
The Race to Replace PDE5i: Recent Advances and Interventions to Treat or Manage Erectile Dysfunction: Evidence from Patent Landscape (2016–2021)

 , , ,
, , ,  , ,
, ,  , and
, and 
Abstract
1. Introduction
2. Clinical Trials Related to ED
2.1. Summary of Clinical Trials Data
2.2. Clinical Trials on Tadalafil
2.3. Clinical Trials on Vardenafil
2.4. Clinical Trials on Avanafil
3. Prospection of Scholarly Articles
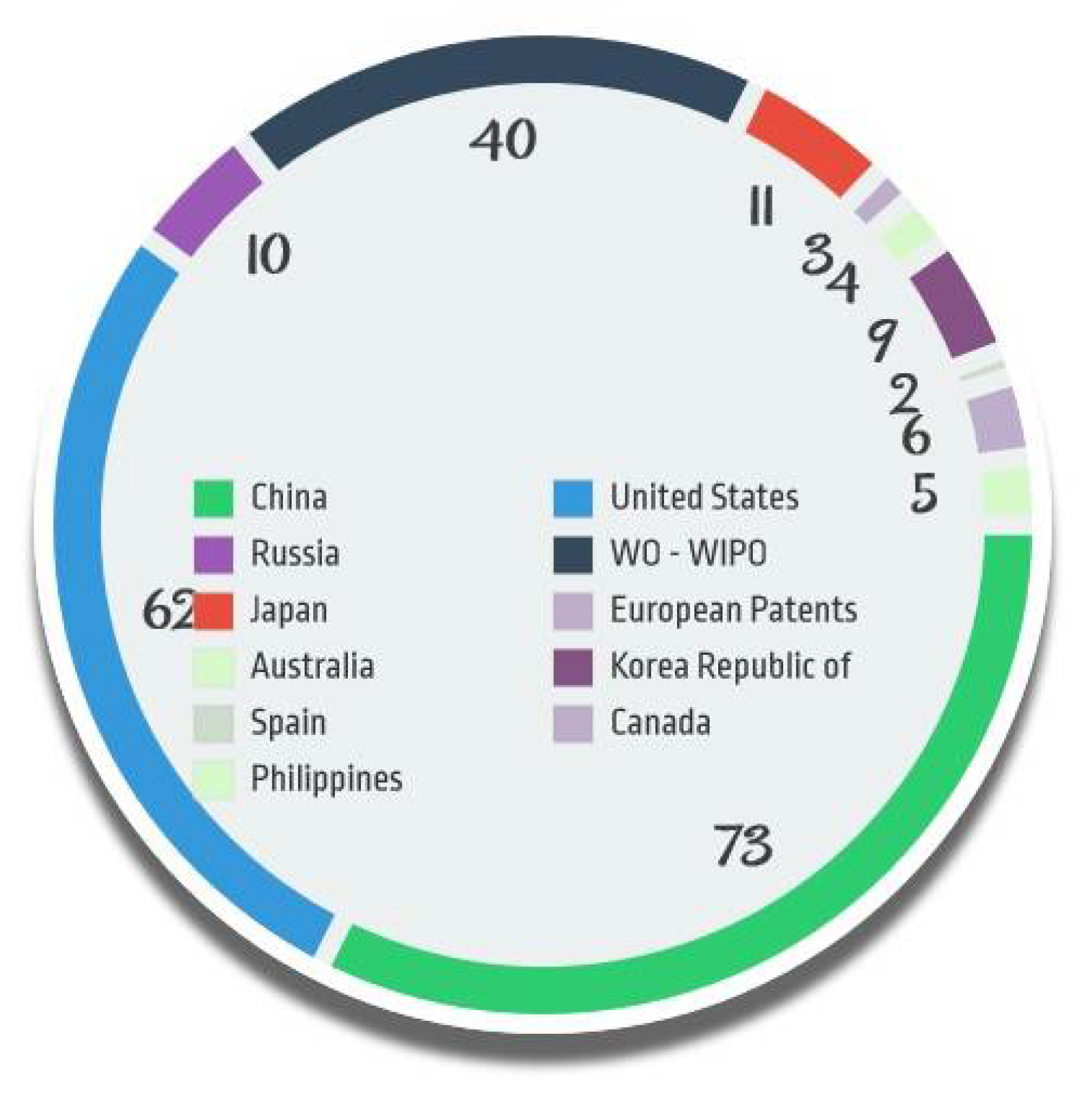
4. Patent Analysis
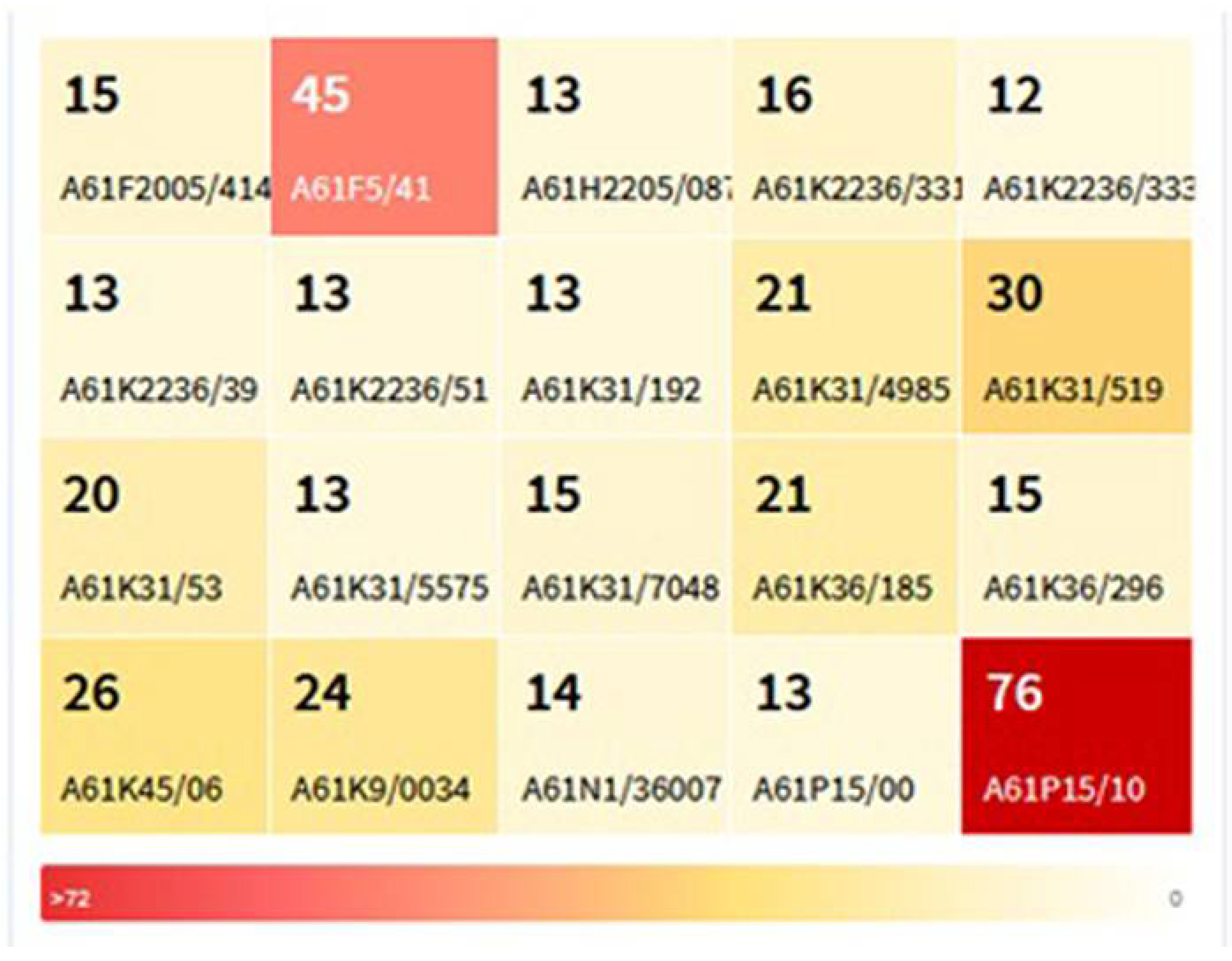
Patents Classification and Concordance
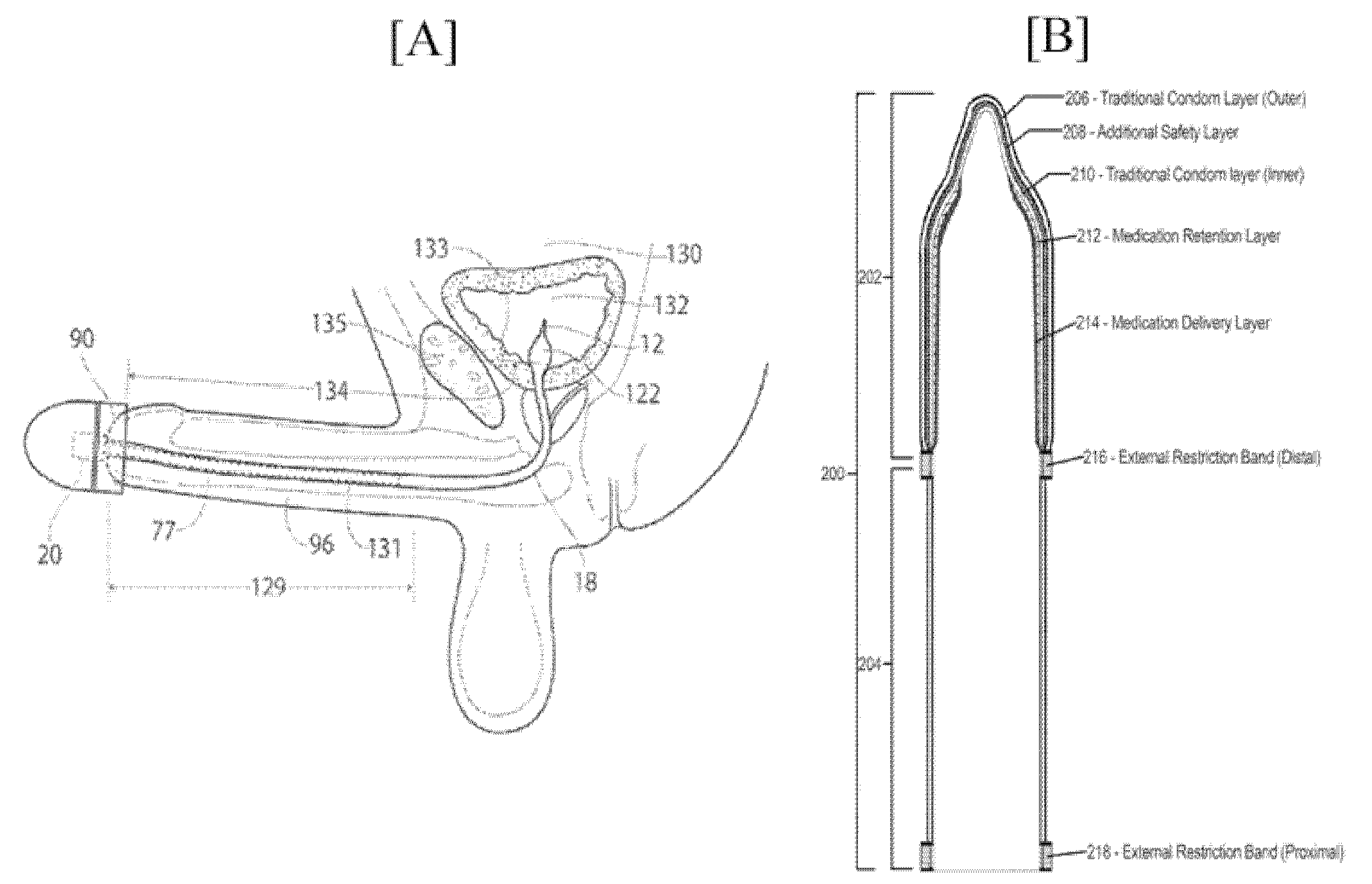
5. Technical Aspects of Few Patents on ED
6. Conclusions
Funding
Acknowledgments
Conflicts of Interest
References
- Porst, H.; Vardi, Y.; Akkus, E.; Melman, A.; Park, N.C.; Seftel, A.D.; Teloken, C.; Wyllie, M. Standards for Clinical Trials in Male Sexual Dysfunctions. J. Sex. Med. 2010, 7, 414–444. [Google Scholar] [CrossRef] [PubMed]
- Kurakula, M.; Naveen, N.R.; Patel, B.; Manne, R.; Patel, D.B. Preparation, Optimization and Evaluation of Chitosan-Based Avanafil Nanocomplex Utilizing Antioxidants for Enhanced Neuroprotective Effect on PC12 Cells. Gels 2021, 7, 96. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, M.D.; Wessells, H. Management of Erectile Dysfunction. In Evidence-Based Urology; BMJ Books: London, UK, 2010; Volume 81, pp. 134–145. ISBN 9781405185943. [Google Scholar]
