
Association between Occupation and Cervical Disc Degeneration in 1211 Asymptomatic Subjects

 , ,
, ,
Abstract
:1. Introduction
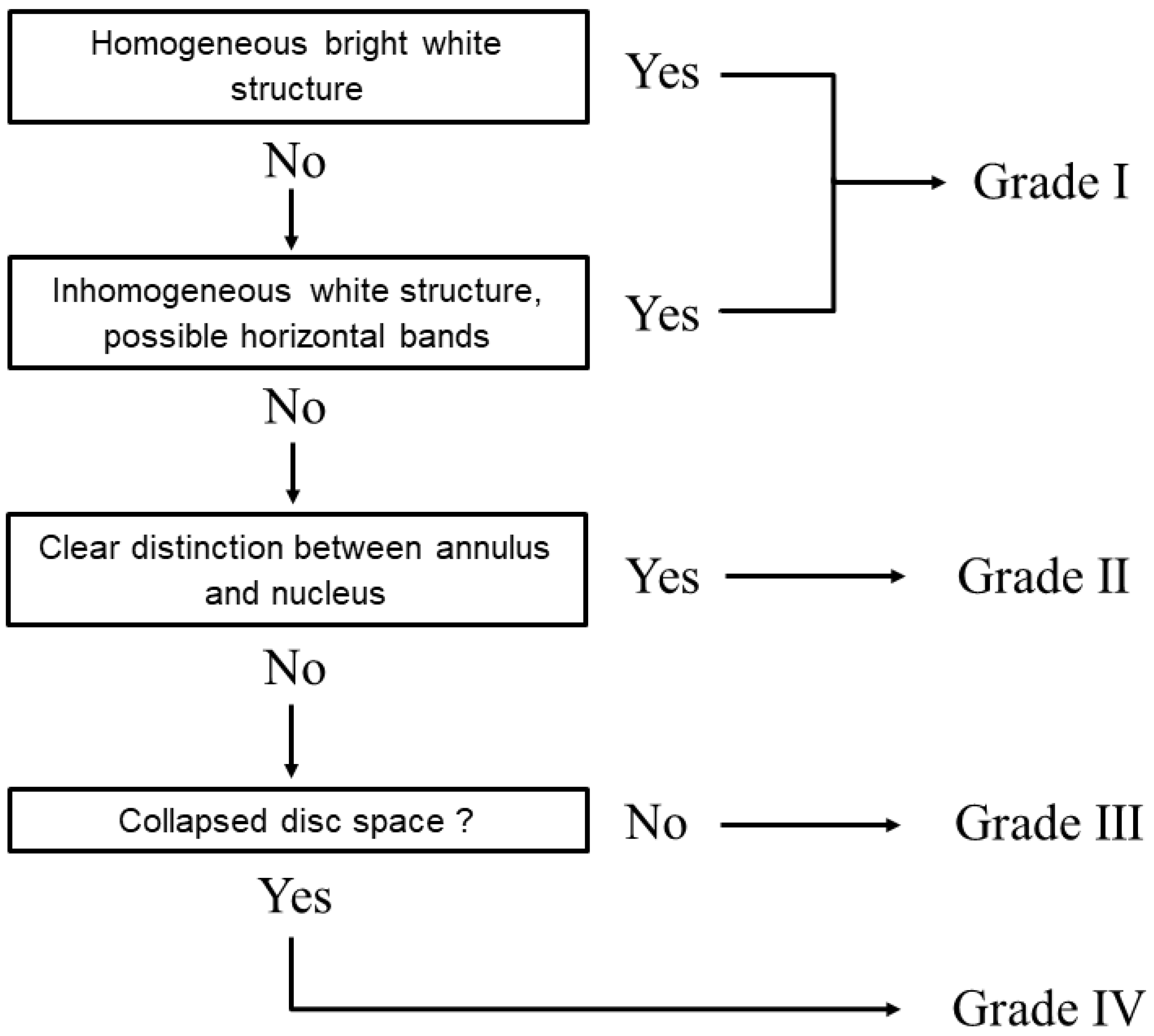
2. Materials and Methods
2.1. Study Population
2.2. Statistical Analysis
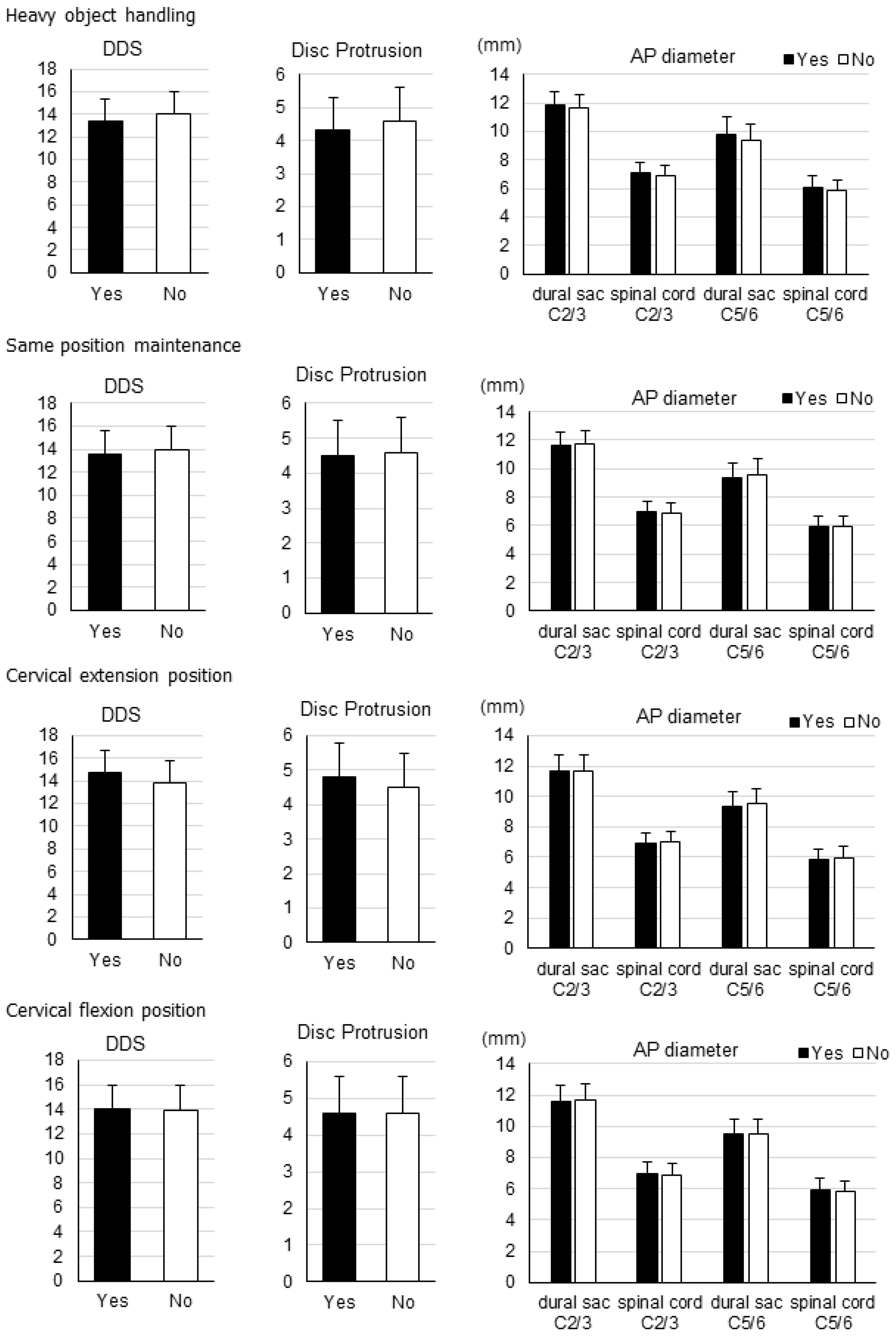
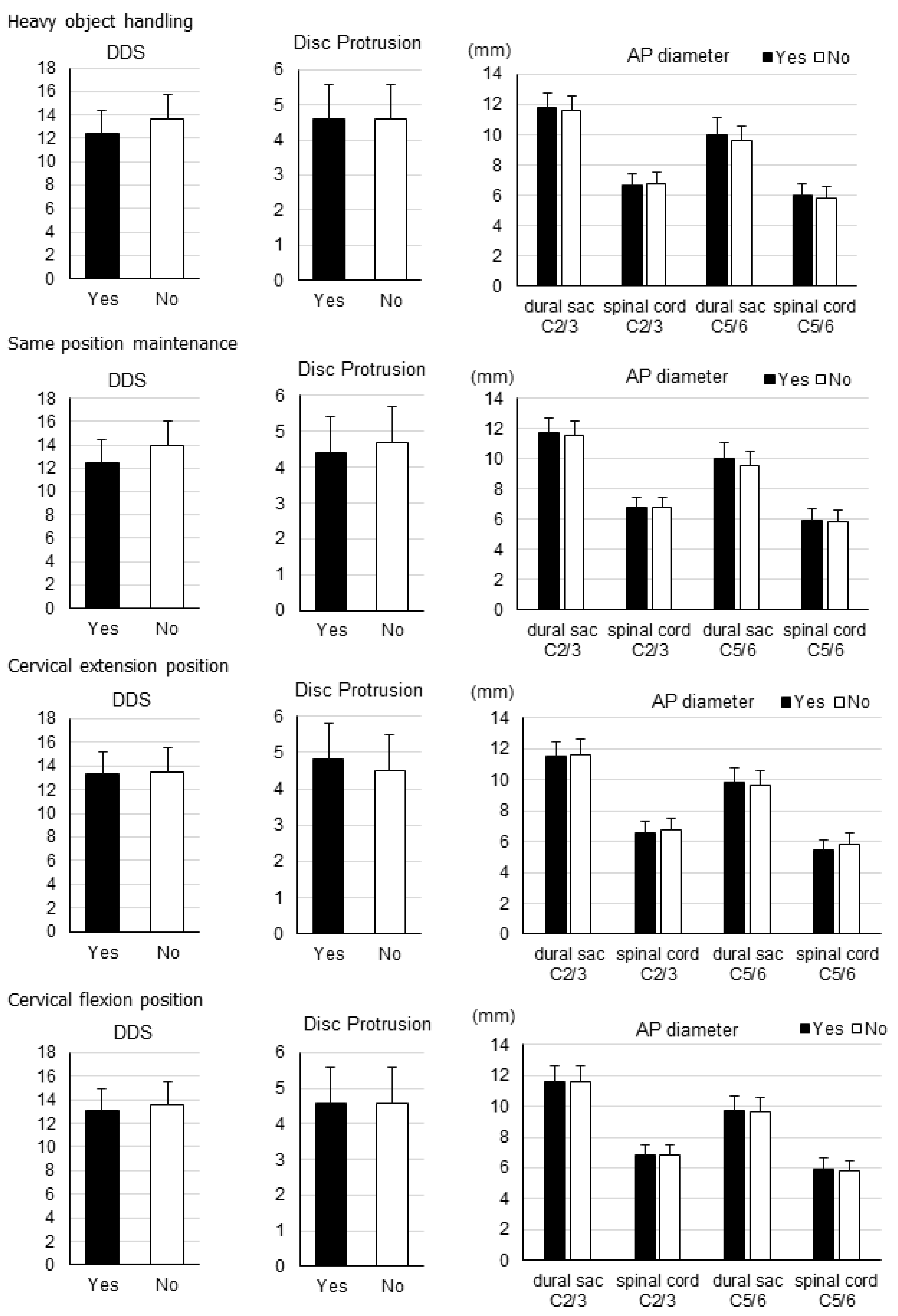
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Boos, N.; Weissbach, S.; Rohrbach, H.; Weiler, C.; Spratt, K.F.; Nerlich, A.G. Classification of age-related changes in lumbar intervertebral discs: 2002 Volvo Award in basic science. Spine 2002, 27, 2631–2644. [Google Scholar] [CrossRef]
- Wilke, H.J.; Rohlmann, F.; Neidlinger-Wilke, C.; Werner, K.; Claes, L.; Kettler, A. Validity and intterobserver agreement of a new radiographic grading system for intervertebral disc degeneration: Part I. Lumbar spine. Eur. Spine J. 2006, 15, 720–730. [Google Scholar] [CrossRef] [Green Version]
- Tertti, M.; Paajanen, H.; Laato, M.; Aho, H.; Komu, M.; Kormano, M. Disc degeneration in magnetic resonance imaging: A comparative biochemical, histologic, and radiologic study in cadaver spines. Spine 1991, 16, 629–634. [Google Scholar] [CrossRef]
- Pfirrmann, C.W.; Metzdorf, A.; Zanetti, M.; Hodler, J.; Boos, N. Magnetic resonance classifi cation of lumbar intervertebral disc degeneration. Spine 2001, 26, 1873–1878. [Google Scholar] [CrossRef]
- Boden, S.D.; McCowin, P.R.; Davis, O.D.; Dina, T.S.; Mark, A.S.; Wiesel, S. Abnormal magnetic-resonance scans of the cervical spine in asymptomatic subjects. A prospective investigation. J. Bone Jt. Surg. 1990, 72, 1178–1184. [Google Scholar] [CrossRef]
