
Predictive Value of Blood Coagulation Parameters in Poor Outcomes in COVID-19 Patients: A Retrospective Observational Study in Romania

 , ,
, ,  , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Settings
2.2. Participants
2.3. Variables and Data Sources
2.4. Statistical Analysis
3. Results
3.1. Participants Selection and Baseline Characteristics
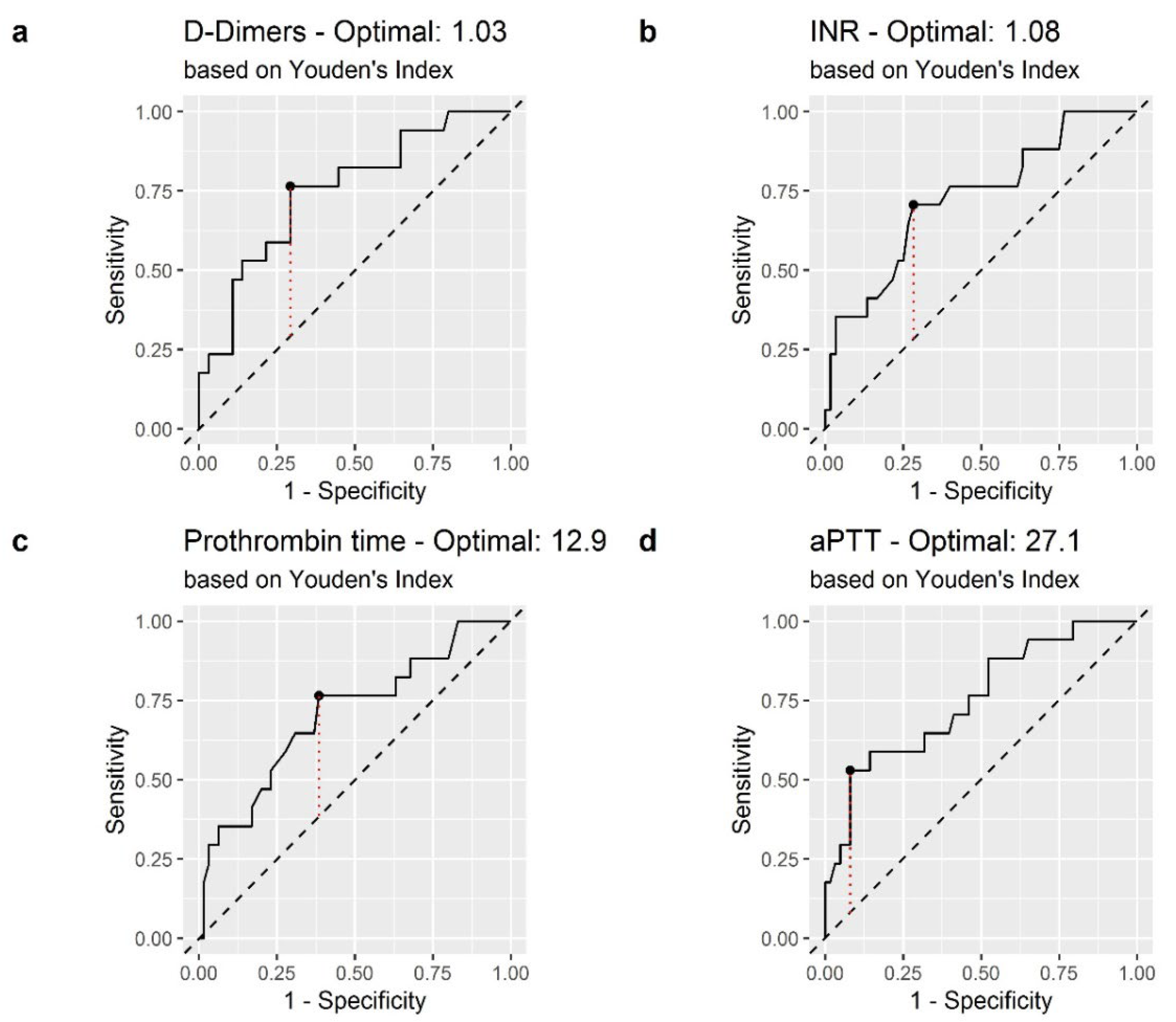
3.2. Coagulation Biomarker Cut-Off Values in Predicting Mortality in Patients with COVID-19
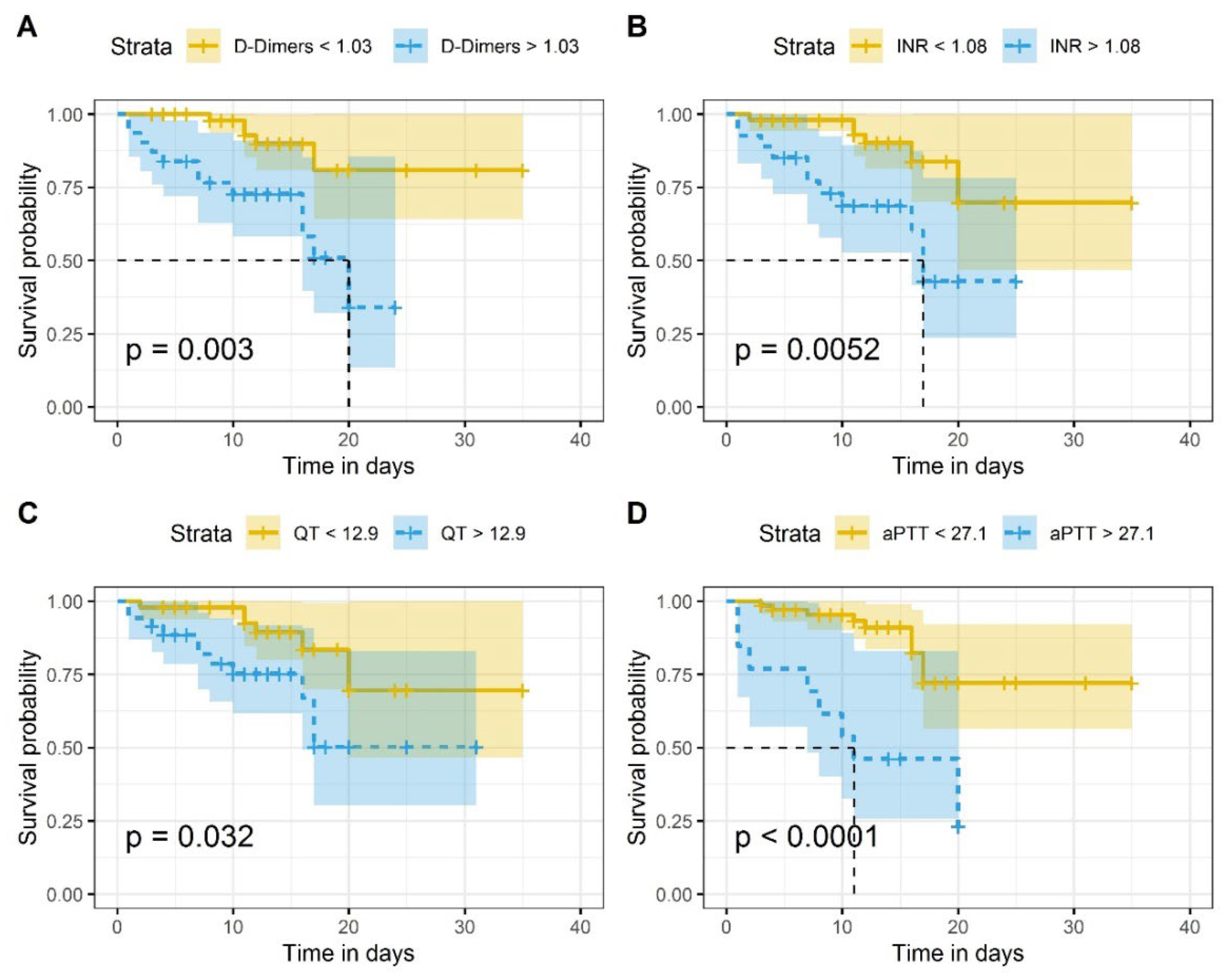
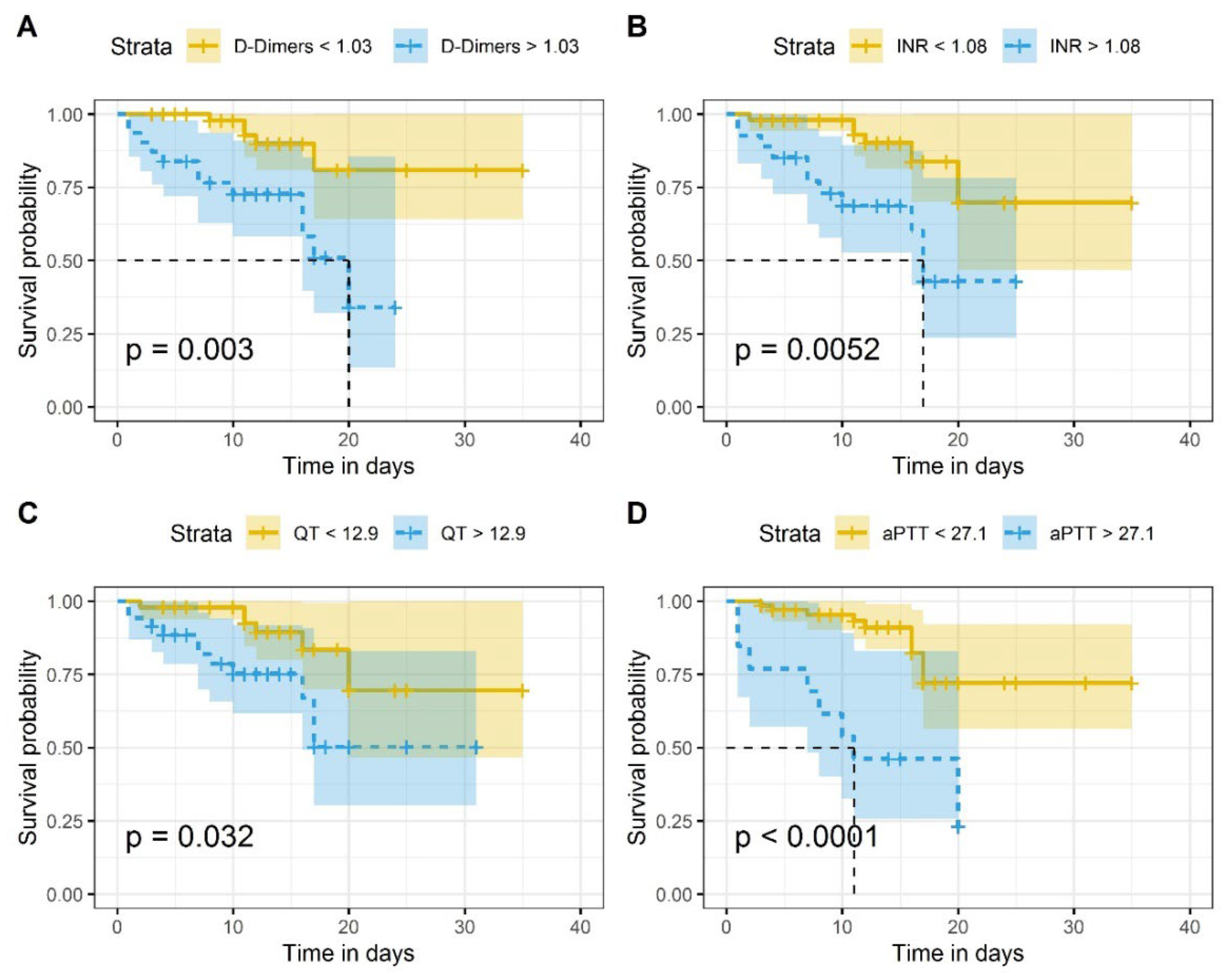
3.3. Association of D-Dimer, INR, PT and aPTT Scores with COVID-19 Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Coronavirus. Available online: https://www.who.int/westernpacific/health-topics/coronavirus (accessed on 27 February 2022).
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [PubMed]
- COVID Live-Coronavirus Statistics—Worldometer. Available online: https://www.worldometers.info/coronavirus/ (accessed on 27 February 2022).