- Yafi, F.A.; Jenkins, L.; Albersen, M.; Corona, G.; Isidori, A.M.; Goldfarb, S.; Maggi, M.; Nelson, C.J.; Parish, S.; Salonia, A.; et al. Erectile Dysfunction. Nat. Rev. Dis. Prim. 2016, 2, 16003. [Google Scholar] [CrossRef] [PubMed]
- Feldman, H.A.; Goldstein, I.; Hatzichristou, D.G.; Krane, R.J.; McKinlay, J.B. Impotence and Its Medical and Psychosocial Correlates: Results of the Massachusetts Male Aging Study. J. Urol. 1994, 151, 54–61. [Google Scholar] [CrossRef]
- Bacon, C.G.; Mittleman, M.A.; Kawachi, I.; Giovannucci, E.; Glasser, D.B.; Rimm, E.B. Sexual Function in Men Older Than 50 Years of Age: Results from the Health Professionals Follow-up Study. Ann. Intern. Med. 2003, 139, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Mccabe, M.P.; Althof, S.E. A Systematic Review of the Psychosocial Outcomes Associated with Erectile Dysfunction: Does the Impact of Erectile Dysfunction Extend beyond a Man’s Inability to Have Sex? J. Sex. Med. 2014, 11, 347–363. [Google Scholar] [CrossRef]
- Kessler, A.; Sollie, S.; Challacombe, B.; Briggs, K.; Van Hemelrijck, M. The Global Prevalence of Erectile Dysfunction: A Review. BJU Int. 2019, 124, 587–599. [Google Scholar] [CrossRef]
- Moreira, E.D.; Lôbo, C.F.L.; Diament, A.; Nicolosi, A.; Glasser, D.B. Incidence of Erectile Dysfunction in Men 40 to 69 Years Old: Results from a Population-Based Cohort Study in Brazil. Urology 2003, 61, 431–436. [Google Scholar] [CrossRef]
