
Effectiveness and Safety of High-Dose Dual Therapy: Results of the European Registry on the Management of Helicobacterpylori Infection (Hp-EuReg)


 , ,
, ,  , , , ,
, , , ,
Abstract
:
1. Introduction
2. Methods
2.1. European Registry on H. pylori Management
2.2. Data Collection
2.3. Study Aim
2.4. Selection Criteria
2.5. Data Management
2.6. Effectiveness Analysis
2.7. Safety and Compliance
3. Results
3.1. Baseline Characteristics
3.2. Treatment Lines
3.3. Prescriptions
3.4. HDDT Effectiveness
3.5. Effectiveness of HDDT + Bismuth
3.6. Compliance and Safety
4. Discussion
- The lower amoxicillin resistance rate of H. pylori compared to other antibiotics [21].
- The advantages of achieving and maintaining high plasma concentrations of amoxicillin thanks to the sequential administration of high doses of amoxicillin three or four times a day; some studies suggest that administering 750 mg of amoxicillin four times a day is superior to administering 1 g three times a day [10] and consider this regimen better than the standard triple, the standard triple with bismuth or the classic bismuth quadruple therapies [11].
- The powerful and persistent suppression of gastric acid secretion with the frequent administration of high PPI doses, and increasing H. pylori sensitivity to amoxicillin [22].
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Malfertheiner, P.; Megraud, F.; O’Morain, C.A.; Gisbert, J.P.; Kuipers, E.J.; Axon, A.T.; Bazzoli, F.; Gasbarrini, A.; Atherton, J.; Graham, D.Y.; et al. Management of Helicobacter pylori infection-the Maastricht V/Florence Consensus Report. Gut 2017, 66, 6–30. [Google Scholar] [CrossRef] [Green Version]
- Nyssen, O.P.; Bordin, D.; Tepes, B.; Pérez-Aisa, Á.; Vaira, D.; Caldas, M.; Bujanda, L.; Castro-Fernandez, M.; Lerang, F.; Leja, M.; et al. European Registry on Helicobacter pylori management (Hp-EuReg): Patterns and trends in first-line empirical eradication prescription and outcomes of 5 years and 21,533 patients. Gut 2021, 70, 40–54. [Google Scholar] [CrossRef] [PubMed]
