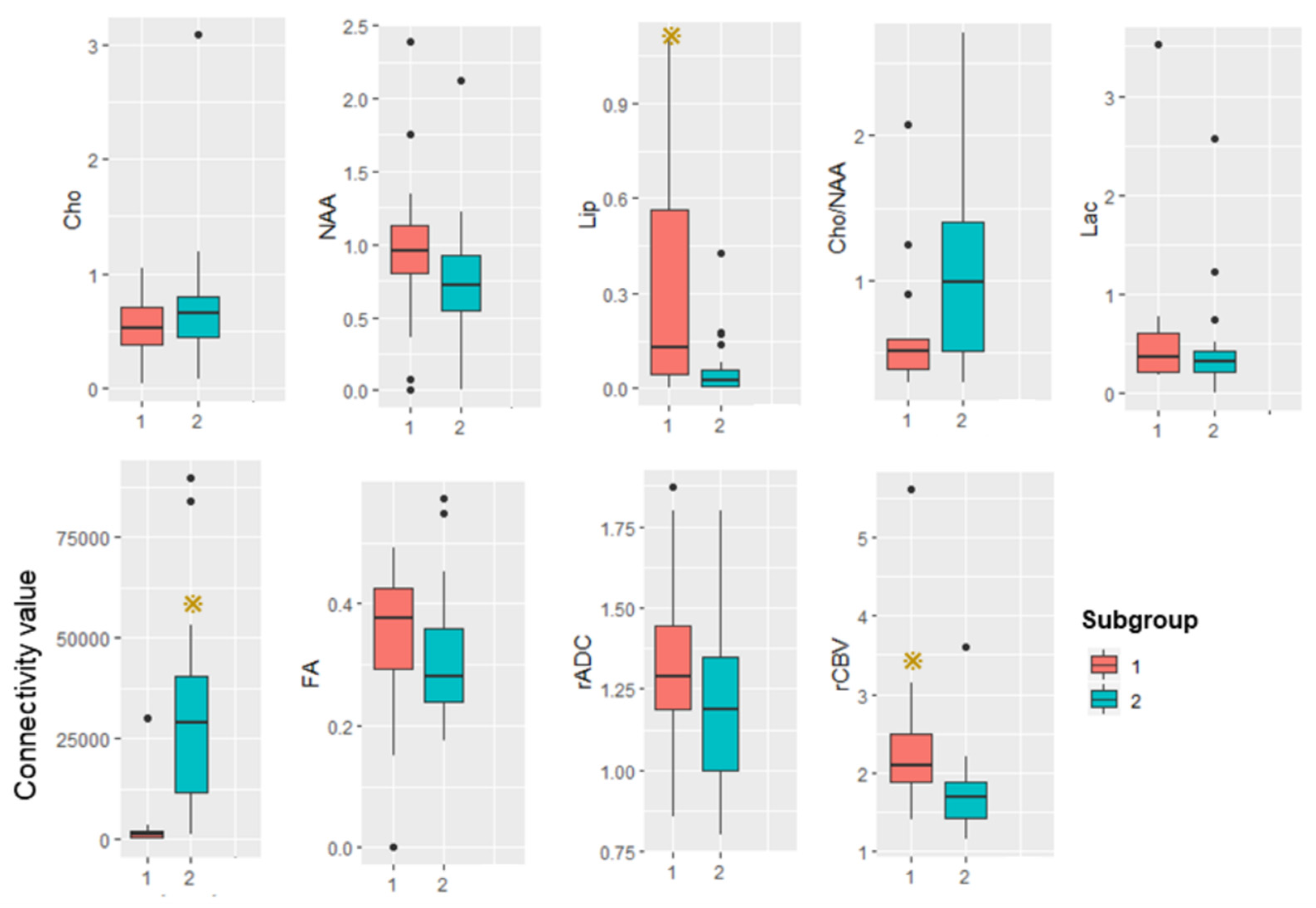
| Connectivity | 2675 ± 1098 | 30432 ± 22707 | −5.23 | p = 0.000016 * |
| FA | 0.34 ± 0.116 | 0.30 ± 0.108 | 1.15 | 0.26 |
| rCBV | 2.31 ± 0.95 | 1.73 ± 0.48 | −3.11 | 0.002 * |
| rADC | 1.32 ± 0.25 | 1.21 ± 0.27 | −1.58 | 0.12 |
| MR spectroscopy | ||||
| Cho/Cr | 0.52 ± 0.26 | 0.74 ± 0.57 | −1.49 | 0.14 |
| NAA/Cr | 0.96 ± 0.62 | 0.77 ± 0.41 | −1.43 | 0.14 |
| Cho/NAA | 1.07 ± 0.54 | 1.34 ± 0.42 | −1.49 | 0.13 |
| Lip/Cr | 0.32 ± 0.22 | 0.060 ± 0.051 | −2.71 | 0.006 * |
| Lac/Cr | 0.62 ± 0.85 | 0.45 ± 0.32 | −0.72 | 0.47 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, S.; Su, X.; Kemp, G.J.; Yang, X.; Wan, X.; Tan, Q.; Yue, Q.; Gong, Q. Two Patterns of White Matter Connection in Multiple Gliomas: Evidence from Probabilistic Fiber Tracking. J. Clin. Med. 2022, 11, 3693. https://doi.org/10.3390/jcm11133693
Zhang S, Su X, Kemp GJ, Yang X, Wan X, Tan Q, Yue Q, Gong Q. Two Patterns of White Matter Connection in Multiple Gliomas: Evidence from Probabilistic Fiber Tracking. Journal of Clinical Medicine. 2022; 11(13):3693. https://doi.org/10.3390/jcm11133693
Chicago/Turabian StyleZhang, Simin, Xiaorui Su, Graham J. Kemp, Xibiao Yang, Xinyue Wan, Qiaoyue Tan, Qiang Yue, and Qiyong Gong. 2022. "Two Patterns of White Matter Connection in Multiple Gliomas: Evidence from Probabilistic Fiber Tracking" Journal of Clinical Medicine 11, no. 13: 3693. https://doi.org/10.3390/jcm11133693
APA StyleZhang, S., Su, X., Kemp, G. J., Yang, X., Wan, X., Tan, Q., Yue, Q., & Gong, Q. (2022). Two Patterns of White Matter Connection in Multiple Gliomas: Evidence from Probabilistic Fiber Tracking. Journal of Clinical Medicine, 11(13), 3693. https://doi.org/10.3390/jcm11133693