
Oral and Dental Considerations of Combat-Induced Post Traumatic Stress Disorder (PTSD)—A Cross-Sectional Study

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Patients Examination
2.3. Extraoral Examination
- (a)
- The pain was localized around the temporomandibular joint (TMJ), temporalis, or masseter muscles.
- (b)
- The patient reported pain in the TMJ, aggravated by palpation of the lateral pole or around it when the mouth was closed.
- (c)
2.4. Intraoral Examination
- Probing depth (PD), measured using a 15-UNC probe and recorded to the nearest 1 mm (PCP- UNC 15; Hu- Friedy, Chicago, IL, USA) at 6 points around all teeth.
- Plaque index (PI) assessed the amount of visible dental plaque [22].
- The DMFt (decayed-D, missing-M, and filled-F teeth) score (ranging from 0–28) assesses the prevalence and treatment needs of dental caries [23]. The score is the sum of carious, absent, and obturated teeth. The third molars were not considered in the count.
- Intraoral hard and soft tissue pathologies.
- Occlusal tooth wear is classified into three categories: 0: no wear; 1: wear confined to the enamel; and 2: severe—wear with exposed dentin [24].
- Number of dental implants.
2.5. Periodontal Diagnosis
2.6. Statistical Analysis
3. Results
4. Discussion
Limitations and Strengths
5. Conclusions
- PTSD patients have high dental and oral pathologies, especially those treated with psychiatric medications.
- Our findings suggest that all patients with PTSD should undergo complete periodontal, oral, and dental examinations periodically and comprehensive education and training regarding proper oral hygiene.
- The use of night guards is frequently indicated in Ci-PTSD.
- The recognition of the particular needs of these patients concerning oral, periodontal, facial, and TMJ health can prevent dental complications and improve quality of life.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brancu, M.; Thompson, N.; Beckham, J.; Green, K.; Calhoun, P.; Elbogen, E.; Robbins, A.; Fairbank, J.; VA Mid-Atlantic MIRECC Registry Workgroup; Wagner, H.R. The impact of social support on psychological distress for U.S. Afghanistan/Iraq era veterans with PTSD and other psychiatric diagnoses. Psychiatry Res. 2014, 217, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Frye, J.S.; Stockton, R.A. Discriminant analysis of post-traumatic stress disorder among a group of Viet Nam veterans. Am. J. Psychiatry 1982, 139, 52–56. [Google Scholar] [PubMed]
- Foy, D.W.; Card, J. Combat-related post-traumatic stress disorder etiology: Replicated findings in a national sample of Vietnam-era men. J. Clin. Psychol. 1987, 43, 28–31. [Google Scholar] [CrossRef]
- Schry, A.R.; Rissling, M.B.; Gentes, E.L.; Beckham, J.C.; Kudler, H.S.; Straits-Tröster, K.; Calhoun, P.S. The Relationship Between Posttraumatic Stress Symptoms and Physical Health in a Survey of U.S. Veterans of the Iraq and Afghanistan Era. Psychosomatics 2015, 56, 674–684. [Google Scholar] [CrossRef]
