
Endothelial Dysfunction and Arterial Stiffness in Patients with Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Data Extraction and Quality Assessment
2.3. Statistical Analysis and Risk of Bias Assessment
2.4. Sensitivity Analyses
2.5. Subgroup Analyses
2.6. Meta Regression Analyses
3. Results
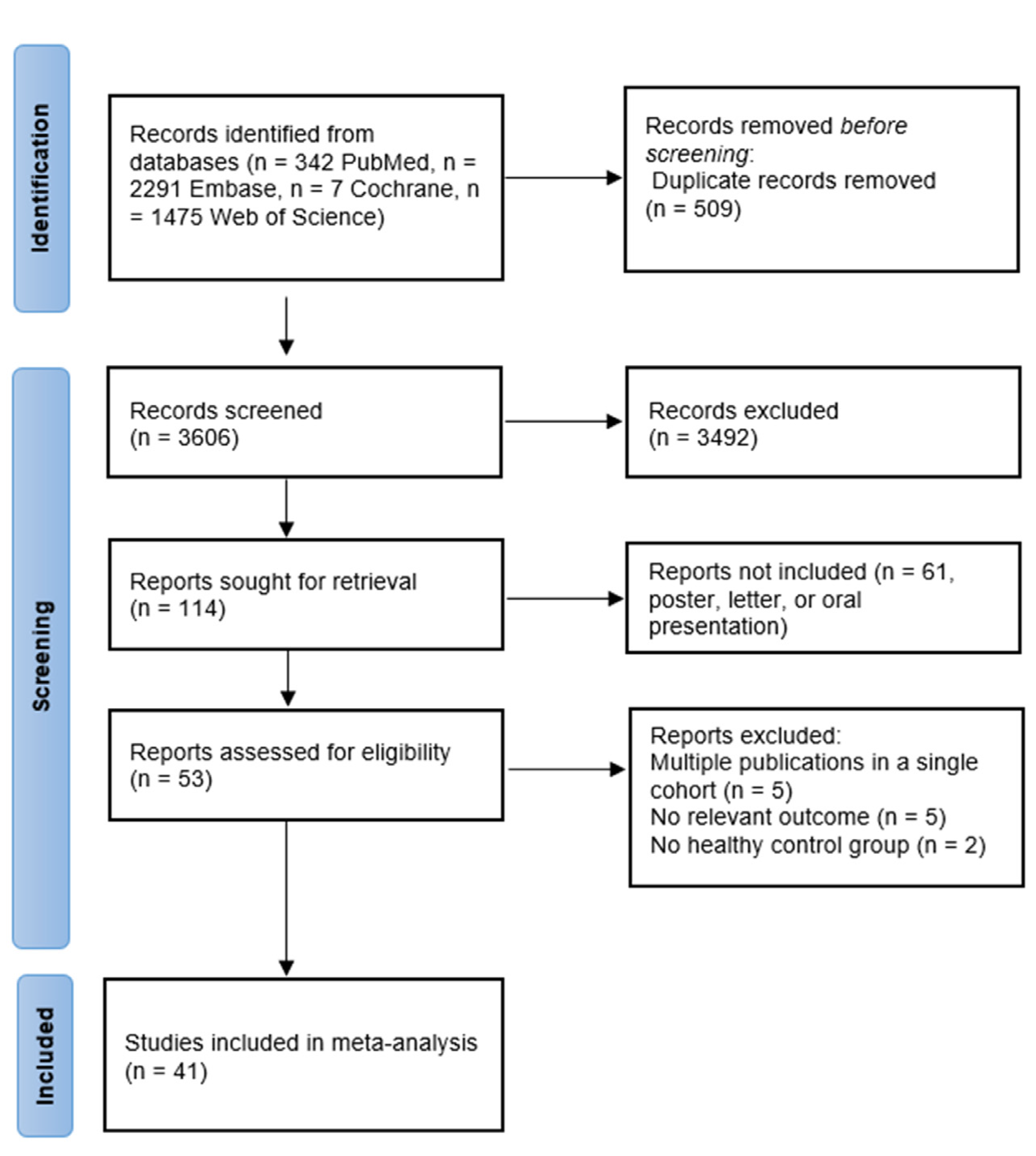
3.1. Descriptions of the Identified Studies
3.2. Study Characteristics
3.3. Carotid Intima-Media Thickness Was Significantly Increased in IBD Patients
3.4. Arterial Stiffness Was Significantly Increased in IBD Patients
3.5. Endothelial Function Was Significantly Impaired in Patients with IBD
3.6. Publication Bias
3.7. Sensitivity Analyses
3.8. Subgroup Analyses
3.9. Meta-Regression Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update From the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- Lerman, A.; Zeiher, A.M. Endothelial function: Cardiac events. Circulation 2005, 111, 363–368. [Google Scholar] [CrossRef] [PubMed]
- Ferrucci, L.; Fabbri, E. Inflammageing: Chronic inflammation in ageing, cardiovascular disease, and frailty. Nat. Rev. Cardiol. 2018, 15, 505–522. [Google Scholar] [CrossRef] [PubMed]
- Mason, J.C.; Libby, P. Cardiovascular disease in patients with chronic inflammation: Mechanisms underlying premature cardi-ovascular events in rheumatologic conditions. Eur. Heart J. 2015, 36, 482c–489c. [Google Scholar]
- Aarestrup, J.; Jess, T.; Kobylecki, C.J.; Nordestgaard, B.G.; Allin, K.H. Cardiovascular Risk Profile Among Patients with Inflammatory Bowel Disease: A Population-based Study of More Than 100.000 Individuals. J. Crohn’s Colitis 2018, 13, 319–323. [Google Scholar] [CrossRef]
- Bernstein, C.N.; Nugent, Z.; Singh, H. Persistently High Rate of Venous Thromboembolic Disease in Inflammatory Bowel Disease: A Population-Based Study. Am. J. Gastroenterol. 2021, 116, 1476–1484. [Google Scholar] [CrossRef]
- Kirchgesner, J.; Beaugerie, L.; Carrat, F.; Andersen, N.N.; Jess, T.; Schwarzinger, M. Increased risk of acute arterial events in young patients and severely active IBD: A nationwide French cohort study. Gut 2017, 67, 1261–1268. [Google Scholar] [CrossRef]
- Choi, Y.J.; Lee, D.H.; Shin, D.W.; Han, K.-D.; Yoon, H.; Shin, C.M.; Park, Y.S.; Kim, N. Patients with inflammatory bowel disease have an increased risk of myocardial infarction: A nationwide study. Aliment. Pharmacol. Ther. 2019, 50, 769–779. [Google Scholar] [CrossRef]
