
Transcatheter Treatment of Mitral Regurgitation

 , , ,
, , ,  ,
,  ,
,
Abstract
1. Introduction
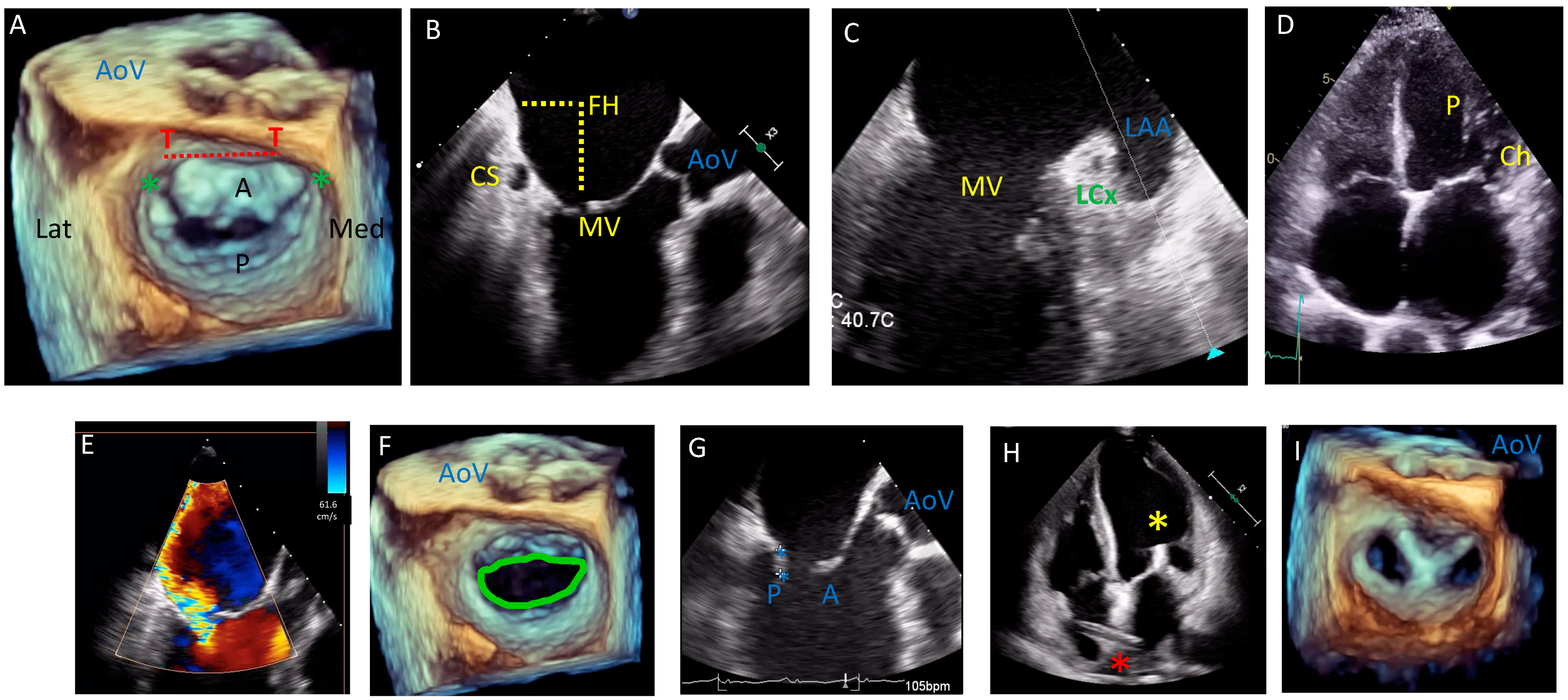
2. Anatomical and Imaging Considerations
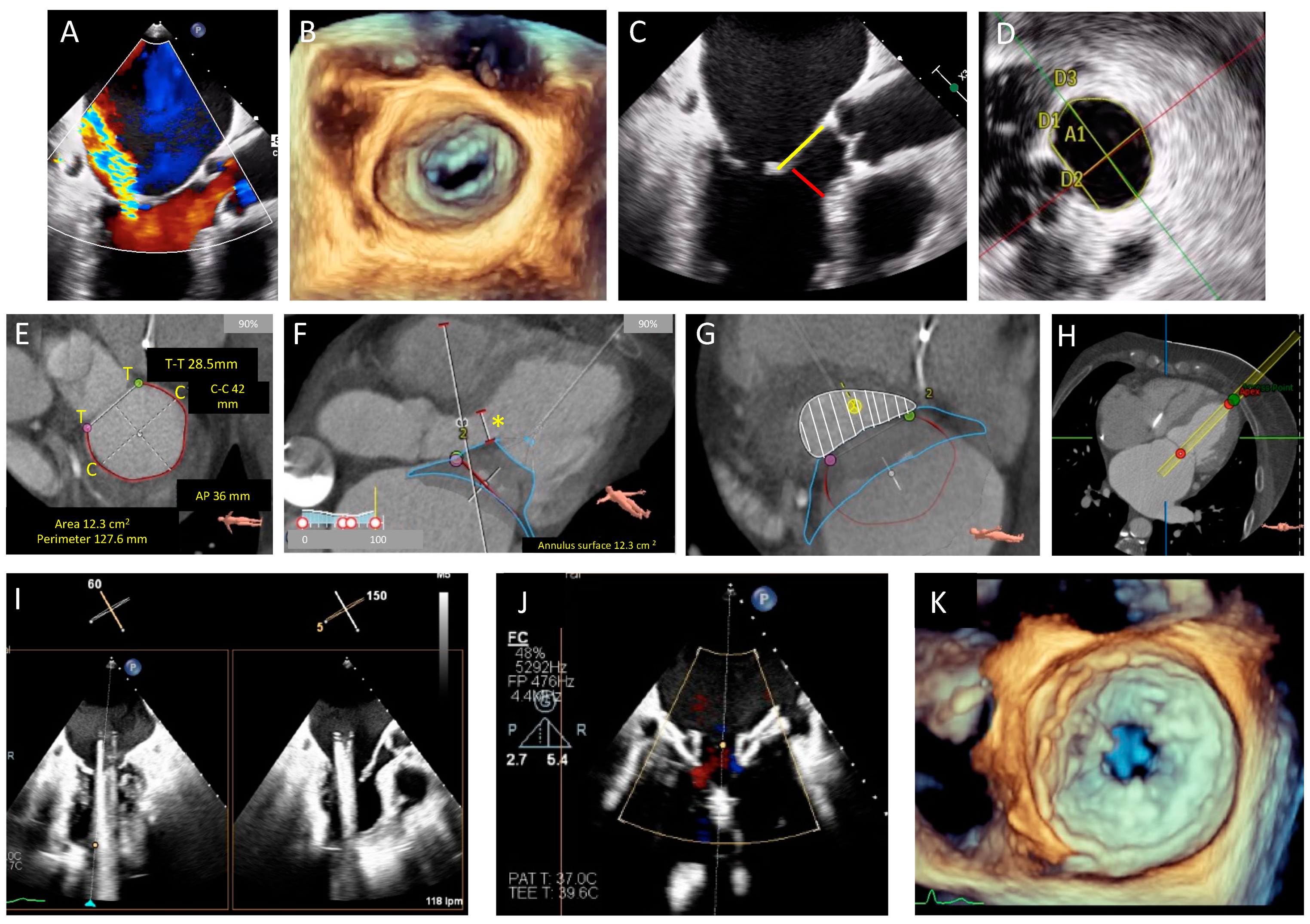
3. Echocardiography
4. Multidetector Row Computed Tomography (MDCT)
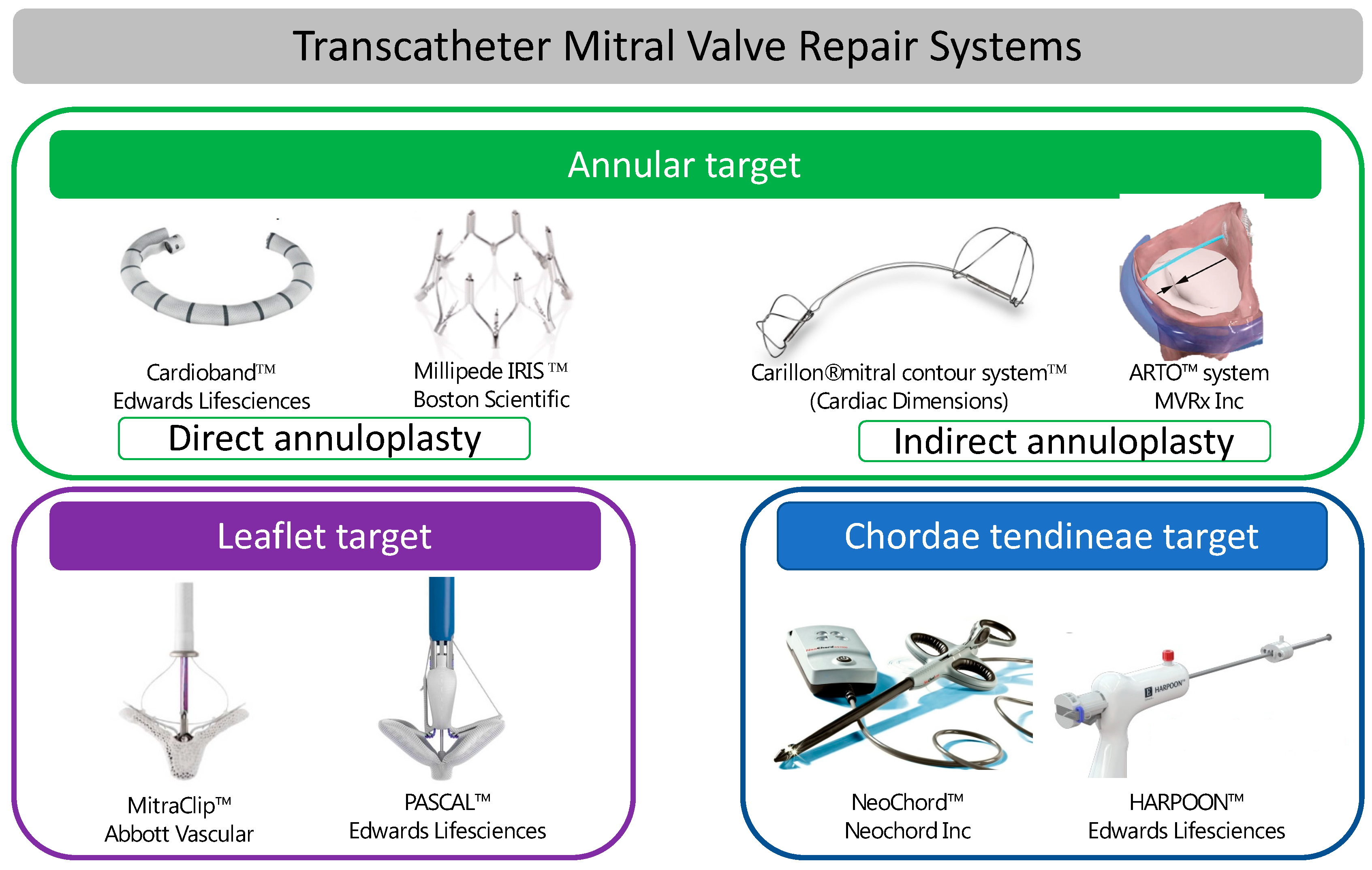
5. Transcatheter Mitral Valve Repair
Devices Aimed at Modifying the MV Annulus
6. Direct Annuloplasty Transcatheter Systems
7. Indirect Annuloplasty Transcatheter Systems
7.1. Devices Targeting the MV Leaflets
7.2. Devices Targeting the Subvalvular Apparatus
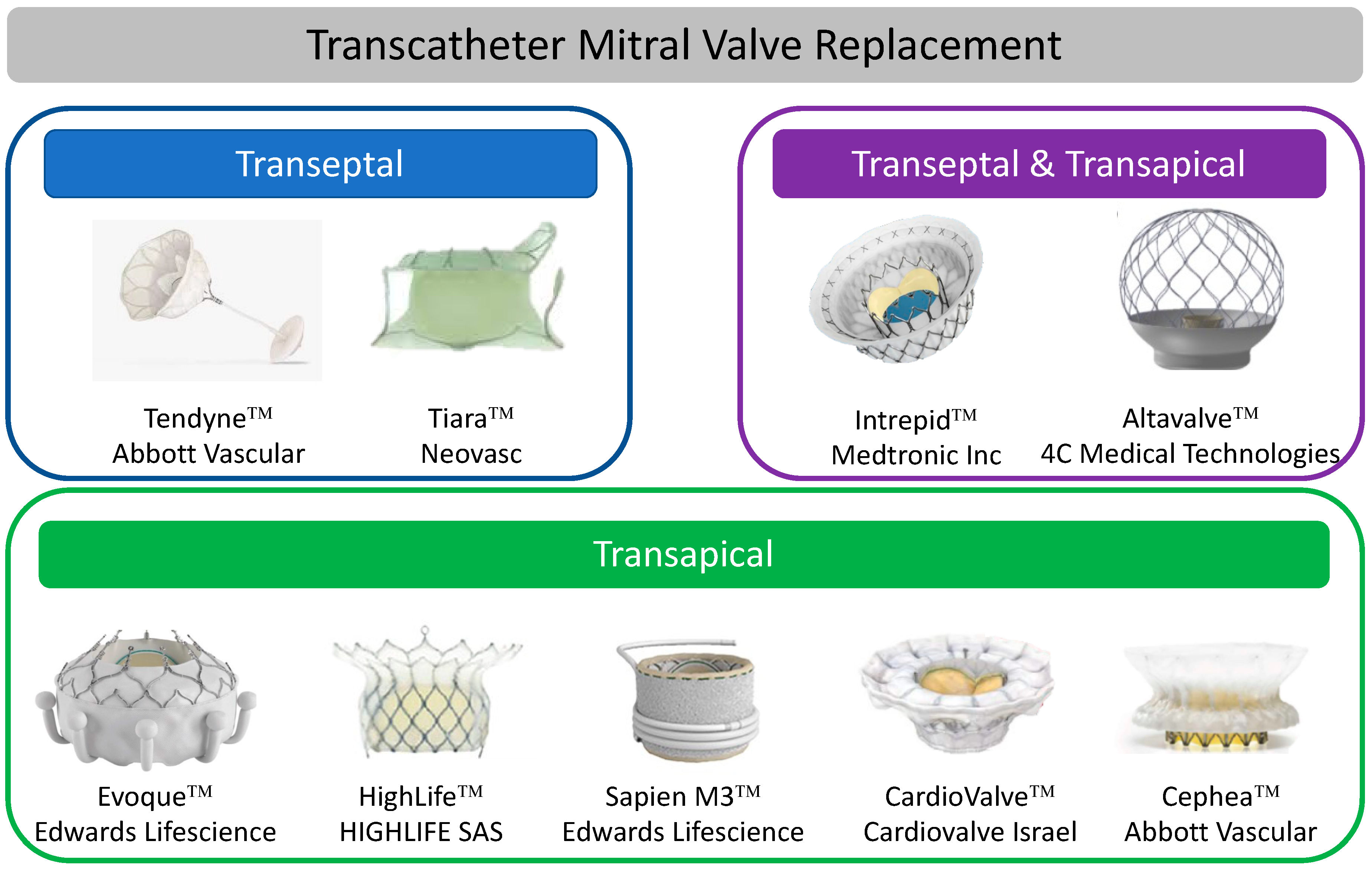
8. Transcatheter Mitral Valve Replacement (TMVR)
9. Transapical TMVR Systems
10. Transeptal TMVR Systems
11. Future Directions
12. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Iung, B.; Delgado, V.; Rosenhek, R.; Price, S.; Prendergast, B.; Wendler, O.; De Bonis, M.; Tribouilloy, C.; Evangelista, A.; Bogachev-Prokophiev, A.; et al. Contemporary Presentation and Management of Valvular Heart Disease: The EURObservational Research Programme Valvular Heart Disease II Survey. Circulation 2019, 140, 1156–1169. [Google Scholar] [CrossRef] [PubMed]
- Cahill, T.J.; Prothero, A.; Wilson, J.; Kennedy, A.; Brubert, J.; Masters, M.; Newton, J.D.; Dawkins, S.; Enriquez-Sarano, M.; Prendergast, B.D.; et al. Community prevalence, mechanisms and outcome of mitral or tricuspid regurgitation. Heart 2021, 107, 1003–1009. [Google Scholar] [CrossRef] [PubMed]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2021, 43, 561–632. [Google Scholar] [CrossRef] [PubMed]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P.; Gentile, F., 3rd; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients with Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021, 143, e72–e227. [Google Scholar] [PubMed]
- Mack, M.; Carroll, J.D.; Thourani, V.; Vemulapalli, S.; Squiers, J.; Manandhar, P.; Deeb, G.M.; Batchelor, W.; Herrmann, H.C.; Cohen, D.J.; et al. Transcatheter Mitral Valve Therapy in the United States: A Report From the STS-ACC TVT Registry. J. Am. Coll. Cardiol. 2021, 78, 2326–2353. [Google Scholar] [CrossRef] [PubMed]
- Gheorghe, L.L.; Mobasseri, S.; Agricola, E.; Wang, D.D.; Milla, F.; Swaans, M.; Pandis, D.; Adams, D.H.; Yadav, P.; Sievert, H.; et al. Imaging for Native Mitral Valve Surgical and Transcatheter Interventions. JACC Cardiovasc. Imaging 2021, 14, 112–127. [Google Scholar] [CrossRef] [PubMed]
- Bax, J.J.; Debonnaire, P.; Lancellotti, P.; Ajmone Marsan, N.; Tops, L.F.; Min, J.K.; Piazza, N.; Leipsic, J.; Hahn, R.T.; Delgado, V. Transcatheter Interventions for Mitral Regurgitation: Multimodality Imaging for Patient Selection and Procedural Guidance. JACC Cardiovasc. Imaging 2019, 12, 2029–2048. [Google Scholar] [CrossRef]
- Silbiger, J.J.; Bazaz, R. Contemporary insights into the functional anatomy of the mitral valve. Am. Heart J. 2009, 158, 887–895. [Google Scholar] [CrossRef]
