
Prevalence and Correlates of Sexually Transmitted Infections in Transgender People: An Italian Multicentric Cross-Sectional Study

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.3. Statistical Analysis
3. Results
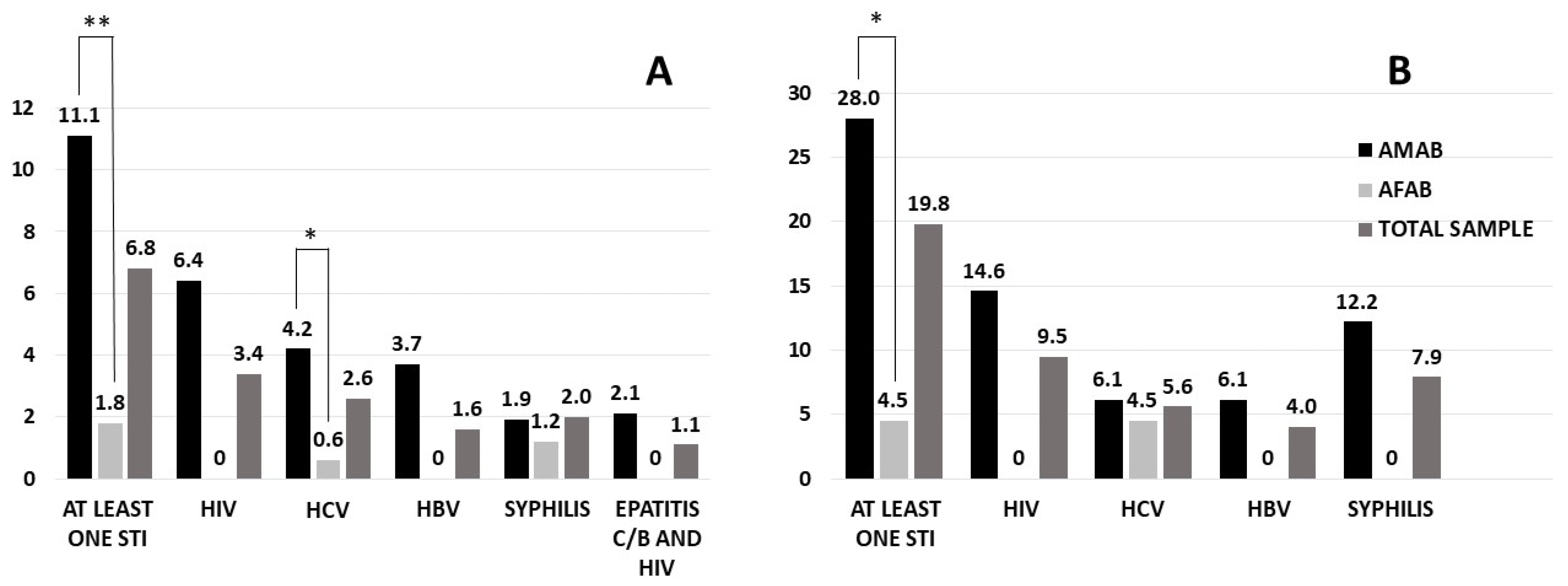
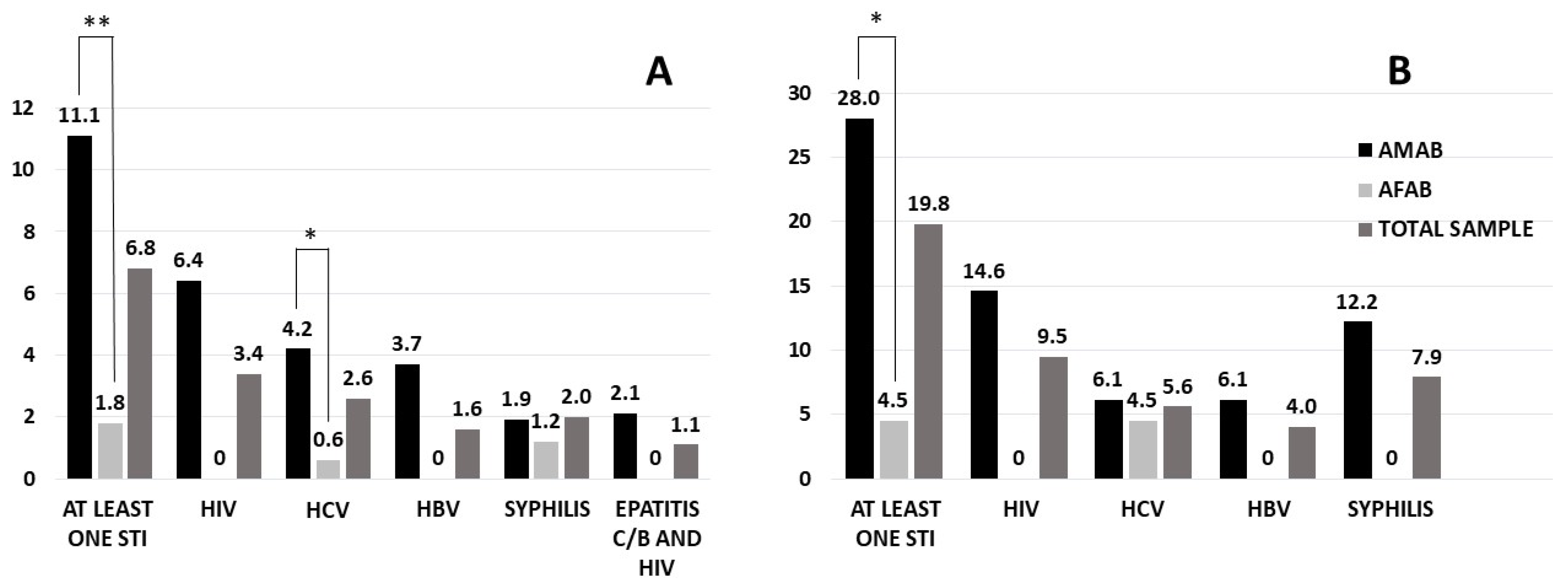
3.1. Self-Reported Prevalence of STIs
3.2. Serological Prevalence of STIs
3.3. Sociodemographic Characteristics
3.4. Lifestyle, General and Mental Health Status
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. International Classification of Diseases and Related Health Problems; 11th Revision (ICD-11); ICD-11 Geneva; World Health Organ: Geneva, Switzerland, 2019. [Google Scholar]
- Fisher, A.D.; Castellini, G.; Ristori, J.; Casale, H.; Giovanardi, G.; Carone, N.; Fanni, E.; Mosconi, M.; Ciocca, G.; Jannini, E.A.; et al. Who has the worst attitudes toward sexual minorities? Comparison of transphobia and homophobia levels in gender dysphoric individuals, the general population and health care providers. J. Endocrinol. Investig. 2016, 40, 263–273. [Google Scholar] [CrossRef] [PubMed]
- Romani, A.; Mazzoli, F.; Ristori, J.; Cocchetti, C.; Cassioli, E.; Castellini, G.; Mosconi, M.; Meriggiola, M.C.; Gualdi, S.; Giovanardi, G.; et al. Psychological Wellbeing and Perceived Social Acceptance in Gender Diverse Individuals. J. Sex. Med. 2021, 18, 1933–1944. [Google Scholar] [CrossRef] [PubMed]
- Hatzenbuehler, M.L.; Phelan, J.C.; Link, B. Stigma as a Fundamental Cause of Population Health Inequalities. Am. J. Public Health 2013, 103, 813–821. [Google Scholar] [CrossRef]
- Brennan, J.; Kuhns, L.M.; Johnson, A.K.; Belzer, M.; Wilson, E.C.; Garofalo, R.; The Adolescent Medicine Trials Network for HIV/AIDS Interventions. Syndemic Theory and HIV-Related Risk Among Young Transgender Women: The Role of Multiple, Co-Occurring Health Problems and Social Marginalization. Am. J. Public Health 2012, 102, 1751–1757. [Google Scholar] [CrossRef]
- Benotsch, E.G.; Zimmerman, R.; Cathers, L.; McNulty, S.; Pierce, J.; Heck, T.; Perrin, B.P.; Snipes, D. Non-medical use of prescription drugs, polysubstance use, and mental health in transgender adults. Drug Alcohol. Depend. 2013, 132, 391–394. [Google Scholar] [CrossRef]
- Bockting, W.O.; Miner, M.H.; Romine, R.E.S.; Hamilton, A.; Coleman, E. Stigma, Mental Health, and Resilience in an Online Sample of the US Transgender Population. Am. J. Public Health 2013, 103, 943–951. [Google Scholar] [CrossRef]
- Operario, D.; Yang, M.-F.; Reisner, S.L.; Iwamoto, M.; Nemoto, T. Stigma and the syndemic of hiv-related health risk behaviors in a diverse sample of transgender women. J. Community Psychol. 2014, 42, 544–557. [Google Scholar] [CrossRef]