- European Helicobacter pylori Study Group. Current European concepts in the management of Helicobacter pylori infection. The Maastricht Consensus Report. Gut 1997, 41, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Pieramico, O.; Zanetti, M.V.; Innerhofer, M.; Malfertheiner, P. Omeprazole-based dual and triple therapy for the treatment of Helicobacter pylori infection in peptic ulcer disease: A randomized trial. Helicobacter 1997, 2, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Wong, B.; Xiao, S.; Hu, P.; Qian, S.; Huang, N.; Li, Y.; Manan, C.; Lesmana, L.; Carpio, R.; Perez, J.Y.; et al. Comparison of lansoprazole-based triple and dual therapy for treatment of Helicobacter pylori-related duodenal ulcer: An Asian multicentre double-blind randomized placebo controlled study. Aliment. Pharmacol. Ther. 2000, 14, 217–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laine, L.; Stein, C.; Neil, G. Limited efficacy of omeprazole-based dual and triple therapy for Helicobacter pylori: A randomized trial employing “optimal” dosing. Am. J. Gastroenterol. 1995, 90, 1407–1410. [Google Scholar]
- Megraud, F.; Bruyndonckx, R.; Coenen, S.; Wittkop, L.; Huang, T.-D.; Hoebeke, M.; Bénéjat, L.; Lehours, P.; Goossens, H.; Glupczynski, Y. Helicobacter pylori resistance to antibiotics in Europe in 2018 and its relationship to antibiotic consumption in the community. Gut 2021, 70, 1815–1822. [Google Scholar] [CrossRef]
- Yang, X.; Wang, J.X.; Han, S.X.; Gao, C.P. High dose dual therapy versus bismuth quadruple therapy for Helicobacter pylori eradication treatment: A systematic review and meta-analysis. Medicine 2019, 98, e14396. [Google Scholar] [CrossRef]
- Gao, C.; Zhang, D.; Zhang, T.; Wang, J.; Han, S.; Graham, D.Y.; Lu, H. PPI-amoxicillin dual therapy for Helicobacter pylori infection: An update based on a systematic review and meta-analysis. Helicobacter 2020, 25, e12692. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Y.-J.; Zhang, Y.; Wang, T.-Y.; Zhao, J.-T.; Zhao, Z.; Zhu, J.-R.; Lan, C.-H. High dose PPI-amoxicillin dual therapy for the treatment of Helicobacter pylori infection: A systematic review with meta-analysis. Ther. Adv. Gastroenterol. 2020, 13, 1756284820937115. [Google Scholar] [CrossRef]