- Wunderlich, N.C.; Beigel, R.; Ho, S.Y.; Nietlispach, F.; Cheng, R.; Agricola, E.; Siegel, R.J. Imaging for Mitral Interventions: Methods and Efficacy. JACC Cardiovasc. Imaging 2018, 11, 872–901. [Google Scholar] [CrossRef]
- Faletra, F.F.; Pozzoli, A.; Agricola, E.; Guidotti, A.; Biasco, L.; Leo, L.A.; Taramasso, M.; Pasotti, E.; Kuwata, S.; Moccetti, M.; et al. Echocardiographic-fluoroscopic fusion imaging for transcatheter mitral valve repair guidance. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 715–726. [Google Scholar] [CrossRef]
- Yoon, S.H.; Bleiziffer, S.; Latib, A.; Eschenbach, L.; Ancona, M.; Vincent, F.; Kim, W.K.; Unbehaum, A.; Asami, M.; Dhoble, A.; et al. Predictors of Left Ventricular Outflow Tract Obstruction after Transcatheter Mitral Valve Replacement. JACC Cardiovasc Interv. 2019, 12, 182–193. [Google Scholar] [CrossRef] [PubMed]
- Messika-Zeitoun, D.; Nickenig, G.; Latib, A.; Kuck, K.H.; Baldus, S.; Schueler, R.; La Canna, G.; Agricola, E.; Kreidel, F.; Huntgeburth, M.; et al. Transcatheter mitral valve repair for functional mitral regurgitation using the Cardioband system: 1 year outcomes. Eur. Heart J. 2019, 40, 466–472. [Google Scholar] [CrossRef] [PubMed]
- Rogers, J.H.; Boyd, W.D.; Smith, T.W.; Bolling, S.F. Transcatheter Mitral Valve Direct Annuloplasty with the Millipede IRIS Ring. Interv. Cardiol. Clin. 2019, 8, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Schofer, J.; Siminiak, T.; Haude, M.; Herrman, J.P.; Vainer, J.; Wu, J.C.; Levy, W.C.; Mauri, L.; Feldman, T.; Kwong, R.Y.; et al. Percutaneous mitral annuloplasty for functional mitral regurgitation: Results of the CARILLON Mitral Annuloplasty Device European Union Study. Circulation 2009, 120, 326–333. [Google Scholar] [CrossRef]
- Siminiak, T.; Wu, J.C.; Haude, M.; Hoppe, U.C.; Sadowski, J.; Lipiecki, J.; Fajadet, J.; Shah, A.M.; Feldman, T.; Kaye, D.M.; et al. Treatment of functional mitral regurgitation by percutaneous annuloplasty: Results of the TITAN Trial. Eur. J. Heart Fail. 2012, 14, 931–938. [Google Scholar] [CrossRef]
- Lipiecki, J.; Siminiak, T.; Sievert, H.; Muller-Ehmsen, J.; Degen, H.; Wu, J.C.; Schandrin, C.; Kalmucki, P.; Hofmann, I.; Reuter, D.; et al. Coronary sinus-based percutaneous annuloplasty as treatment for functional mitral regurgitation: The TITAN II trial. Open Heart 2016, 3, e000411. [Google Scholar] [CrossRef]
- Witte, K.K.; Lipiecki, J.; Siminiak, T.; Meredith, I.T.; Malkin, C.J.; Goldberg, S.L.; Stark, M.A.; von Bardeleben, R.S.; Cremer, P.C.; Jaber, W.A.; et al. The REDUCE FMR Trial: A Randomized Sham-Controlled Study of Percutaneous Mitral Annuloplasty in Functional Mitral Regurgitation. JACC Heart Fail. 2019, 7, 945–955. [Google Scholar] [CrossRef]
- Lipiecki, J.; Fahrat, H.; Monzy, S.; Caillot, N.; Siminiak, T.; Johnson, T.; Vogt, S.; Stark, M.A.; Goldberg, S.L. Long-term prognosis of patients treated by coronary sinus-based percutaneous annuloplasty: Single centre experience. ESC Heart Fail. 2020, 7, 3329–3335. [Google Scholar] [CrossRef]
