
A Compound Hop Index for Assessing Soccer Players’ Performance

 ,
,  ,
,  ,
,  , ,
, ,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Test–Retest Reliability of the Compound Hop Index
2.2. Participants
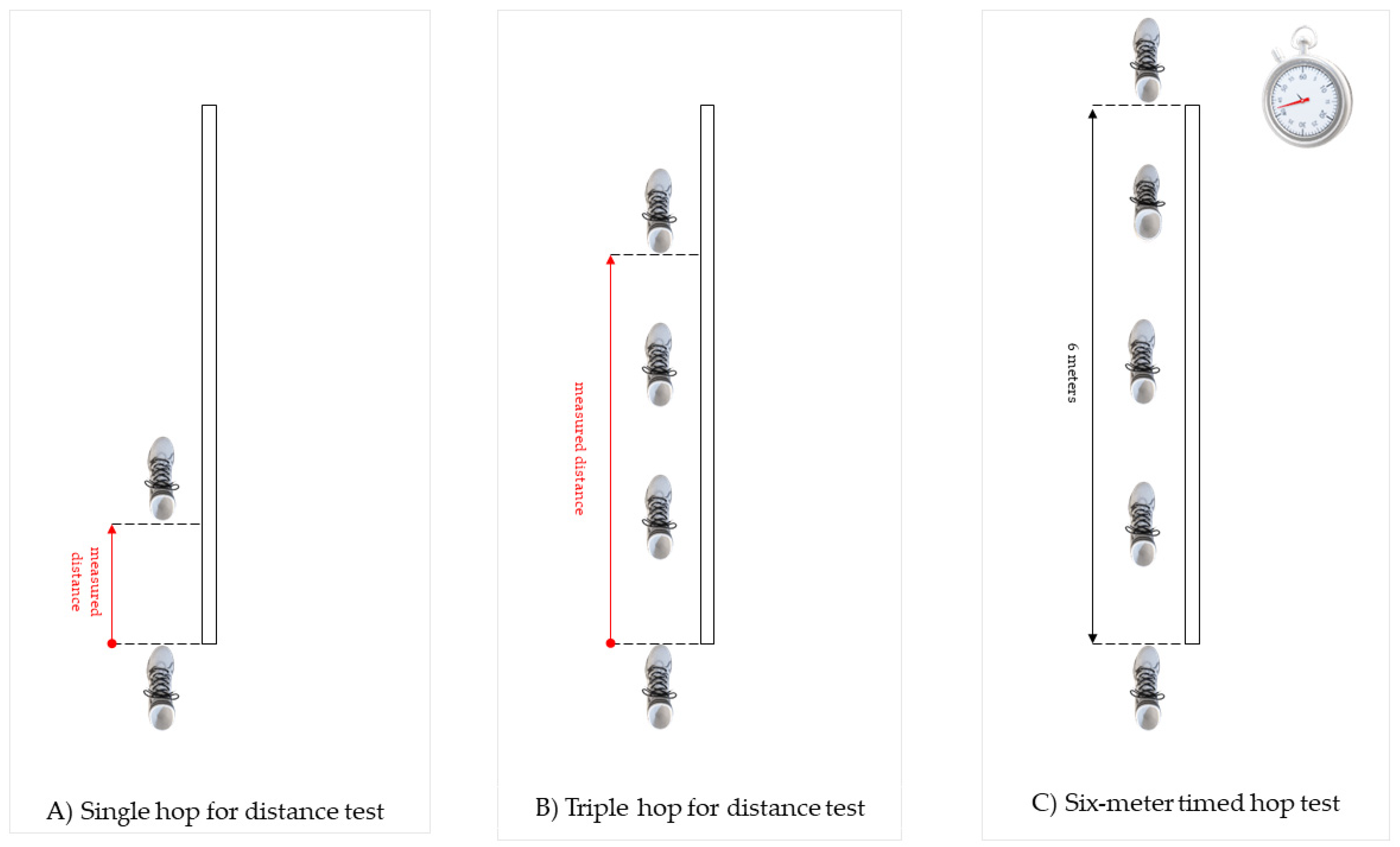
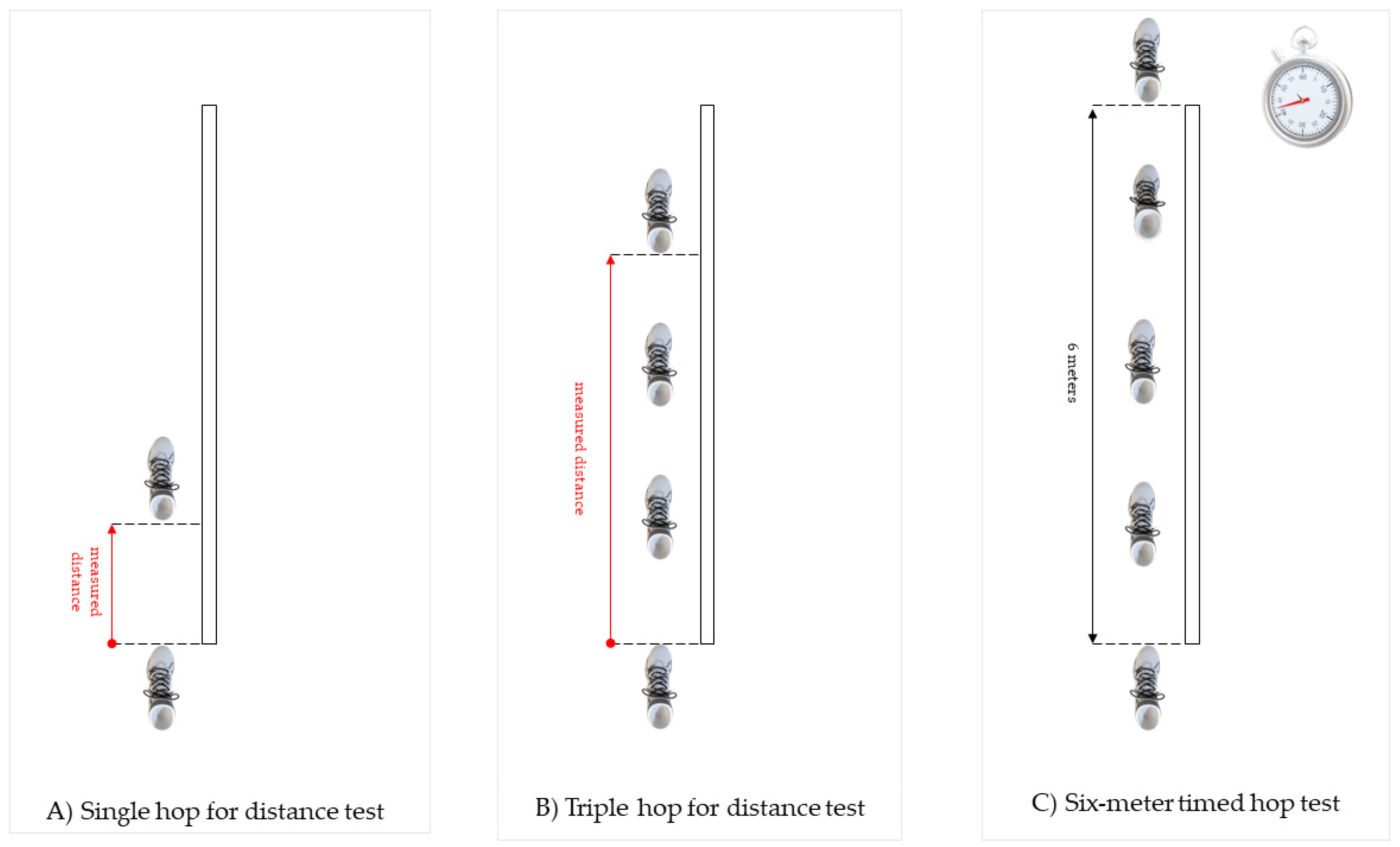
2.3. Single-Leg Hop Tests Battery
2.4. Calculation of the Compound Hop Index
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Madsen, L.P.; Booth, R.L.; Volz, J.D.; Docherty, C.L. Using normative data and unilateral hopping tests to reduce ambiguity in return-to-play decisions. J. Athl. Train. 2020, 55, 699–706. [Google Scholar] [CrossRef]
- Turner, A. Total score of athleticism: A strategy for assessing an athlete’s athleticism. Prof. Strength Cond. 2014, 33, 13–17. [Google Scholar]
- Turner, A.N.; Jones, B.; Stewart, P.; Bishop, C.; Parmar, N.; Chavda, S.; Read, P. Total score of athleticism: Holistic athlete profiling to enhance decision-making. Strength Cond. J. 2019, 41, 91–101. [Google Scholar] [CrossRef]
- Ebert, J.R.; Du Preez, L.; Furzer, B.; Edwards, P.; Joss, B. Which hop tests can best identify functional limb asymmetry in patients 9-12 months after anterior cruciate ligament reconstruction employing a hamstrings tendon autograft? Int. J. Sports Phys. Ther. 2021, 16, 393–403. [Google Scholar] [CrossRef] [PubMed]
- Grindem, H.; Snyder-Mackler, L.; Moksnes, H.; Engebretsen, L.; Risberg, M.A. Simple decision rules can reduce reinjury risk by 84% after acl reconstruction: The delaware-oslo acl cohort study. Br. J. Sports Med. 2016, 50, 804–808. [Google Scholar] [CrossRef]
