
Comprehensive Clinical Characterisation of Brain Fog in Adults Reporting Long COVID Symptoms



Abstract
:1. Introduction
2. Methods and Materials
2.1. Study and Cohort Description
2.2. Procedures
2.2.1. Demographics
2.2.2. Symptomatology
2.2.3. Computer-Assisted Cognitive Tasks
2.2.4. Neurocardiovascular Assessment
2.2.5. Physical Performance Assessments
2.3. Statistical Analyses
2.4. Ethical Approval
3. Results
3.1. Sociodemographics and Medical History
3.2. Long COVID Symptomatology
3.3. Battery of Clinical Assessments
3.3.1. Computer-Assisted Cognitive Tasks
3.3.2. Neurocardiovascular Assessment
3.3.3. Gait Assessments
3.3.4. Strength Assessments
3.4. Multivariable Analyses
3.4.1. Binary Logistic Regression Model
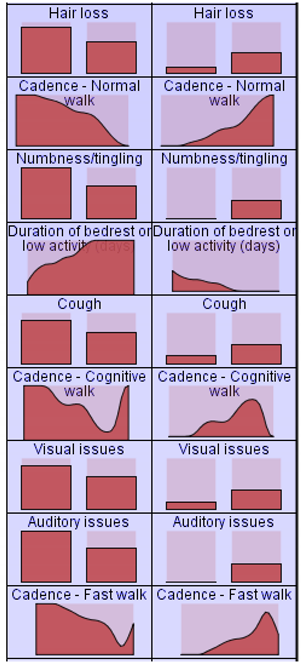
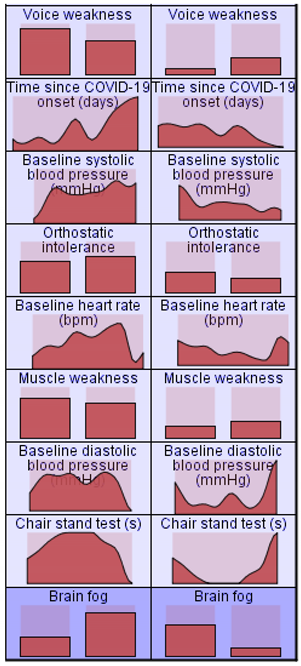