- Schouten, B.W.V.; Bosch, J.L.H.R.; Bernsen, R.M.D.; Blanker, M.H.; Thomas, S.; Bohnen, A.M. Incidence Rates of Erectile Dysfunction in the Dutch General Population. Effects of Definition, Clinical Relevance and Duration of Follow-up in the Krimpen Study. Int. J. Impot. Res. 2005, 17, 58–62. [Google Scholar] [CrossRef]
- Lizza, E.F.; Rosen, R.C. Definition and Classification of Erectile Dysfunction: Report of the Nomenclature Committee of the International Society of Impotence Research. Int. J. Impot. Res. 1999, 11, 141–143. [Google Scholar] [CrossRef]
- McVary, K.T. Clinical Practice. Erectile Dysfunction. N. Engl. J. Med. 2007, 357, 2472–2481. [Google Scholar] [CrossRef] [PubMed]
- Erectile Dysfunction (ED) Guideline—American Urological Association. Available online: https://www.auanet.org/guidelines/guidelines/erectile-dysfunction-(ed)-guideline (accessed on 24 August 2021).
- Bocchio, M.; Scarpelli, P.; Necozione, S.; Pelliccione, F.; Spartera, C.; Francavilla, F.; Francavilla, S. Penile Duplex Pharmaco-Ultrasonography of Cavernous Arteries in Men with Erectile Dysfunction and Generalized Atherosclerosis. Int. J. Androl. 2006, 29, 496–501. [Google Scholar] [CrossRef] [PubMed]
- Montague, D.K.; Jarow, J.P.; Broderick, G.A.; Dmochowski, R.R.; Heaton, J.P.W.; Lue, T.F.; Milbank, A.J.; Nehra, A.; Sharlip, I.D. Chapter 1: The Management of Erectile Dysfunction: An AUA Update. J. Urol. 2005, 174, 230–239. [Google Scholar] [CrossRef] [PubMed]
- Search of: Erectile Dysfunction—List Results. Available online: https://clinicaltrials.gov/ct2/results?cond=erectile+dysfunction&term=&cntry=&state=&city=&dist= (accessed on 24 August 2021).