- Merad, M.; Martin, J.C. Pathological Inflammation in Patients with COVID-19: A Key Role for Monocytes and Macrophages. Nat. Rev. Immunol. 2020, 20, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, T.S.; de Sá, K.S.G.; Ishimoto, A.Y.; Becerra, A.; Oliveira, S.; Almeida, L.; Gonçalves, A.V.; Perucello, D.B.; Andrade, W.A.; Castro, R.; et al. Inflammasomes Are Activated in Response to SARS-CoV-2 Infection and Are Associated with COVID-19 Severity in Patients. J. Exp. Med. 2020, 218, e20201707. [Google Scholar] [CrossRef] [PubMed]
- Luo, H.; You, C.; Lu, S.; Fu, Y. Characteristics of Coagulation Alteration in Patients with COVID-19. Ann. Hematol. 2021, 100, 45–52. [Google Scholar] [CrossRef]
- Lorini, F.L.; Di Matteo, M.; Gritti, P.; Grazioli, L.; Benigni, A.; Zacchetti, L.; Bianchi, I.; Fabretti, F.; Longhi, L. Coagulopathy and COVID-19. Eur. Heart J. Suppl. 2021, 23 (Suppl. E), E95–E98. [Google Scholar] [CrossRef]
- Jin, S.; Jin, Y.; Xu, B.; Hong, J.; Yang, X. Prevalence and Impact of Coagulation Dysfunction in COVID-19 in China: A Meta-Analysis. Thromb. Haemost. 2020, 120, 1524–1535. [Google Scholar] [CrossRef]
- Martín-Rojas, R.M.; Pérez-Rus, G.; Delgado-Pinos, V.E.; Domingo-González, A.; Regalado-Artamendi, I.; Alba-Urdiales, N.; Demelo-Rodríguez, P.; Monsalvo, S.; Rodríguez-Macías, G.; Ballesteros, M.; et al. COVID-19 Coagulopathy: An In-depth Analysis of the Coagulation System. Eur. J. Haematol. 2020, 105, 741–750. [Google Scholar] [CrossRef]
- Tang, N.; Li, D.; Wang, X.; Sun, Z. Abnormal Coagulation Parameters Are Associated with Poor Prognosis in Patients with Novel Coronavirus Pneumonia. J. Thromb. Haemost. 2020, 18, 844–847. [Google Scholar] [CrossRef] [Green Version]
- Cui, S.; Chen, S.; Li, X.; Liu, S.; Wang, F. Prevalence of Venous Thromboembolism in Patients with Severe Novel Coronavirus Pneumonia. J. Thromb. Haemost. 2020, 18, 1421–1424. [Google Scholar] [CrossRef]
- Citu, C.; Gorun, F.; Motoc, A.; Ratiu, A.; Gorun, O.M.; Burlea, B.; Neagoe, O.; Citu, I.M.; Rosca, O.; Bratosin, F.; et al. Evaluation and Comparison of the Predictive Value of 4C Mortality Score, NEWS, and CURB-65 in Poor Outcomes in COVID-19 Patients: A Retrospective Study from a Single Center in Romania. Diagnostics 2022, 12, 703. [Google Scholar] [CrossRef]
- Citu, C.; Gorun, F.; Motoc, A.; Sas, I.; Gorun, O.M.; Burlea, B.; Tuta-Sas, I.; Tomescu, L.; Neamtu, R.; Malita, D.; et al. The Predictive Role of NLR, d-NLR, MLR, and SIRI in COVID-19 Mortality. Diagnostics 2022, 12, 122. [Google Scholar] [CrossRef] [PubMed]
- Tan, E.; Song, J.; Deane, A.M.; Plummer, M.P. Global Impact of Coronavirus Disease 2019 Infection Requiring Admission to the ICU. Chest 2021, 159, 524–536. [Google Scholar] [CrossRef] [PubMed]
- Araya, S.; Mamo, M.A.; Tsegay, Y.G.; Atlaw, A.; Aytenew, A.; Hordofa, A.; Negeso, A.E.; Wordofa, M.; Niguse, T.; Cheru, M.; et al. Blood Coagulation Parameter Abnormalities in Hospitalized Patients with Confirmed COVID-19 in Ethiopia. PLoS ONE 2021, 16, e0252939. [Google Scholar] [CrossRef] [PubMed]
- Adam, E.H.; Zacharowski, K.; Miesbach, W. A Comprehensive Assessment of the Coagulation Profile in Critically Ill COVID-19 Patients. Thromb. Res. 2020, 194, 42–44. [Google Scholar] [CrossRef]