- Palacios, I.F.; Condado, J.A.; Brandi, S.; Rodriguez, V.; Bosch, F.; Silva, G.; Low, R.I.; Rogers, J.H. Safety and feasibility of acute percutaneous septal sinus shortening: First-in-human experience. Catheter. Cardiovasc. Interv. 2007, 69, 513–518. [Google Scholar] [CrossRef]
- Patterson, T.; Gregson, J.; Erglis, A.; Joseph, J.; Rajani, R.; Wilson, K.; Prendergast, B.; Worthley, S.; Hildick-Smith, D.; Rafter, T.; et al. Two-year outcomes from the MitrAl ValvE RepaIr Clinical (MAVERIC) trial: A novel percutaneous treatment of functional mitral regurgitation. Eur. J. Heart Fail. 2021, 23, 1775–1783. [Google Scholar] [CrossRef]
- Worthley, S.; Redwood, S.; Hildick-Smith, D.; Rafter, T.; Whelan, A.; De Marco, F.; Horrigan, M.; Delacroix, S.; Gregson, J.; Erglis, A. Transcatheter reshaping of the mitral annulus in patients with functional mitral regurgitation: One-year outcomes of the MAVERIC trial. EuroIntervention 2021, 16, 1106–1113. [Google Scholar] [CrossRef] [PubMed]
- Alfieri, O.; De Bonis, M.; Lapenna, E.; Regesta, T.; Maisano, F.; Torracca, L.; La Canna, G. “Edge-to-edge” repair for anterior mitral leaflet prolapse. Semin. Thorac. Cardiovasc. Surg. 2004, 16, 182–187. [Google Scholar] [CrossRef] [PubMed]
- Feldman, T.; Wasserman, H.S.; Herrmann, H.C.; Gray, W.; Block, P.C.; Whitlow, P.; St Goar, F.; Rodriguez, L.; Silvestry, F.; Schwartz, A.; et al. Percutaneous mitral valve repair using the edge-to-edge technique: Six-month results of the EVEREST Phase I Clinical Trial. J. Am. Coll. Cardiol. 2005, 46, 2134–2140. [Google Scholar] [CrossRef] [PubMed]
- Feldman, T.; Foster, E.; Glower, D.D.; Kar, S.; Rinaldi, M.J.; Fail, P.S.; Smalling, R.W.; Siegel, R.; Rose, G.A.; Engeron, E.; et al. Percutaneous repair or surgery for mitral regurgitation. N. Engl. J. Med. 2011, 364, 1395–1406. [Google Scholar] [CrossRef] [PubMed]
- Mauri, L.; Garg, P.; Massaro, J.M.; Foster, E.; Glower, D.; Mehoudar, P.; Powell, F.; Komtebedde, J.; McDermott, E.; Feldman, T. The EVEREST II Trial: Design and rationale for a randomized study of the evalve mitraclip system compared with mitral valve surgery for mitral regurgitation. Am. Heart J. 2010, 160, 23–29. [Google Scholar] [CrossRef]
- Stone, G.W.; Lindenfeld, J.; Abraham, W.T.; Kar, S.; Lim, D.S.; Mishell, J.M.; Whisenant, B.; Grayburn, P.A.; Rinaldi, M.; Kapadia, S.R.; et al. Transcatheter Mitral-Valve Repair in Patients with Heart Failure. N. Engl. J. Med. 2018, 379, 2307–2318. [Google Scholar] [CrossRef]
- Obadia, J.F.; Messika-Zeitoun, D.; Leurent, G.; Iung, B.; Bonnet, G.; Piriou, N.; Lefevre, T.; Piot, C.; Rouleau, F.; Carrie, D.; et al. Percutaneous Repair or Medical Treatment for Secondary Mitral Regurgitation. N. Engl. J. Med. 2018, 379, 2297–2306. [Google Scholar] [CrossRef]
- Pibarot, P.; Delgado, V.; Bax, J.J. MITRA-FR vs. COAPT: Lessons from two trials with diametrically opposed results. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 620–624. [Google Scholar] [CrossRef]