3.4.2. Cluster Analysis
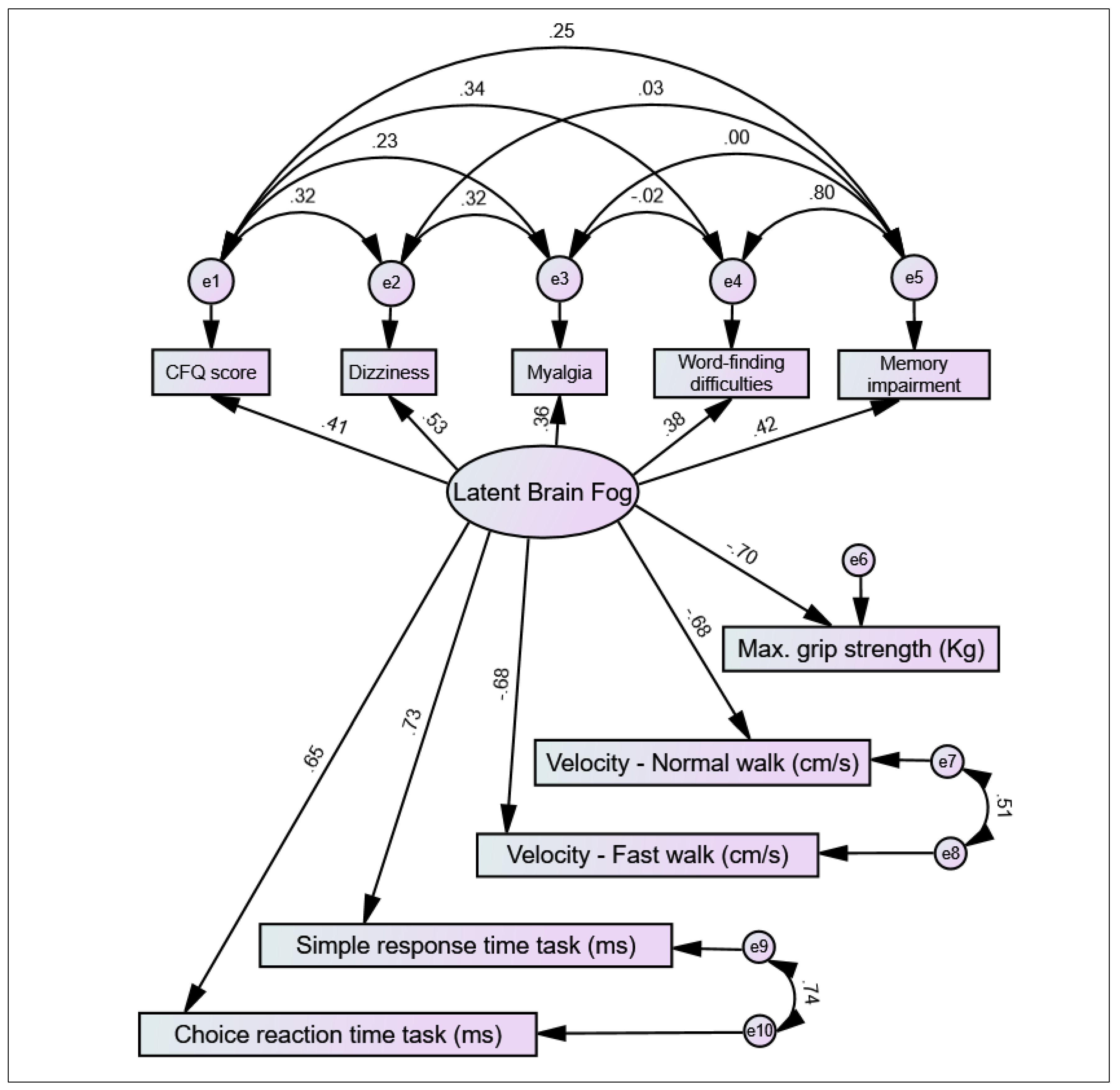
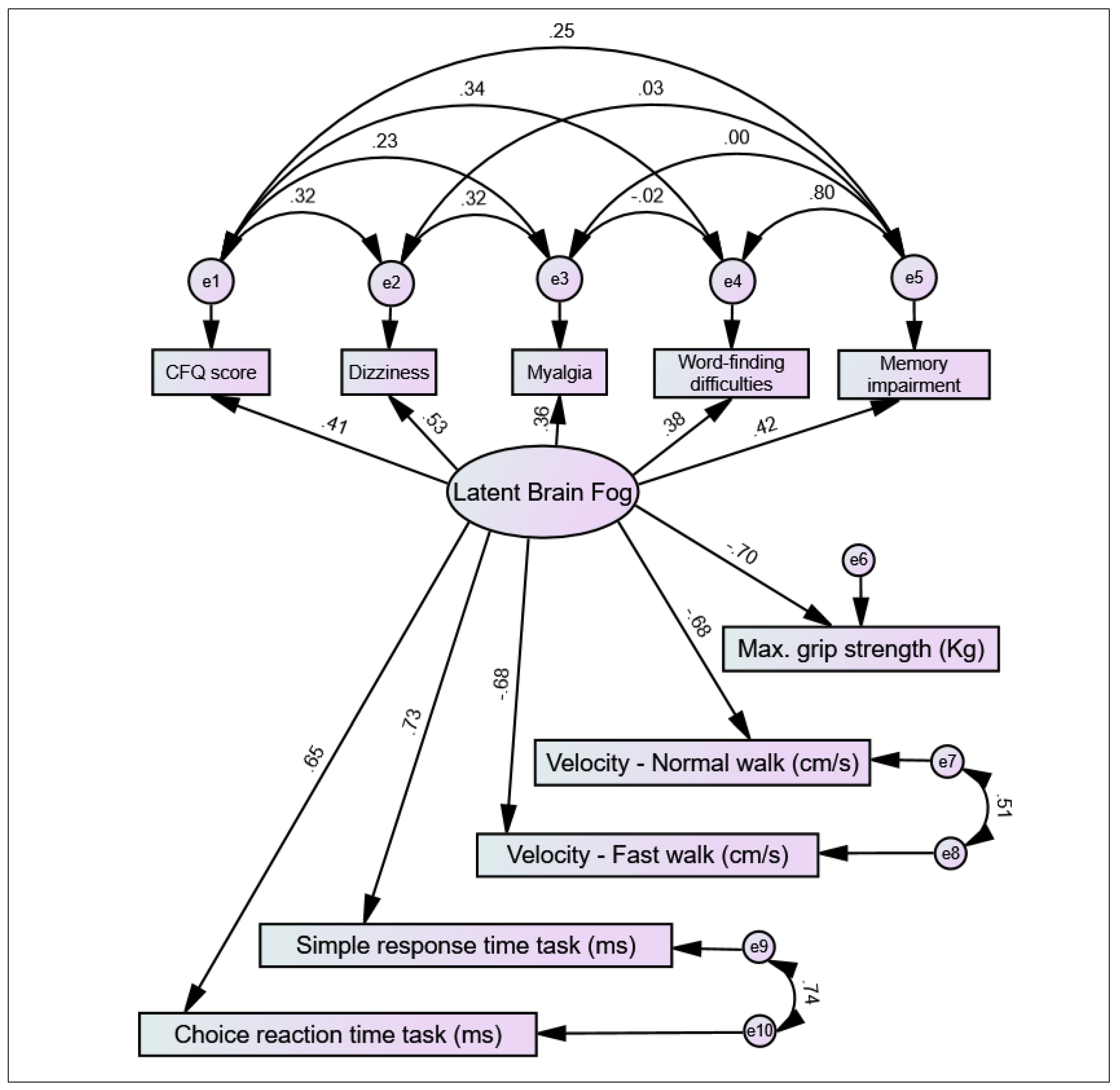
3.4.3. Structural Equation Model
4. Discussion
4.1. Statement of Principal Findings
4.2. Strengths and Weaknesses of the Study
4.3. Meaning of the Study
4.4. Unanswered Questions and Future Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Cluster | Cluster 1 | Cluster 2 | Cluster 1 | Cluster 2 |
|---|---|---|---|---|
| Label: | Brain Fog Cluster | Non-Brain Fog Cluster | (cont.) | (cont.) |
| Description | 81.1% in this cluster of 74 participants reported brain fog | 67.6% in this cluster of 34 participants did not report brain fog |  | |
| Size |  68.5% (74) |  31.5% (34) | ||
| Inputs Input (Predictor) Importance:   |  | |||
 |  | |||
References
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [PubMed]
- World Health Organisation. WHO Coronavirus (COVID-19) Dashboard: World Health Organisation. 2021. Available online: https://covid19.who.int/ (accessed on 7 April 2022).
- Grant, M.C.; Geoghegan, L.; Arbyn, M.; Mohammed, Z.; McGuinness, L.; Clarke, E.L.; Wade, R.G. The Prevalence of Symptoms in 24,410 Adults Infected by the Novel Coronavirus (SARS-CoV-2; COVID-19): A Systematic Review and Meta-Analysis of 148 Studies from 9 Countries. PLoS ONE 2020, 15, e0234765. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. A Clinical Case Definition of Post-COVID-19 Condition by a Delphi Consensus. 2021. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Post_COVID-19_condition-Clinical_case_definition-2021.1 (accessed on 7 April 2022).