- Li, C.; Shi, Y.; Suo, B.; Tian, X.; Zhou, L.; Song, Z. PPI-amoxicillin dual therapy four times daily is superior to guidelines recommended regimens in the Helicobacter pylori eradication therapy within Asia: A systematic review and meta-analysis. Helicobacter 2021, 26, e12816. [Google Scholar] [CrossRef] [PubMed]
- Huang, Q.; Shi, Z.; Cheng, H.; Ye, H.; Zhang, X. Efficacy and Safety of Modified Dual Therapy as the First-line Regimen for the Treatment of Helicobacter pylori Infection: A Meta-Analysis of Randomized Controlled Trials. J. Clin. Gastroenterol. 2021, 55, 856–864. [Google Scholar] [CrossRef]
- McNicholl, A.G.; O’Morain, C.A.; Megraud, F.; Gisbert, J.P. Protocol of the European Registry on the management of Helicobacter pylori infection (Hp-EuReg). Helicobacter 2019, 24, e12630. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graham, D.Y.; Lu, H.; Dore, M.P. Relative potency of proton-pump inhibitors, Helicobacter pylori therapy cure rates, and meaning of double-dose PPI. Helicobacter 2019, 24, e12554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirchheiner, J.; Glatt, S.; Fuhr, U.; Klotz, U.; Meineke, I.; Seufferlein, T.; Brockmöller, J. Relative potency of proton-pump inhibitors-comparison of effects on intragastric pH. Eur. J. Clin. Pharmacol. 2009, 65, 19–31. [Google Scholar] [CrossRef]
- Al-Assi, M.T.; Cole, R.A.; Karttunen, T.J.; El-Zimaity, H.; Genta, R.M.; Graham, D.Y. Treatment of Helicobacter pylori infection with omeprazole-amoxicillin combination therapy versus ranitidine/sodium bicarbonate-amoxicillin. Am. J. Gastroenterol. 1995, 90, 1411–1414. [Google Scholar]
- Labenz, J.; Rühl, G.H.; Bertrams, J.; Börsch, G. Medium- and high-dose omeprazole plus amoxicillin for eradication of Helicobacter pylori in duodenal ulcer disease. Dig. Dis. Sci. 1994, 39, 1483–1487. [Google Scholar] [CrossRef]
