
Remdesivir in the Treatment of COVID-19: A Propensity Score-Matched Analysis from a Public Hospital in New York City Assessing Renal and Hepatic Safety

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Study Setting, Patient Population
2.2. Data Sources
2.3. Exposure of Interest and Outcomes
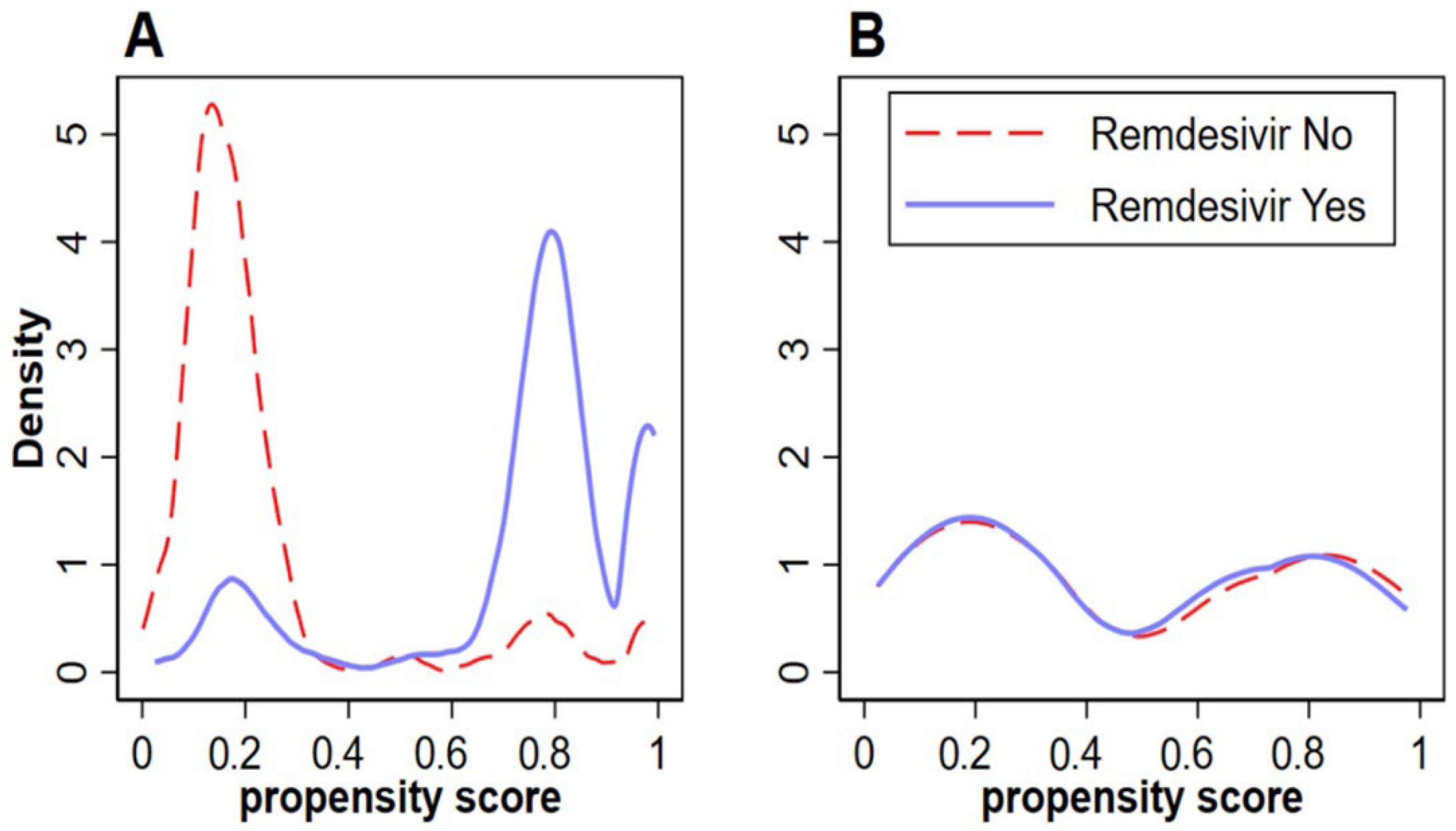
2.4. Statistical Analysis
3. Results
3.1. Baseline Patient Characteristics
3.2. Laboratory Markers on Presentation
3.3. Outcomes
3.4. Logistic Regression Analyses
3.4.1. Acute Kidney Injury
3.4.2. Acute Liver Injury
3.4.3. Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Dos Santos, W.G. Natural history of COVID-19 and current knowledge on treatment therapeutic options. Biomed. Pharmacother. 2020, 129, 110493. [Google Scholar] [CrossRef] [PubMed]
- Santoro, M.G.; Carafoli, E. Remdesivir: From Ebola to COVID-19. Biochem. Biophys. Res. Commun. 2021, 538, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Eastman, R.T.; Roth, J.S.; Brimacombe, K.R.; Simeonov, A.; Shen, M.; Patnaik, S.; Hall, M.D. Remdesivir: A Review of Its Discovery and Development Leading to Emergency Use Authorization for Treatment of COVID-19. ACS Cent. Sci. 2020, 6, 672–683. [Google Scholar] [CrossRef]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the Treatment of COVID-19—Final Report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef] [PubMed]
- FDA. Remdesivir EUA Letter of Authorization. FDA News Release. Available online: https://www.fda.gov/media/137564/download (accessed on 23 March 2022).
