
Influence of the Antithrombotic Therapy in the Healing of Simple Post-Extraction Sockets: A Randomized Clinical Trial

 ,
,  ,
,  ,
, 


Abstract
1. Introduction
2. Materials and Methods
- Patients above 18 years;
- Patients following long-term intake of oral anti-platelet therapy;
- Patients requiring extractions of a minimum of 1 single-rooted tooth/root.
- Patients refusing participation in the study and/or without written informed consent;
- Patients possessing a history of hypersensitivity or local anesthetic allergies;
- Patients following a treatment protocol of oral antiplatelet therapy for a period of less than three months;
- Immuno-supressed and immuno-compromised patients;
- Disabled patients;
- Patients with a state of acute infection related to the tooth to be extracted;
- Patients in treatment or treated with amino-bisphosphonates or antiresorptive drugs;
- Psychiatric patients;
- Patients with thrombocytopenia: primary or secondary to another disease (platelets < 40,000);
- Essential coagulation disorders patients (e.g., thrombocytosis);
- Congenital coagulation deficiencies patients (e.g., hemophilia);
- Patients with severe cirrhosis;
- Patients with severe chronic kidney disease;
- Patients with uncompensated diabetes;
- Patients who are pregnant or nursing;
- Patients requiring socket preservation in any of the included extractions sites;
- Patients performing radio- therapy and/or chemotherapy.
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Amler, M.H. The time sequence of tissue regeneration in human extraction wounds. Oral Surg. Oral Med. Oral Pathol. 1969, 27, 309–318. [Google Scholar] [CrossRef]
- Evian, C.I.; Rosenberg, E.S.; Coslet, J.G.; Corn, H. The Osteogenic Activity of Bone Removed from Healing Extraction Sockets in Humans. J. Periodontol. 1982, 53, 81–85. [Google Scholar] [CrossRef] [PubMed]
- Cardaropoli, G.; Araújo, M.; Lindhe, J. Dynamics of bone tissue formation in tooth extraction sites. J. Clin. Periodontol. 2003, 30, 809–818. [Google Scholar] [CrossRef] [PubMed]
- Araújo, M.G.; Lindhe, J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J. Clin. Periodontol. 2005, 32, 212–218. [Google Scholar] [CrossRef]