- Matsumoto, M.; Fujimura, Y.; Suzuki, N.; Nishi, Y.; Nakamura, M.; Yabe, Y.; Shiga, H. MRI of cervical intervertebral discs in asymptomatic subjects. J. Bone Jt. Surg. Br. 1998, 80, 19–24. [Google Scholar] [CrossRef]
- Okada, E.; Matsumoto, M.; Ichihara, D.; Chiba, K.; Toyama, Y.; Fujiwara, H.; Momoshima, S.; Nishiwaki, Y.; Hashimoto, T.; Ogawa, J.; et al. Aging of the cervical spine in healthy volunteers: A 10-year longitudinal magnetic resonance imaging study. Spine 2009, 34, 706–712. [Google Scholar] [CrossRef]
- Machino, M.; Yukawa, Y.; Imagama, S.; Ito, K.; Katayama, Y.; Matsumoto, T.; Inoue, T.; Ouchida, J.; Tomita, K.; Ishiguro, N.; et al. Age-related and degenerative changes in the osseous anatomy, alignment, and range of motion of the cervical spine: A comparative study of radiographic data from 1016 patients with cervical spondylotic myelopathy and 1230 asymptomatic subjects. Spine 2016, 41, 476–482. [Google Scholar] [CrossRef]
- Roughley, P.J. Biology of intervertebral disc aging and degeneration: Involvement of the extracellular matrix. Spine 2004, 29, 2691–2699. [Google Scholar] [CrossRef]
- Adams, M.A.; Roughley, P.J. What is intervertebral disc degeneration, and what causes it? Spine 2006, 31, 2151–2161. [Google Scholar] [CrossRef] [Green Version]
- Hadjipavlou, A.G.; Tzermiadianos, M.N.; Bogduk, N.; Zindrick, M.R. The pathophysiology of disc degeneration: A critical review. J. Bone Jt. Surg. Br. 2008, 90, 1261–1270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, F.; Sambrook, P. Neck and back pain and intervertebral disc degeneration: Role of occupational factors. Best Pr. Res. Clin. Rheumatol. 