- Jennings, G.; Monaghan, A.; Xue, F.; Mockler, D.; Romero-Ortuño, R. A Systematic Review of Persistent Symptoms and Residual Abnormal Functioning following Acute COVID-19: Ongoing Symptomatic Phase vs. Post-COVID-19 Syndrome. J. Clin. Med. 2021, 10, 5913. [Google Scholar] [CrossRef] [PubMed]
- Romero-Ortuño, R.; Jennings, G.; Xue, F.; Duggan, E.; Gormley, J.; Monaghan, A. Predictors of Submaximal Exercise Test Attainment in Adults Reporting Long COVID Symptoms. J. Clin. Med. 2022, 11, 2376. [Google Scholar] [CrossRef]
- Townsend, L.; Dyer, A.H.; Jones, K.; Dunne, J.; Mooney, A.; Gaffney, F.; O’Connor, L.; Leavy, D.; O’Brien, K.; Dowds, J.; et al. Persistent Fatigue Following SARS-CoV-2 Infection Is Common and Independent of Severity of Initial Infection. PLoS ONE 2020, 15, e0240784. [Google Scholar] [CrossRef]
- Asadi-Pooya, A.A.; Akbari, A.; Emami, A.; Lotfi, M.; Rostamihosseinkhani, M.; Nemati, H.; Barzegar, Z.; Kabiri, M.; Zeraatpisheh, Z.; Farjoud-Kouhanjani, M.; et al. Long COVID Syndrome-Associated Brain Fog. J. Med. Virol. 2021, 94, 979–984. [Google Scholar] [CrossRef]
- Ross, A.J.; Medow, M.S.; Rowe, P.C.; Stewart, J.M. What is Brain Fog? An Evaluation of the Symptom in Postural Tachycardia Syndrome. Clin. Auton. Res. 2013, 23, 305–311. [Google Scholar] [CrossRef]
- Ocon, A.J. Caught in the Thickness of Brain Fog: Exploring the Cognitive Symptoms of Chronic Fatigue Syndrome. Front. Physiol. 2013, 4, 63. [Google Scholar] [CrossRef] [Green Version]
- Ismail, Z.; Elbayoumi, H.; Fischer, C.E.; Hogan, D.B.; Millikin, C.P.; Schweizer, T.; Mortby, M.E.; Smith, E.E.; Patten, S.B.; Fiest, K.M. Prevalence of Depression in Patients With Mild Cognitive Impairment. JAMA Psychiatry 2017, 74, 58–67. [Google Scholar] [CrossRef]
- Musella, A.; Gentile, A.; Rizzo, F.R.; De Vito, F.; Fresegna, D.; Bullitta, S.; Vanni, V.; Guadalupi, L.; Bassi, S.M.; Buttari, F.; et al. Interplay Between Age and Neuroinflammation in Multiple Sclerosis: Effects on Motor and Cognitive Functions. Front. Aging Neurosci. 2018, 10, 238. [Google Scholar] [CrossRef]
- Jackson, C. The Chalder Fatigue Scale (CFQ 11). Occup. Med. 2014, 65, 86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eaton, W.W.; Smith, C.; Ybarra, M.; Muntaner, C.; Tien, A. Center for Epidemiologic Studies Depression Scale: Review and Revision (CESD and CESD-R). In The Use of Psychological Testing for Treatment Planning and Outcomes Assessment: Instruments for Adults; Maruish, M.E., Ed.; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 2004; pp. 363–377. [Google Scholar]
- Hyer, K.; Brown, L. The Impact of Event Scale—Revised: A Quick Measure of a Patient’s Response to Trauma. Am. J. Nurs. Sci. 2008, 108, 60–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stoet, G. PsyToolkit: A software package for programming psychological experiments using Linux. Behav. Res. Methods 2010, 42, 1096–1104. [Google Scholar] [CrossRef] [PubMed]