- Zabojszcz, M.; Malinowski, K.P.; Janion-Sadowska, A.; Lillis, T.; Ziakas, A.; Sławska, A.; Janion, M.; Siudak, Z. Safety of dental extractions in patients on dual antiplatelet therapy—A meta-analysis. Postepy Kardiol Interwencyjnej 2019, 15, 68–73. [Google Scholar] [CrossRef]
- Perry, D.J.; Noakes, T.J.C.; Helliwell, P.S. Guidelines for the management of patients on oral anticoagulants requiring dental surgery. Nat. Publ. Group 2013, 13, 389–393. [Google Scholar] [CrossRef]
- Curto, A.; Albaladejo, A.; Alvarado, A. Dental management of patients taking novel oral anticoagulants (NOAs): Dabigatran. J. Clin. Exp. Dent. 2017, 9, 289–293. [Google Scholar] [CrossRef][Green Version]
- Caliskan, M.; Tükel, H.C.; Benlidayi, E.; Deniz, A. Is it necessary to alter anticoagulation therapy for tooth extraction in patients taking direct oral anticoagulants? Med. Oral Patol. Oral Cir. Bucal 2017, 22, 767–773. [Google Scholar] [CrossRef]
- Landry, R.G.; Turnbell, R.S.; Howley, T. Effectiveness of Benzydamine HCL i Treatment of Periodontal Post-Surgical Patients; Faculty of Dentistry, University of Toronto: Toronto, ON, USA, 1985. [Google Scholar]
- Halley, D.; Weld-Moore, R.; Duane, B. No evidence for stopping long-term aspirin therapy before tooth extraction. Evid.-Based Dent. 2015, 16849, 118–119. [Google Scholar] [CrossRef]
- Zhao, B.; Wang, P.; Dong, Y.; Zhu, Y.; Zhao, H. Should aspirin be stopped before tooth extraction? A meta-analysis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2015, 119, 522–530. [Google Scholar] [CrossRef]
- Sadeghi-Ghahrody, M.; Yousefi-Malekshah, S.H.; Karimi-Sari, H.; Yazdanpanah, H.; Rezaee-Zavareh, M.S.; Yavarahmadi, M. Bleding after tooth extraction in patients taking aspirin and clopidogrel (Plavix) compared with healthy controls. Br. J. Oral Maxillofac. Surg. 2016, 54, 568–572. [Google Scholar] [CrossRef]
- Werner, S.; Grose, R. Regulation of wound healing by growth factors and cytokines. Physiol. Rev. 2003, 83, 835–870. [Google Scholar] [CrossRef]
- Sammartino, G.; Marenzi, G.; Howard, C.M.; Minimo, C.; Trosino, O.; Califano, L.; Claudio, P.P. Chondrosarcoma of the jaw: A closer look at its management. J. Oral Maxillofac. Surg. 2008, 66, 2349–2355. [Google Scholar] [CrossRef]