- Solomon, Z.; Shklar, R.; Singer, Y.; Mikulincer, M. Reactions to combat stress in Israeli veterans twenty years after the 1982 Lebanon war. J. Nerv. Ment. Dis. 2009, 194, 935–939. [Google Scholar] [CrossRef]
- Shlosberg, A.; Strous, R.D. Long-term follow-up (32 Years) of PTSD in Israeli Yom Kippur War veteran. J. Nerv. Ment. Dis. 2005, 193, 693–696. [Google Scholar] [CrossRef]
- El-Gabalawy, R.; Blaney, C.; Tsai, J.; Sumner, J.A.; Pietrzak, R.H. Physical health conditions associated with full and subthreshold PTSD in U.S. military veterans: Results from the National Health and Resilience in Veterans Study. J. Affect. Disord. 2018, 227, 849–853. [Google Scholar] [CrossRef]
- Friedlander, A.H.; Mills, M.J.; Wittlin, B.J. Dental management considerations for the patient with post-traumatic stress disorder. Oral Surg. Oral Med. Oral Pathol. 1987, 63, 669–673. [Google Scholar] [CrossRef]
- Uhac, I.; Kovac, Z.; Muhvić-Urek, M.; Kovacević, D.; Francisković, T.; Simunović-Soskić, M. The prevalence of temporomandibular disorders in war veterans with post-traumatic stress disorder. Mil. Med. 2006, 171, 1147–1149. [Google Scholar] [CrossRef][Green Version]
- Tagger-Green, N.; Nemcovsky, C.; Gadoth, N.; Cohen, O.; Kolerman, R. Oral and dental considerations of combat-induced PTSD: A descriptive study. Quintessence Int. 2020, 51, 678–685. [Google Scholar]
- Wright, E.F.; Thompson, R.L.; Paunovich, E.D. Post-traumatic stress disorder: Considerations for dentistry. Quintessence Int. 2004, 35, 206–210. [Google Scholar] [PubMed]
- Wetselaar, P.; Manfredini, D.; Ahlberg, J.; Johansson, A.; Aarab, G.; Papagianni, C.E.; Reyes Sevilla, M.; Koutris, M.; Lobbezoo, F. Associations between tooth wear and dental sleep disorders: A narrative overview. J. Oral Rehabil. 2019, 46, 765–775. [Google Scholar] [CrossRef] [PubMed]
- Holtfreter, B.; Stubbe, B.; Gläser, S.; Trabandt, J.; Völzke, H.; Ewert, R.; Kocher, T.; Ittermann, T.; Schäper, C. Periodontitis Is Related to Exercise Capacity: Two Cross-sectional Studies. J. Dent. Res. 2021, 100, 824–832. [Google Scholar] [CrossRef]
- Hajishengallis, G. Periodontitis: From microbial immune subversion to systemic inflammation. Nat. Rev. Immunol. 2015, 15, 30–44. [Google Scholar] [CrossRef] [PubMed]
- Berglundh, T.; Giannobile, E.V.; Lang, N.P.; Sanz, M. Lindhe’s Clinical Periodontology and Implant Dentistry, 7th ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2022; p. 752. [Google Scholar]
- De Oliveira Solis, A.C.; Araújo, Á.C.; Corchs, F.; Bernik, M.; Duran, É.P.; Silva, C.; Lotufo-Neto, F. Impact of post-traumatic stress disorder on oral health. J. Affect. Disord. 2017, 219, 126–132. [Google Scholar] [CrossRef] [PubMed]
- Muhvić-Urek, M.; Uhac, I.; Vuksić-Mihaljević, Z.; Leović, D.; Blecić, N.; Kovac, Z. Oral health status in war veterans with post-traumatic stress disorder. J. Oral Rehabil. 2007, 34, 1–8. [Google Scholar] [CrossRef]
- Li, C.; Lu, Z.; Shi, Z.; Zhu, Y.; Wu, Y.; Li, L.; Iheozor-Ejiofor, Z. Periodontal therapy for the management of cardiovascular disease in patients with chronic periodontitis. Cochrane Database Syst. Rev. 2017, 7, 11. [Google Scholar] [CrossRef]