- WHO Solidarity Trial Consortium. Repurposed Antiviral Drugs for COVID-19—Interim WHO Solidarity Trial Results. N. Engl. J. Med. 2020, 384, 497–511. [Google Scholar] [CrossRef]
- Kaka, A.S.; MacDonald, R.; Greer, N.; Vela, K.; Duan-Porter, W.; Obley, A.; Wilt, T.J. Major Update: Remdesivir for Adults With COVID-19. Ann. Intern. Med. 2021, 174, 663–672. [Google Scholar] [CrossRef]
- Gottlieb, R.L.; Vaca, C.E.; Paredes, R.; Mera, J.; Webb, B.J.; Perez, G.; Oguchi, G.; Ryan, P.; Nielsen, B.U.; Brown, M.; et al. Early Remdesivir to Prevent Progression to Severe COVID-19 in Outpatients. N. Engl. J. Med. 2021, 386, 305–315. [Google Scholar] [CrossRef]
- Adarsh Bhimraj, R.L.M.; Shumaker, A.H.; Lavergne, V.; Baden, L.; Chi-Chung Cheng, V.; Edwards, K.M.; Gandhi, R.; Gallagher, J.; Muller, W.J.; O’Horo, J.C.; et al. IDSA Guidelines on the Treatment and Management of Patients with COVID-19; Infectious Disease Society of America: Eastville, VA, USA, 2022. [Google Scholar]
- Gérard, A.O.; Laurain, A.; Fresse, A.; Parassol, N.; Muzzone, M.; Rocher, F.; Esnault, V.L.M.; Drici, M.-D. Remdesivir and Acute Renal Failure: A Potential Safety Signal From Disproportionality Analysis of the WHO Safety Database. Clin. Pharmacol. Ther. 2021, 109, 1021–1024. [Google Scholar] [CrossRef]
- Van Laar, S.A.; de Boer, M.G.J.; Gombert-Handoko, K.B.; Guchelaar, H.J.; Zwaveling, J.; group LU-C-r. Liver and kidney function in patients with Covid-19 treated with remdesivir. Br. J. Clin. Pharm. 2021, 87, 4450–4454. [Google Scholar] [CrossRef]
- Velkury Product Information. Committee for Medicinal Products for Human Use. Available online: https://www.ema.europa.eu/en/documents/other/veklury-product-information-approved-chmp-25-june-2020-pending-endorsement-european-commission_en.pdf (accessed on 23 March 2022).
- Adamsick, M.L.; Gandhi, R.G.; Bidell, M.R.; Elshaboury, R.H.; Bhattacharyya, R.P.; Kim, A.Y.; Nigwekar, S.; Rhee, E.P.; Sise, M.E. Remdesivir in Patients with Acute or Chronic Kidney Disease and COVID-19. J. Am. Soc. Nephrol. 2020, 31, 1384–1386. [Google Scholar] [CrossRef]
- Seethapathy, R.; Zhao, S.; Long, J.D.; Strohbehn, I.A.; Sise, M.E. A Propensity Score-Matched Observational Study of Remdesivir in Patients with COVID-19 and Severe Kidney Disease. Kidney360 2022, 3, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Thakare, S.; Gandhi, C.; Modi, T.; Bose, S.; Deb, S.; Saxena, N.; Katyal, A.; Patil, A.; Patil, S.; Pajai, A.; et al. Safety of Remdesivir in Patients With Acute Kidney Injury or CKD. Kidney Int. Rep. 2021, 6, 206–210. [Google Scholar] [CrossRef] [PubMed]
- Wu, B.; Luo, M.; Wu, F.; He, Z.; Li, Y.; Xu, T. Acute Kidney Injury Associated With Remdesivir: A Comprehensive Pharmacovigilance Analysis of COVID-19 Reports in FAERS. Front. Pharm. 2022, 13, 692828. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhang, D.; Du, G.; Du, R.; Zhao, J.; Jin, Y.; Fu, S.; Gao, L.; Cheng, Z.; Lu, Q.; et al. Remdesivir in adults with severe COVID-19: A randomised, double-blind, placebo-controlled, multicentre trial. Lancet 2020, 395, 1569–1578. [Google Scholar] [CrossRef]
- Li, J.; Fan, J.G. Characteristics and Mechanism of Liver Injury in 2019 Coronavirus Disease. J. Clin. Transl. Hepatol. 2020, 8, 13–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourgonje, A.R.; Abdulle, A.E.; Timens, W.; Hillebrands, J.-L.; Navis, G.J.; Gordijn, S.J.; Bolling, M.C.; Dijkstra, G.; Voors, A.A.; Osterhaus, A.D.; et al. Angiotensin-converting enzyme 2 (ACE2), SARS-CoV-2 and the pathophysiology of coronavirus disease 2019 (COVID-19). J. Pathol. 2020, 251, 228–248. [Google Scholar] [CrossRef]
- Testing for SARS-CoV-2 Infection. Available online: https://www.covid19treatmentguidelines.nih.gov/overview/clinical-spectrum/ (accessed on 8 February 2022).