- Paolantoni, G.; Marenzi, G.; Blasi, A.; Mignogna, J.; Sammartino, G. Findings of a Four-Year Randomized Controlled Clinical Trial Comparing Two-Piece and One-Piece Zirconia Abutments Supporting Single Prosthetic Restorations in Maxillary Anterior Region. BioMed Res. Int. 2016, 2016, 8767845. [Google Scholar] [CrossRef]
- Marenzi, G.; Riccitiello, F.; Tia, M.; di Lauro, A.; Sammartino, G. Influence of Leukocyte- and Platelet-Rich Fibrin (L-PRF) in the Healing of Simple Postextraction Sockets: A Split-Mouth Study. BioMed Res. Int. 2015, 2015, 369273. [Google Scholar] [CrossRef]
- Singer, A.J.; Clark, R.A. Cutaneous wound healing. N. Engl. J. Med. 1999, 341, 738–746. [Google Scholar] [CrossRef]
- Mazzucco, L.; Borzini, P.; Gope, R. Platelet-derived factors involved in tissue repairfrom signal to function. Transfus. Med. Rev. 2010, 24, 218–234. [Google Scholar] [CrossRef]
- Nissen, N.N.; Polverini, P.; Koch, A.E.; Volin, M.V.; Gamelli, R.L.; DiPietro, L.A. Vascular endothelial growth factor mediates angiogenic activity during the proliferative phase of wound healing. Am. J. Pathol. 1998, 152, 1445–1452. [Google Scholar]
- Lynch, K.M.; Ahsan, T. Correlating the effects of bone morphogenic protein to secreted soluble factors from fibroblasts and mesenchymal stem cells in regulating regenerative processes in vitro. Tissue Eng. Part A 2014, 20, 3122–3129. [Google Scholar] [CrossRef]
- Förster, Y.; Schmidt, J.R.; Wissenbach, D.K.; Pfeiffer, S.E.; Baumann, S.; Hofbauer, L.C.; Von Bergen, M.; Kalkhof, S.; Rammelt, S. Microdialysis Sampling from Wound Fluids Enables Quantitative Assessment of Cytokines, Proteins, and Metabolites Reveals Bone Defect-Specific Molecular Profiles. PLoS ONE 2016, 11, e0159580. [Google Scholar] [CrossRef]
- Reid, I.R.; Bolland, M.J.; Grey, A.B. Is bisphosphonate-associated osteonecrosis of the jaw caused by soft tissue toxicity? Bone Sep. 2007, 41, 318–320. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| NAME | AGE | GENDER | GROUP |
|---|---|---|---|
| F. A. | 53 | male | Control |
| D. C. | 48 | male | Control |