- Buvat, J.; Büttner, H.; Hatzimouratidis, K.; Vendeira, P.A.S.; Moncada, I.; Boehmer, M.; Henneges, C.; Boess, F.G. Adherence to Initial PDE-5 Inhibitor Treatment: Randomized Open-Label Study Comparing Tadalafil Once a Day, Tadalafil on Demand, and Sildenafil on Demand in Patients with Erectile Dysfunction. J. Sex. Med. 2013, 10, 1592–1602. [Google Scholar] [CrossRef]
- A Study in Patients with Erectile Dysfunction—Full Text View. Available online: https://clinicaltrials.gov/ct2/show/NCT01122264?cond=erectile+dysfunction&phase=3&draw=5&rank=1 (accessed on 4 April 2022).
- Evaluating the Efficacy Vardenafil 10 mg vs Tadalafil 10 mg in in Subjects with Erectile Dysfunction (ED)—Full Text View. Available online: https://clinicaltrials.gov/ct2/show/NCT00663130?cond=erectile+dysfunction&phase=3&draw=2&rank=7 (accessed on 4 April 2022).
- Carrier, S.; Brock, G.B.; Pommerville, P.J.; Shin, J.; Anglin, G.; Whitaker, S.; Beasley, C.M. Efficacy and Safety of Oral Tadalafil in the Treatment of Men in Canada with Erectile Dysfunction: A Randomized, Double-Blind, Parallel, Placebo-Controlled Clinical Trial. J. Sex. Med. 2005, 2, 685–698. [Google Scholar] [CrossRef] [PubMed]
- Boddi, V.; Castellini, G.; Casale, H.; Rastrelli, G.; Boni, L.; Corona, G.; Maggi, M. An Integrated Approach with Vardenafil Orodispersible Tablet and Cognitive Behavioral Sex Therapy for Treatment of Erectile Dysfunction: A Randomized Controlled Pilot Study. Andrology 2015, 3, 909–918. [Google Scholar] [CrossRef]
- Vardenafil and Cognitive-behavioral Sex Therapy for the Treatment of Erectile Dysfunction (STEDOV)—Full Text View. Available online: https://clinicaltrials.gov/ct2/show/NCT02450188?cond=erectile+dysfunction&phase=3&draw=5&rank=2 (accessed on 4 April 2022).
- Mastiholimath, V.S.; Dandagi, P.M.; Jain, S.S.; Gadad, A.P.; Kulkarni, A.R. Time and pH Dependent Colon Specific, Pulsatile Delivery of Theophylline for Nocturnal Asthma. Int. J. Pharm. 2007, 328, 49–56. [Google Scholar] [CrossRef]
- Evaluation of Efficacy and Safety of Vardenafil in Patients with Erectile Dysfunction and Type 1 Diabetes—Full Text View. Available online: https://clinicaltrials.gov/ct2/show/NCT00660998?cond=erectile+dysfunction&phase=3&draw=2&rank=11 (accessed on 4 April 2022).
- Evaluation of the Safety and Efficacy of Vardenafil in Subjects with Erectile Dysfunction—Full Text View. Available online: https://clinicaltrials.gov/ct2/show/NCT00681772?cond=erectile+dysfunction&phase=3&draw=2&rank=4 (accessed on 4 April 2022).
- Evaluating of the Efficacy and Safety of Vardenafil in Subjects with Erectile Dysfunction—Full Text View. Available online: https://clinicaltrials.gov/ct2/show/NCT00662441?cond=erectile+dysfunction&phase=3&draw=2&rank=6 (accessed on 4 April 2022).
- Daily Avanafil for Erectile Dysfunction—Full Text View. Available online: https://clinicaltrials.gov/ct2/show/NCT04374994?cond=erectile+dysfunction&phase=3&draw=2&rank=24 (accessed on 4 April 2022).