- KDIGO Clinical Practice Guideline for Acute Kidney Injury. Available online: https://kdigo.org/wp-content/uploads/2016/10/KDIGO-2012-AKI-Guideline-English.pdf (accessed on 23 March 2022).
- Yu, Y.-C.; Mao, Y.-M.; Chen, C.-W.; Chen, J.-J.; Chen, J.; Cong, W.-M.; Ding, Y.; Duan, Z.-P.; Fu, Q.-C.; Guo, X.-Y.; et al. CSH guidelines for the diagnosis and treatment of drug-induced liver injury. Hepatol. Int. 2017, 11, 221–241. [Google Scholar] [CrossRef]
- Austin, P.C. An Introduction to Propensity Score Methods for Reducing the Effects of Confounding in Observational Studies. Multivar. Behav. Res. 2011, 46, 399–424. [Google Scholar] [CrossRef] [Green Version]
- Austin, P.C. Optimal caliper widths for propensity-score matching when estimating differences in means and differences in proportions in observational studies. Pharm. Stat. 2011, 10, 150–161. [Google Scholar] [CrossRef] [Green Version]
- Imai, K.; King, G.; Stuart, E.A. Misunderstandings between experimentalists and observationalists about causal inference. J. R. Stat. Soc. Ser. A (Stat. Soc.) 2008, 171, 481–502. [Google Scholar] [CrossRef] [Green Version]
- Leuven, E.; Sianesi, B. PSMATCH2, Stata Module to Perform Full Mahalanobis and Propensity Score Matching, Common Support Graphing, and Covariate Imbalance Testing; Boston College Department of Economics: Chestnut Hill, MA, USA, 2018. [Google Scholar]
- Chan, L.; Chaudhary, K.; Saha, A.; Chauhan, K.; Vaid, A.; Zhao, S.; Paranjpe, I.; Somani, S.; Richter, F.; Miotto, R.; et al. AKI in Hospitalized Patients with COVID-19. J. Am. Soc. Nephrol. 2021, 32, 151–160. [Google Scholar] [CrossRef] [PubMed]
- Zaim, S.; Chong, J.H.; Sankaranarayanan, V.; Harky, A. COVID-19 and Multiorgan Response. Curr. Probl. Cardiol. 2020, 45, 100618. [Google Scholar] [CrossRef] [PubMed]
- Thakur, V.; Ratho, R.K.; Kumar, P.; Bhatia, S.K.; Bora, I.; Mohi, G.K.; Saxena, S.K.; Devi, M.; Yadav, D.; Mehariya, S. Multi-Organ Involvement in COVID-19: Beyond Pulmonary Manifestations. J. Clin. Med. 2021, 10, 446. [Google Scholar] [CrossRef] [PubMed]
- Su, H.; Yang, M.; Wan, C.; Yi, L.X.; Tang, F.; Zhu, H.Y.; Yi, F.; Yang, H.C.; Fogo, A.B.; Nie, X.; et al. Renal histopathological analysis of 26 postmortem findings of patients with COVID-19 in China. Kidney Int. 2020, 98, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Diao, B.; Wang, C.; Wang, R.; Feng, Z.; Tan, Y.; Wang, H.; Wang, C.; Liu, L.; Liu, Y.; Liu, Y.; et al. Human Kidney is a Target for Novel Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection. Nat. Commun. 2021, 12, 2506. [Google Scholar] [CrossRef] [PubMed]
- Yin, L.; Zhao, H.; Zhang, H.; Li, Y.; Dong, Y.; Ju, H.; Kong, F.; Zhao, S. Remdesivir Alleviates Acute Kidney Injury by Inhibiting the Activation of NLRP3 Inflammasome. Front. Immunol. 2021, 12, 1790. [Google Scholar] [CrossRef]
- Ogbuagu, O.; Tashima, K.T.; Günthard, H.F.; McPhail, M.; Sanyal, A.J.; Elboudwarej, E.; Tian, Y.H.; Telep, L.H.; Tan, S.K.; Chokkalingam, A.P.; et al. Acute kidney injury in patients with moderate COVID-19 treated with remdesivir versus SoC. Top. Antivir. Med. 2021, 29, 140. [Google Scholar]