2011, 25, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Teraguchi, M.; Yoshimura, N.; Hashizume, H.; Muraki, S.; Yamada, H.; Minamide, A.; Oka, H.; Ishimoto, Y.; Nagata, K.; Kagotani, R.; et al. Prevalence and distribution of intervertebral disc degeneration over the entire spine in a population-based cohort: The Wakayama Spine Study. Osteoarthr. Cartil. 2014, 22, 104–110. [Google Scholar] [CrossRef] [Green Version]
- Machino, M.; Ando, K.; Kobayashi, K.; Nakashima, H.; Ito, S.; Morozumi, M.; Kanbara, S.; Segi, N.; Tomita, H.; Koshimizu, H.; et al. Associations between Neck and Shoulder Pain and Neuropathic Pain in a middle-aged Community-Living Population. Spine 2022, 47, 632–639. [Google Scholar] [CrossRef]
- Cheung, K.M.C.; Karppinen, J.; Chan, D.; Ho, D.W.H.; Song, Y.-Q.; Sham, P.; Cheah, K.S.E.; Leong, J.C.Y.; Luk, K.D.K. Prevalence and Pattern of Lumbar Magnetic Resonance Imaging Changes in a Population Study of One Thousand Forty-Three Individuals. Spine 2009, 34, 934–940. [Google Scholar] [CrossRef]
- Chan, D.; Song, Y.; Sham, P.; Cheung, K.M.C. Genetics of disc degeneration. Eur. Spine J. 2006, 15, 317–325. [Google Scholar] [CrossRef] [Green Version]
- Bass, E.C.; Duncan, N.A.; Hariharan, J.S.; Dusick, J.; Bueff, U.H.; Lotz, J.C. Frozen Storage Affects the Compressive Creep Behavior of the Porcine Intervertebral Disc. Spine 1997, 22, 2867–2876. [Google Scholar] [CrossRef]