- Clements-Nolle, K.; Marx, R.; Guzman, R.; Katz, M. HIV prevalence, risk behaviors, health care use, and mental health status of transgender persons: Implications for public health intervention. Am. J. Public Health 2001, 91, 915–921. [Google Scholar] [CrossRef] [Green Version]
- Luzzati, R.; Zatta, M.; Pavan, N.; Serafin, M.; Maurel, C.; Trombetta, C.; Barbone, F. Prevalence of Human Immunodeficiency Virus, Hepatitis B Virus, and Hepatitis C Virus Infections Among Transgender Persons Referred to an Italian Center for Total Sex Reassignment Surgery. Sex. Transm. Dis. 2016, 43, 407–411. [Google Scholar] [CrossRef]
- Carobene, M.; Bolcic, F.; Farías, M.S.D.R.; Quarleri, J.; Ávila, M.M. HIV, HBV, and HCV molecular epidemiology among trans (transvestites, transsexuals, and transgender) sex workers in Argentina. J. Med. Virol. 2014, 86, 64–70. [Google Scholar] [CrossRef]
- D’Antuono, A.; Cocci, C.; Carlà, E.; De Tommaso, S. Prevalence of STIs and HIV infection among immigrant sex workers attending an STD centre in Bologna, Italy. Sex. Transm. Infect. 1999, 75, 273–274. [Google Scholar] [PubMed]
- Farías, M.S.D.R.; Garcia, M.N.; Reynaga, E.; Romero, M.; Vaulet, M.L.G.; Fermepin, M.R.; Toscano, M.F.; Rey, J.; Marone, R.; Squiquera, L.; et al. First report on sexually transmitted infections among trans (male to female transvestites, transsexuals, or transgender) and male sex workers in Argentina: High HIV, HPV, HBV, and syphilis prevalence. Int. J. Infect. Dis. 2011, 15, e635–e640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russi, J.C.; Serra, M.; Vinoles, J.; Pérez, M.T.; Ruchansky, D.; Alonso, G.; Sanchez, J.L.; Russell, K.L.; Montano, S.M.; Negrete, M.; et al. Sexual transmission of hepatitis B virus, hepatitis C virus, and human immunodeficiency virus type 1 infections among male transvestite commercial sex workers in Montevideo, Uruguay. Am. J. Trop. Med. Hyg. 2003, 68, 716–720. [Google Scholar] [CrossRef] [PubMed]
- Spizzichino, L.; Zaccarelli, M.; Rezza, G.; Ippolito, G.; Antinori, A.; Gattari, P. HIV infection among foreign transsexual sex workers in Rome: Prevalence, behavior patterns, and seroconversion rates. Sex. Transm. Dis. 2001, 28, 405–411. [Google Scholar] [CrossRef]
- Herbst, J.H.; Jacobs, E.D.; Finlayson, T.J.; McKleroy, V.S.; Neumann, M.S.; Crepaz, N.; HIV/AIDS Prevention Research Synthesis Team. Estimating HIV prevalence and risk behaviors of transgender persons in the United States: A systematic review. AIDS Behav. 2008, 12, 1–17. [Google Scholar] [CrossRef]