| N. L. | 69 | female | Control |
| B. T. | 22 | female | Control |
| C. V. | 65 | male | Control |
| C. S. | 50 | male | Control |
| D. A. | 43 | male | Control |
| C. M. | 56 | male | Control |
| B. C. | 47 | male | Control |
| C. E. | 51 | female | Control |
| B. G. | 55 | male | Control |
| R. A. | 61 | female | Control |
| P. C. | 56 | female | Control |
| T. A. | 47 | female | Control |
| E. A. | 50 | female | Control |
| L. M. | 46 | female | Control |
| I. L. | 68 | male | Control |
| M. M. | 60 | male | Control |
| I. A. | 54 | male | Control |
| C. M. | 48 | female | Control |
| D. M. | 64 | male | Control |
| E. M. | 77 | male | Control |
| C. A. | 64 | female | Control |
| G. A. | 61 | female | Control |
| A. V. | 63 | female | Control |
| I. G. | 78 | male | Control |
| M. R. | 54 | female | Control |
| P. M. | 60 | female | Control |
| S. A. | 63 | male | Control |
| P. S. | 43 | female | Test |
| D. T. | 78 | female | Test |
| P. P. | 89 | female | Test |
| D. M. | 45 | female | Test |
| A. R. | 74 | male | Test |
| L. A. | 65 | male | Test |
| L. L. | 77 | male | Test |
| M. B. | 71 | female | Test |
| R. A. | 55 | female | Test |
| B. S. | 76 | male | Test |
| L. G. | 50 | male | Test |
| A. F. | 64 | male | Test |
| A. V. | 72 | male | Test |
| B. A. | 58 | male | Test |
| D. R. | 60 | male | Test |
| I. A. | 67 | female | Test |
| P. S. | 73 | male | Test |
| F. G. | 56 | male | Test |
| P. R. | 64 | male | Test |
| M. M. | 70 | female | Test |
| A. M. | 60 | male | Test |
| C. B. | 26 | female | Test |
| E. C. | 73 | male | Test |
| M. F. | 59 | male | Test |
| S. T. | 63 | male | Test |
| M. F. | 87 | female | Test |
| C. R. | 50 | male | Test |
| G. T. | 67 | male | Test |
| O.M. | 48 | male | Test |
| Tissue colour: | 50% of gingiva red |
| Granulation tissue: | Present | |
| Incision margin: | Not epithelialized, with loss of epithelium beyond incision margin | |
| Suppuration: | Present | |
| Tissue colour: | 50% of gingiva red |
| Granulation tissue: | Present | |
| Incision margin: | Not epithelialized, with connective tissue exposed | |
| Suppuration: | None | |
| Tissue colour: | 50% of gingiva red |