- Mobley, D.F.; Khera, M.; Baum, N. Recent Advances in the Treatment of Erectile Dysfunction. Postgrad. Med. J. 2017, 93, 679–685. [Google Scholar] [CrossRef]
- Khera, M.; Albersen, M.; Mulhall, J.P. Mesenchymal Stem Cell Therapy for the Treatment of Erectile Dysfunction. J. Sex. Med. 2015, 12, 1105–1106. [Google Scholar] [CrossRef]
- Gong, B.; Ma, M.; Xie, W.; Yang, X.; Huang, Y.; Sun, T.; Luo, Y.; Huang, J. Direct Comparison of Tadalafil with Sildenafil for the Treatment of Erectile Dysfunction: A Systematic Review and Meta-Analysis. Int. Urol. Nephrol. 2017, 49, 1731–1740. [Google Scholar] [CrossRef]
- Sin, V.J.E.; Anand, G.S.; Koh, H.L. Botanical Medicine and Natural Products Used for Erectile Dysfunction. Sex. Med. Rev. 2021, 9, 568–592. [Google Scholar] [CrossRef] [PubMed]
- Scott, S.; Roberts, M.; Chung, E. Platelet-Rich Plasma and Treatment of Erectile Dysfunction: Critical Review of Literature and Global Trends in Platelet-Rich Plasma Clinics. Sex. Med. Rev. 2019, 7, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Angulo, J.C.; Arance, I.; de las Heras, M.M.; Meilán, E.; Esquinas, C.; Andrés, E.M. Eficacia de la Terapia de Ondas de Choque de Baja Intensidad para la Disfunción Eréctil: Revisión Sistemática y Metaanálisis. Actas Urol. Esp. 2017, 41, 479–490. [Google Scholar] [CrossRef] [PubMed]
- Guillén, V.; Rueda, J.R.; Lopez-Argumedo, M.; Solà, I.; Ballesteros, J. Apomorphine for the Treatment of Erectile Dysfunction: Systematic Review and Meta-Analysis. Arch. Sex. Behav. 2020, 49, 2963–2979. [Google Scholar] [CrossRef]
- Diehm, N.; Marggi, S.; Ueki, Y.; Schumacher, D.; Keo, H.H.; Regli, C.; Do, D.D.; Moeltgen, T.; Grimsehl, P.; Wyler, S.; et al. Endovascular Therapy for Erectile Dysfunction—Who Benefits Most? Insights From a Single-Center Experience. J. Endovasc. Ther. 2019, 26, 181–190. [Google Scholar] [CrossRef]
- Hsieh, C.H.; Hsu, G.L.; Chang, S.J.; Yang, S.S.D.; Liu, S.P.; Hsieh, J.T. Surgical Niche for the Treatment of Erectile Dysfunction. Int. J. Urol. 2020, 27, 117–133. [Google Scholar] [CrossRef]
- Güven, E. Lipid-Based Nanoparticles in the Treatment of Erectile Dysfunction. Int. J. Impot. Res. 2020, 32, 578–586. [Google Scholar] [CrossRef] [PubMed]
- Hosny, K.M.; Aldawsari, H.M. Avanafil Liposomes as Transdermal Drug Delivery for Erectile Dysfunction Treatment: Preparation, Characterization, and In Vitro, Ex Vivo and In Vivo Studies. Trop. J. Pharm. Res. 2015, 14, 559–565. [Google Scholar] [CrossRef][Green Version]
- Hosny, K.M.; Ahmed, O.A.A.; Fahmy, U.A.; Alkhalidi, H.M. Nanovesicular Systems Loaded with a Recently Approved Second Generation Type-5 Phospo-Diesterase Inhibitor (Avanafil): I. Plackett-Burman Screening and Characterization. J. Drug Deliv. Sci. Technol. 2018, 43, 154–159. [Google Scholar] [CrossRef]
- Kurakula, M.; Ahmed, O.A.A.; Fahmy, U.A.; Ahmed, T.A. Solid Lipid Nanoparticles for Transdermal Delivery of Avanafil: Optimization, Formulation, In-Vitro and Ex-Vivo Studies. J. Liposome Res. 2016, 26, 288–296. [Google Scholar] [CrossRef]
- Fahmy, U.A.; Ahmed, O.A.A.; Hosny, K.M. Development and Evaluation of Avanafil Self-nanoemulsifying Drug Delivery System with Rapid Onset of Action and Enhanced Bioavailability. AAPS PharmSciTech 2014, 16, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Fahmy, U.A. Nanoethosomal Transdermal Delivery of Vardenafil for Treatment of Erectile Dysfunction: Optimization, Characterization, and In Vivo Evaluation. Drug Des. Devel. Ther. 2015, 9, 6129. [Google Scholar] [CrossRef] [PubMed]
- Parikh, K.J.; Sawant, K.K. Solubilization of Vardenafil HCl in Lipid-Based Formulations Enhances Its Oral Bioavailability In Vivo: A Comparative Study using Tween-20 and Cremophor-EL. J. Mol. Liq. 2019, 277, 189–199. [Google Scholar] [CrossRef]
- Badr-Eldin, S.M.; Ahmed, O.A. Optimized Nano-Transfersomal Films for Enhanced Sildenafil Citrate Transdermal Delivery: Ex Vivo and In Vivo Evaluation. Drug Des. Devel. Ther. 2016, 10, 1323. [Google Scholar] [CrossRef]
- Hosny, K.M.; Aljaeid, B.M. Sildenafil Citrate as Oral Solid Lipid Nanoparticles: A Novel Formula with Higher Bioavailability and Sustained Action for Treatment of Erectile Dysfunction. Expert Opin. Drug Deliv. 2014, 11, 1015–1022. [Google Scholar] [CrossRef]
- Ali, M.F.M.; Salem, H.F.; Abdelmohsen, H.F.; Attia, S.K. Preparation and Clinical Evaluation of Nano-Transferosomes for Treatment of Erectile Dysfunction. Drug Des. Devel. Ther. 2015, 9, 2431. [Google Scholar] [CrossRef]
- Baek, J.S.; Pham, C.V.; Myung, C.S.; Cho, C.W. Tadalafil-Loaded Nanostructured Lipid Carriers Using Permeation Enhancers. Int. J. Pharm. 2015, 495, 701–709. [Google Scholar] [CrossRef]
- Fahmy, U.A.; Aljaeid, B.M. Tadalafil Transdermal Delivery with Alpha-Lipoic Acid Self Nanoemulsion for Treatment of Erectile Dysfunction by Diabetes Mellitus. Int. J. Pharmacol. 2018, 14, 945–951. [Google Scholar] [CrossRef]