- Chai, X.; Hu, L.; Zhang, Y.; Han, W.; Lu, Z.; Ke, A.; Zhou, J.; Shi, G.; Fang, N.; Fan, J.; et al. Specific ACE2 Expression in Cholangiocytes May Cause Liver Damage After 2019-nCoV Infection. bioRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- The RECOVERY Collaborative Group. Dexamethasone in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2020, 384, 693–704. [Google Scholar] [CrossRef]
- Leisman, D.E. Ten Pearls and Pitfalls of Propensity Scores in Critical Care Research: A Guide for Clinicians and Researchers. Crit. Care. Med. 2019, 47, 176–185. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Before Matching | After Matching without Replacement | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Remdesivir | Remdesivir | |||||||||
| Total | No | Yes | Total | No | Yes | |||||
| n = 927 | n = 500 | n = 427 | p-Value | SMD | n = 248 | n = 124 | n = 124 | p-Value | SMD | |
| Gender—n (%) | 0.285 | 0.070 | 0.525 | 0.080 | ||||||
| Male | 447 (48.2) | 233 (46.6) | 214 (50.1) | 127 (51.2) | 61 (49.2) | 66 (53.2) | ||||
| Female | 480 (51.8) | 267 (53.4) | 213 (49.9) | 121 (48.8) | 63 (50.8) | 58 (46.8) | ||||
| Age—median (IQR) | 61.0 (47.0–73.0) | 59.0 (39.5–73.0) | 63.0 (53.0–73.0) | <0.001 | 0.304 | 62.00 (50.5–73.5) | 64.50 (51.0–74.0) | 62.00 (49.0–72.5) | 0.569 | 0.072 |
| Age Category—n (%) | <0.001 | 0.249 | 0.801 | 0.075 | ||||||
| 18–44 | 195 (21.0) | 148 (29.6) | 47 (11.0) | 40 (16.1) | 19 (15.3) | 21 (16.9) | ||||
| 45–54 | 129 (13.9) | 55 (11.0) | 74 (17.3) | 42 (16.9) | 21 (16.9) | 21 (16.9) | ||||
| 55–64 | 198 (21.4) | 93 (18.6) | 105 (24.6) | 50 (20.2) | 22 (17.7) | 28 (22.6) | ||||
| 65–74 | 203 (21.9) | 91 (18.2) | 112 (26.2) | 61 (24.6) | 34 (27.4) | 27 (21.8) | ||||
| ≥75 | 202 (21.8) | 113 (22.6) | 89 (20.8) | 55 (22.2) | 28 (22.6) | 27 (21.8) | ||||
| BMI—median (IQR) | 28.51 (24.4–33.5) | 27.46 (23.8–31.9) | 30.02 (25.5–34.5) | <0.001 | 0.365 | 28.19 (24.4–33.7) | 28.09 (25.5–33.5) | 28.75 (23.5–33.8) | 0.871 | 0.021 |
| BMI Category—n (%) | <0.001 | 0.349 | 0.022 | 0.090 | ||||||
| <25 | 259 (28.3) | 165 (33.7) | 94 (22.1) | 64 (25.8) | 25 (20.2) | 39 (31.5) | ||||
| 25–29.9 | 273 (29.8) | 158 (32.2) | 115 (27.0) | 83 (33.5) | 51 (41.1) | 32 (25.8) | ||||
| ≥30 | 384 (41.9) | 167 (34.1) | 217 (50.9) | 101 (40.7) | 48 (38.7) | 53 (42.7) | ||||
| HTN—n (%) | <0.001 | 0.267 | 0.609 | 0.064 | ||||||
| No | 400 (43.2) | 246 (49.2) | 154 (36.1) | 110 (44.4) | 53 (42.7) | 57 (46.0) | ||||
| Yes | 527 (56.9) | 254 (50.8) | 273 (63.9) | 138 (55.7) | 71 (57.3) | 67 (54.0) | ||||
| HLD—n (%) | 0.582 | 0.036 | 0.780 | 0.035 | ||||||
| No | 681 (73.5) | 371 (74.2) | 310 (72.6) | 176 (80.0) | 89 (71.8) | 87 (70.2) | ||||
| Yes | 246 (26.5) | 129 (25.8) | 117 (27.4) | 72 (29.0) | 35 (28.2) | 37 (29.8) | ||||
| DM—n (%) | 0.004 | 0.188 | 0.372 | 0.113 | ||||||
| No | 567 (61.2) | 327 (65.4) | 240 (56.2) | 135 (54.4) | 64 (51.6) | 71 (57.3) | ||||
| Yes | 360 (38.8) | 173 (34.6) | 187 (43.8) | 113 (45.6) | 60 (48.4) | 53 (42.7) | ||||
| CAD—n (%) | 0.926 | 0.006 | 0.718 | 0.045 | ||||||
| No | 834 (90.1) | 449 (90.0) | 385 (90.2) | 212 (85.5) | 107 (86.3) | 105 (84.7) | ||||
| Yes | 92 (9.9) | 50 (10.0) | 42 (9.8) | 36 (14.5) | 17 (13.7) | 19 (15.3) | ||||
| CHF—n (%) | 0.518 | 0.042 | 1.000 | 0.000 | ||||||