- Schnabel, R.B.; Schulz, A.; Wild, P.S.; Sinning, C.R.; Wilde, S.; Eleftheriadis, M.; Herkenhoff, S.; Zeller, T.; Lubos, E.; Lackner, K.J.; et al. Noninvasive vascular function measurement in the community: Cross-sectional relations and comparison of methods. Circ. Cardiovasc. Imaging 2011, 4, 371–380. [Google Scholar] [CrossRef] [Green Version]
- Hansen, T.; Staessen, J.A.; Torp-Pedersen, C.; Rasmussen, S.; Thijs, L.; Ibsen, H.; Jeppesen, J. Prognostic Value of Aortic Pulse Wave Velocity as Index of Arterial Stiffness in the General Population. Circulation 2006, 113, 664–670. [Google Scholar] [CrossRef]
- Xu, S.; Ilyas, I.; Little, P.J.; Li, H.; Kamato, D.; Zheng, X.; Luo, S.; Li, Z.; Liu, P.; Han, J.; et al. Endothelial Dysfunction in Atherosclerotic Cardiovascular Diseases and Beyond: From Mechanism to Pharmacotherapies. Pharmacol. Rev. 2021, 73, 924–967. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, M.W.; Sitzer, M.; Markus, H.S.; Bots, M.L.; Rosvall, M. Prediction of Clinical Cardiovascular Events With Carotid Intima-Media Thickness: A Systematic Review and Meta-Analysis. Circulation 2007, 116, e318. [Google Scholar] [CrossRef]
- Ozturk, K.; Guler, A.K.; Cakir, M.; Ozen, A.; Demirci, H.; Turker, T.; Demirbas, S.; Uygun, A.; Gulsen, M.; Bagci, S. Pulse Wave Velocity, Intima Media Thickness, and Flow-mediated Dilatation in Patients with Normotensive Normoglycemic Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2015, 21, 1314–1320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Principi, M.; Mastrolonardo, M.; Scicchitano, P.; Gesualdo, M.; Sassara, M.; Guida, P.; Bucci, A.; Zito, A.; Caputo, P.; Albano, F.; et al. Endothelial function and cardiovascular risk in active inflammatory bowel diseases. J. Crohn’s Colitis 2013, 7, e427–e433. [Google Scholar] [CrossRef] [Green Version]
- Zanoli, L.; Rastelli, S.; Granata, A.; Inserra, G.; Empana, J.P.; Boutouyrie, P.; Laurent, S.; Castellino, P. Arterial stiffness in inflammatory bowel disease: A systematic review and meta-analysis. J. Hypertens. 2016, 34, 822–829. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.-C.; Leng, R.-X.; Lu, Q.; Fan, Y.-G.; Wang, D.-G.; Ye, D. Subclinical Atherosclerosis in Patients With Inflammatory Bowel Diseases: A Systematic Review and Meta-Analysis. Angiology 2016, 68, 447–461. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Ottawa Hospital Research Institute. 2011. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 5 February 2022).