- Mack, M.J.; Lindenfeld, J.; Abraham, W.T.; Kar, S.; Lim, D.S.; Mishell, J.M.; Whisenant, B.K.; Grayburn, P.A.; Rinaldi, M.J.; Kapadia, S.R.; et al. 3-Year Outcomes of Transcatheter Mitral Valve Repair in Patients with Heart Failure. J. Am. Coll. Cardiol. 2021, 77, 1029–1040. [Google Scholar] [CrossRef]
- Chakravarty, T.; Makar, M.; Patel, D.; Oakley, L.; Yoon, S.H.; Stegic, J.; Singh, S.; Skaf, S.; Nakamura, M.; Makkar, R.R. Transcatheter Edge-to-Edge Mitral Valve Repair with the MitraClip G4 System. JACC Cardiovasc. Interv. 2020, 13, 2402–2414. [Google Scholar] [CrossRef]
- Szerlip, M.; Spargias, K.S.; Makkar, R.; Kar, S.; Kipperman, R.M.; O’Neill, W.W.; Ng, M.K.C.; Smith, R.L.; Fam, N.P.; Rinaldi, M.J.; et al. 2-Year Outcomes for Transcatheter Repair in Patients with Mitral Regurgitation From the CLASP Study. JACC Cardiovasc. Interv. 2021, 14, 1538–1548. [Google Scholar] [CrossRef] [PubMed]
- Seeburger, J.; Rinaldi, M.; Nielsen, S.L.; Salizzoni, S.; Lange, R.; Schoenburg, M.; Alfieri, O.; Borger, M.A.; Mohr, F.W.; Aidietis, A. Off-pump transapical implantation of artificial neo-chordae to correct mitral regurgitation: The TACT Trial (Transapical Artificial Chordae Tendinae) proof of concept. J. Am. Coll. Cardiol. 2014, 63, 914–919. [Google Scholar] [CrossRef] [PubMed]
- Colli, A.; Manzan, E.; Aidietis, A.; Rucinskas, K.; Bizzotto, E.; Besola, L.; Pradegan, N.; Pittarello, D.; Janusauskas, V.; Zakarkaite, D.; et al. An early European experience with transapical off-pump mitral valve repair with NeoChord implantation. Eur. J. Cardiothorac. Surg. 2018, 54, 460–466. [Google Scholar] [CrossRef] [PubMed]
- Gammie, J.S.; Bartus, K.; Gackowski, A.; Szymanski, P.; Bilewska, A.; Kusmierczyk, M.; Kapelak, B.; Rzucidlo-Resil, J.; Duncan, A.; Yadav, R.; et al. Safety and performance of a novel transventricular beating heart mitral valve repair system: 1-year outcomes. Eur. J. Cardiothorac. Surg. 2021, 59, 199–206. [Google Scholar] [CrossRef]
- Hensey, M.; Brown, R.A.; Lal, S.; Sathananthan, J.; Ye, J.; Cheung, A.; Blanke, P.; Leipsic, J.; Moss, R.; Boone, R.; et al. Transcatheter Mitral Valve Replacement: An Update on Current Techniques, Technologies, and Future Directions. JACC Cardiovasc. Interv. 2021, 14, 489–500. [Google Scholar] [CrossRef]
- Guerrero, M.; Pursnani, A.; Narang, A.; Salinger, M.; Wang, D.D.; Eleid, M.; Kodali, S.K.; George, I.; Satler, L.; Waksman, R.; et al. Prospective Evaluation of Transseptal TMVR for Failed Surgical Bioprostheses: MITRAL Trial Valve-in-Valve Arm 1-Year Outcomes. JACC Cardiovasc. Interv. 2021, 14, 859–872. [Google Scholar] [CrossRef]
- Guerrero, M.; Wang, D.D.; Pursnani, A.; Salinger, M.; Russell, H.M.; Eleid, M.; Chakravarty, T.; Ng, M.H.; Kodali, S.K.; Meduri, C.U.; et al. Prospective Evaluation of TMVR for Failed Surgical Annuloplasty Rings: MITRAL Trial Valve-in-Ring Arm 1-Year Outcomes. JACC Cardiovasc. Interv. 2021, 14, 846–858. [Google Scholar] [CrossRef]