| No | 823 (88.8) | 447 (89.4) | 376 (88.1) | 214 (86.3) | 107 (86.3) | 107 (86.3) | ||||
| Yes | 104 (11.2) | 53 (10.6) | 51 (11.9) | 34 (13.7) | 17 (13.7) | 17 (13.7) | ||||
| Stroke—n (%) | 0.052 | 0.128 | 0.527 | 0.080 | ||||||
| No | 846 (91.3) | 448 (89.6) | 398 (93.2) | 223 (89.9) | 113 (91.1) | 110 (88.7) | ||||
| Yes | 81 (8.7) | 52 (10.4) | 29 (6.8) | 25 (10.1) | 11 (8.9) | 14 (11.3) | ||||
| CKD—n (%) | 0.006 | 0.133 | 0.040 | 0.088 | ||||||
| No | 809 (87.5) | 433 (87.0) | 376 (88.1) | 199 (80.2) | 103 (83.1) | 96 (77.4) | ||||
| IIIA | 53 (5.7) | 20 (4.0) | 33 (7.7) | 22 (8.9) | 5 (4.0) | 17 (13.7) | ||||
| IIIB | 25 (2.7) | 16 (3.2) | 9 (2.1) | 10 (4.0) | 4 (3.2) | 6 (4.8) | ||||
| IV | 11 (1.2) | 9 (1.8) | 2 (0.5) | 4 (1.6) | 2 (1.6) | 2 (1.6) | ||||
| V | 18 (2.0) | 15 (3.0) | 3 (0.7) | 11 (4.4) | 9 (7.3) | 2 (1.6) | ||||
| ESRD with HD—n (%) | 9 (1.0) | 5 (1.0) | 4 (0.9) | 2 (0.8) | 1 (0.8) | 1 (0.8) | ||||
| Chronic liver disease—n (%) | 0.113 | 0.110 | 1.000 | 0.000 | ||||||
| No | 897 (97.0) | 477 (95.8) | 420 (98.4) | 240 (96.8) | 120 (96.8) | 120 (96.8) | ||||
| Alcoholic hepatitis | 25 (2.7) | 19 (3.8) | 6 (1.4) | 8 (3.2) | 4 (3.2) | 4 (3.2) | ||||
| HepB | 1 (0.1) | 1 (0.2) | 0 (0.0) | |||||||
| HepC | 2 (0.2) | 1 (0.2) | 1 (0.2) | |||||||
| Cirrhosis—n (%) | 0.123 | 0.129 | 0.845 | 0.038 | ||||||
| No | 911 (98.4) | 487 (97.6) | 424 (99.3) | 243 (98.0) | 121 (97.6) | 122 (98.4) | ||||
| Compensated | 10 (1.1) | 8 (1.6) | 2 (0.5) | 3 (1.2) | 2 (1.6) | 1 (0.8) | ||||
| Decompensated | 5 (0.5) | 4 (0.8) | 1 (0.2) | 2 (0.8) | 1 (0.8) | 1 (0.8) | ||||
| Chronic alcohol use disorder—n (%) | 0.002 | 0.236 | 0.485 | 0.021 | ||||||
| No | 882 (95.4) | 464 (93.2) | 418 (97.9) | 234 (94.4) | 118 (95.2) | 116 (93.6) | ||||
| In remission | 22 (2.4) | 16 (3.2) | 6 (1.4) | 7 (2.8) | 2 (1.6) | 5 (4.0) | ||||
| Active | 21 (2.3) | 18 (3.6) | 3 (0.7) | 7 (2.8) | 4 (3.2) | 3 (2.4) | ||||
| COVID-19 severity on admission—n (%) | <0.001 | 1.655 | 0.456 | 0.057 | ||||||
| Moderate | 486 (52.5) | 428 (85.8) | 58 (13.6) | 117 (47.2) | 59 (47.6) | 58 (46.8) | ||||
| Severe | 331 (35.8) | 50 (10.0) | 281 (65.8) | 97 (39.1) | 45 (36.3) | 52 (41.9) | ||||
| Critical | 109 (11.8) | 21 (4.2) | 88 (20.6) | 34 (13.7) | 20 (16.1) | 14 (11.3) | ||||
| Laboratory Tests | Before Matching | After Matching without Replacement | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Remdesivir | Remdesivir | |||||||||
| Total—n (%) | No—n (%) | Yes—n (%) | Total—n (%) | No—n (%) | Yes—n (%) | |||||
| n = 927 | n = 500 | n = 427 | p-Value | SMD | n = 248 | n = 124 | n = 124 | p-Value | SMD | |
| BUN (mg/dL)—median (IQR) | 15.00 (11.0–24.0) | 14.00 (10.0–22.0) | 15.00 (11.0–25.0) | 0.081 | 0.115 | 16.00 (11.0–29.0) | 16.00 (11.0–33.0) | 15.00 (11.0–27.0) | 0.200 | 0.164 |
| Cr (mg/dL)—median (IQR) | 1.00 (0.8–1.3) | 0.90 (0.7–1.3) | 1.00 (0.8–1.3) | 0.782 | 0.018 | 1.10 (0.8–1.6) | 1.10 (0.8–1.6) | 1.00 (0.8–1.5) | 0.157 | 0.181 |
| Albumin (g/dL)—median (IQR) | 3.80 (3.5–4.2) | 3.90 (3.5–4.3) | 3.80 (3.5–4.0) | 0.005 | 0.189 | 3.80 (3.3–4.1) | 3.70 (3.2–4.1) | 3.80 (3.5–4.1) | 0.559 | 0.075 |
| Total Bilirubin (mg/dL)—median (IQR) | 0.40 (0.3–0.6) | 0.40 (0.3–0.7) | 0.40 (0.3–0.5) | 0.002 | 0.214 | 0.40 (0.3–0.6) | 0.40 (0.3–0.7) | 0.30 (0.2–0.5) | 0.023 | 0.297 |