- Rokkas, T.; Gisbert, J.P.; Malfertheiner, P.; Niv, Y.; Gasbarrini, A.; Leja, M.; Megraud, F.; O’Morain, C.; Graham, D.Y. Comparative Effectiveness of Multiple Different First-Line Treatment Regimens for Helicobacter pylori Infection: A Network Meta-analysis. Gastroenterology 2021, 161, 495–507. [Google Scholar] [CrossRef]
- Yun, J.; Wu, Z.; Qi, G.; Han, T.; Zhang, D. The high-dose amoxicillin-proton pump inhibitor dual therapy in eradication of Helicobacter pylori infection. Expert Rev. Gastroenterol. Hepatol. 2021, 15, 149–157. [Google Scholar] [CrossRef]
- Shiota, S.; Reddy, R.; Alsarraj, A.; El-Serag, H.B.; Graham, D.Y. Antibiotic Resistance of Helicobacter pylori among Male United States Veterans. Clin. Gastroenterol. Hepatol. 2015, 13, 1616–1624. [Google Scholar] [CrossRef] [PubMed]
- Miehlke, S.; Mannes, G.A.; Lehn, N.; Hele, C.; Stolte, M.; Bayerdörffer, E. An increasing dose of omeprazole combined with amoxycillin cures Helicobacter pylori infection more effectively. Aliment. Pharmacol. Ther. 1997, 11, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Shirai, N.; Furuta, T.; Moriyama, Y.; Okochi, H.; Kobayashi, K.; Takashima, M.; Xiao, F.; Kosuge, K.; Nakagawa, K.; Hanai, H.; et al. Effects of CYP2C19 genotypic differences in the metabolism of omeprazole and rabeprazole on intragastric pH. Aliment. Pharmacol. Ther. 2001, 15, 1929–1937. [Google Scholar] [CrossRef]
- Lou, H.Y.; Chang, C.C.; Sheu, M.T.; Chen, Y.C.; Ho, H.O. Optimal dose regimens of esomeprazole for gastric acid suppression with minimal influence of the CYP2C19 polymorphism. Eur. J. Clin. Pharmacol. 2009, 65, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Zou, P.Y.; Hu, J.; Zhao, J.T.; Zhao, Z.; Mei, H.; Yang, J.; Zhu, Y.J.; Zhang, Y.; Lan, C.H. 10-Day and 14-day high-dose dual therapy for the treatment of Helicobacter pylori: A propensity score matching analysis. Helicobacter 2021, 26, e12833. [Google Scholar] [CrossRef]
- Gisbert, J.P.; McNicholl, A.G. Optimization strategies aimed to increase the efficacy of H. pylori eradication therapies. Helicobacter 2017, 22, e12392. [Google Scholar] [CrossRef]