- Yoon, S.H.; Whisenant, B.K.; Bleiziffer, S.; Delgado, V.; Dhoble, A.; Schofer, N.; Eschenbach, L.; Bansal, E.; Murdoch, D.J.; Ancona, M.; et al. Outcomes of transcatheter mitral valve replacement for degenerated bioprostheses, failed annuloplasty rings, and mitral annular calcification. Eur. Heart J. 2019, 40, 441–451. [Google Scholar] [CrossRef]
- Simonato, M.; Whisenant, B.; Ribeiro, H.B.; Webb, J.G.; Kornowski, R.; Guerrero, M.; Wijeysundera, H.; Sondergaard, L.; De Backer, O.; Villablanca, P.; et al. Transcatheter Mitral Valve Replacement after Surgical Repair or Replacement: Comprehensive Midterm Evaluation of Valve-in-Valve and Valve-in-Ring Implantation from the VIVID Registry. Circulation 2021, 143, 104–116. [Google Scholar] [CrossRef]
- Guerrero, M.; Wang, D.D.; Eleid, M.F.; Pursnani, A.; Salinger, M.; Russell, H.M.; Kodali, S.K.; George, I.; Bapat, V.N.; Dangas, G.D.; et al. Prospective Study of TMVR Using Balloon-Expandable Aortic Transcatheter Valves in MAC: MITRAL Trial 1-Year Outcomes. JACC Cardiovasc. Interv. 2021, 14, 830–845. [Google Scholar] [CrossRef]
- Coisne, A.; Pontana, F.; Tchetche, D.; Richardson, M.; Longere, B.; Vahdat, O.; Berthoumieu, P.; Van Belle, E.; Rousse, N.; Lancellotti, P.; et al. Transcatheter mitral valve replacement: Factors associated with screening success and failure. EuroIntervention 2019, 15, e983–e989. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.D.; Guerrero, M.; Eng, M.H.; Eleid, M.F.; Meduri, C.U.; Rajagopal, V.; Yadav, P.K.; Fifer, M.A.; Palacios, I.F.; Rihal, C.S.; et al. Alcohol Septal Ablation to Prevent Left Ventricular Outflow Tract Obstruction during Transcatheter Mitral Valve Replacement: First-in-Man Study. JACC Cardiovasc. Interv. 2019, 12, 1268–1279. [Google Scholar] [CrossRef] [PubMed]
- Khan, J.M.; Babaliaros, V.C.; Greenbaum, A.B.; Foerst, J.R.; Yazdani, S.; McCabe, J.M.; Paone, G.; Eng, M.H.; Leshnower, B.G.; Gleason, P.T.; et al. Anterior Leaflet Laceration to Prevent Ventricular Outflow Tract Obstruction during Transcatheter Mitral Valve Replacement. J. Am. Coll. Cardiol. 2019, 73, 2521–2534. [Google Scholar] [CrossRef]
- Sorajja, P.; Moat, N.; Badhwar, V.; Walters, D.; Paone, G.; Bethea, B.; Bae, R.; Dahle, G.; Mumtaz, M.; Grayburn, P.; et al. Initial Feasibility Study of a New Transcatheter Mitral Prosthesis: The First 100 Patients. J. Am. Coll. Cardiol. 2019, 73, 1250–1260. [Google Scholar] [CrossRef] [PubMed]
- Muller, D.W.M.; Sorajja, P.; Duncan, A.; Bethea, B.; Dahle, G.; Grayburn, P.; Babaliaros, V.; Guerrero, M.; Thourani, V.H.; Bedogni, F.; et al. 2-Year Outcomes of Transcatheter Mitral Valve Replacement in Patients with Severe Symptomatic Mitral Regurgitation. J. Am. Coll. Cardiol. 2021, 78, 1847–1859. [Google Scholar] [CrossRef]
- Fukui, M.; Sorajja, P.; Gossl, M.; Bae, R.; Lesser, J.R.; Sun, B.; Duncan, A.; Muller, D.; Cavalcante, J.L. Left Ventricular Remodeling after Transcatheter Mitral Valve Replacement with Tendyne: New Insights from Computed Tomography. JACC Cardiovasc. Interv. 2020, 13, 2038–2048. [Google Scholar] [CrossRef]