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Peters, J.L.; Sutton, A.J.; Jones, D.R.; Abrams, K.; Rushton, L. Performance of the trim and fill method in the presence of publication bias and between-study heterogeneity. Stat. Med. 2007, 26, 4544–4562. [Google Scholar] [CrossRef]
- Deeks, J.J.; Higgins, J.P.; Altman, D.G. Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019; pp. 241–284. [Google Scholar]
- Zanoli, L.; Ozturk, K.; Cappello, M.; Inserra, G.; Geraci, G.; Tuttolomondo, A.; Torres, D.; Pinto, A.; Duminuco, A.; Riguccio, G.; et al. Inflammation and Aortic Pulse Wave Velocity: A Multicenter Longitudinal Study in Patients With Inflammatory Bowel Disease. J. Am. Heart Assoc. 2019, 8, e010942. [Google Scholar] [CrossRef] [Green Version]
- Zanoli, L.; Tuttolomondo, A.; Inserra, G.; Cappello, M.; Granata, A.; Malatino, L.; Castellino, P. Anxiety, depression, chronic inflammation and aortic stiffness in Crohn’s disease: The brain–gut–vascular axis. J. Hypertens. 2020, 38, 2008–2017. [Google Scholar] [CrossRef] [PubMed]
- Fan, F.; Galvin, A.; Fang, L.; White, D.A.; Moore, X.-L.; Sparrow, M.; Cicuttini, F.; Dart, A.M. Comparison of inflammation, arterial stiffness and traditional cardiovascular risk factors between rheumatoid arthritis and inflammatory bowel disease. J. Inflamm. 2014, 11, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kayahan, H.; Sari, I.; Cullu, N.; Yuksel, F.; Demir, S.; Akarsu, M.; Goktay, Y.; Unsal, B.; Akpinar, H. Evaluation of early atherosclerosis in patients with inflam-matory bowel disease. Dig. Dis. Sci. 2012, 57, 2137–2143. [Google Scholar] [CrossRef] [PubMed]
- Kocaman, O.; Sahin, T.; Aygun, C.; Senturk, O.; Hulagu, S. Endothelial dysfunction in patients with ulcerative colitis. Inflamm. Bowel Dis. 2006, 12, 166–171. [Google Scholar] [CrossRef]
- Üstün, Y.; Kilincalp, S.; Çoban, Ş.; Coşkun, Y.; Yüksel, İ.; Ongun, A.; Soykan, İ.; Bektaş, M.; Törüner, M.; Çetinkaya, H.; et al. Evaluation of Early Atherosclerosis Markers in Patients with Inflammatory Bowel Disease. Med. Sci. Monit. 2016, 22, 3943–3950. [Google Scholar] [CrossRef] [Green Version]
- Akdoǧan, R.A.; Durakoǧlugil, M.E.; Kocaman, S.A.; Çiçek, Y.; Durakoǧlugil, T.; Ergül, E.; Rakıcı, H. Increased pulse wave velocity and carotid intima-media thickness in patients with ulcerative colitis. Dig. Dis. Sci. 2013, 58, 2293–2300. [Google Scholar] [CrossRef]
- Alkan, E.; Karakas, M.S.; Yildirim, B. Evaluation of increased subclinical atherosclerosis risk with carotid intima-media thickness and pulse wave velocity in inflamatory bowel disease. Turk. J. Gastroenterol. 2015, 25, 20–25. [Google Scholar] [CrossRef]
- Aloi, M.; Tromba, L.; Di Nardo, G.; Dilillo, A.; Del Giudice, E.; Marocchi, E.; Viola, F.; Civitelli, F.; Berni, A.; Cucchiara, S. Premature Subclinical Atherosclerosis in Pediatric Inflammatory Bowel Disease. J. Pediatr. 2012, 161, 589–594.e1. [Google Scholar] [CrossRef]
- Aloi, M.; Tromba, L.; Rizzo, V.; D’Arcangelo, G.; Dilillo, A.; Blasi, S.; Civitelli, F.; Kiltzanidi, D.; Redler, A.; Viola, F. Aortic Intima-Media Thickness as an Early Marker of Atherosclerosis in Children With Inflammatory Bowel Disease. J. Pediatr. Gastroenterol. Nutr. 2015, 61, 41–46. [Google Scholar] [CrossRef]
- Broide, E.; Schopan, A.; Zaretsky, M.; Kimchi, N.A.; Shapiro, M.; Scapa, E. Intima-Media Thickness of the Common Carotid Artery Is Not Significantly Higher in Crohn’s Disease Patients Compared to Healthy Population. Am. J. Dig. Dis. 2010, 56, 197–202. [Google Scholar] [CrossRef]