- Guadamuz, T.E.; Wimonsate, W.; Varangrat, A.; Phanuphak, P.; Jommaroeng, R.; McNicholl, J.M.; Mock, P.A.; Tappero, J.W.; van Griensven, F. HIV Prevalence, Risk Behavior, Hormone Use and Surgical History Among Transgender Persons in Thailand. AIDS Behav. 2010, 15, 650–658. [Google Scholar] [CrossRef] [Green Version]
- Baral, S.D.; Poteat, T.; Strömdahl, S.; Wirtz, A.L.; Guadamuz, T.E.; Beyrer, C. Worldwide burden of HIV in transgender women: A systematic review and meta-analysis. Lancet Infect. Dis. 2013, 13, 214–222. [Google Scholar] [CrossRef]
- Van Gerwen, O.T.; Jani, A.; Long, D.M.; Austin, E.L.; Musgrove, K.; Muzny, C.A. Prevalence of Sexually Transmitted Infections and Human Immunodeficiency Virus in Transgender Persons: A Systematic Review. Transgender Health 2020, 5, 90–103. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; DSM-5; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Mast, E.E.; Margolis, H.S.; Fiore, A.E.; Brink, E.W.; Goldstein, S.T.; Wang, S.A.; Moyer, L.A.; Bell, B.P.; Alter, M.J.; Advisory Committee on Immunization Practices (ACIP). A comprehensive immunization strategy to eliminate transmission of hepatitis B virus infection in the United States: Recommendations of the Advisory Committee on Immunization Practices (ACIP) part 1: Immunization of infants, children, and adolescents. MMWR. Recomm. Rep. 2005, 54, 1–31. [Google Scholar]
- Nemoto, T.; Operario, D.; Keatley, J.; Villegas, D. Social context of HIV risk behaviours among male-to-female transgenders of colour. AIDS Care 2004, 16, 724–735. [Google Scholar] [CrossRef]
- Fisher, A.D.; Bandini, E.; Casale, H.; Ferruccio, N.; Meriggiola, M.C.; Gualerzi, A.; Manieri, C.; Jannini, E.; Mannucci, E.; Monami, M.; et al. Sociodemographic and Clinical Features of Gender Identity Disorder: An Italian Multicentric Evaluation. J. Sex. Med. 2013, 10, 408–419. [Google Scholar] [CrossRef] [PubMed]
- Garofalo, R.; Deleon, J.; Osmer, E.; Doll, M.; Harper, G.W. Overlooked, misunderstood and at-risk: Exploring the lives and HIV risk of ethnic minority male-to-female transgender youth. J. Adolesc. Health 2006, 38, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Ristori, J.; Rossi, E.; Cocchetti, C.; Mazzoli, F.; Castellini, G.; Vignozzi, L.; Ricca, V.; Maggi, M.; Fisher, A.D. Sexual habits among Italian transgender adolescents: A cross-sectional study. Int. J. Impot. Res. 2021, 33, 687–693. [Google Scholar] [CrossRef]