- Kurakula, M. Prospection of Recent Chitosan Biomedical Trends: Evidence from Patent Analysis (2009–2020). Int. J. Biol. Macromol. 2020, 165, 1924–1938. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| S. No. | Study Title | Interventions | Locations |
|---|---|---|---|
| 1. | A Study in Patients With Erectile Dysfunction | Drug: Tadalafil Drug: Sildenafil Citrate | Carpentras, France Chambery, France La Bouexiere, France |
| 2. | Vardenafil and Cognitive-behavioral Sex Therapy for the Treatment of Erectile Dysfunction (STEDOV) | Drug: Vardenafil Behavioral: CBST | AmbulatoriMedicinadellaSessualità e Andrologia Florence, Italy |
| 3. | Evaluation of the Safety and Efficacy of Vardenafil in Subjects With Erectile Dysfunction | Drug: Levitra (Vardenafil, BAY38-9456) | |
| 4. | Assessment of Vardenafil in Patients With Erectile Dysfunction in Asia | Drug: Vardenafil (Levitra, BAY38-9456) Drug: Placebo | Hong Kong, Jakarta, Indonesia Petlaing Jaya, Salangor, Malaysia |
| 5. | Evaluating of the Efficacy and Safety of Vardenafil in Subjects With Erectile Dysfunction | Drug: Levitra (Vardenafil, BAY38-9456) | |
| 6. | Evaluating the Efficacy Vardenafil 10 mg vsTadalafil 10 mg in in Subjects With Erectile Dysfunction (ED) | Drug: Levitra (Vardenafil, BAY38-9456) Drug: Tadalafil | |
| 7. | Investigate the Responsiveness of the Erectile Quality Scale to Vardenafil Flexible Dose vs. Placebo in Males With Erectile Dysfunction (ED) | Drug: Placebo Drug: Levitra (Vardenafil, BAY38-9456) | Phoenix, Arizona, United States Beverly Hills, California, United States Laguna Hills, California, United States |
| 8. | Efficacy and Safety of Lodenafil Carbonate in the Treatment of Erectile Dysfunction in Patients With Diabetes. | Drug: lodenafil carbonate | SP, Brazil |
| 9. | BAY38-9456, 5/10/20 mg, vs.Placebo in Erectile Dysfunction | Drug: Levitra (Vardenafil, BAY38-9456) Drug: Placebo | Adana, Turkey |
| 10. | Evaluation of Efficacy and Safety of Vardenafil in Patients With Erectile Dysfunction and Type 1 Diabetes | Drug: Levitra (Vardenafil, BAY38-9456) Drug: Placebo | |
| 11. | The Efficacy and Safety of New Herbal Formula (KBMSI-2) in the Treatment of Erectile Dysfunction | Drug: KBMSI-2 | Department of Urology, Pusan National University Hospital Busan, Korea, |
| 12. | Assessing Efficacy and Safety of Flexible Dosing With Vardenafil in Subjects With Erectile Dysfunction and Hyperlipidemia | Drug: Levitra (Vardenafil, BAY38-9456) Drug: Placebo | |
| 13. | A Study of Tadalafil (LY450190) in Chinese Men With Erectile Dysfunction | Drug: Tadalafil | Beijing, China Changsha, China |
| 14. | Research Evaluating a PDE5 Inhibitor for Erectile Dysfunction | Drug: Placebo Drug: Avanafil 100 mg Drug: Avanafil 200 mg | Jupiter, Florida, United States Raleigh, North Carolina, United States Wilmington, North Carolina, United States |
| 15. | Satisfaction, Confidence and Naturalness in Men With Psychogenic Erectile Dysfunction (ED) | Behavioral: Group Psychotherapy Other: Group Psychotherapy plus Sildenafil citrate Drug: Sildenafil citrate | |
| 16. | Evaluation of LEVITRA to Advance the Treatment of Erectile Dysfunction | Behavioral: Levitra (Vardenafil, BAY38-9456) Other: No Education | |
| 17. | A Study Evaluating Vardenafil Compared to Placebo in Subjects With Erectile Dysfunction (ED) and Dyslipidemia | Drug: LEVITRA (vardenafil) Drug: placebo | Investigational Site Fairhope, Alabama, United States Investigational Site Homewood, Alabama, United States Investigational Site Huntsville, Alabama, United States |
| 18. | A Study of Tadalafil and Sildenafil in Men With Erectile Dysfunction in China | Drug: Tadalafil Drug: Sildenafil | Beijing, China Changsha, China Hangzhou, China |
| 19. | L-Arginine and Erectile Dysfunction | Drug: L-arginine Drug: Placebo | Institute of Clinical Pharmacology, Hannover Medical School Hannover, Lower Saxony, Germany |
| 20. | Effect of Tadalafil on the Quality of Life and Sexual Life in Erectile Dysfunction | Drug: tadalafil | Tampere, Finland |
| 21. | Daily Avanafil for Erectile Dysfunction | Drug: Avanafil 50 MG Drug: Placebo oral tablet | Faculty of Medicine, Alexandria University. Alexandria, Elazareta, Egypt |
| 22. | A Randomized, Open-Label, Crossover, Multicenter, Single Dose Comparator Study Evaluating Onset Of Penile Rigidity In Men With Erectile Dysfunction Who Are Treated With Sildenafil And Tadalafil | Drug: tadalafil Drug: sildenafil | Pfizer Investigational Site Oslo, Norway Leeds, UK |
| 23. | A Study in Erectile Dysfunction | Drug: Placebo Drug: Tadalafil | Indianapolis, Indiana, United States |
| 24. | Evaluating the Efficacy of Vardenafil in Subjects With Erectile Dysfunction (ED) Administered 12, 18 or 24 Hours Prior to Intercourse | Drug: Levitra (Vardenafil, BAY38-9456) Drug: Placebo | |