- Johnstone, B.; Urban, J.P.; Roberts, S.; Menage, J. The fluid content of the human intervertebral disc: Comparison between fluid content and swelling pressure profiles of discs removed at surgery and those taken postmortem. Spine 1992, 17, 412–416. [Google Scholar] [CrossRef]
- Aihara, T.; Takahashi, K.; Ogasawara, A.; Itadera, E.; Ono, Y.; Moriya, H. Intervertebral disc degeneration associated with lumbosacral transitional vertebrae: A clinical and anatomical study. J. Bone Jt. Surg. Br. 2005, 87-B, 687–691. [Google Scholar] [CrossRef]
- Lee, C.K. Accelerated Degeneration of the Segment Adjacent to a Lumbar Fusion. Spine 1988, 13, 375–377. [Google Scholar] [CrossRef]
- Phillips, F.M.; Reuben, J.; Wettzel, F.T. Intervertebral disc degeneration adjacent to a lumbar fusion. J. Bone Jt. Surg. Br. 2002, 84-B, 289–294. [Google Scholar] [CrossRef]
- Iatridis, J.C.; MacLean, J.J.; Roughley, P.J.; Alini, M. Effects of mechanical loading on intervertebral disc metabolism in vivo. J. Bone Jt. Surg. Am. 2006, 88, 41–46. [Google Scholar]
- Jensen, M.V.; Tüchsen, F.; Ørhede, E. Prolapsed Cervical Intervertebral Disc in Male Professional Drivers in Denmark, 1981–1990. Spine 1996, 21, 2352–2355. [Google Scholar] [CrossRef] [PubMed]
- Petersen, J.A.; Brauer, C.; Thygesen, L.C.; Flachs, E.M.; Lund, C.B.; Thomsen, J.F. Prospective, population-based study of occupational movements and postures of the neck as risk factors for cervical disc herniation. BMJ Open 2022, 12, e053999. [Google Scholar] [CrossRef] [PubMed]
- Battié, M.; Videman, T.; Gibbons, E.L.; Fisher, L.D.; Manninen, H.; Gill, K. Volvo Award in clinical sciences. Determinants of lumbar disc degeneration. A study relating lifetime exposures and magnetic resonance imaging findings in identical twins. Spine 1995, 20, 2601–2612. [Google Scholar] [CrossRef]