- Bruzzese, V.; Palermo, G.; Ridola, L.; Lorenzetti, R.; Hassan, C.; Izzo, A.; Zullo, A. Preclinical atherosclerosis in patients with inflammatory bowel diseases: A case-control study. Ann. Transl. Med. 2017, 5, 158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caliskan, Z.; Keles, N.; Kahraman, R.; Özdil, K.; Karagoz, V.; Aksu, F.; Aciksari, G.; Yilmaz, Y.; Kul, S.; Caliskan, M. Imparied retrobulbar blood flow and increased carotid IMT in patients with Crohn’s disease. Int. J. Cardiovasc. Imaging 2016, 32, 1617–1623. [Google Scholar] [CrossRef] [PubMed]
- Cappello, M.; Licata, A.; Calvaruso, V.; Bravatà, I.; Aiello, A.; Torres, D.; Della Corte, V.; Tuttolomondo, A.; Perticone, M.; Licata, G.; et al. Increased expression of markers of early atherosclerosis in patients with inflammatory bowel disease. Eur. J. Intern. Med. 2017, 37, 83–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dagli, N.; Poyrazoglu, O.K.; Ferda Dagli, A.; Sahbaz, F.; Karaca, I.; Ali Kobat, M.; Bahcecioglu, I.H. Is inflammatory bowel disease a risk factor for early atherosclerosis? Angiology 2010, 61, 198–204. [Google Scholar] [CrossRef]
- Ekmen, N.; Can, G.; Yozgat, A.; Can, H.; Bayraktar, M.F.; Demirkol, M.E.; Kayhan, M.A.; Sasani, H. Evaluation of epicardial adipose tissue and carotid intima-media thickness as a marker of atherosclerosis in patients with inflammatory bowel disease. Rev. Esp. Enferm. Dig. 2020, 113, 643–648. [Google Scholar] [CrossRef]
- Gozel, N.; Eyvaz, A.; Ozel, B.D.; Dogan, Y.; Sarli, B.; Ozturk, A.B.; Poyrazoglu, O.B.; Poyrazoglu, O.K. An imaging method for the evaluation of early atherosclerosis in inflammatory bowel disease: Epicardial adipose tissue. Prog. Nutr. 2019, 21, 836–842. [Google Scholar] [CrossRef]
- Hernández-Camba, A.; Carrillo-Palau, M.; Ramos, L.; Alvarez-Buylla, N.H.; Alonso-Abreu, I.; Hernández-Pérez, A.; Vela, M.; Arranz, L.; Hernández-Guerra, M.; González-Gay, M.; et al. Carotid Plaque Assessment Reclassifies Patients with Inflammatory Bowel Disease into Very-High Cardiovascular Risk. J. Clin. Med. 2021, 10, 1671. [Google Scholar] [CrossRef]
- Jain, S.S.; Shah, D.K.; Gambhire, P.A.; Varma, R.U.; Contractor, Q.Q.; Rathi, P.M. Early atherosclerosis in ulcerative colitis: Cross-sectional case-control study. J. Dig. Dis. 2015, 16, 656–664. [Google Scholar] [CrossRef]
- Kim, K.O.; Jang, B.I.; Lee, S.H. Does carotid intima-media thickness increase in patients with inflammatory bowel disease? Intest. Res. 2014, 12, 293–298. [Google Scholar] [CrossRef]
- Kothari, H.G.; Gupta, S.J.; Gaikwad, N.R. Utility of Carotid Intima-Media Thickness as an Auxiliary Vascular Parameter of Structural Alteration in Ulcerative Colitis. Inflamm. Intest. Dis. 2019, 4, 27–34. [Google Scholar] [CrossRef]
- Maharshak, N.; Arbel, Y.; Bornstein, N.M.; Gal-Oz, A.; Gur, A.Y.; Shapira, I.; Rogowski, O.; Berliner, S.; Halpern, Z.; Dotan, I. Inflammatory Bowel Disease Is Not Associated With Increased Intimal Media Thickening. Am. J. Gastroenterol. 2007, 102, 1050–1055. [Google Scholar] [CrossRef] [PubMed]
- Papa, A.; Santoliquido, A.; Danese, S.; Covino, M.; Di Campli, C.; Urgesi, R.; Grillo, A.; Guglielmo, S.; Tondi, P.; Guidi, L.; et al. Increased carotid intima-media thickness in patients with inflammatory bowel disease. Aliment. Pharmacol. Ther. 2005, 22, 839–846. [Google Scholar] [CrossRef] [PubMed]