- Safren, S.A.; Reisner, S.L.; Herrick, A.; Mimiaga, M.J.; Stall, R.D. Mental Health and HIV Risk in Men Who Have Sex With Men. JAIDS J. Acquir. Immune Defic. Syndr. 2010, 55, S74–S77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, E.C.; Garofalo, R.; Harris, R.D.; Herrick, A.; Martinez, M.; Martinez, J.; Belzer, M. Transgender Female Youth and Sex Work: HIV Risk and a Comparison of Life Factors Related to Engagement in Sex Work. AIDS Behav. 2009, 13, 902–913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, N.; Hoenigl, M.; Morris, S.; Little, S.J. Risk Behavior and Sexually Transmitted Infections Among Transgender Women and Men Undergoing Community-Based Screening for Acute and Early HIV Infection in San Diego. Medicine 2015, 94, e1830. [Google Scholar] [CrossRef] [PubMed]
- Lyons, T.; Krüsi, A.; Pierre, L.; Kerr, T.; Small, W.; Shannon, K. Negotiating violence in the context of transphobia and criminalization: The experiences of trans sex workers in Vancouver, Canada. Qual. Health Res. 2017, 27, 182–190. [Google Scholar] [CrossRef] [Green Version]
- Lombardi, E.L.; Wilchins, R.A.; Priesing, D.; Malouf, D. Gender Violence. J. Homosex. 2002, 42, 89–101. [Google Scholar] [CrossRef]
- Reisner, S.L.; White, J.M.; Mayer, K.H.; Mimiaga, M.J. Sexual risk behaviors and psychosocial health concerns of female-to-male transgender men screening for STDs at an urban community health center. AIDS Care 2014, 26, 857–864. [Google Scholar] [CrossRef] [Green Version]
- Chakrapani, V.; Newman, P.A.; Shunmugam, M.; Logie, C.H.; Samuel, M. Syndemics of depression, alcohol use, and victimisation, and their association with HIV-related sexual risk among men who have sex with men and transgender women in India. Glob. Public Health 2015, 12, 250–265. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| All (n = 705) % (n) | At Least One STI (n = 48) % (n) | No STI (n = 657) % (n) | p | HR [95% Confidence Interval] | Adjusted p | |
|---|---|---|---|---|---|---|
| Age | 30.81 ± 10.09 | 39.42 ± 8.42 | 30.19 ± 9.92 | p < 0.0001 | ||
| Assigned gender at birth | ||||||
| AMAB | 53.5% (377) | 87.5% (42) | 51.0% (335) | p < 0.0001 | 5.436 [2.253–13.118] | p < 0.0001 |
| AFAB | 46.5% (328) | 12.5% (6) | 49.0% (322) | |||
| Gender affirming path | ||||||
| HT | 39.1% (276) | 83.0% (40) | 35.9% (236) | p < 0.0001 | 0.164 [0.074–0.363] | p < 0.0001 |
| GAS | 11.0% (78) | 25.0% (12) | 10.0% (66) | p = 0.001 | 1.574 [0.743–3.336] | p = 0.236 |
| Non-italian natives | 11.2% (79) | 31.3% (15) | 9.7% (64) | p < 0.0001 | 4.465 [2.229–8.943] | p < 0.0001 |
| Marital status | ||||||
| Unmarried | 91.6 (646) | 77.1% (37) | 92.7% (609) | p < 0.0001 | 0.515 [0.231–1.149] | p = 0.105 |