- Finucane, C.; Van Wijnen, V.K.; Fan, C.W.; Soraghan, C.; Byrne, L.; Westerhof, B.E.; Freeman, R.; Fedorowski, A.; Harms, M.P.; Wieling, W.; et al. A Practical Guide to Active Stand Testing and Analysis using Continuous Beat-to-Beat Non-Invasive Blood Pressure Monitoring. Clin. Auton. Res. 2019, 29, 427–441. [Google Scholar] [CrossRef]
- Monaghan, A.; Jennings, G.; Xue, F.; Byrne, L.; Duggan, E.; Romero-Ortuño, R. Orthostatic Intolerance in Adults Reporting Long COVID Symptoms was not Associated with Postural Orthostatic Tachycardia Syndrome. Front. Physiol. 2022, 13, 833650. [Google Scholar] [CrossRef]
- Xue, F.; Monaghan, A.; Jennings, G.; Byrne, L.; Foran, T.; Duggan, E.; Romero-Ortuño, R. A Novel Methodology for the Synchronous Collection and Multimodal Visualization of Continuous Neurocardiovascular and Neuromuscular Physiological Data in Adults with Long COVID. Sensors 2022, 22, 1758. [Google Scholar] [CrossRef]
- Espinosa Rodríguez, P.; Martínez Aguilar, A.; Ripoll Muñoz, M.P.; Rodríguez Navarro, M.Á. Long COVID: Is it really myalgic encephalomyelitis? Bibliographic review and considerations. Semergen 2022, 48, 63–69. [Google Scholar] [CrossRef]
- Wong, T.L.; Weitzer, D.J. Long COVID and myalgic encephalomyelitis/chronic fatigue syndrome: A systemic review and comparison of clinical presentation and symptomatology. Medicina 2021, 57, 418. [Google Scholar] [CrossRef]
- Poenaru, S.; Abdallah, S.J.; Corrales-Medina, V.; Cowan, J. COVID-19 and post-infectious myalgic encephalomyelitis/chronic fatigue syndrome: A narrative review. Ther. Adv. Infect. Dis. 2021, 8, 20499361211009385. [Google Scholar] [CrossRef]
- Komaroff, A.L.; Lipkin, W.I. Insights from myalgic encephalomyelitis/chronic fatigue syndrome may help unravel the pathogenesis of post-acute COVID-19 syndrome. Trends Mol. Med. 2021, 27, 895–906. [Google Scholar] [CrossRef]
- Sebaiti, M.A.; Hainselin, M.; Gouden, Y.; Sirbu, C.A.; Sekulic, S.; Lorusso, L.; Nacul, L.; Authier, F.J. Systematic review and meta-analysis of cognitive impairment in myalgic encephalomyelitis/chronic fatigue syndrome. Sci. Rep. 2022, 12, 2157. [Google Scholar] [CrossRef] [PubMed]
- Attree, E.A.; Arroll, M.A.; Dancey, C.P.; Griffith, C.; Bansal, A.S. Psychosocial factors involved in memory and cognitive failures in people with myalgic encephalomyelitis/chronic fatigue syndrome. Psychol. Res. Behav. Manag. 2014, 7, 67–76. [Google Scholar] [PubMed] [Green Version]
- Hunt, J.; Blease, C.; Geraghty, K.J. Long Covid at the crossroads: Comparisons and lessons from the treatment of patients with myalgic encephalomyelitis/chronic fatigue syndrome. J. Health Psychol. 2022, 27, 13591053221084494. [Google Scholar] [CrossRef] [PubMed]