- Bapat, V.; Rajagopal, V.; Meduri, C.; Farivar, R.S.; Walton, A.; Duffy, S.J.; Gooley, R.; Almeida, A.; Reardon, M.J.; Kleiman, N.S.; et al. Intrepid Global Pilot Study I. Early Experience with New Transcatheter Mitral Valve Replacement. J. Am. Coll. Cardiol. 2018, 71, 12–21. [Google Scholar] [CrossRef]
- Zahr, F.; Song, H.K.; Chadderdon, S.M.; Gada, H.; Mumtaz, M.; Byrne, T.; Kirshner, M.; Bajwa, T.; Weiss, E.; Kodali, S.; et al. Thirty-Day Outcomes Following Transfemoral Transseptal Transcatheter Mitral Valve Replacement: Intrepid TMVR Early Feasibility Study Results. JACC Cardiovasc. Interv. 2021, 15, 80–89. [Google Scholar] [CrossRef]
- Cheung, A. Tiara: Device Description, Results and Ongoing Studies. In Proceedings of the Transcatheter Cardiovascular Therapeutics (TCT) 2019, San Francisco, CA, USA, 25–29 September 2019; Available online: https://www.tctmd.com/slide/transapical-iii-tiara-device-description-results-and-ongoing-studies (accessed on 26 November 2021).
- Webb, J.; Hensey, M.; Fam, N.; Rodes-Cabau, J.; Daniels, D.; Smith, R.; Szeto, W.; Boone, R.; Ye, J.; Moss, R.; et al. Transcatheter Mitral Valve Replacement with the Transseptal EVOQUE System. JACC Cardiovasc. Interv. 2020, 13, 2418–2426. [Google Scholar] [CrossRef]
- Hildick-Smith, D. HighLife TSMVR Study Status and New Developments. In Proceedings of the PCR London Valves 2021, London, UK, 21–23 November 2021; Available online: https://course.pcronline.com/vod/highlife-tsmvr-study-status-and-new-developments (accessed on 26 November 2021).
- Webb, J.G.; Murdoch, D.J.; Boone, R.H.; Moss, R.; Attinger-Toller, A.; Blanke, P.; Cheung, A.; Hensey, M.; Leipsic, J.; Ong, K.; et al. Percutaneous Transcatheter Mitral Valve Replacement: First-in-Human Experience with a New Transseptal System. J. Am. Coll. Cardiol. 2019, 73, 1239–1246. [Google Scholar] [CrossRef]
- Maisano, F. CardioValve Device Attributes Implant Procedure and Early Results. In Proceedings of the EuroPCR 2019, Paris, France, 21–24 May 2019; Available online: https://www.pcronline.com/Cases-resources-images/Resources/Course-videos-slides/2019/Early-trials-and-First-in-Man-in-mitral-valve-replacement (accessed on 26 November 2021).
- Alperi, A.; Dagenais, F.; Del Val, D.; Bernier, M.; Vahl, T.P.; Khalique, O.K.; Modine, T.; Granada, J.F.; Rodes-Cabau, J. Early Experience with a Novel Transfemoral Mitral Valve Implantation System in Complex Degenerative Mitral Regurgitation. JACC Cardiovasc. Interv. 2020, 13, 2427–2437. [Google Scholar] [CrossRef] [PubMed]
- Genereux, P. AltaValve—Device Description, Results, and Ongoing Studies. In Proceedings of the Transcatheter Cardiovascular Therapeutics (TCT) 2019, San Francisco, CA, USA, 25–29 September 2019; Available online: https://www.tctmd.com/slide/transseptal-vii-altavalve-device-description-results-and-ongoing-studies (accessed on 6 November 2021).