| Granulation tissue: | None | |
| Incision margin: | No connective tissue exposed | |
| Suppuration: | None | |
| Tissue colour: | 25% of gingiva red |
| Granulation tissue: | None | |
| Incision margin: | No connective tissue exposed | |
| Suppuration: | None | |
| Tissue colour: | All tissues pink |
| Granulation tissue: | None | |
| Incision margin: | No connective tissue exposed | |
| Suppuration: | None |
| Test Group | Control Group | Significance | |||
|---|---|---|---|---|---|
| Mean ± Std Dev | Median; IQR | Mean ± Std Dev | Median; IQR | ||
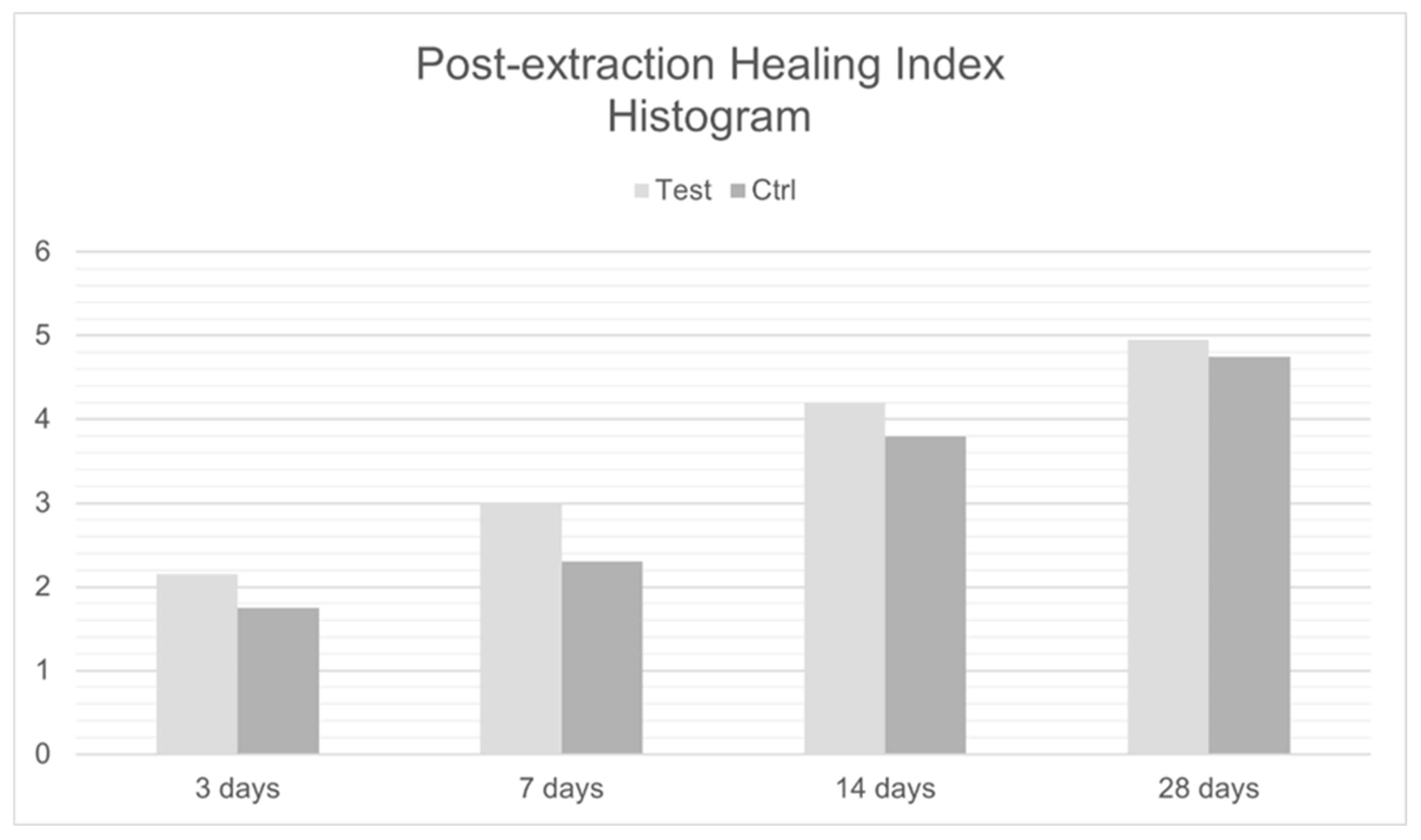
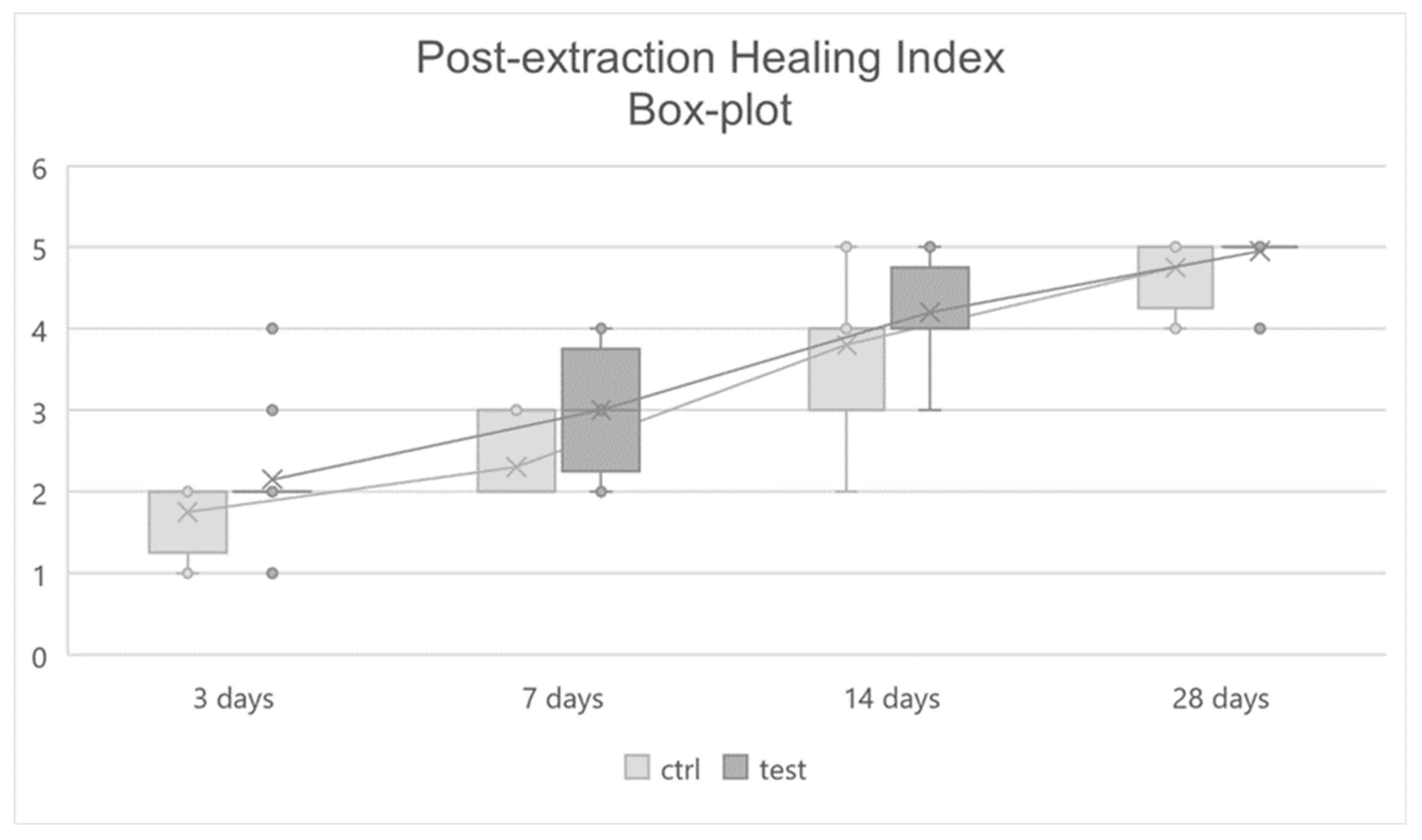
| 3 days | 2.15 ± 0.67 | 2; 0 | 1.75 ± 0.44 | 2; 0.25 | 0.038 |
| 7 days | 3 ± 0.73 | 3; 0.5 | 2.3 ± 0.47 | 2; 1 | 0.002 |
| 14 days | 4.2 ± 0.52 | 4; 0.25 | 3.8 ± 0.77 | 4; 1 | 0.074 |
| 28 days | 4.95 ± 0.22 | 5; 0 | 4.75 ± 0.44 | 5; 0.25 | 0.080 |
| Significance | 0.0001 | 0.0001 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sammartino, G.; Gasparro, R.; Spagnuolo, G.; Miniello, A.; Blasi, A.; Marenzi, G. Influence of the Antithrombotic Therapy in the Healing of Simple Post-Extraction Sockets: A Randomized Clinical Trial. J. Clin. Med. 2022, 11, 3654. https://doi.org/10.3390/jcm11133654
Sammartino G, Gasparro R, Spagnuolo G, Miniello A, Blasi A, Marenzi G. Influence of the Antithrombotic Therapy in the Healing of Simple Post-Extraction Sockets: A Randomized Clinical Trial. Journal of Clinical Medicine. 2022; 11(13):3654. https://doi.org/10.3390/jcm11133654
Chicago/Turabian StyleSammartino, Gilberto, Roberta Gasparro, Gianrico Spagnuolo, Alessandra Miniello, Andrea Blasi, and Gaetano Marenzi. 2022. "Influence of the Antithrombotic Therapy in the Healing of Simple Post-Extraction Sockets: A Randomized Clinical Trial" Journal of Clinical Medicine 11, no. 13: 3654. https://doi.org/10.3390/jcm11133654
APA StyleSammartino, G., Gasparro, R., Spagnuolo, G., Miniello, A., Blasi, A., & Marenzi, G. (2022). Influence of the Antithrombotic Therapy in the Healing of Simple Post-Extraction Sockets: A Randomized Clinical Trial. Journal of Clinical Medicine, 11(13), 3654. https://doi.org/10.3390/jcm11133654