- Lockhart, P.B.; Bolger, A.F.; Papapanou, P.N.; Osinbowale, O.; Trevisan, M.; Levison, M.E.; Taubert, K.A.; Newburger, J.W.; Gornik, H.L.; Gewitz, M.H.; et al. American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee of the Council on Cardiovascular Disease in the Young, Council on Epidemiology and Prevention, Council on Peripheral Vascular Disease, and Council on Clinical Cardiology. Periodontal disease and atherosclerotic vascular disease: Does the evidence support an independent association? A scientific statement from the American Heart Association. Circulation 2012, 125, 2520–2544. [Google Scholar] [PubMed]
- Lobbezoo, F.; Ahlberg, J.; Raphael, K.G.; Wetselaar, P.; Glaros, A.G.; Kato, T.; Santiago, V.; Winocur, E.; De Laat, A.; De Leeuw, R.; et al. International consensus on the assessment of bruxism: Report of a work in progress. J. Oral Rehabil. 2018, 45, 837–844. [Google Scholar] [CrossRef] [PubMed]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: Recommendations of the International RDC/TMD Consortium Network and Orofacial Pain Special Interest Group. J. Oral Facial Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef]
- O’Leary, T.J.; Drake, R.B.; Naylor, J.E. The plaque control record. J. Periodontol. 1972, 43, 38. [Google Scholar] [CrossRef]
- Klein, H. The family and dental disease; dental disease (DMF) experience in parents and offspring. J. Am. Dent. Assoc. 1946, 33, 1136–1141. [Google Scholar] [CrossRef] [PubMed]
- Wetselaar, P.; Lobbezoo, F. The tooth wear evaluation system: A modular clinical guideline for the diagnosis and management planning of worn dentitions. Review J. Oral Rehabil. 2016, 43, 69–80. [Google Scholar] [CrossRef] [PubMed]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.C.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A new classification scheme for periodontal and peri-implant diseases and conditions—Introduction and key changes from the 1999 classification. J. Periodontol. 2018, 8, S1–S8. [Google Scholar]
- Tonetti, M.S.; Jepsen, S.; Jin, L.; Otomo-Corgel, J. Impact of the global burden of periodontal diseases on health, nutrition and wellbeing of mankind: A call for global action. J. Clin. Periodontol. 2017, 44, 456–462. [Google Scholar] [CrossRef] [PubMed]
- Eke, P.I.; Wei, L.; Thornton-Evans, G.O.; Borrell, L.N.; Borgnakke, W.S.; Dye, B.; Genco, R.J. Risk Indicators for Periodontitis in USA adults: NHANES 2009 to 2012. J. Periodontol. 2016, 87, 1174–1185. [Google Scholar] [CrossRef]
- Zhan, Y.; Holtfreter, B.; Meisel, P.; Hoffmann, T.; Micheelis, W.; Dietrich, T.; Kocher, T. Prediction of periodontal disease: Modelling and validation in different general German populations. J. Clin. Periodontol. 2014, 41, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Genco, R.J.; Borgnakke, W.S. Risk factors for periodontal disease. Periodontol. 2000 2013, 62, 59–94. [Google Scholar] [CrossRef] [PubMed]