- Theocharidou, E.; Gossios, T.D.; Griva, T.; Giouleme, O.; Douma, S.; Athyros, V.G.; Karagiannis, A. Is There an Association Between Inflammatory Bowel Diseases and Carotid Intima-media Thickness? Preliminary Data. Angiology 2013, 65, 543–550. [Google Scholar] [CrossRef] [PubMed]
- Uysal, F.; Akbal, E.; Akbal, A.; Cevizci, S.; Arık, K.; Gazi, E. Epicardial Adipose Tissue Is Increased in Patients With Inflammatory Bowel Disease. J. Ultrasound Med. 2016, 35, 1859–1864. [Google Scholar] [CrossRef] [Green Version]
- van Leuven, S.I.; Hezemans, R.; Levels, J.H.; Snoek, S.; Stokkers, P.C.; Hovingh, G.K.; Kastelein, J.J.; Stroes, E.S.; de Groot, E.; Hommes, D.W. Enhanced atherogenesis and altered high density lipoprotein in patients with Crohn’s disease. J. Lipid Res. 2007, 48, 2640–2646. [Google Scholar] [CrossRef] [Green Version]
- Aytaç, E.; Büyüktaş, D.; Baysal, B.; Atar, M.; Yıldız, M.; Baca, B.; Karahasanoğlu, T.; Çelik, A.; Seymen, H.O.; Hamzaoğlu, İ. Visual evoked potentials and pulse wave velocity in inflam-matory bowel disease. Turk. J. Gastroenterol. 2015, 26, 15–19. [Google Scholar] [CrossRef]
- Korkmaz, H.; Sahin, F.; Ipekci, S.H.; Temel, T.; Kebapcilar, L. Increased pulse wave velocity and relationship with inflammation, insulin, and insulin resistance in inflammatory bowel disease. Eur. J. Gastroenterol. Hepatol. 2014, 26, 725–732. [Google Scholar] [CrossRef]
- Nemes, A.; Gavallér, H.; Nagy, F.; Náfrády, J.; Wittmann, T.; Forster, T. Increased aortic stiffness in ulcerative colitis. Open Med. 2014, 9, 40–44. [Google Scholar] [CrossRef]
- Theocharidou, E.; Tellis, C.C.; Mavroudi, M.; Soufleris, K.; Gossios, T.D.; Giouleme, O.; Athyros, V.G.; Tselepis, A.D.; Karagiannis, A. Lipoprotein-associated phospholipase A2 and arterial stiffness evaluation in patients with inflammatory bowel diseases. J. Crohn’s Colitis 2014, 8, 936–944. [Google Scholar] [CrossRef] [Green Version]
- Zanoli, L.; Cannavo, M.; Rastelli, S.; Di Pino, L.; Monte, I.; Di Gangi, M.; Boutouyrie, P.; Inserra, G.; Laurent, S.; Castellino, P. Arterial stiffness is increased in patients with inflam-matory bowel disease. J. Hypertens. 2012, 30, 1775–1781. [Google Scholar] [CrossRef] [Green Version]
- Zanoli, L.; Lentini, P.; Boutouyrie, P.; Fatuzzo, P.; Granata, A.; Corrao, S.; Gaudio, A.; Inserra, G.; Rapisarda, F.; Rastelli, S.; et al. Pulse wave velocity differs between ulcerative colitis and chronic kidney disease. Eur. J. Intern. Med. 2017, 47, 36–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zanoli, L.; Rastelli, S.; Inserra, G.; Lentini, P.; Valvo, E.; Calcagno, E.; Boutouyrie, P.; Laurent, S.; Castellino, P. Increased arterial stiffness in inflammatory bowel diseases is dependent upon inflammation and reduced by immunomodulatory drugs. Atherosclerosis 2014, 234, 346–351. [Google Scholar] [CrossRef] [PubMed]
- Zivkovic, P.M.; Matetic, A.; Hadjina, I.T.; Rusic, D.; Vilovic, M.; Supe-Domic, D.; Borovac, J.A.; Mudnic, I.; Tonkic, A.; Bozic, J. Serum Catestatin Levels and Arterial Stiffness Parameters Are Increased in Patients with Inflammatory Bowel Disease. J. Clin. Med. 2020, 9, 628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andreozzi, M.; Giugliano, F.P.; Strisciuglio, T.; Pirozzi, E.; Papparella, A.; Caprio, A.M.; Miele, E.; Strisciuglio, C.; Filardi, P.P. The Role of Inflammation in the Endothelial Dysfunction in a Cohort of Pediatric Patients with Inflammatory Bowel Disease. J. Pediatr. Gastroenterol. Nutr. 2019, 69, 330–335. [Google Scholar] [CrossRef]