- Hampshire, A.; Trender, W.; Chamberlain, S.R.; Jolly, A.E.; Grant, J.E.; Patrick, F.; Mazibuko, N.; Williams, S.C.; Barnby, J.M.; Hellyer, P.; et al. Cognitive Deficits in People who have Recovered from COVID-19. eClinicalMedicine 2021, 39, e101044. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Gabriel, U.; Gygax, P. Testing the Effectiveness of the Internet-Based Instrument PsyToolkit: A Comparison between Web-Based (PsyToolkit) and Lab-Based (E-Prime 3.0) Measurements of Response Choice and Response Time in a Complex Psycholinguistic Task. PLoS ONE 2019, 14, e0221802. [Google Scholar] [CrossRef] [PubMed]
- Pelà, G.; Goldoni, M.; Solinas, E.; Cavalli, C.; Tagliaferri, S.; Ranzieri, S.; Frizzelli, A.; Marchi, L.; Mori, P.A.; Majori, M.; et al. Sex-Related Differences in Long-COVID-19 Syndrome. J. Women’s Health 2022, 31, 620–630. [Google Scholar] [CrossRef] [PubMed]
- Thelle, D.S.; Laake, P. Epidemiology. In Planning and Preparation to Grant Application and Publication; Laake, P., Benestad, H.B., Olsen, B.R., Eds.; Academic Press: Cambridge, MA, USA, 2015; pp. 275–320. [Google Scholar]
- Hess, A.S.; Abd-Elsayed, A. Observational Studies: Uses and Limitations. In Pain; Abd-Elsayed, A., Ed.; Springer: Berlin/Heidelberg, Germany, 2019; pp. 123–125. [Google Scholar]
| With Brain Fog (n = 71) | Without Brain Fog (n = 37) | p-Value | ||||
|---|---|---|---|---|---|---|
| Sociodemographics: | ||||||
| (SD) | 46.4 | (9.5) | 46.1 | (11.7) | 0.912 ^ | |
| 77.1 | 59.5 | 0.055 § | ||||
| (SD) | 28.0 | (4.6) | 27.8 | (5.5) | 0.912 ^ | |
| Smoker, % | 42.5 | 37.1 | 0.284 § | |||
| Third-level education, % | 69.0 | 59.5 | 0.588 § | |||
| Health/Social care worker, % | 38.0 | 21.6 | 0.084 § | |||
| Comorbid medical conditions: | ||||||
| Hypertension, % | 16.7 | 28.6 | 0.238 § | |||
| Heart disease, % | 11.7 | 0.0 | 0.111 ++ | |||
| Respiratory disease, % | 16.7 | 14.3 | 0.551 ++ | |||
| Diabetes, % | 5.0 | 0.0 | 0.401 ++ | |||
| Medication: | ||||||
| Prescribed medication, % | 60.9 | 45.2 | 0.143 § | |||
| Antihypertensives, % | 10.3 | 12.9 | 0.471 ++ | |||
| β-blockers, % | 16.2 | 12.9 | 0.464 ++ | |||
| Antidepressants, % | 19.1 | 16.1 | 0.721 § | |||
| Benzodiazepines, % | 5.9 | 0.0 | 0.216 ++ | |||
| COVID-19 history: | ||||||
| Time post-COVID-19 onset (days), (SD) | 380.0 | (162.1) | 314.9 | (164.7) | 0.039 + | |
| Acute COVID-19 hospitalisation, % | 22.5 | 20.0 | 0.766 § | |||
| Acute COVID-19 ICU admission, % | 2.8 | 5.4 | 0.292 ++ | |||
| Duration of hospitalisation (days), (SD) | 15.5 | (17.7) | 16.0 | (13.0) | 0.622 + | |
| Duration of acute phase (days), (SD) | 20.1 | (16.8) | 15.3 | (12.4) | 0.336 + | |
| Duration of low activity (days), (SD) | 18.2 | (17.5) | 10.9 | (12.2) | 0.036 + | |
| Full vaccination against SARS-CoV-2, % | 86.9 | 85.0 | 0.656 § | |||
| With Brain Fog (n = 71) | Without Brain Fog (n = 37) | p-Value | With Brain Fog (n = 71) | Without Brain Fog (n = 37) | p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|