- Xu, H.; Wang, W.; Ma, X.; Feng, R.; Su, Y.; Cheng, L.; Yang, Y.; Zhang, D. Comparative efficacy and safety of high-dose dual therapy, bismuth-based quadruple therapy and non-bismuth quadruple therapies for Helicobacter pylori infection: A network meta-analysis. Eur. J. Gastroenterol. Hepatol. 2021, 33, 775–786. [Google Scholar] [CrossRef]
- Zullo, A.; Ridola, L.; De Francesco, V.; Gatta, L.; Hassan, C.; Alvaro, D.; Bellesia, A.; De Nucci, G.; Manes, G. High-dose esomeprazole and amoxicillin dual therapy for first-line Helicobacter pylori eradication: A proof of concept study. Ann. Gastroenterol. 2015, 28, 448–451. [Google Scholar]
- Sjomina, O.; Lielause, A.; Rudule, A.; Vangravs, R.; Parsutins, S.; Polaka, I.; Daugule, I.; Stonans, I.; Park, J.Y.; Leja, M. Randomised clinical trial: Comparison of efficacy and adverse effects of a standard triple clarithromycin-containing regimen with high-dose amoxicillin and bismuth therapy in Helicobacter pylori eradication. Eur. J. Cancer Prev. 2021, 31, 333–338. [Google Scholar] [CrossRef]
- Nyssen, O.P.; Perez-Aisa, A.; Tepes, B.; Castro-Fernandez, M.; Kupcinskas, J.; Jonaitis, L.; Bujanda, L.; Lucendo, A.; Jurecic, N.B.; Perez-Lasala, J.; et al. Adverse Event Profile during the Treatment of Helicobacter pylori: A Real-World Experience of 22,000 Patients from the European Registry on H. pylori Management (Hp-EuReg). Am. J. Gastroenterol. 2021, 116, 1220–1229. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Rescue Patients n/N (%) | |
|---|---|
| Amoxicillin | 40/41 (97.5%) |
| Clarithromycin | 38/41 (92.6%) |
| Levofloxacin/Moxifloxacin | 35/41 (85.3%) |
| Bismuth salts | 31/41 (75.6%) |
| Metronidazole/tinidazole | 30/41 (73.1%) |
| Tetracycline/Doxycycline | 24/41 (58.5%) |
| Rifabutin | 20/41 (48.7%) |
| Rifaximin | 4/41 (9.7%) |
| ITT n/N (%) | p * | PP n/N (%) | p * | mITT n/N (%) | p * | |
|---|---|---|---|---|---|---|
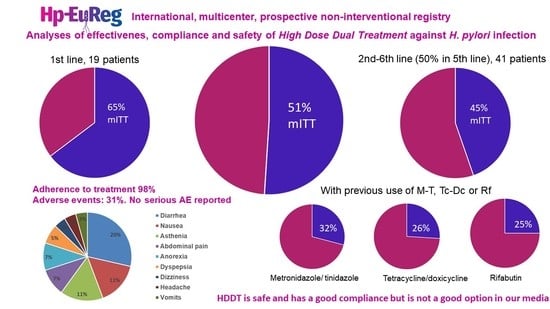
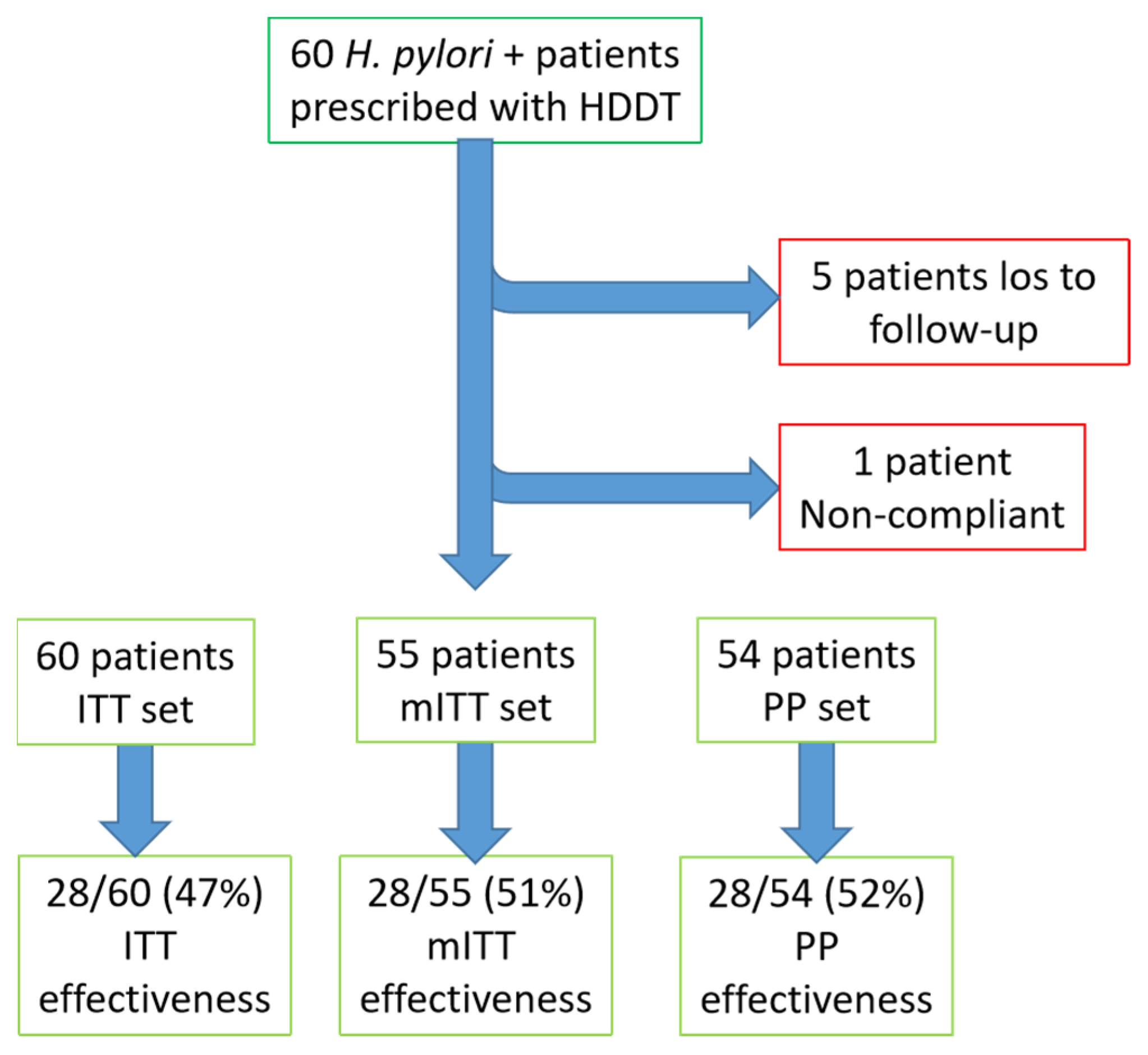
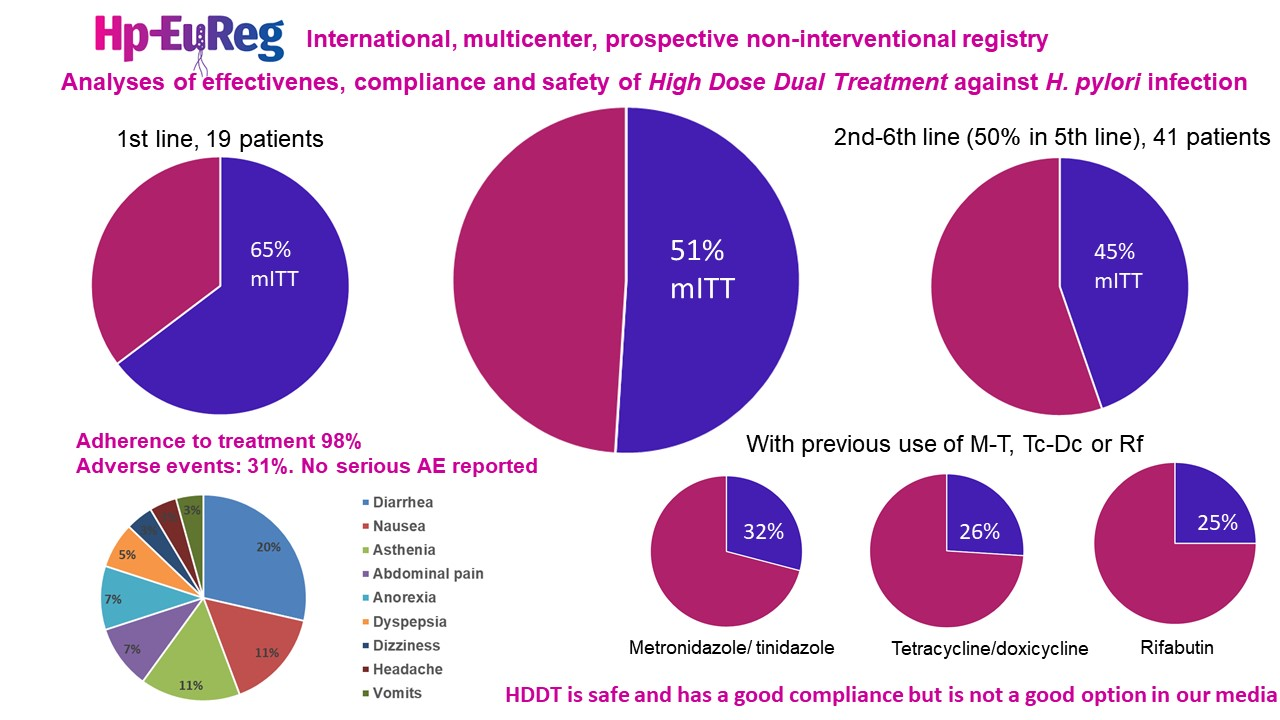
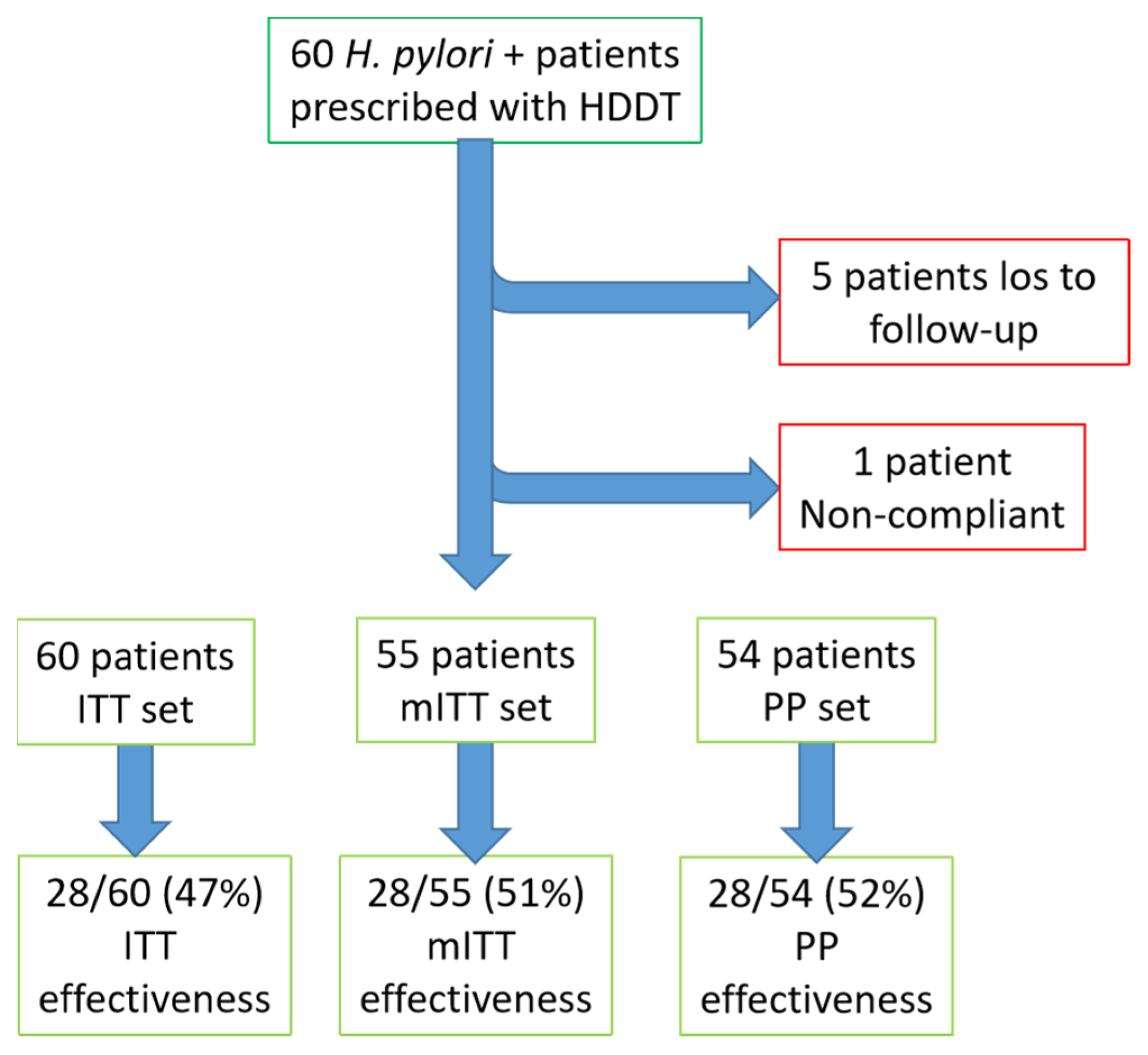
| HDDT overall | 28/60 (46.7%) CI 38–65 | 28/54 (51.9%) CI 38–65 | 28/55 (50.9%) CI 37–64 | |||