| ALP (U/L)—median (IQR) | 79.00 (62.0–109.0) | 85.00 (64.0–119.0) | 75.00 (58.0–97.0) | 0.002 | 0.214 | 79.00 (60.0–111.0) | 82.00 (61.0–133.0) | 74.00 (58.0–93.0) | 0.007 | 0.359 |
| AST (U/L)—median (IQR) | 34.00 (24.0–60.0) | 29.00 (21.0–49.0) | 42.00 (28.0–64.0) | 0.251 | 0.079 | 38.00 (27.0–63.0) | 34.00 (25.0–62.0) | 42.00 (30.0–63.0) | 0.029 | 0.281 |
| ALT (U/L)—median (IQR) | 26.00 (16.0–45.5) | 23.50 (14.0–42.0) | 28.00 (19.0–48.0) | 0.256 | 0.078 | 29.00 (18.0–53.0) | 29.50 (17.0–67.0) | 27.00 (20.0–46.0) | 0.019 | 0.303 |
| Outcomes | Before Matching | After Matching without Replacement | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Remdesivir | Remdesivir | |||||||||
| Total—n (%) | No—n (%) | Yes—n (%) | Total—n (%) | No—n (%) | Yes– n (%) | |||||
| n = 927 | n = 500 | n = 427 | p-Value | SMD | n = 248 | n = 124 | n = 124 | p-Value | SMD | |
| Intubation—n (%) | <0.001 | 0.373 | 0.078 | 0.22 | ||||||
| No | 809 (87.3) | 465 (93.0) | 344 (80.6) | 210 (84.7) | 100 (80.7) | 110 (88.7) | ||||
| Yes | 118 (12.7) | 35 (7.0) | 83 (19.4) | 38 (15.3) | 24 (19.4) | 14 (11.3) | ||||
| Admission to ICU—n (%) | <0.001 | 0.451 | 0.548 | 0.08 | ||||||
| No | 748 (80.7) | 444 (88.8) | 304 (71.2) | 190 (76.6) | 93 (75.0) | 97 (78.2) | ||||
| Yes | 179 (19.3) | 56 (11.2) | 123 (28.8) | 58 (23.4) | 31 (25.0) | 27 (21.8) | ||||
| Death—n (%) | <0.001 | 0.352 | 0.593 | 0.07 | ||||||
| No | 817 (88.1) | 467 (93.4) | 350 (82.0) | 211 (85.1) | 104 (83.9) | 107 (86.3) | ||||
| Yes | 110 (11.9) | 33 (6.6) | 77 (18.0) | 37 (14.9) | 20 (16.1) | 17 (13.7) | ||||
| AKI during hospitalization | 0.056 | 0.125 | 0.042 | 0.26 | ||||||
| No | 805 (86.8) | 444 (88.8) | 361 (84.5) | 206 (83.1) | 97 (78.2) | 109 (87.9) | ||||
| Yes | 122 (13.2) | 56 (11.2) | 66 (15.5) | 42 (16.9) | 27 (21.8) | 15 (12.1) | ||||
| New dialysis during hospitalization | 0.055 | 0.123 | 0.156 | 0.180 | ||||||
| No | 918 (99.0) | 498 (99.6) | 420 (98.4) | 246 (99.2) | 122 (98.4) | 124 (100.0) | ||||
| Yes | 9 (1.0) | 2 (0.4) | 7 (1.6) | 2 (0.8) | 2 (1.6) | 0 (0.0) | ||||
| ALI during hospitalization | 0.150 | 0.094 | 0.067 | 0.23 | ||||||
| No | 851 (91.8) | 465 (93.0) | 386 (90.4) | 221 (89.1) | 106 (85.5) | 115 (92.7) | ||||
| Yes | 76 (8.2) | 35 (7.0) | 41 (9.6) | 27 (10.9) | 18 (14.5) | 9 (7.3) | ||||
| Before Matching | After Matching without Replacement | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Remdesivir | Remdesivir | |||||||||
| Total—n (%) | No—n (%) | Yes—n (%) | Total—n (%) | No—n (%) | Yes—n (%) | |||||
| Patients with CKD | n = 107 | n = 60 | n = 47 | p-value | SMD | n = 37 | n = 15 | n = 22 | p-value | SMD |
| AKI during hospitalization | 0.141 | 0.291 | 0.967 | 0.013 | ||||||
| No | 84 (78.5) | 44 (73.3) | 40 (85.1) | 27 (73.0) | 11 (73.3) | 16 (72.4) | ||||
| Yes | 23 (21.5) | 16 (26.7) | 7 (14.9) | 10 (27.0) | 4 (26.7) | 6 (27.3) | ||||
| Patients with Chronic Liver Disease | n = 28 | n = 21 | n = 7 | n = 8 | n = 4 | n = 4 | ||||
| ALI during hospitalization | 0.111 | 0.872 | 0.285 | 0.707 | ||||||
| No | 22 (78.6) | 15 (71.4) | 7 (100.0) | 7 (87.5) | 3 (75.0) | 4 (100.0) | ||||