| Constitutional symptoms: | Respiratory symptoms: | ||||||||
| Fatigue, % | 98.6 | 94.6 | 0.270 ++ | Dyspnoea, % | 80.3 | 64.9 | 0.079 § | ||
| Hyperhidrosis, % | 56.3 | 27.0 | 0.004 § | Chest tightness, % | 62.0 | 45.9 | 0.111 § | ||
| Weight loss, % | 12.7 | 5.4 | 0.325 ++ | Throat pain, % | 42.3 | 18.9 | 0.015 § | ||
| Fever, % | 15.5 | 5.4 | 0.212 ++ | Cough, % | 36.6 | 16.2 | 0.028 § | ||
| Flushing, % | 12.7 | 2.7 | 0.159 ++ | Expectoration, % | 21.1 | 18.9 | 0.787 § | ||
| Neurological symptoms: | Voice weakness, % | 12.7 | 0.0 | 0.026 ++ | |||||
| Insomnia, % | 71.8 | 56.8 | 0.115 § | Gastrointestinal symptoms: | |||||
| Headache, % | 71.8 | 54.1 | 0.065 § | Diarrhoea, % | 31.0 | 24.3 | 0.468 § | ||
| Dizziness, % | 76.1 | 37.8 | <0.001 § | Loss of appetite, % | 29.6 | 16.2 | 0.128 § | ||
| Word-finding difficulties, % | 66.2 | 16.2 | <0.001 § | Nausea, % | 28.2 | 18.9 | 0.292 § | ||
| Memory impairment, % | 66.2 | 13.5 | <0.001 § | Constipation, % | 12.7 | 5.4 | 0.325 ++ | ||
| Eye irritation, % | 46.5 | 32.4 | 0.160 § | Bloating, % | 11.3 | 2.7 | 0.161 ++ | ||
| Visual issues, % | 31.0 | 13.5 | 0.047 § | Stomach pain, % | 14.1 | 2.7 | 0.093 ++ | ||
| Dysosmia, % | 25.4 | 8.1 | 0.032 § | Reflux, % | 9.9 | 2.7 | 0.259 ++ | ||
| Dysgeusia, % | 21.1 | 13.5 | 0.334 § | Vomiting, % | 5.6 | 0.0 | 0.297 ++ | ||
| Numbness/Tingling, % | 18.3 | 2.7 | 0.032 ++ | Dermatological symptoms: | |||||
| Auditory issues, % | 12.7 | 0.0 | 0.026 ++ | Skin marks/rashes, % | 47.1 | 21.6 | 0.010 § | ||
| Ear irritation, % | 4.2 | 5.4 | 1.000 ++ | Hair loss, % | 33.8 | 13.5 | 0.024 § | ||
| Cardiovascular symptoms: | Musculoskeletal symptoms: | ||||||||
| Palpitations, % | 64.8 | 45.9 | 0.059 § | Myalgia, % | 71.8 | 32.4 | <0.001 § | ||
| Chest pain, % | 42.3 | 21.6 | 0.033 § | Arthralgia, % | 57.7 | 29.7 | 0.006 § | ||
| Muscle weakness, % | 8.5 | 8.1 | 1.000 ++ | ||||||
| With Brain Fog (n = 71) | Without Brain Fog (n = 37) | p-Value | ||||
|---|---|---|---|---|---|---|
| Chalder Fatigue Scale: | ||||||
| CFQ score, (SD) | 26.9 | (4.7) | 20.9 | (5.1) | <0.001 + | |
| Fatigued, % | 97.1 | 90.9 | 0.325 ++ | |||
| Center for Epidemiological Studies Depression Scale: | ||||||
| CESD score, (SD) | 22.2 | (12.6) | 15.0 | (9.8) | 0.013 + | |
| At risk of depression, % | 69.8 | 46.2 | 0.017 § | |||
| Impact of Events Scale—Revised: | ||||||
| IES-R score, (SD) | 32.5 | (21.1) | 20.2 | (15.4) | 0.008 + | |
| PTSD symptoms, % | 47.8 | 28.1 | 0.064 § | |||
| With Brain Fog (n = 71) | Without Brain Fog (n = 37) | p-Value | ||||
|---|---|---|---|---|---|---|
| Cognitive tests: | ||||||
| Simple response time task, ms, (SD) | 422.2 | (226.6) | 345.8 | (152.6) | 0.028 + | |
| Choice reaction time task, ms, (SD) | 693.3 | (364.6) | 572.6 | (208.4) | 0.035 + | |
| Resting physiological parameters: | ||||||