| HDDT 1st line ** | 11/19 (57.9%) CI 39–90 | 0.291 | 11/17 (64.7%) CI 39–90 | 0.278 | 11/17 (64.7%) CI 39–90 | 0.234 |
| HDDT rescue treatment (from 2nd to 6th line) *** | 15/35 (42.9%) CI 29–67 | 15/31 (48.4%) CI 29–67 | 15/32 (46.9%) CI 29–67 | |||
| HDDT rescue treatment (from 2nd to 6th line) | 17/41 (41.5%) CI 29–62 | 17/37 (45.9%) CI 29–62 | 17/38 (44.7%) CI 29–62 | |||
| HDDT 2nd line | 2/4 (50%) | 0.187 | 2/3 (66.7%) | 0.102 | 2/3 (66.7%) | 0.110 |
| HDDT 3rd line | 2/5 (40%) | 2/4 (50%) | 2/4 (50%) | |||
| HDDT 4th line | 1/ 2 (50%) | 1/ 2 (50%) | 1/ 2 (50%) | |||
| HDDT 5th line | 12/23 (52.2%) | 12/21 (57.1%) | 12/22 (54.5%) | |||
| HDDT 6th line | 0/7 (0%) | 0/7 (0%) | 0/7 (0%) |
| ITT n/N (%) | p | PP n/N (%) | p | mITT n/N (%) | p | ||||
|---|---|---|---|---|---|---|---|---|---|
| Not Previously Used | Previously Used | Not Previously Used | Previously Used | Not Previously Used | Previously Used | ||||
| A | 11/20 (55%) | 17/40 (42.5%) | 0.360 | 11/17 (64.7%) | 17/37 (45.9%) | 0.200 | 11/17 (64.7%) | 17/38 (45.9%) | 0.171 |
| C | 12/22 (54.5%) | 16/38 (42.1%) | 0.352 | 12/19 (63.2%) | 16/35 (45.7%) | 0.221 | 12/19 (63.7%) | 16/36 (44.4%) | 0.187 |
| M-T | 19/30 (63.3%) | 9/30 (30.1%) | 0.010 | 19/27 (70.4%) | 9/27 (33.3%) | 0.006 | 19/27 (70.4%) | 9/28 (32.1%) | 0.005 |
| L-Mx | 13/25 (52%) | 15/35 (42.9% | 0.484 | 13/22 (59.1%) | 15/32 (46.9%) | 0.377 | 13/22 (59.1%) | 15/33 (45.5%) | 0.322 |
| B | 15/29 (51.7%) | 13/31 (41.9%) | 0.448 | 15/24 (60%) | 13/29 (44.8%) | 0.266 | 15/25 (60%) | 13/30 (43.3%) | 0.218 |
| Tc-Dc | 22/36 (61.1%) | 6/24 (25%) | 0.006 | 22/32 (68.8%) | 6/22 (27.3%) | 0.003 | 22/32 (68.8%) | 6/23 (26.1%) | 0.002 |
| Rf | 23/40 (57.5%) | 5/20 (25%) | 0.017 | 23/35 (65.7%) | 5/19 (22.7%) | 0.006 | 23/35(65.7%) | 5/20 (25%) | 0.004 |
| ITT n/N (%) | p * | PP n/N (%) | p * | mITT n/N (%) | p * | |
|---|---|---|---|---|---|---|
| With B | 4/13 (30.8%) | 0.344 | 4/12 (33.3%) | 0.286 | 4/13 (30.8%) | 0.212 |
| Without B | 13/28 (46.4%) | 13/25 (52%) | 13/25 (52%) |
| Adverse Events | n/N (%) |
|---|---|
| Diarrhea | 11/55 (20%) |
| Nausea | 6/55 (11%) |