- Wang, L.; He, W.-B.; Yu, X.-M.; Hu, D.-L.; Jiang, H. Prolonged Prothrombin Time at Admission Predicts Poor Clinical Outcome in COVID-19 Patients. World J. Clin. Cases 2020, 8, 4370–4379. [Google Scholar] [CrossRef] [PubMed]
- Saurabh, A.; Dey, B.; Raphael, V.; Deb, P.; Khonglah, Y.; Tiewsoh, I. Role of Coagulation Profile in Predicting Disease Severity Among Patients of COVID-19. Cureus 2021, 13, e19124. [Google Scholar] [CrossRef] [PubMed]
- Yao, Y.; Cao, J.; Wang, Q.; Shi, Q.; Liu, K.; Luo, Z.; Chen, X.; Chen, S.; Yu, K.; Huang, Z.; et al. D-Dimer as a Biomarker for Disease Severity and Mortality in COVID-19 Patients: A Case Control Study. J. Intensive Care 2020, 8, 49. [Google Scholar] [CrossRef]
- Zhao, R.; Su, Z.; Komissarov, A.A.; Liu, S.-L.; Yi, G.; Idell, S.; Matthay, M.A.; Ji, H.-L. Associations of D-Dimer on Admission and Clinical Features of COVID-19 Patients: A Systematic Review, Meta-Analysis, and Meta-Regression. Front. Immunol. 2021, 12, 691249. [Google Scholar] [CrossRef]
- Poudel, A.; Poudel, Y.; Adhikari, A.; Aryal, B.B.; Dangol, D.; Bajracharya, T.; Maharjan, A.; Gautam, R. D-Dimer as a Biomarker for Assessment of COVID-19 Prognosis: D-Dimer Levels on Admission and Its Role in Predicting Disease Outcome in Hospitalized Patients with COVID-19. PLoS ONE 2021, 16, e0256744. [Google Scholar] [CrossRef]
- Smadja, D.M.; Bory, O.M.; Diehl, J.-L.; Mareau, A.; Gendron, N.; Jannot, A.-S.; Chocron, R. Daily Monitoring of D-Dimer Allows Outcomes Prediction in COVID-19. TH Open Companion J. Thromb. Haemost. 2022, 6, e21–e25. [Google Scholar] [CrossRef]
- Cidade, J.P.; Coelho, L.; Costa, V.; Morais, R.; Moniz, P.; Morais, L.; Fidalgo, P.; Tralhão, A.; Paulino, C.; Nora, D.; et al. Predictive Value of D-Dimer in the Clinical Outcome of Severe COVID19 Patients: Are We Giving It Too Much Credit? Clin. Appl. Thromb. Off. J. Int. Acad. Clin. Appl. Thromb. 2022, 28, 10760296221079612. [Google Scholar] [CrossRef] [PubMed]
- Zinellu, A.; Paliogiannis, P.; Carru, C.; Mangoni, A.A. INR and COVID-19 Severity and Mortality: A Systematic Review with Meta-Analysis and Meta-Regression. Adv. Med. Sci. 2021, 66, 372–380. [Google Scholar] [CrossRef] [PubMed]
- Long, H.; Nie, L.; Xiang, X.; Li, H.; Zhang, X.; Fu, X.; Ren, H.; Liu, W.; Wang, Q.; Wu, Q. D-Dimer and Prothrombin Time Are the Significant Indicators of Severe COVID-19 and Poor Prognosis. BioMed Res. Int. 2020, 2020, e6159720. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Wang, Q.; Xu, M.; Li, C. A Retrospective Analysis of the Coagulation Dysfunction in COVID-19 Patients. Clin. Appl. Thromb. 2020, 26, 1076029620964868. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Variables | Total | Survivors n = 65 (79.3%) | Non-Survivors n = 17 (20.7%) | p-Value |
|---|---|---|---|---|
| Demographics | ||||
| Age [Median (IQR)] | 66.5 (17) | 65 (13.91) | 71 (12.13) | 0.01 |
| Gender: Female [n (%)] | 42 (51.2%) | 33 (50.8%) | 9 (52.9%) | 0.87 |
| Comorbidities [n (%)] | ||||
| Hypertension | 53 (64.6%) | 40 (61.5%) | 13 (76.5%) | 0.25 |
| CKD | 35 (42.7%) | 26 (40.0%) | 9 (52.9%) | 0.33 |
| COPD | 14 (17.1%) | 10 (15.4%) | 4 (23.5%) | 0.42 |
| Cardiac disease | 35 (42.7%) | 24 (36.9%) | 11 (64.7%) | 0.03 |