- Principi, M.; Scicchitano, P.; Carparelli, S.; Nitti, R.; Ruggieri, R.; Bellino, M.C.; Cecere, A.; Manca, F.; Ciccone, M.M. Influence of systemic manifestations of inflam-matory bowel diseases on endothelial function and cardiovascular risk. Minerva Med. 2021, 113, 291–299. [Google Scholar] [CrossRef]
- Petr, J.; Michal, H.; Jan, S.; Ladislav, T.; Jiri, K.; Josef, S. Reactive hyperaemia index as a marker of endothelial dysfunction in children with Crohn’s disease is significantly lower than healthy controls. Acta Paediatr. 2014, 103, E55–E60. [Google Scholar] [CrossRef]
- Roifman, I.; Sun, Y.C.; Fedwick, J.P.; Panaccione, R.; Buret, A.G.; Liu, H.; Rostom, A.; Anderson, T.J.; Beck, P.L. Evidence of Endothelial Dysfunction in Patients With Inflammatory Bowel Disease. Clin. Gastroenterol. Hepatol. 2009, 7, 175–182. [Google Scholar] [CrossRef]
- Winderman, R.; Rabinowitz, S.S.; Vaidy, K.; Schwarz, S.M. Measurement of Microvascular Function in Pediatric Inflammatory Bowel Disease. J. Pediatr. Gastroenterol. Nutr. 2019, 68, 662–668. [Google Scholar] [CrossRef]
- Wu, H.; Hu, T.; Hao, H.; A Hill, M.; Xu, C.; Liu, Z. Inflammatory bowel disease and cardiovascular diseases: A concise review. Eur. Heart J. Open 2021, 2, oeab029. [Google Scholar] [CrossRef]
- Yeboah, J.; Folsom, A.R.; Burke, G.L.; Johnson, C.; Polak, J.F.; Post, W.; Lima, J.A.; Crouse, J.R.; Herrington, D.M. Predictive value of brachial flow-mediated dilation for incident cardiovascular events in a population-based study: The multi-ethnic study of atherosclerosis. Circulation 2009, 120, 502–509. [Google Scholar] [CrossRef] [Green Version]
- Maruhashi, T.; Soga, J.; Fujimura, N.; Idei, N.; Mikami, S.; Iwamoto, Y.; Kajikawa, M.; Matsumoto, T.; Hidaka, T.; Kihara, Y.; et al. Nitroglycerine-induced vasodilation for assessment of vascular function: A comparison with flow-mediated vasodilation. Arterioscler. Thromb. Vasc. Biol. 2013, 33, 1401–1408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenberry, R.; Nelson, M.D. Reactive hyperemia: A review of methods, mechanisms, and considerations. Am. J. Physiol. Integr. Comp. Physiol. 2020, 318, R605–R618. [Google Scholar] [CrossRef] [PubMed]
- Bonetti, P.O.; Pumper, G.M.; Higano, S.T.; Holmes, D.R., Jr.; Kuvin, J.T.; Lerman, A. Noninvasive identification of patients with early coronary atherosclerosis by assessment of digital reactive hyperemia. J. Am. Coll. Cardiol. 2004, 44, 2137–2141. [Google Scholar] [CrossRef] [Green Version]
- Laurent, S.; Boutouyrie, P.; Asmar, R.; Gautier, I.; Laloux, B.; Guize, L.; Ducimetiere, P.; Benetos, A. Aortic Stiffness Is an Independent Predictor of All-Cause and Cardiovascular Mortality in Hypertensive Patients. Hypertension 2001, 37, 1236–1241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitchell, G.F.; Hwang, S.-J.; Vasan, R.S.; Larson, M.G.; Levy, D.; Benjamin, E.J.; Pencina, M.J.; Hamburg, N.M.; Vita, J.A. Arterial Stiffness and Cardiovascular Events: The Framingham Heart Study. Circulation 2010, 121, 505–511. [Google Scholar] [CrossRef] [Green Version]
- Vlachopoulos, C.; Aznaouridis, K.; O’Rourke, M.F.; Safar, M.E.; Baou, K.; Stefanadis, C. Prediction of cardiovascular events and all-cause mortality with central haemodynamics: A systematic review and meta-analysis. Eur. Heart J. 2010, 31, 1865–1871. [Google Scholar] [CrossRef] [Green Version]
- Janner, J.H.; Godtfredsen, N.S.; Ladelund, S.; Vestbo, J.; Prescott, E. High aortic augmentation index predicts mortality and cardio-vascular events in men from a general population, but not in women. Eur. J. Prev. Cardiol. 2013, 20, 1005–1012. [Google Scholar] [CrossRef]