| Asthenia | 5/55 (11%) |
| Abdominal pain | 4/55 (7%) |
| Anorexia | 4/55 (7%) |
| Dyspepsia | 3/55 (5%) |
| Dizziness | 2/55 (3%) |
| Headache | 2/55 (3%) |
| Vomits | 2/55 (3%) |
| Heartburn | 0/55 (0%) |
| Metallic taste | 0/55 (0%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Salazar, L.; Campillo, A.; Rodrigo, L.; Pérez-Aisa, Á.; González-Santiago, J.M.; Segarra Ortega, X.; Denkovski, M.; Brglez Jurecic, N.; Bujanda, L.; Gómez Rodríguez, B.J.; et al. Effectiveness and Safety of High-Dose Dual Therapy: Results of the European Registry on the Management of Helicobacterpylori Infection (Hp-EuReg). J. Clin. Med. 2022, 11, 3544. https://doi.org/10.3390/jcm11123544
Fernández-Salazar L, Campillo A, Rodrigo L, Pérez-Aisa Á, González-Santiago JM, Segarra Ortega X, Denkovski M, Brglez Jurecic N, Bujanda L, Gómez Rodríguez BJ, et al. Effectiveness and Safety of High-Dose Dual Therapy: Results of the European Registry on the Management of Helicobacterpylori Infection (Hp-EuReg). Journal of Clinical Medicine. 2022; 11(12):3544. https://doi.org/10.3390/jcm11123544
Chicago/Turabian StyleFernández-Salazar, Luis, Ana Campillo, Luis Rodrigo, Ángeles Pérez-Aisa, Jesús M. González-Santiago, Xavier Segarra Ortega, Maja Denkovski, Natasa Brglez Jurecic, Luis Bujanda, Blas José Gómez Rodríguez, and et al. 2022. "Effectiveness and Safety of High-Dose Dual Therapy: Results of the European Registry on the Management of Helicobacterpylori Infection (Hp-EuReg)" Journal of Clinical Medicine 11, no. 12: 3544. https://doi.org/10.3390/jcm11123544
APA StyleFernández-Salazar, L., Campillo, A., Rodrigo, L., Pérez-Aisa, Á., González-Santiago, J. M., Segarra Ortega, X., Denkovski, M., Brglez Jurecic, N., Bujanda, L., Gómez Rodríguez, B. J., Ortuño, J., Georgopoulos, S., Jonaitis, L., Puig, I., Nyssen, O. P., Megraud, F., O’Morain, C., & Gisbert, J. P. (2022). Effectiveness and Safety of High-Dose Dual Therapy: Results of the European Registry on the Management of Helicobacterpylori Infection (Hp-EuReg). Journal of Clinical Medicine, 11(12), 3544. https://doi.org/10.3390/jcm11123544