| Married | 3.1% (22) | 7.0% (3) | 2.9% (19) | p= 0.137 | 0.825 [0.207–3.291] | p = 0.785 |
| Divorced | 3.3% (23) | 4.7% (2) | 3.2% (21) | p = 0.606 | 0.741 [0.159–3.441] | p = 0.701 |
| Widowed | 0.3% (2) | 2.3% (1) | 0.2% (1) | p = 0.01 | 10.696 [0.530–215.9] | p = 0.122 |
| Parenthood | 5.4% (38) | 2.3% (1) | 5.6% (37) | p = 0.342 | 0.078 [0.010–0.638] | p = 0.017 |
| Education | ||||||
| Primary school | 26.5% (187) | 31.9% (15) | 26.1% (172) | p = 0.384 | 1.272 [0.657–2.461] | p = 0.476 |
| Secondary school/professional diploma | 58.7% (414) | 51.1% (25) | 59.3% (389) | p = 0.268 | 0.860 [0.465–1.592] | p = 0.632 |
| University | 14.8% (104) | 17.0% (8) | 14.6% (96) | p = 0.650 | 0.913 [0.399–2.089] | p = 0.830 |
| Employment | ||||||
| Student | 18.2% (128) | 0.0% (0) | 19.5% (128) | p = 0.001 | 0.000 [0.000-] | p = 0.996 |
| Employed | 58.1% (410) | 66.0% (32) | 57.5% (378) | p = 0.257 | 0.923 [0.479–1.781] | p = 0.811 |
| Retired | 1.7% (12) | 4.3% (2) | 1.5% (10) | p = 0.165 | 0.565 [0.103–3.095] | p = 0.511 |
| Unemployed | 23.9% (168) | 34.0% (16) | 23.2% (152) | p = 0.091 | 2.152 [1.109–4.175] | p = 0.023 |
| Living status | ||||||
| With family | 45.9% (324) | 12.8% (6) | 48.3% (318) | p < 0.0001 | 0.268 [0.108–0.668] | p = 0.005 |
| With partner | 18.7% (132) | 21.3% (10) | 18.5% (122) | p = 0.636 | 0.788 [0.368–1.688] | p = 0.54 |
| With flatmate | 11.4% (80) | 14.9% (7) | 11.1% (73) | p = 0.428 | 1.864 [0.776–4.476] | p = 0.164 |
| Alone | 23.1% (163) | 42.6% (20) | 21.7% (143) | p = 0.001 | 1.552 [0.807–2.985] | p = 0.188 |
| Institute | 1.0% (7) | 4.2% (2) | 0.8% (5) | p = 0.03 | 5.292 [0.90–31.129] | p = 0.065 |
| Prison | 0.6% (4) | 4.2% (2) | 0.3% (2) | p = 0.001 | 9.614 [1.242–74.398] | p = 0.03 |
| Previous incarceration | 2.1% (15) | 12.5% (6) | 1.4% (9) | p < 0.0001 | 8.118 [2.352–28.022] | p = 0.001 |
| Sex work | 10.8% (76) | 59.3% (28) | 7.3% (48) | p < 0.0001 | 14.196 [6.719–29.991] | p < 0.0001 |
| Justice problems | 9.4% (66) | 35.1% (17) | 7.5% (49) | p < 0.0001 | 4.716 [2.168–10.258] | p < 0.0001 |
| All (n = 705) % (n) | At Least One STI (n = 48) % (n) | No STI (n = 657) % (n) | p | HR [95% Confidence Interval] | Adjusted p | |
|---|---|---|---|---|---|---|
| Smoking status | ||||||
| Ex-smoker | 15.7% (111) | 13.0% (6) | 15.9% (104) | p = 0.610 | 0.664 [0.267–1.653] | p = 0.379 |
| Current smoker | 45.5% (321) | 54.3% (26) | 44.9% (295) | p = 0.215 | 1.435 [0.772–2.668] | p = 0.253 |
| Comorbilities | ||||||
| Cardiovascular disease | 1.6% (11) | 4.3% (2) | 1.4% (9) | p = 0.128 | 1.525 [0.297–7.829] | p = 0.613 |