| Yes | 6 (21.4) | 6 (28.6) | 0 (0.0) | 1 (12.5) | 1 (25.0) | 0 (0.0) | ||||
| Outcomes | Before Matching | After Matching without Replacement | ||
|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | |
| n = 926 | n = 248 | |||
| OR, 95% CI, p-Value | OR, 95% CI, p-Value | OR, 95% CI, p-Value | OR, 95% CI, p-Value | |
| Female | 0.73 (0.50–1.08) p = 0.113 | 0.84 (0.43–1.64) p = 0.614 | ||
| Age Category | 1.57 (1.36–1.80) p < 0.001 | 1.36 (1.15–1.62) p < 0.001 | 1.42 (1.09–1.85) p = 0.009 | 1.26 (0.93–1.69) p = 0.131 |
| BMI | 1.02 (0.99–1.04) p = 0.134 | 1.02 (0.98–1.06) p = 0.290 | ||
| Hypertension | 2.88 (1.85–4.50) p < 0.001 | 1.82 (1.08–3.07) p = 0.026 | 2.27 (1.10–4.68) p = 0.027 | 1.67 (0.79–3.50) p = 0.177 |
| Hyperlipidemia | 1.48 (0.99–2.23) p = 0.059 | 1.45 (0.72–2.93) p = 0.298 | ||
| Diabetes | 1.97 (1.34–2.89) p = 0.001 | 1.09 (0.69–1.74) p = 0.712 | 1.75 (0.90–3.43) p = 0.102 | |
| CAD | 1.09 (0.59–2.04) p = 0.775 | 1.50 (0.63–3.57) p = 0.364 | ||
| CHF | 2.52 (1.54–4.13) p < 0.001 | 1.44 (0.84–2.46) p = 0.181 | 2.82 (1.25–6.38) p = 0.013 | 1.59 (0.67–3.78) p = 0.297 |
| Stroke | 1.29 (0.69–2.42) p = 0.422 | 1.26 (0.44–3.57) p = 0.668 | ||
| CKD or ESRD | 1.17 (1.00–1.37) p = 0.051 | 1.57 (0.72–3.40) p = 0.254 | ||
| Chronic liver disease | 1.03 (0.60–1.78) p = 0.906 | 3.09 (0.71–13.51) p = 0.134 | ||
| Cirrhosis | 1.40 (0.63–3.08) p = 0.410 | 2.32 (0.57–9.46) p = 0.241 | ||
| COVID-19 severity on admission | 2.86 (2.14–3.81) p < 0.001 | 3.69 (2.61–5.21) p < 0.001 | 3.28 (1.94–5.53) p < 0.001 | 2.99 (1.76–5.09) p < 0.001 |
| Remdesivir | 1.45 (0.99–2.12) p = 0.057 | 0.40 (0.24–0.67) p = 0.000 | 0.49 (0.25–0.98) p = 0.045 | 0.48 (0.23–1.01) p = 0.054 |
| Outcomes | Before Matching | After Matching without Replacement | ||
|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | |
| n = 924 | n = 248 | |||
| OR, 95% CI, p-Value | OR, 95% CI, p-Value | OR, 95% CI, p-Value | OR, 95% CI, p-Value | |
| Female sex | 0.45 (0.28–0.74) p = 0.002 | 0.58 (0.35–0.98) p = 0.041 | 0.69 (0.31–1.56) p = 0.378 | |
| Age Category | 0.90 (0.78–1.04) p = 0.151 | 0.84 (0.64–1.09) p = 0.191 | ||
| BMI | 1.01 (0.98–1.04) p = 0.446 | 1.00 (0.96–1.04) p = 0.963 | ||
| Hypertension | 0.52 (0.33–0.84) p = 0.008 | 0.57 (0.32–1.02) p = 0.060 | 0.60 (0.27–1.35) p = 0.219 | |
| Hyperlipidemia | 0.44 (0.23–0.86) p = 0.015 | 0.66 (0.32–1.35) p = 0.255 | 0.84 (0.34–2.09) p = 0.707 | |
| Diabetes | 0.58 (0.34–0.97) p = 0.039 | 0.67 (0.36–1.23) p = 0.199 | 0.56 (0.24–1.31) p = 0.182 | |
| CAD | 0.48 (0.17–1.35) p = 0.164 | 0.71 (0.20–2.51) p = 0.597 | ||
| CHF | 0.66 (0.28–1.56) p = 0.341 | 0.47 (0.11–2.10) p = 0.324 | ||
| Stroke | 1.07 (0.47–2.40) p = 0.879 | 1.66 (0.52–5.26) p = 0.392 | ||
| CKD or ESRD | 0.69 (0.31–1.54) p = 0.363 | 0.91 (0.33–2.56) p = 0.864 | ||
| Chronic liver disease | 1.49 (0.89–2.51) p = 0.131 | 1.18 (0.14–9.98) p = 0.882 | ||
| Cirrhosis | 0.69 (0.17–2.88) p = 0.613 | cannot be estimated | ||
| COVID-19 severity on admission | 2.19 (1.57–3.05) p < 0.001 | 2.75 (1.81–4.16) p < 0.001 | 2.20 (1.23–3.92) p = 0.008 | 2.16 (1.22–3.82) p = 0.008 |
| Remdesivir | 1.41 (0.88–2.26) p = 0.152 | 0.68 (0.35–1.30) p = 0.241 | 0.46 (0.20–1.07) p = 0.072 | 0.47 (0.20–1.11) p = 0.087 |