- Lötters, F.; Burdorf, A.; Kuiper, J.; Miedema, H. Model for the work-relatedness of low-back pain. Scand. J. Work. Environ. Health 2003, 29, 431–440. [Google Scholar] [CrossRef] [Green Version]
- Williams, F.M.K.; Spector, T.D.; MacGregor, A. Pain reporting at different body sites is explained by a single underlying genetic factor. Rheumatology 2010, 49, 1753–1755. [Google Scholar] [CrossRef] [Green Version]
- Nell, C.; Bülow, R.; Hosten, N.; Schmidt, C.O.; Hegenscheid, K. Reference values for the cervical spinal ca-nal and the vertebral bodies by MRI in a general population. PLoS ONE 2019, 14, e0222682. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Decade | Males | Females | |
|---|---|---|---|
| 20s | Number | 101 | 100 |
| Age (years) | 25.5 ± 2.6 | 25.5 ± 2.6 | |
| Body height (cm) | 172.4 ± 5.8 | 158.5 ± 5.5 | |
| Body weight (kg) | 65.6 ± 8.8 | 51.5 ± 6.0 | |
| BMI (kg/m2) | 22.1 ± 2.7 | 20.5 ± 2.3 | |
| 30s | Number | 104 | 99 |
| Age (years) | 34.7 ± 2.7 | 34.8 ± 3.0 | |
| Body height (cm) | 172.5 ± 6.2 | 158.4 ± 6.0 | |
| Body weight (kg) | 70.3 ± 12.6 | 54.2 ± 8.1 | |
| BMI (kg/m2) | 23.6 ± 3.7 | 21.6 ± 3.1 | |
| 40s | Number | 100 | 100 |
| Age (years) | 44.2 ± 3.0 | 44.2 ± 2.6 | |
| Body height (cm) | 171.0 ± 5.8 | 156.8 ± 5.2 | |
| Body weight (kg) | 69.4 ± 10.9 | 53.8 ± 8.4 | |
| BMI (kg/m2) | 23.7 ± 3.2 | 21.9 ± 3.3 | |
| 50s | Number | 99 | 103 |
| Age (years) | 54.7 ± 2.6 | 54.6 ± 2.8 | |
| Body height (cm) | 168.6 ± 5.7 | 156.6 ± 5.8 | |