- Chung, W.-S.; Lin, C.-L.; Hsu, W.-H.; Kao, C.-H. Inflammatory Bowel Disease Increases the Risks of Deep Vein Thrombosis and Pulmonary Embolism in the Hospitalized Patients: A Nationwide Cohort Study. Thromb. Res. 2015, 135, 492–496. [Google Scholar] [CrossRef]
- Kristensen, S.L.; Ahlehoff, O.; Lindhardsen, J.; Erichsen, R.; Jensen, G.V.; Torp-Pedersen, C.; Nielsen, O.H.; Gislason, G.H.; Hansen, P.R. Disease activity in inflammatory bowel disease is associated with increased risk of myocardial infarction, stroke and cardiovascular death—A Danish nationwide cohort study. PLoS ONE 2013, 8, e56944. [Google Scholar] [CrossRef]
- Dregan, A.; Charlton, J.; Chowienczyk, P.; Gulliford, M.C. Chronic Inflammatory Disorders and Risk of Type 2 Diabetes Mellitus, Coronary Heart Disease, and Stroke: A population-based cohort study. Circulation 2014, 130, 837–844. [Google Scholar] [CrossRef] [Green Version]
- Kristensen, S.L.; Ahlehoff, O.; Lindhardsen, J.; Erichsen, R.; Lamberts, M.; Khalid, U.; Nielsen, O.H.; Torp-Pedersen, C.; Gislason, G.H.; Hansen, P.R. Inflammatory bowel disease is associated with an increased risk of hospitalization for heart failure: A Danish Nationwide Cohort study. Circ. Heart Fail. 2014, 7, 717–722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rungoe, C.; Basit, S.; Ranthe, M.F.; Wohlfahrt, J.; Langholz, E.; Jess, T. Risk of ischaemic heart disease in patients with inflammatory bowel disease: A nationwide Danish cohort study. Gut 2012, 62, 689–694. [Google Scholar] [CrossRef] [PubMed]
- Picchi, A.; Gao, X.; Belmadani, S.; Potter, B.J.; Focardi, M.; Chilian, W.M.; Zhang, C. Tumor necrosis factor-alpha induces endothelial dys-function in Lepr(db) mice. Circulation 2007, 115, 245–254. [Google Scholar]
- Esteve, E.; Castro, A.; Lopez-Bermejo, A.; Vendrell, J.; Ricart, W.; Fernandez-Real, J.-M. Serum Interleukin-6 Correlates With Endothelial Dysfunction in Healthy Men Independently of Insulin Sensitivity. Diabetes Care 2007, 30, 939–945. [Google Scholar] [CrossRef] [Green Version]
- Close, H.; Mason, J.; Wilson, D.W.; Hungin, A.P.; Jones, R.; Rubin, G. Risk of Ischaemic Heart Disease in Patients with Inflammatory Bowel Disease: Cohort Study Using the General Practice Research Database. PLoS ONE 2015, 10, e0139745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Fonseka, A.M.; Tuskey, A.; Conaway, M.R.; Behm, B.W. Antitumor Necrosis Factor-α Therapy Is Associated With Reduced Risk of Thromboembolic Events in Hospitalized Patients With Inflammatory Bowel Disease. J. Clin. Gastroenterol. 2016, 50, 578–583. [Google Scholar] [CrossRef] [PubMed]
- Tripodi, A.; Spina, L.; Pisani, L.F.; Padovan, L.; Cavallaro, F.; Chantarangkul, V.; Valsecchi, C.; Peyvandi, F.; Vecchi, M. Anti-TNF-α Treatment Reduces the Baseline Procoagulant Imbalance of Patients With Inflammatory Bowel Diseases. Inflamm. Bowel Dis. 2021, 27, 1901–1908. [Google Scholar] [CrossRef]
- Lewis, J.D.; Scott, F.I.; Brensinger, C.M.; Roy, J.A.; Osterman, M.T.; Mamtani, R.; Bewtra, M.; Chen, L.; Yun, H.; Xie, F.; et al. Increased Mortality Rates With Prolonged Cor-ticosteroid Therapy When Compared With Antitumor Necrosis Factor-α-Directed Therapy for Inflammatory Bowel Disease. Am. J. Gastroenterol. 2018, 113, 405–417. [Google Scholar] [CrossRef] [Green Version]