| Outcomes | Before Matching | After Matching without Replacement | ||
|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | |
| n = 924 | n = 248 | |||
| OR, 95% CI, p-Value | OR, 95% CI, p-Value | OR, 95% CI, p-Value | OR, 95% CI, p-Value | |
| Female sex | 0.72 (0.48–1.07) p = 0.107 | 0.87 (0.43–1.76) p = 0.708 | ||
| Age Category | 1.49 (1.28–1.72) p < 0.001 | 1.36 (1.11–1.67) p = 0.003 | 1.22 (0.94–1.59) p = 0.130 | |
| BMI | 1.01 (0.99–1.04) p = 0.295 | 1.02 (0.97–1.06) p = 0.484 | ||
| Hypertension | 1.32 (0.87–1.99) p = 0.186 | 1.20 (0.59–2.45) p = 0.614 | ||
| Hyperlipidemia | 1.04 (0.67–1.63) p = 0.852 | 1.40 (0.67–2.93) p = 0.378 | ||
| Diabetes | 1.20 (0.80–1.80) p = 0.373 | 1.31 (0.65–2.65) p = 0.445 | ||
| CAD | 0.90 (0.45–1.78) p = 0.753 | 0.91 (0.33–2.51) p = 0.851 | ||
| CHF | 2.09 (1.23–3.54) p = 0.006 | 1.17 (0.62–2.22) p = 0.627 | 1.96 (0.81–4.76) p = 0.136 | |
| Stroke | 1.80 (0.99–3.27) p = 0.056 | 4.83 (1.97–11.87) p = 0.001 | 3.34 (0.94–11.80) p = 0.061 | |
| CKD or ESRD | 1.29 (1.10–1.51) p = 0.001 | 1.29 (1.08–1.54) p = 0.006 | 1.25 (0.98–1.60) p = 0.071 | |
| Chronic liver disease | 0.96 (0.52–1.76) p = 0.889 | 3.64 (0.83–15.96) p = 0.087 | ||
| Cirrhosis | 0.88 (0.32–2.42) p = 0.799 | 1.69 (0.48–5.95) p = 0.410 | ||
| COVID-19 severity on admission | 8.23 (5.46–12.43) p < 0.001 | 9.25 (5.99–14.29) p < 0.001 | 10.89 (4.50–26.36) p < 0.001 | 10.24 (4.14–25.31) p < 0.001 |
| Remdesivir | 3.11 (2.02–4.79) p < 0.001 | 0.57 (0.32–1.01) p = 0.053 | 0.83 (0.41–1.67) p = 0.594 | 0.97 (0.42–2.22) p = 0.941 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, H.; Palaiodimos, L.; Berto, C.G.; Tedunjaiye, O.; Malik, P.; Nagraj, S.; Choi, H.; Hti Lar Seng, N.S.; Kladas, M.; Kharawala, A.; et al. Remdesivir in the Treatment of COVID-19: A Propensity Score-Matched Analysis from a Public Hospital in New York City Assessing Renal and Hepatic Safety. J. Clin. Med. 2022, 11, 3132. https://doi.org/10.3390/jcm11113132
Lim H, Palaiodimos L, Berto CG, Tedunjaiye O, Malik P, Nagraj S, Choi H, Hti Lar Seng NS, Kladas M, Kharawala A, et al. Remdesivir in the Treatment of COVID-19: A Propensity Score-Matched Analysis from a Public Hospital in New York City Assessing Renal and Hepatic Safety. Journal of Clinical Medicine. 2022; 11(11):3132. https://doi.org/10.3390/jcm11113132
Chicago/Turabian StyleLim, Hyomin, Leonidas Palaiodimos, Cesar G. Berto, Oluwatitomi Tedunjaiye, Paras Malik, Sanjana Nagraj, Hansol Choi, Nang San Hti Lar Seng, Michail Kladas, Amrin Kharawala, and et al. 2022. "Remdesivir in the Treatment of COVID-19: A Propensity Score-Matched Analysis from a Public Hospital in New York City Assessing Renal and Hepatic Safety" Journal of Clinical Medicine 11, no. 11: 3132. https://doi.org/10.3390/jcm11113132
APA StyleLim, H., Palaiodimos, L., Berto, C. G., Tedunjaiye, O., Malik, P., Nagraj, S., Choi, H., Hti Lar Seng, N. S., Kladas, M., Kharawala, A., Karamanis, D., Varma, N., & Anjali, A. (2022). Remdesivir in the Treatment of COVID-19: A Propensity Score-Matched Analysis from a Public Hospital in New York City Assessing Renal and Hepatic Safety. Journal of Clinical Medicine, 11(11), 3132. https://doi.org/10.3390/jcm11113132