- Grossi, S.G.; Genco, R.J.; Machtei, E.E.; Ho, A.W.; Koch, G.; Dunford, R.; Zambon, J.J.; Hausmann, E. Assessment of risk for periodontal disease. II. Risk indicators for alveolar bone loss. J. Periodontol. 1995, 66, 23–29. [Google Scholar] [CrossRef]
- Muhvić-Urek, M.; Vukšić, Ž.; Simonić-Kocijan, S.; Braut, V.; Braut, A.; Uhač, I. Co-occurence of chronic head face and neck pain, and depression in war veterans with PTSD. Acta Clin. Croat. 2015, 54, 266–271. [Google Scholar]
- Winocur, E.; Hermesh, H.; Littner, D.; Shiloh, R.; Peleg, L.; Eli, I. Signs of bruxism and temporomandibular disorders among psychiatric patients. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2007, 103, 60–63. [Google Scholar] [CrossRef]
- Tsiggos, N.; Tortopidis, D.; Hatzikyriakos, A.; Menexes, G. Association between self-reported bruxism activity and occurrence of dental attrition, abfraction, and occlusal pits on natural teeth. J. Prosthet. Dent. 2008, 100, 41–46. [Google Scholar] [CrossRef]
- Murali, R.V.; Rangarajan, P.; Mounissamy, A. Bruxism: Conceptual discussion and review. J. Pharm. Bioallied Sci. 2015, 7, S265–S270. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.B.; Kumar, S.K. Myofascial pain secondary to medication-induced bruxism. J. Am. Dent. Assoc. 2012, 143, 67–69. [Google Scholar] [CrossRef]
- Rajan, R.; Sun, Y.M. Reevaluating Antidepressant Selection in Patients with Bruxism and Temporomandibular Joint Disorder. J. Psychiatr. Pract. 2017, 23, 173–179. [Google Scholar] [CrossRef]
- Yoshizawa, S.; Suganuma, T.; Takaba, M.; Ono, Y.; Sakai, T.; Yoshizawa, A.; Kawana, F.; Kato, T.; Baba, K. Phasic jaw motor episodes in healthy subjects with or without clinical signs and symptoms of sleep bruxism: A pilot study. Sleep Breath. 2014, 18, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Van’t Spijker, A.; Rodriguez, J.M.; Kreulen, C.M.; Bronkhorst, E.M.; Bartlett, D.W.; Creugers, N.H. Prevalence of tooth wear in adults. Int. J. Prosthodont. 2009, 22, 35–42. [Google Scholar]
- Schierz, O.; Dommel, S.; Hirsch, C.; Reissmann, D.R. Occlusal tooth wear in the general population of Germany: Effects of age, sex, and location of teeth. J. Prosthet. Dent. 2014, 112, 465–471. [Google Scholar] [CrossRef]
- Arrica, M.; Carta, G.; Cocco, F.; Cagetti, M.G.; Campus, G.; Ierardo, G.; Ottolenghi, L.; Sale, S.; Strohmenger, L. Does a social/behavioural gradient in dental health exist among adults? A cross-sectional study. J. Int. Med. Res. 2017, 45, 451–461. [Google Scholar] [CrossRef]
- Turner, M. Hyposalivation and Xerostomia: Etiology, Complications, and Medical Management. Dent. Clin. N. Am. 2016, 60, 435–443. [Google Scholar] [CrossRef]
- O’Sullivan, E.M. Dental health of Irish alcohol/drug abuse treatment centre residents. Community Dent. Health. 2012, 29, 263–267. [Google Scholar] [PubMed]
- Walsh, K.; Elliott, J.C.; Shmulewitz, D.; Aharonovich, E.; Strous, R.; Frisch, A.; Weizman, A.; Spivak, B.; Grant, B.F.; Hasin, D. Trauma exposure, post-traumatic stress disorder and risk for alcohol, nicotine, and marijuana dependence in Israel. Compr. Psychiatry 2014, 55, 621–630. [Google Scholar] [CrossRef] [PubMed]