- Nunes Ferreira-Neto, A.; Dagenais, F.; Bernier, M.; Dumont, E.; Freitas-Ferraz, A.B.; Rodes-Cabau, J. Transcatheter Mitral Valve Replacement with a New Supra-Annular Valve: First-in-Human Experience with the AltaValve System. JACC Cardiovasc. Interv. 2019, 12, 208–209. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Device Target | Device | Device Description | Delivery System | Mitral Valve Access | Primary Mitral Regurgitation | Secondary Mitral Regurgitation | Approval Status |
|---|---|---|---|---|---|---|---|
| Mitral Valve Annulus | |||||||
| Direct annuloplasty | Cardioband™ | Polyester sleeve with anchors and a tightening wire to adjust annular dimensions | 25 Fr sheath, steerable catheter | Transeptal | No | Yes | Conformité Européne (CE) marked |
| Millipede™ | Semi-rigid complete nitinol ring with 8 helical stainless-steel anchors | 24 Fr deflectable catheter | Transeptal | No | Yes | - | |
| Indirect annuloplasty | Carillon™ mitralcontour | Proximal and distal nitinol anchors connected by a nitinol connector ribbon | 10 Fr | Via coronary sinus | No | Yes | CE marked |
| The ARTO™ system | A bridge suture connects an anchor in the great cardiac vein (GCV) with an anchor in the interatrial septum | 12 Fr | Via coronary sinus and transeptal puncture | No | Yes | - | |
| Mitral Valve Leaflets | |||||||
| Edge to edge repair | MitraClip™ | Cobalt chromium device with a polyester coating. Consists of two arms that are opened to grasp the leaflet edges and closed to approximate the leaflets creating a figure of 8 double orifice. | 24 Fr | Transeptal | Yes | Yes | CE markedFDA approved |
| PASCAL™ | Consists of two paddles, two clasps, and a spacer. The leaflets are grasped between the paddles and clasps, and the spacer acts to reduce the effective regurgitant orifice area (EROA) | 22 Fr | Transeptal | Yes | Yes | CE markedFDA approved | |
| Chordae Tendineae | |||||||
| Implantation of new chordae tendineae | NeoChord™ | Expanded polytetrafluoroethylene (ePTFE) suture creates a neochord that is tightened and attached to a pledget on the epicardial surface of the ventricle | - | Transapical | Yes | No | CE marked |
| HAPOON™ | Expanded polytetrafluoroethylene (ePTFE) chordal system | 14 Fr | Transapical | Yes Only in severe MR due to PMVL prolapse | No | CE marked | |
| ACC/AHA Guidelines | ESC Guidelines | |||
|---|---|---|---|---|
| 2014 | 2020 | 2017 | 2021 | |
| Primary Mitral Regurgitation (PMR) | May be considered in severely symptomatic patients (New York Heart Association class (NYHA) III or IV) with prohibitive surgical risk IIb B recommendation | Reasonable in severely symptomatic patients (NYHA III or IV) of high or prohibitive surgical risk if anatomy is amenable 2A B-NR recommendation | May be considered for symptomatic severe PMR with suitable anatomy and judged to be at inoperable or high surgical risk by the heart team IIB C recommendation | May be considered for symptomatic patients with suitable anatomy and judged to be at inoperable or high surgical risk by the heart team IIB B recommendation |
| Secondary Mitral Regurgitation (SMR) | No recommendation | Reasonable in patients with persistent symptoms on optimal guideline directed medical therapy (GDMT) and who have appropriate anatomy and with LVEF 20–50%, LVESD ≤ 70 mm and PASP ≤ 70 mmHg 2a B-R recommendation | May be considered when revascularization is not indicated and surgical risk is not low with LVEF > 30% who remain symptomatic despite optimal GDMT (including cardiac resynchronizing therapy (CRT)) IIb C recommendation | Should be considered in selected patients not eligible for surgery and fulfilling criteria suggesting an increased chance of responding to treatment IIa B recommendation |
| May be considered in patients with LVEF < 30% with no revascularization option and remain symptomatic on optimum GDMT (including CRT) after careful evaluation for ventricular assist device or heart transplant IIb C recommendation | May be considered by the heart team in high-risk symptomatic patients not fulfilling criteria suggesting an increased chance of responding to TEER after careful evaluation for ventricular assist device or heart transplant IIb C recommendation | |||
| EVEREST Echocardiographic Criteria |
| Mitral valve orifice area > 4.0 cm2 |
| Transvalvular gradient < 4 mmHg |
| Width of flail segment < 15 mm |
| Flail gap < 10 mm |
| Coaptation depth < 11 mm |
| Mobile leaflet length > 10 mm |
| COAPT Criteria |
| Secondary mitral regurgitation |
| At least one HF admission in the previous year or increased natriuretic peptide |
| NYHA ≥ II |
| Left ventricular ejection fraction (LVEF) 20–50% |
| Left ventricular end-systolic diameter ≤ 70 mm |
| Device | Device Description | Delivery System | Recapture | Valve Sizes | Mitral Valve Access | Primary Mitral Regurgitation | Secondary Mitral Regurgitation | Approval Status |
|---|---|---|---|---|---|---|---|---|
| Transapical TMVR systems | ||||||||
| Tendyne™ | A two-stent configuration: Inner stent housing the bovine pericardial valve. An outer stent that conforms to the native MV. Stents are connected with a PET fabric cuff. The valve is tethered to the LV and connected to an epicardial pad to hold it in position | 34 or 36 Fr depending on valve size | Repositionable and recapturable | Valve has two profiles Low profile: EOA 2.2 cm2 Standard profile: EOA 3.0 cm2 Outer stent available in a number of sizes to conform to mitral annulus anatomy | Transapical | Yes | Yes | CE marked |
| Tiara™ | Self-expanding nitinol stent with a trileaflet bovine pericardial valve. D-shaped configuration to conform to the MV annulus | 32 for 35 mm valve 36 Fr for 40 mm valve | Repositionable and recapturable | Two sizes: 35mm and 40 mm | Transapical | Yes | Yes | - |
| Transapical and Transeptal systems | ||||||||
| Intrepid™ | A two-stent configuration: Inner stent housing the bovine pericardial valve. Outer stent forms a fixation ring. Both stents are covered with PET | 35 Fr transapical 35 Fr transseptal | Repositionable and recapturable | Single size valve: 27 mm Outer stent available in two sizes (42 and 48 mm) | Transapical Transseptal | Yes | Yes | - |
| AltaValve™ | Self-expanding supra-annular nitinol sphere housing a 27 mm bovine pericardial valve. | 32 Fr | Recapturable and retrievable | 27 mm valve Spherical frame ranging from 50–90 mm | Transapical Transeptal | Yes | Yes | - |
| Transeptal TMVR systems | ||||||||
| EVOQUE™ | Self-expanding nitinol frame with a bovine pericardial valve. The valve is anchored by capturing the native MV leaflets and subvalvular apparatus. An atrial sealing skirt prevents PVL | 28 Fr | No | 44 and 48 mm | Transeptal | Yes | Yes | - |
| HighLife™ | Two components consisting of a subannular ring implant delivered retrogradely via the femoral artery and aortic valve, and the valve component delivered transeptally | 30 Fr for transeptal valve delivery 18Fr femoral artery access for subannular ring implant | No | 28 mm valve and ring | Transeptal | Yes | Yes | - |