- Olivera, P.A.; Zuily, S.; Kotze, P.G.; Regnault, V.; Al Awadhi, S.; Bossuyt, P.; Gearry, R.B.; Ghosh, S.; Kobayashi, T.; Lacolley, P.; et al. International consensus on the prevention of venous and arterial thrombotic events in patients with inflammatory bowel disease. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 857–873. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Population (n) IBD/Controls | Studies (n) | IBD | Controls | Log Odds Ratio or Cohen’s d | 95% CI | p Value | I2 % |
|---|---|---|---|---|---|---|---|---|
| Female | 1058/988 | 41 | 45.4% | 48.6% | −0.100 | −0.223, 0.023 | 0.1127 | 0 |
| Smoking | 241/195 | 35 | 12.5% | 11.6% | 0.090 | −0.131, 0.312 | 0.4252 | 0 |
| Hypertension | 71/66 | 33 | 3.5% | 3.8% | 0.054 | −0.292, 0.400 | 0.7586 | 0 |
| DM | 15/16 | 39 | 0.7% | 0.8% | −0.095 | −0.601, 0.412 | 0.7134 | 0 |
| Age (years) | 2330/2032 | 41 | 37.4 | 37.7 | 0.081 | −0.003, 0.165 | 0.06 | 43.46 |
| BMI (kg/m2) | 2136/1862 | 36 | 23.9 | 24.7 | −0.237 | −0.369, −0.105 | 0.0004 | 74.71 |
| TC (mg/dL) | 1549/1368 | 26 | 172 | 184 | −0.238 | −0.365, −0.111 | 0.0002 | 61.94 |
| LDLc (mg/dL) | 1486/1238 | 25 | 102 | 111 | −0.200 | −0.349, −0.050 | 0.0088 | 70.94 |
| HDLc (mg/dL) | 1557/1340 | 25 | 50 | 52 | −0.152 | −0.267, −0.037 | 0.0095 | 52.88 |
| TGs (mg/dL) | 1638/1360 | 26 | 114 | 112 | −0.042 | −0.175, 0.091 | 0.5368 | 66.00 |
| No. of Studies | No. of Cases/Controls | Cohen’s d [95% CI] | p Value | I2 % | |
|---|---|---|---|---|---|
| Panel A | |||||
| cIMT | 17 | 1023/905 | 0.710 [0.345, 1.075] | 0.0001 | 92.89 |
| cfPWV | 10 | 648/524 | 0.673 [0.488, 0.857] | <0.0001 | 55.99 |
| FMD | 3 | 214/137 | −0.741 [−0.964, −0.519] | <0.0001 | 0 |
| Panel B | |||||
| cIMT | 21 | 1281/1069 | 0.616 [0.295, 0.937] | 0.0002 | 92.55 |
| cfPWV | 12 | 714/571 | 0.759 [0.541, 0.977] | <0.0001 | 70.03 |
| FMD | 6 | 375/248 | −0.679 [−1.134, −0.225] | 0.0034 | 85.42 |
| Panel C | |||||
| cIMT | 11 | 506/379 | 0.652 [0.073, 1.231] | 0.0272 | 93.74 |
| cfPWV | 6 | 348/296 | 0.858 [0.426, 1.290] | 0.0001 | 84.80 |
| FMD | 0 | NA | NA | NA | NA |
| Moderators | Coefficient | 95% CI | Z-Test | p Value |
|---|---|---|---|---|
| CRP | −0.0097 | −0.0441, 0.0247 | −0.55 | 0.580 |
| ESR | 0.0265 | −0.0053, 0.0584 | 1.63 | 0.102 |
| Disease duration | −0.0462 | −0.1544, 0.0621 | −0.84 | 0.403 |
| Salicylates | 0.0033 | −0.0085, 0.0151 | 0.54 | 0.488 |
| Steroids | −0.0130 | −0.0304, 0.0045 | −1.46 | 0.145 |
| Immunomodulator | −0.0047 | −0.0244, 0.0150 | −0.47 | 0.640 |
| Biologics | −0.0104 | −0.0233, 0.0025 | −1.58 | 0.113 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, H.; Xu, M.; Hao, H.; Hill, M.A.; Xu, C.; Liu, Z. Endothelial Dysfunction and Arterial Stiffness in Patients with Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 3179. https://doi.org/10.3390/jcm11113179
Wu H, Xu M, Hao H, Hill MA, Xu C, Liu Z. Endothelial Dysfunction and Arterial Stiffness in Patients with Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2022; 11(11):3179. https://doi.org/10.3390/jcm11113179
Chicago/Turabian StyleWu, Hao, Meihua Xu, Hong Hao, Michael A. Hill, Canxia Xu, and Zhenguo Liu. 2022. "Endothelial Dysfunction and Arterial Stiffness in Patients with Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 11, no. 11: 3179. https://doi.org/10.3390/jcm11113179
APA StyleWu, H., Xu, M., Hao, H., Hill, M. A., Xu, C., & Liu, Z. (2022). Endothelial Dysfunction and Arterial Stiffness in Patients with Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 11(11), 3179. https://doi.org/10.3390/jcm11113179