| Body weight (kg) | 67.6 ± 9.3 | 54.2 ± 8.1 | |
| BMI (kg/m2) | 23.8 ± 2.9 | 21.9 ± 3.7 | |
| 60s | Number | 101 | 103 |
| Age (years) | 64.4 ± 2.6 | 64.4 ± 3.0 | |
| Body height (cm) | 165.5 ± 5.9 | 153.2 ± 6.0 | |
| Body weight (kg) | 64.0 ± 9.2 | 53.6 ± 7.8 | |
| BMI (kg/m2) | 23.3 ± 3.0 | 22.8 ± 2.8 | |
| 70s | Number | 101 | 100 |
| Age (years) | 73.8 ± 2.6 | 73.1 ± 2.6 | |
| Body height (cm) | 162.4 ± 5.3 | 150.3 ± 5.2 | |
| Body weight (kg) | 61.5 ± 7.9 | 51.6 ± 7.7 | |
| BMI (kg/m2) | 23.3 ± 2.6 | 22.8 ± 3.0 | |
| Total | Number | 606 | 605 |
| Age (years) | 49.5 ± 16.9 | 49.6 ± 16.7 | |
| Body height (cm) | 168.7 ± 6.9 | 155.6 ± 6.3 | |
| Body weight (kg) | 66.4 ± 10.3 | 53.1 ± 7.8 | |
| BMI (kg/m2) | 23.3 ± 3.1 | 21.9 ± 3.2 |
| Occupation | Number | Age (Years) |
|---|---|---|
| Office worker | 196 | 42.2 ± 13.3 |
| Doctor, nurse, and medical coworker | 196 | 37.7 ± 11.6 |
| Housekeeper | 193 | 60.9 ± 13.4 |
| Service provider | 101 | 50.7 ± 13.6 |
| Builder | 78 | 46.9 ± 14.3 |
| Teacher | 58 | 39.4 ± 13.8 |
| Salesperson | 57 | 42.6 ± 13.5 |
| Manufacturer | 54 | 56.6 ± 16.2 |
| Student | 16 | 22.8 ± 2.8 |
| Carrier | 15 | 53.4 ± 13.2 |
| Farmer | 3 | 71.3 ± 4.2 |
| Unemployed person | 124 | 50.2 ± 15.2 |
| Other, Unknown | 120 | 70.2 ± 6.2 |
| Total | 1211 | 49.5 ± 16.8 |
| Heavy Object Handling | ||||
| Males | Females | |||
| Yes | No | Yes | No | |
| Number | 116 | 428 | 84 | 420 |
| Age (years) | 46.3 ± 15.7 | 49.5 ± 16.9 | 42.8 ± 13.0 | 49.5 ± 16.0 |
| Same Position Maintenance | ||||
| Males | Females | |||
| Yes | No | Yes | No | |