| 25. | The Therapy of Nebido as Mono or in Combination With PDE-5 Inhibitors in Hypogonadal Patients With Erectile Dysfunction | Drug: Testosterone Undecanoate,1000 mg | Siriraj Hospital Bangkoknoi, Ramathibodi Hospital Rajthevee, King Chulalongkorn Memorial Hospital Bangkok, Thailand |
| 26. | A Randomised Study of Levitra to Treat Men With Erections Problems and Previously Untreated With Similar Therapy. | Drug: Levitra (Vardenafil, BAY38-9456) Drug: Placebo | Bruxelles-Brussel, Belgium Drieslinter, Belgium Genk, Belgium |
| 27. | A Safety and Efficacy Study of Prograf in the Prevention of Erectile Dysfunction After Radical Prostatectomy | Drug: Tacrolimus Drug: Placebo | Ann Arbor, Michigan, United States New York, New York, United States |
| 28. | Study of Vardenafil in Patients Suffering From Erectile Dysfunction and Metabolic Syndrome | Drug: Vardenafil (Levitra, BAY38-9456) Drug: Placebo | Cham, Bayern, Germany Regensburg, Bayern, Germany Frankfurt, Hessen, Germany |
| 29. | Exploratory CSII Trial on Erectile Dysfunction in T2DM Patients | Drug: Insulin | Jothydev’s Diabetes & Research Center Thiruvananthapuram, Kerala, India |
| 30. | Study Evaluating the Effects of Avanafil on Semen Parameters | Drug: avanafil Drug: Placebo | Research Facility Huntsville, Alabama, LA, California, San Diego, California, United States |
| 31. | Correlation Study of Vascular Parameters in Hypertensive Men With Erectile Dysfunction | Drug: Vardenafil | Hospital Universitário Pedro Ernesto Rio de Janeiro, Brazil |
| 32. | A Study of Tadalafil After Radical Prostatectomy | Drug: Tadalafil Drug: Placebo | Kortrijk, Belgium Leuven, Belgium Liège, Belgium |
| 33. | Assessment of Duration of Erection With Vardenafil 10 mg | Drug: Levitra (Vardenafil, BAY38-9456) Drug: Placebo | |
| 34. | Levitra®—Real Life Safety and Efficacy of Levitra | Drug: Levitra (Vardenafil, BAY38-9456) | |
| 35. | Early Intervention for Erectile Dysfunction After Laparoscopic Resection for Rectal Cancer | Other: vacuum erection device | Department of General Surgery, Nanfang Hospital of Southern Medical University Guangzhou, Guangdong, China |
| 36. | A Study of Semen Characteristics After 9 Months of Daily Tadalafil 20 mg | Drug: tadalafil Drug: placebo | Bothell, Washington, United States |
| 37. | Bioequivalence Study Comparing Two Test Products With One Reference Product, All Containing 5 mg Yohimbine | Drug: Yohimbine | SocraTec R&D GmbH Erfurt, Germany |
| 38. | Assess Efficacy in Subjects With Traumatic Spinal Cord Injury | Drug: Vardenafil (Levitra, BAY 38-9456), 10 mg Drug: Placebo Drug: Vardenafil (Levitra, BAY 38-9456), 20 mg | Badalona, Barcelona, Spain Toledo, Spain |
| S. No | ED Drug | Lipid Based System | Route/Mode of Administration | Ref. |
|---|---|---|---|---|
| 1. | Avanafil | Lipsome | Transdermal | [38] |
| Nanoethosome | Transdermal | [39] | ||
| Solid lipid nanoparticle | Transdermal | [40] | ||
| Self-emulsifying drug delivery systems | Oral | [41] | ||
| Nano complex | Oral | [2] | ||
| 2. | Vardenafil | Nanoethosome | Transdermal | [42] |
| Self-emulsifying drug delivery systems | Oral | [43] | ||
| 3. | Sildenafil Citrate | Nanotransfersome | Transdermal | [44] |
| Solid lipid nanoparticle | Oral | [45] | ||
| 4. | Papaverine Hydrochloride | Nanotransfersome | Transdermal | [46] |
| 5. | Tadalafil | Nano lipid carrier | Transdermal | [47] |
| 6. | Tadalafil and alpha lipolic acid | Self emulsifying drug delivery systems | Transdermal | [48] |
| Jurisdi-ction | Publication Year | Application Number | Title | Applicants |
|---|---|---|---|---|
| US | 2021 | US 16355248 | Erectile dysfunction treatment system and method | Sergio Castaneda |
| US | 2021 | US 201916597212 A | Composition for treating erectile dysfunction by orchisanatolica extract | Jordan Univ Of Science And Technology |
| US | 2021 | US 201916444906 A | Compositions and methods for treating, inhibiting the onset, and slowing the progression of erectile dysfunction including naturally occurring age related erectile dysfunction | K L R M Llc |
| US | 2021 | US 201916266293 A | Method for treating organic erectile dysfunction | Bmr Medical Llc |
| US | 2021 | US 201715793905 A | Implantable electroacupuncture device and method for treating erectile dysfunction | Valencia Tech Corporation;;Valencia Bioscience Inc |
| RU | 2021 | RU 2020111687 A | Method of treating erectile dysfunction in patients suffering radical prostatectomy or brachytherapy | FederalnoeGosudarstvennoeByudzhetnoeUchrezhdenieNatsionalnyjMeditsinskijIssledovatelskijTsent |
| US | 2021 | US 202117214142 A | Device for managing male urinary incontinence and reducing erectile dysfunction | Mohamed Adel W |
| US | 2021 | US 201815979265 A | Compositions and methods useful in treatment of lower urinary tract symptoms, benign prostatic hyperplasia, erectile dysfunction and other diseases or symptoms | NaturexInc |