| Sapien M3™ | Two components consisting of a subvalvular “dock”, which encases the balloon expandable Sapien valve (29 mm) | 20 Fr | Subvalvular “dock” component is recapturable | 29 mm valve | Transeptal | Yes | Yes | - |
| CardioValve™ | Two nitinol self-expanding frames: atrial and ventricular encasing bovine pericardial leaflets. | 30 Fr | - | Three sizes available covering commissural diameters from 36 to 53 mm | Transeptal | Yes | Yes | - |
| Cephea™ | Double disc system connected via a central column that houses the bovine pericardial valve. | Not stated | Recapturable | One size available with a 36 mm central waist | Transeptal | Yes | Yes | - |
| Device | Study Name | Study Design | Inclusion Criteria | Primary Outcome |
|---|---|---|---|---|
| Tendyne | Clinical trial to evaluate the safety and effectiveness of using the Tendyne mitral valve system for the treatment of symptomatic mitral regurgitation (MR) (SUMMIT) NCT03433274 | Prospective multicentre study with three cohorts: (a) Randomized cohort: 1:1 basis with MitraClip (b) Non-randomized cohort © MAC cohort Number of participants: 958 | Symptomatic, moderate-severe, or severe MR, or severe mitral annular calcification (MAC) | (a) Randomized cohort: Survival free of HF hospitalization at 12 months (b) Non-randomized cohort: composite of all-cause mortality, CV related rehospitalization, stroke, or MV reintervention or reoperati©(c) MAC cohort: survival free of HF rehospitalization at 12 months |
| Intrepid | Transcatheter mitral valve replacement with the medtronic Intrepid™ TMVR system in patients with severe symptomatic MR (APOLLO) NCT03242642 | Multicentre, single arm, non-randomized study with two cohorts (a) Primary cohort: moderate-severe or severe MR not suitable for TEER or surgical MVR (b) MAC cohort: moderate-severe or severe-MR with MAC | Moderate-severe or severe MR High surgical risk Not suitable for TEER | (a) Primary cohort: all-cause mortality or heart failure hospitalization at 30 days or KCCQ improvement < 10 composite (b) MAC cohort: composite of all-cause mortality and heart failure hospitalization |
| EVOQUE | Edwards EVOQUE EOS mitral valve replacement: investigation of safety and performance after mitral valve replacement with a transcatheter device (MISCEND) NCT02718001 | Multicentre, prospective, single arm non-randomized study examining the safety and performance of the EVOQUE device in MR Number of participants: 83 | Symptomatic mitral regurgitation High surgical risk Meeting anatomical criteria for the EVOQUE device | Major adverse events within 30 days |
| HighLife | Feasibility study of the HighLife 28mm trans-septal trans-catheter mitral valve in patients with moderate-severe or severe mitral regurgitation and at high surgical risk NCT04029363 | Multicentre, single arm non-randomized study evaluating the feasibility, safety, and performance of the HighLife 28 mm TMVR Number of participants: 50 | Moderate-severe or severe MR High risk for surgery Meeting anatomical criteria for the HighLife valve | Major adverse events within 30 days |
| HighLife Clarity | HighLife TSMVR feasibility study of the open cell CLARITY valve in patients with moderate-severe or severe MR, high surgical risk, and with a high risk for left ventricular outflow tract obstruction (LVOTO) NCT04888247 | Open label, single centre, single arm, non-randomized study to assess the feasibility, safety, and performance of the HighLife CLARITY transeptal mitral valve replacement system Number of participants: 15 | Moderate-severe or severe MR High surgical risk Meets anatomical criteria for HighLife Clarity valve High risk of LVOTO | Technical success: (a) Successful vascular access delivery and retrieval (b) Deployment and correct positi©ng (c) Freedom from additional emergency surgery or re-intervention related to the device or access |
| Sapien M3 | Sapien M3 system transcatheter mitral valve replacement via transseptal access. The ENCIRCLE trial NCT04153292 | Open label, single arm non-randomized study with two cohorts (a) Patients deemed unsuitable for surgical MVR (b) Patients with failed attempt at TEER Number of participants: 400 | Moderate-severe or severe MR Unsuitable for surgical MVR due to clinical anatomical or technical considerations Failed attempt at TEER | Death and/or HF rehospitalization |
| CardioValve | CardioValve transfemoral mitral valve system (AHEAD) (United States) NCT03813524 | Open label, multicentre, single arm, non-randomized study (United States centres) Number of participants: 15 | Symptomatic severe MR High surgical risk LVEF ≥ 30% Cardiac index > 2.0 Patients must be receiving GDMT for at least 30 days prior to enrollment | Technical success (a) Successful access, delivery, and retrieval of the device (b) Successful deployment and correct pos©oning (c) Freedom from emergency surgery or reintervention related to the device Without procedure death, stroke, or device dysfunction |
| European feasibility study of the CardioValve transfemoral mitral valve system (AHEAD study) | Open label, multicentre, single arm, non-randomized study (European centres) Number of participants: 30 | Symptomatic severe MR High surgical risk Anatomy suitable for the CardioValve device Patients must be receiving GDMT for at least 30 days prior to enrolment (or CRT if indicated) | Freedom from all-cause mortality and major adverse events | |
| AltaValve | AltaValve early feasibility study protocol | Open label, multicentre, single arm, non-randomized study Number of participants: 15 | Severe symptomatic MR High surgical risk | Major adverse cardiac events at 30 days (death, stroke, and MV related repeat intervention) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McInerney, A.; Marroquin-Donday, L.; Tirado-Conte, G.; Hennessey, B.; Espejo, C.; Pozo, E.; de Agustín, A.; Gonzalo, N.; Salinas, P.; Núñez-Gil, I.; et al. Transcatheter Treatment of Mitral Regurgitation. J. Clin. Med. 2022, 11, 2921. https://doi.org/10.3390/jcm11102921
McInerney A, Marroquin-Donday L, Tirado-Conte G, Hennessey B, Espejo C, Pozo E, de Agustín A, Gonzalo N, Salinas P, Núñez-Gil I, et al. Transcatheter Treatment of Mitral Regurgitation. Journal of Clinical Medicine. 2022; 11(10):2921. https://doi.org/10.3390/jcm11102921
Chicago/Turabian StyleMcInerney, Angela, Luis Marroquin-Donday, Gabriela Tirado-Conte, Breda Hennessey, Carolina Espejo, Eduardo Pozo, Alberto de Agustín, Nieves Gonzalo, Pablo Salinas, Iván Núñez-Gil, and et al. 2022. "Transcatheter Treatment of Mitral Regurgitation" Journal of Clinical Medicine 11, no. 10: 2921. https://doi.org/10.3390/jcm11102921
APA StyleMcInerney, A., Marroquin-Donday, L., Tirado-Conte, G., Hennessey, B., Espejo, C., Pozo, E., de Agustín, A., Gonzalo, N., Salinas, P., Núñez-Gil, I., Fernández-Ortiz, A., Mejía-Rentería, H., Macaya, F., Escaned, J., Nombela-Franco, L., & Jiménez-Quevedo, P. (2022). Transcatheter Treatment of Mitral Regurgitation. Journal of Clinical Medicine, 11(10), 2921. https://doi.org/10.3390/jcm11102921