| Number | 187 | 354 | 179 | 327 |
| Age (years) | 48.1 ± 14.4 | 50.0 ± 17.4 | 43.3 ± 13.0 | 51.8 ± 17.0 |
| Cervical Extension Position | ||||
| Males | Females | |||
| Yes | No | Yes | No | |
| Number | 33 | 498 | 13 | 480 |
| Age (years) | 51.9 ± 16.7 | 48.3 ± 16.8 | 45.4 ± 14.0 | 48.3 ± 16.0 |
| Cervical Flexion Position | ||||
| Males | Females | |||
| Yes | No | Yes | No | |
| Number | 142 | 395 | 145 | 362 |
| Age (years) | 49.8 ± 17.0 | 48.6 ± 16.0 | 45.4 ± 14.0 | 49.5 ± 17.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Machino, M.; Nakashima, H.; Ito, K.; Ando, K.; Ito, S.; Kato, F.; Imagama, S. Association between Occupation and Cervical Disc Degeneration in 1211 Asymptomatic Subjects. J. Clin. Med. 2022, 11, 3301. https://doi.org/10.3390/jcm11123301
Machino M, Nakashima H, Ito K, Ando K, Ito S, Kato F, Imagama S. Association between Occupation and Cervical Disc Degeneration in 1211 Asymptomatic Subjects. Journal of Clinical Medicine. 2022; 11(12):3301. https://doi.org/10.3390/jcm11123301
Chicago/Turabian StyleMachino, Masaaki, Hiroaki Nakashima, Keigo Ito, Kei Ando, Sadayuki Ito, Fumihiko Kato, and Shiro Imagama. 2022. "Association between Occupation and Cervical Disc Degeneration in 1211 Asymptomatic Subjects" Journal of Clinical Medicine 11, no. 12: 3301. https://doi.org/10.3390/jcm11123301
APA StyleMachino, M., Nakashima, H., Ito, K., Ando, K., Ito, S., Kato, F., & Imagama, S. (2022). Association between Occupation and Cervical Disc Degeneration in 1211 Asymptomatic Subjects. Journal of Clinical Medicine, 11(12), 3301. https://doi.org/10.3390/jcm11123301