- Petrušić, N.; Posavac, M.; Sabol, I.; Mravak-Stipetić, M. The Effect of Tobacco Smoking on Salivation. Acta. Stomatol. Croat. 2015, 49, 309–315. [Google Scholar] [CrossRef]
- Guggenheimer, J.; Moore, P.A. Xerostomia: Etiology, recognition and treatment. J. Am. Dent. Assoc. 2003, 134, 61–69. [Google Scholar] [CrossRef]
- Eveson, J.W. Xerostomia. Periodontol. 2000 2008, 48, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Cappetta, K.; Beyer, C.; Johnson, J.A.; Bloch, M.H. Meta-analysis: Risk of dry mouth with second generation antidepressants. Prog. Neuropsychopharmacol. Biol. Psychiatry 2018, 84, 282–293. [Google Scholar] [CrossRef]
- Costa, S.M.; Martins, C.C.; Pinto, M.Q.C.; Vasconcelos, M.; Abreu, M.H.N.G. Socioeconomic Factors and Caries in People between 19 and 60 Years of Age: An Update of a Systematic Review and Meta-Analysis of Observational Studies. Int. J. Environ. Res. Public Health 2018, 18, 1775. [Google Scholar] [CrossRef]
- Hamid, S.H.; Dashash, M.A.D. The impact of post-traumatic stress disorder on dental and gingival status of children during Syrian crisis: A preliminary study. J. Investig. Clin. Dent. 2019, 10, e12372. [Google Scholar] [CrossRef]
- Zusman, S.P.; Ponizovsky, A.M.; Dekel, D.; Masarwa, A.E.; Ramon, T.; Natapov, L.; Grinshpoon, A. An assessment of the dental health of chronic institutionalized patients with psychiatric disease in Israel. Spec. Care Dent. 2010, 30, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Skodol, A.E.; Schwartz, S.; Dohrenwend, B.P.; Levav, I.; Shrout, P.A.; Reiff, M. PTSD Symptoms and Comorbid Mental Disorders in Israeli War Veterans. Br. J. Psychiatry 1996, 169, 717–725. [Google Scholar] [CrossRef] [PubMed]
- Lenk, M.; Berth, H.; Joraschky, P.; Petrowski, K.; Weidner, K.; Hannig, C. Fear of dental treatment—An underrecognized symptom in people with impaired mental health. Dtsch. Ärzteblatt Int. 2013, 31–32, 517–522. [Google Scholar]
- Høyvik, A.C.; Lie, B.; Willumsen, T. Dental anxiety in relation to torture experiences and symptoms of post-traumatic stress disorder. Eur. J. Oral Sci. 2019, 127, 65–71. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| PTSD | PTSD | Control | Significance | ||||
|---|---|---|---|---|---|---|---|
| Total (n = 100) | With Medication (n = 40) | Without Medication (n = 60) | (n = 103) | Overall (ANOVA 3 Groups) | Post-Hoc (Tukey B Test) | ||
| Sex | Male | 97 (97%) | 39 (97.5%) | 58 (97%) | 102 (99%) | ||
| Female | 3 (3%) | 1 (2.5%) | 2 (3%) | 1 (1%) | |||
| Age | 60.55 ± 11.70 | 63.30 ± 10.79 | 56.43 ± 11.92 | 59.93 ± 13.29 | p = 0.024 | Med non- med p < 0.05 | |
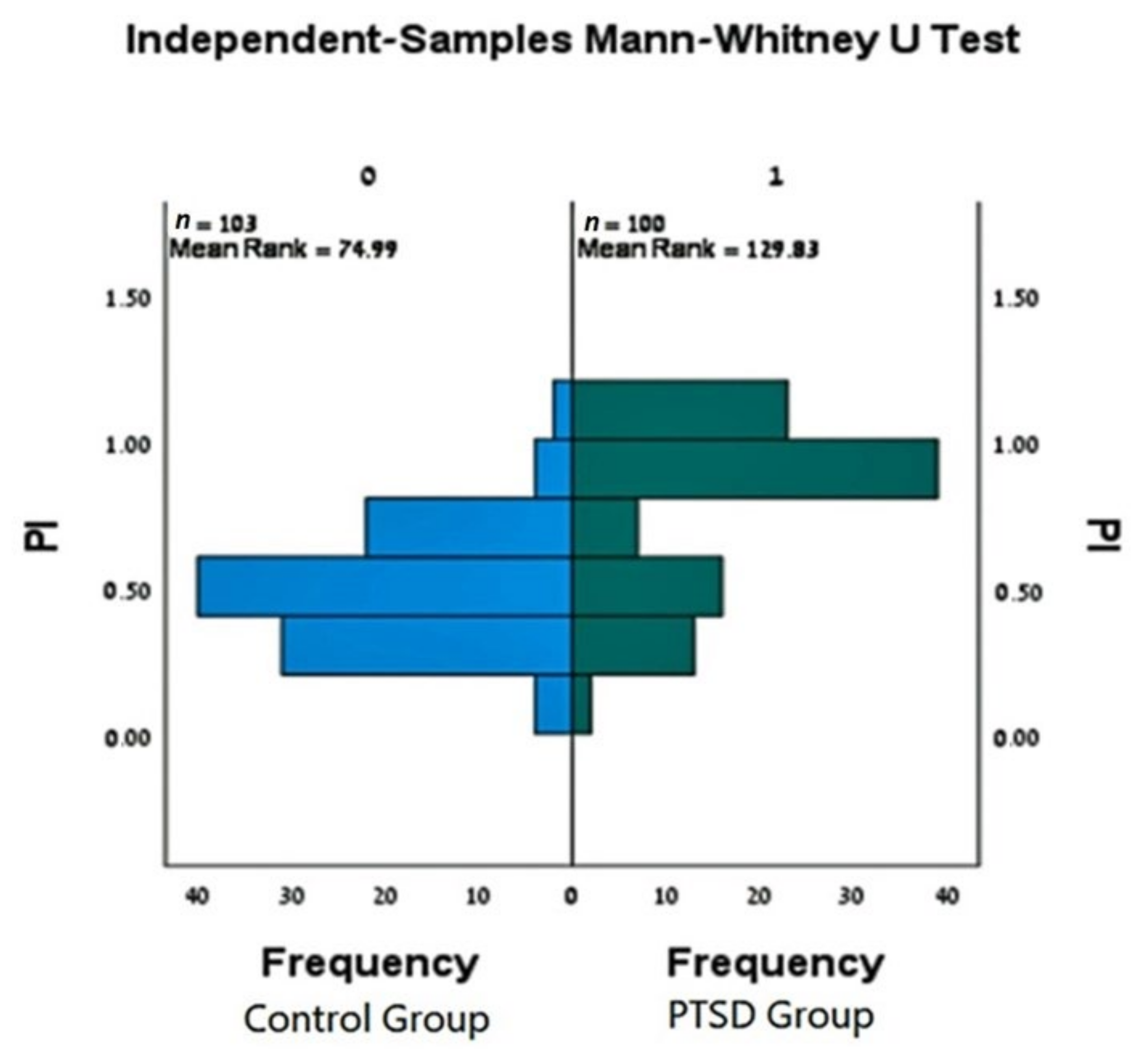
| PI | 0.72 ± 0.28 | 0.80 ± 0.24 | 0.67 ± 0.29 | 0.45 ± 0.29 | p < 0.001 (*) | Any two groups of the 3 are different with p < 0.05 | |
| Decayed Missing Filled | 3.47 ± 3.46 | 4.13 ± 4.63 | 3.03 ± 2.33 | 0.58 ± 1.24 | p < 0.001 | - “ - | |