| US | 2021 | US 201916532367 A | Compositions and methods useful in treatment of lower urinary tract symptoms, benign prostatic hyperplasia, erectile dysfunction and other diseases or symptoms | NaturexInc |
| RU | 2020 | RU 2019128290 A | Agent for treating erectile dysfunction | Pivipi Labs Pte Ltd. |
| US | 2020 | US 201715710914 A | Methods for the treatment of erectile dysfunction by human birth tissue material composition | BiodlogicsLlc |
| US | 2020 | US 201715434226 A | Compositions and methods for treatment of erectile dysfunction | Caprio James J |
| US | 2020 | US 201815878423 A | Methods and devices for treating erectile dysfunction | Ohh Med Medical Ltd. |
| RU | 2020 | RU 2020107786 A | Method of treating patients with erectile dysfunction | FederalnoeGosudarstvennoeByudzhetnoeUchrezhdenieNatsionalnyjMeditsinskijIssledovatelskijTsent |
| US | 2020 | US 201815873000 A | Method of implanting a penile prosthetic in treating erectile dysfunction | Coloplast As |
| RU | 2020 | RU 2019125324 A | Portable device for personal diagnosis of erectile dysfunction symptoms | Andreev YurijGermanovich |
| US | 2020 | US 201715652258 A | Topical medication method for erectile dysfunction | Lange Iv Carl W |
| US | 2019 | US 201615133840 A | Treating erectile dysfunction by orchisanatolica extract | Jordan Univ Of Science And Technology |
| RU | 2019 | RU 2018133729 A | Method of treating premature ejaculation and erectile dysfunction | FederalnoeGosudarstvennoeByudzhetnoeUchrezhdenieNovosibirskijNauchnoIssledovatelskijInstitut |
| RU | 2019 | RU 2019106747 A | Method of treating erectile dysfunction | FederalnoeGosudarstvennoeByudzhetnoeUchrezhdenieNatsionalnyjMeditsinskijIssledovatelskijTsent |
| US | 2019 | US 201615064162 A | Method for treating organic erectile dysfunction | Bmr Medical Llc |
| RU | 2019 | RU 2018127153 A | Method of treatment of peyronie’s disease, complicated by erectile dysfunction | FederalnoeGosudarstvennoeByudzhetnoeUchrezhdenieNovosibirskijNauchnoIssledovatelskijInstitut |
| US | 2018 | US 201715618751 A | Methods and devices for treating erectile dysfunction | Ohh Med Medical Ltd. |
| US | 2018 | US 201815982713 A | Methods of treating erectile dysfunction | BiomimetixJvLlc;;Nat Jewish Health |
| KR | 2018 | KR 20170084904 A | Composition for preventing improving or treating erectile dysfunction comprising cavernous derived exosome | UnivInha Res & Business Found;;PostechAcadInd Found |
| RU | 2018 | RU 2016134676 A | Method for treatment of chronic abacterial prostatitis/chronic pelvic pain syndrome, combined with erectile dysfunction | ChurakovAleksejArkadevich |
| US | 2017 | US 201615085304 A | Method for treating erectile dysfunction | Hussein Hany |
| KR | 2017 | KR 20160177086 A | Medical device for erectile dysfunction | Ideafactoryofchoebyongchul Corp |
| RU | 2017 | RU 2016127046 A | Method for treatment of patients with erectile dysfunction | FederalnoeGosudarstvennoeByudzhetnoeObrazovatelnoeUchrezhdenieVysshegoObrazovaniyaSamarskij G |
| RU | 2017 | RU 2016121765 A | Method for erectile dysfunction treatment | Fed GosudarstvennoeAvtonomnoeObrazovatelnoeUchrezhdenieVysshegoObrazovaniyaPervyjMoskovskij G |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Islam, M.M.; Naveen, N.R.; Anitha, P.; Goudanavar, P.S.; Rao, G.S.N.K.; Fattepur, S.; Rahman, M.M.; Shiroorkar, P.N.; Habeebuddin, M.; Meravanige, G.; et al. The Race to Replace PDE5i: Recent Advances and Interventions to Treat or Manage Erectile Dysfunction: Evidence from Patent Landscape (2016–2021). J. Clin. Med. 2022, 11, 3140. https://doi.org/10.3390/jcm11113140
Islam MM, Naveen NR, Anitha P, Goudanavar PS, Rao GSNK, Fattepur S, Rahman MM, Shiroorkar PN, Habeebuddin M, Meravanige G, et al. The Race to Replace PDE5i: Recent Advances and Interventions to Treat or Manage Erectile Dysfunction: Evidence from Patent Landscape (2016–2021). Journal of Clinical Medicine. 2022; 11(11):3140. https://doi.org/10.3390/jcm11113140
Chicago/Turabian StyleIslam, Mohammed Monirul, Nimbagal Raghavendra Naveen, Posina Anitha, Prakash S. Goudanavar, G. S. N. Koteswara Rao, Santosh Fattepur, Muhammad Muhitur Rahman, Predeepkumar Narayanappa Shiroorkar, Mohammed Habeebuddin, Girish Meravanige, and et al. 2022. "The Race to Replace PDE5i: Recent Advances and Interventions to Treat or Manage Erectile Dysfunction: Evidence from Patent Landscape (2016–2021)" Journal of Clinical Medicine 11, no. 11: 3140. https://doi.org/10.3390/jcm11113140
APA StyleIslam, M. M., Naveen, N. R., Anitha, P., Goudanavar, P. S., Rao, G. S. N. K., Fattepur, S., Rahman, M. M., Shiroorkar, P. N., Habeebuddin, M., Meravanige, G., Telsang, M., Nagaraja, S., Asdaq, S. M. B., & Anwer, M. K. (2022). The Race to Replace PDE5i: Recent Advances and Interventions to Treat or Manage Erectile Dysfunction: Evidence from Patent Landscape (2016–2021). Journal of Clinical Medicine, 11(11), 3140. https://doi.org/10.3390/jcm11113140