| Diabetes | 1.1% (8) | 2.1% (1) | 1.1% (7) | p = 0.512 | 1.389 [0.149–12.970] | p = 0.773 |
| Dyslipidemia | 1.4% (10) | 2.1% (1) | 1.2% (8) | p = 0.598 | 0.861 [0.101–7.322] | p = 0.891 |
| Hypertension | 2.1% (15) | 4.3% (2) | 2.0% (13) | p = 0.301 | 0.944 [0.195–4.572] | p = 0.943 |
| Cerebrovascular disease | 0.4% (3) | 0.0% (0) | 0.5% (3) | p = 0.641 | 0.000 [0.000-] | p = 0.999 |
| Current medication use | 2.7% (19) | 4.3% (2) | 2.6% (17) | p = 0.501 | 2.808 [0.597–13.212] | p = 0.191 |
| Alcohol consumption * | 1.8% (13) | 2.2% (1) | 1.9% (12) | p = 0.885 | 1.01 [0.122–8.343] | p = 0.993 |
| Lifetime substance abuse | 31.4% (221) | 50.0% (24) | 30.0% (197) | p = 0.003 | 2.552 [1.374–4.740] | p = 0.003 |
| Alcohol | 11.9% (84) | 8.3% (4) | 12.2% (80) | p = 0.492 | 0.788 [0.231–2.692] | p = 0.704 |
| Cannabis | 19.4% (137) | 22.9% (11) | 19.2% (126) | p = 0.668 | 1.504 [0.651–3.477] | p = 0.339 |
| Opiates | 3.1% (22) | 18.7% (9) | 2.0% (13) | p < 0.0001 | 8.673 [3.115–24.147] | p < 0.0001 |
| Cocaine | 8.8% (62) | 27.1% (13) | 7.5% (49) | p < 0.0001 | 4.608 [2.046–10.378] | p < 0.0001 |
| Hallucinogens | 2.1% (15) | 2.1% (1) | 2.1% (14) | p = 0.794 | 1.191 [0.148–9.573] | p = 0.870 |
| Ketamine | 1.1% (8) | 0.0% (0) | 1.2% (8) | p = 0.517 | 0.000 [0.000-] | p = 0.999 |
| Psychiatric disorders in the family | 27.7% (195) | 25.5% (12) | 27.8% (183) | p = 0.730 | 0.946 [0.470–1.903] | p = 0.876 |
| Sexual abuse | ||||||
| Childhood | 6.8% (48) | 6.4% (3) | 6.9% (45) | p = 0.886 | 0.757 [0.220–2.603] | p = 0.659 |
| Adolescence | 4.7% (33) | 14.9% (7) | 4.0% (26) | p = 0.001 | 4.178 [1.642–10.626] | p = 0.003 |
| Self-harming behaviors | 28.0% (197) | 29.2% (14) | 27.8% (183) | p = 0.705 | 1.350 [0.687–2.652] | p = 0.384 |
| Bullying | ||||||
| Childhood | 15.0% (106) | 8.3% (4) | 15.5% (102) | p = 0.215 | 0.693 [0.237–2.026] | p = 0.503 |
| Adolescence | 17.3% (122) | 6.5% (3) | 18.1% (119) | p = 0.046 | 0.519 [0.154–1.749] | p = 0.290 |
| Suicidal ideation | 51.9% (366) | 58.3% (28) | 51.4% (338) | p = 0.283 | 1.529 [0.819–2.857] | p = 0.183 |
| Current psychiatric medications | 11.3% (80) | 25.0% (12) | 10.3% (68) | p = 0.002 | 2.579 [1.237–5.380] | p = 0.012 |
| Antidepressants | 6.5% (46) | 8.3% (4) | 6.4% (42) | p = 0.555 | 1.108 [0.367–3.345] | p = 0.856 |
| Antipsychotics | 1.4% (10) | 2.1% (1) | 1.4% (9) | p = 0.680 | 1.249 [0.143–10.936] | p = 0.841 |
| Mood stabilizers | 2.6% (18) | 4.2% (2) | 2.4% (16) | p = 0.457 | 1.728 [0.349–8.556] | p = 0.503 |
| Benzodiazepines | 4.5% (32) | 12.5% (6) | 4.0% (26) | p = 0.006 | 3.072 [1.157–8.155] | p = 0.024 |