| 5.78 ± 6.95 | 5.60 ± 7.80 | 5.90 ± 6.38 | 3.98 ± 4.89 | p = 0.102 | N/S | ||
| 10.70 ± 5.63 | 9.65 ± 6.60 | 11.4 ± 4.85 | 8.50± 4.76 | p = 0.003 | Control–non- med p < 0.05 | ||
| DMF | 19.97 ± 8.07 | 19.48 ± 9.28 | 20.30 ± 7.22 | 13.05 ± 6.23 | p < 0.001 | Control–PTSD p < 0.05 | |
| Implants | 1.15 ± 2.12 | 1.08 ± 2.011 | 1.25 ± 2.30 | 2.0 ± 3.21 | p = 0.085 | N/S | |
| PTSD | Control | Test #Conditions × #Groups Significance | |||
|---|---|---|---|---|---|
| With Medication | Without Medication | ||||
| Smoking status | Never | 16 (40.0%) | 43 (71.7%) | 71 (68.9%) | Pearson Chi-Square 4 × 3 p < 0.001 |
| Heavy | 22(55.0%) | 13 (21.7%) | 16 (15.5%) | ||
| Light | 0 (0.0%) | 1 (1.7%) | 10 (9.7%) | ||
| Former | 2 (5.0%) | 3 (5%) | 6 (5.8%) | ||
| Periodontal disease status: Severity | Mild- Moderate (Stages I or II) | 15 (37.5%) | 42 (70.0%) | 75 (72.8%) | Pearson Chi-Square 2 × 3 p < 0.001 |
| Severe (Stages III or IV) | 25 (62.5%) | 18 (30.0%) | 28 (27.2%) | ||
| Grading | B | 12 (30.0%) | 25 (41.7%) | 35 (34.0%) | Non-Significant |
| C | 22 (55%) | 21 (35.0%) | 28 (27.2%) | Non-Significant | |
| Local– General | Localized | 12 (30%) | 26 (43.3%) | 53 (51.5%) | Pearson Chi-Square 2 × 3 p = 0.066 |
| Generalized | 28 (70%) | 34 (56.7%) | 50 (48.5) | ||
| Tooth wear (edentulous patients not included) | None | 2 (5.6%) | 3 (5.1%) | 27 (26.5%) | Pearson Chi-Square 3 × 3 p < 0.001 |
| Mild | 8 (22.2%) | 13 (22%) | 42 (41.2%) | ||
| Severe | 26 (72.2%) | 43 (72.9%) | 33 (32.4%) | ||
| Night guard (no edentulous patients) | No | 12 (33.3%) | 34 (57.6%) | 94 (92.2%) | Pearson Chi-Square 2 × 3 p < 0.001 |
| Yes | 24 (66.7%) | 25 (42.4%) | 8 (7.8%) | ||
| TMJ/Facial pain | No | 12 (30.0%) | 31 (51.7%) | 90 (88.2%) | Pearson Chi-Square 2 × 3 p < 0.001 |
| Yes | 28 (70.0%) | 29 (48.3%) | 12 (11.8%) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tagger-Green, N.; Nemcovsky, C.; Fridenberg, N.; Green, O.; Chaushu, L.; Kolerman, R. Oral and Dental Considerations of Combat-Induced Post Traumatic Stress Disorder (PTSD)—A Cross-Sectional Study. J. Clin. Med. 2022, 11, 3249. https://doi.org/10.3390/jcm11113249
Tagger-Green N, Nemcovsky C, Fridenberg N, Green O, Chaushu L, Kolerman R. Oral and Dental Considerations of Combat-Induced Post Traumatic Stress Disorder (PTSD)—A Cross-Sectional Study. Journal of Clinical Medicine. 2022; 11(11):3249. https://doi.org/10.3390/jcm11113249
Chicago/Turabian StyleTagger-Green, Nirit, Carlos Nemcovsky, Naama Fridenberg, Orr Green, Liat Chaushu, and Roni Kolerman. 2022. "Oral and Dental Considerations of Combat-Induced Post Traumatic Stress Disorder (PTSD)—A Cross-Sectional Study" Journal of Clinical Medicine 11, no. 11: 3249. https://doi.org/10.3390/jcm11113249
APA StyleTagger-Green, N., Nemcovsky, C., Fridenberg, N., Green, O., Chaushu, L., & Kolerman, R. (2022). Oral and Dental Considerations of Combat-Induced Post Traumatic Stress Disorder (PTSD)—A Cross-Sectional Study. Journal of Clinical Medicine, 11(11), 3249. https://doi.org/10.3390/jcm11113249