| Diabetes | 32 (39.0%) | 25 (38.5%) | 7 (41.2%) | 0.83 |
| Cancer | 12 (14.6%) | 9 (13.8%) | 3 (17.6%) | 0.69 |
| Coagulation Biomarkers [Median (IQR)] | ||||
| D-dimers (μ/mL) | 0.79 (1.18) | 0.65 (0.77) | 1.95 (1.36) | 0.001 |
| INR | 1.04 (0.18) | 1.02 (0.15) | 1.11 (0.38) | 0.004 |
| aPTT (seconds) | 22.65 (4.7) | 22.0 (3.95) | 27.1 (5.90) | 0.001 |
| PT (seconds) | 12.65 | 12.3 (1.6) | 13.3 (3.1) | 0.009 |
| Fibrinogen (mg/dL) | 567.12 (246.0) | 563.71 (262.0) | 609.72 (202.7) | 0.97 |
| Clinical course | ||||
| Length of hospitalization [Median (IQR)] | 13 (6.75) | 14 (5) | 10 (12) | 0.03 |
| ICU admission [n (%)] | 17 (20.7%) | 7 (10.8%) | 10 (58.8%) | <0.001 |
| Biomarker | Cut-Off | AUC | Youden | Sensitivity | Specificity |
|---|---|---|---|---|---|
| D-Dimer | 1.03 | 0.751 | 0.472 | 76% | 70% |
| INR | 1.08 | 0.724 | 0.442 | 70% | 71% |
| PT | 12.9 | 0.706 | 0.380 | 76% | 61% |
| aPTT | 27.1 | 0.753 | 0.450 | 52% | 92% |
| Variables | Estimate | Std. Error | z-Statistic | p Value | Confidence Interval | |
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| D-Dimer > 1.03 | 1.76 | 0.59 | 2.94 | <0.001 | 0.63 | 3.01 |
| INR > 1.08 | 1.62 | 0.58 | 2.76 | 0.005 | 0.49 | 2.82 |
| PT > 12.9 | 1.14 | 0.56 | 2.01 | 0.04 | 0.05 | 2.31 |
| aPTT > 27.1 | 2.33 | 0.67 | 3.46 | <0.001 | 1.04 | 3.72 |
| Variables | aOR | Std. Error | z-Statistic | p Value | Confidence Interval | |
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| D-Dimer > 1.03 | 6.05 | 0.72 | 2.50 | 0.01 | 1.57 | 27.5 |
| INR > 1.08 | 6.50 | 0.67 | 2.81 | <0.001 | 1.86 | 26.3 |
| PT > 12.9 | 3.94 | 0.64 | 2.13 | 0.03 | 1.16 | 15.2 |
| aPTT > 27.1 | 11.7 | 0.82 | 2.98 | <0.001 | 2.53 | 68.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Citu, C.; Burlea, B.; Gorun, F.; Motoc, A.; Gorun, O.M.; Malita, D.; Ratiu, A.; Margan, R.; Grigoras, M.L.; Bratosin, F.; et al. Predictive Value of Blood Coagulation Parameters in Poor Outcomes in COVID-19 Patients: A Retrospective Observational Study in Romania. J. Clin. Med. 2022, 11, 2831. https://doi.org/10.3390/jcm11102831
Citu C, Burlea B, Gorun F, Motoc A, Gorun OM, Malita D, Ratiu A, Margan R, Grigoras ML, Bratosin F, et al. Predictive Value of Blood Coagulation Parameters in Poor Outcomes in COVID-19 Patients: A Retrospective Observational Study in Romania. Journal of Clinical Medicine. 2022; 11(10):2831. https://doi.org/10.3390/jcm11102831
Chicago/Turabian StyleCitu, Cosmin, Bogdan Burlea, Florin Gorun, Andrei Motoc, Oana Maria Gorun, Daniel Malita, Adrian Ratiu, Roxana Margan, Mirela Loredana Grigoras, Felix Bratosin, and et al. 2022. "Predictive Value of Blood Coagulation Parameters in Poor Outcomes in COVID-19 Patients: A Retrospective Observational Study in Romania" Journal of Clinical Medicine 11, no. 10: 2831. https://doi.org/10.3390/jcm11102831
APA StyleCitu, C., Burlea, B., Gorun, F., Motoc, A., Gorun, O. M., Malita, D., Ratiu, A., Margan, R., Grigoras, M. L., Bratosin, F., & Citu, I. M. (2022). Predictive Value of Blood Coagulation Parameters in Poor Outcomes in COVID-19 Patients: A Retrospective Observational Study in Romania. Journal of Clinical Medicine, 11(10), 2831. https://doi.org/10.3390/jcm11102831