| Lifetime psychiatric disorders | 21.5% (152) | 37.5% (18) | 20.4% (134) | p = 0.010 | 1.988 [1.013–3.901] | p = 0.046 |
| GAD | 2.0% (14) | 0.0% (0) | 2.1% (14) | p = 0.339 | 0.000 [0.000-] | p = 0.999 |
| Depression | 16.0% (113) | 33.3% (16) | 14.8% (97) | p = 0.002 | 2.329 [1.154–4.701] | p = 0.018 |
| Dysthymia | 0.1% (1) | 0.0% (0) | 0.2% (1) | p = 0.790 | 0.000 [0.000-] | p = 1.000 |
| Bipolar disorder | 1.1% (8) | 0.0% (0) | 1.2% (8) | p = 0.479 | 0.000 [0.000-] | p = 0.999 |
| Panic disorder | 4.3% (30) | 2.1% (1) | 4.4% (29) | p = 0.510 | 0.368 [0.047–2.882] | p = 0.341 |
| Sociophobia | 0.4% (3) | 0.0% (0) | 0.5% (3) | p = 0.644 | 0.000 [0.000-] | p = 0.999 |
| PTSD | 0.3% (2) | 0.0% (0) | 0.3% (2) | p = 0.706 | 0.000 [0.000-] | p = 0.999 |
| OCD | 0.9% (6) | 0.0% (0) | 0.9% (6) | p = 0.513 | 0.000 [0.000-] | p = 0.999 |
| Any personality disorder | 0.6% (4) | 4.2% (2) | 0.3% (2) | p < 0.0001 | 13.176 [1.582–109.719] | p = 0.017 |
| Anorexia nervosa | 0.9% (6) | 2.1% (1) | 0.8% (5) | p = 0.319 | 4.585 [0.467–45.068] | p = 0.192 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cocchetti, C.; Romani, A.; Mazzoli, F.; Ristori, J.; Lagi, F.; Meriggiola, M.C.; Motta, G.; Pierdominici, M.; Bartoloni, A.; Vignozzi, L.; et al. Prevalence and Correlates of Sexually Transmitted Infections in Transgender People: An Italian Multicentric Cross-Sectional Study. J. Clin. Med. 2022, 11, 2774. https://doi.org/10.3390/jcm11102774
Cocchetti C, Romani A, Mazzoli F, Ristori J, Lagi F, Meriggiola MC, Motta G, Pierdominici M, Bartoloni A, Vignozzi L, et al. Prevalence and Correlates of Sexually Transmitted Infections in Transgender People: An Italian Multicentric Cross-Sectional Study. Journal of Clinical Medicine. 2022; 11(10):2774. https://doi.org/10.3390/jcm11102774
Chicago/Turabian StyleCocchetti, Carlotta, Alessia Romani, Francesca Mazzoli, Jiska Ristori, Filippo Lagi, Maria Cristina Meriggiola, Giovanna Motta, Marina Pierdominici, Alessandro Bartoloni, Linda Vignozzi, and et al. 2022. "Prevalence and Correlates of Sexually Transmitted Infections in Transgender People: An Italian Multicentric Cross-Sectional Study" Journal of Clinical Medicine 11, no. 10: 2774. https://doi.org/10.3390/jcm11102774
APA StyleCocchetti, C., Romani, A., Mazzoli, F., Ristori, J., Lagi, F., Meriggiola, M. C., Motta, G., Pierdominici, M., Bartoloni, A., Vignozzi, L., Maggi, M., & Fisher, A. D. (2022). Prevalence and Correlates of Sexually Transmitted Infections in Transgender People: An Italian Multicentric Cross-Sectional Study. Journal of Clinical Medicine, 11(10), 2774. https://doi.org/10.3390/jcm11102774