| Heart rate, bpm, (SD) | 68.8 | (10.8) | 71.0 | (11.1) | 0.325 ^ | |
| Systolic blood pressure, mmHg, (SD) | 132.0 | (14.2) | 130.3 | (15.1) | 0.731 + | |
| Diastolic blood pressure, mmHg, (SD) | 79.9 | (7.7) | 82.0 | (10.3) | 0.297 ^ | |
| Parameters from the active stand: | ||||||
| Orthostatic intolerance, % | 70.3 | 74.3 | 0.675 § | |||
| With Brain Fog (n = 71) | Without Brain Fog (n = 37) | p-Value | ||||
|---|---|---|---|---|---|---|
| Normal gait assessment: | ||||||
| Ambulation time, s, (SD) | 5.9 | (1.9) | 4.9 | (1.1) | 0.001 + | |
| Velocity, cm/s, (SD) | 119.2 | (24.0) | 136.2 | (21.6) | <0.001 ^ | |
| Steps, (SD) | 10.3 | (2.1) | 9.1 | (1.8) | 0.003 + | |
| Cadence, steps/min (SD) | 106.7 | (10.6) | 113.0 | (9.4) | 0.003 ^ | |
| Dual-task gait assessment: | ||||||
| Ambulation time, s, (SD) | 7.4 | (3.9) | 5.7 | (1.6) | 0.002 + | |
| Velocity, cm/s, (SD) | 102.8 | (28.0) | 126.4 | (31.9) | <0.001 ^ | |
| Steps, (SD) | 10.9 | (2.5) | 9.6 | (1.9) | 0.006 + | |
| Cadence, steps/min (SD) | 94.7 | (17.5) | 103.9 | (16.3) | 0.019 + | |
| Maximum gait assessment: | ||||||
| Ambulation time, s, (SD) | 4.1 | (1.5) | 3.7 | (1.3) | 0.090 + | |
| Velocity, cm/s, (SD) | 167.3 | (31.9) | 181.9 | (35.5) | 0.034 ^ | |
| Steps, (SD) | 8.5 | (1.9) | 8.0 | (2.1) | 0.155 + | |
| Cadence, steps/min (SD) | 127.7 | (13.0) | 131.9 | (14.8) | 0.155 + | |
| Strength assessments: | ||||||
| Maximum grip strength, kg, (SD) | 27.2 | (11.4) | 34.2 | (10.1) | 0.002 + | |
| Chair stand test, s, (SD) | 14.4 | (7.9) | 14.1 | (11.8) | 0.068 + | |
| 95% Confidence Interval for Exp(B) | ||||
|---|---|---|---|---|
| Variable | OR | Lower | Upper | p-Value |
| Memory impairment | 5.07 | 1.49 | 17.27 | 0.009 |
| CFQ | 1.14 | 1.01 | 1.27 | 0.030 |
| Myalgia | 3.82 | 1.21 | 12.04 | 0.022 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jennings, G.; Monaghan, A.; Xue, F.; Duggan, E.; Romero-Ortuño, R. Comprehensive Clinical Characterisation of Brain Fog in Adults Reporting Long COVID Symptoms. J. Clin. Med. 2022, 11, 3440. https://doi.org/10.3390/jcm11123440
Jennings G, Monaghan A, Xue F, Duggan E, Romero-Ortuño R. Comprehensive Clinical Characterisation of Brain Fog in Adults Reporting Long COVID Symptoms. Journal of Clinical Medicine. 2022; 11(12):3440. https://doi.org/10.3390/jcm11123440
Chicago/Turabian StyleJennings, Glenn, Ann Monaghan, Feng Xue, Eoin Duggan, and Román Romero-Ortuño. 2022. "Comprehensive Clinical Characterisation of Brain Fog in Adults Reporting Long COVID Symptoms" Journal of Clinical Medicine 11, no. 12: 3440. https://doi.org/10.3390/jcm11123440
APA StyleJennings, G., Monaghan, A., Xue, F., Duggan, E., & Romero-Ortuño, R. (2022). Comprehensive Clinical Characterisation of Brain Fog in Adults Reporting Long COVID Symptoms. Journal of Clinical Medicine, 11(12), 3440. https://doi.org/10.3390/jcm11123440