- Kyritsis, P.; Bahr, R.; Landreau, P.; Miladi, R.; Witvrouw, E. Likelihood of acl graft rupture: Not meeting six clinical discharge criteria before return to sport is associated with a four times greater risk of rupture. Br. J. Sports Med. 2016, 50, 946–951. [Google Scholar] [CrossRef] [PubMed]
- Reid, A.; Birmingham, T.B.; Stratford, P.W.; Alcock, G.K.; Giffin, J.R. Hop testing provides a reliable and valid outcome measure during rehabilitation after anterior cruciate ligament reconstruction. Phys. Ther. 2007, 87, 337–349. [Google Scholar] [CrossRef] [Green Version]
- Gokeler, A.; Welling, W.; Benjaminse, A.; Lemmink, K.; Seil, R.; Zaffagnini, S. A critical analysis of limb symmetry indices of hop tests in athletes after anterior cruciate ligament reconstruction: A case control study. Orthop. Traumatol. Surg. Res. 2017, 103, 947–951. [Google Scholar] [CrossRef] [PubMed]
- Zwolski, C.; Schmitt, L.C.; Thomas, S.; Hewett, T.E.; Paterno, M.V. The utility of limb symmetry indices in return-to-sport assessment in patients with bilateral anterior cruciate ligament reconstruction. Am. J. Sports Med. 2016, 44, 2030–2038. [Google Scholar] [CrossRef]
- Patterson, B.E.; Crossley, K.M.; Perraton, L.G.; Kumar, A.S.; King, M.G.; Heerey, J.J.; Barton, C.J.; Culvenor, A.G. Limb symmetry index on a functional test battery improves between one and five years after anterior cruciate ligament reconstruction, primarily due to worsening contralateral limb function. Phys. Ther. Sport 2020, 44, 67–74. [Google Scholar] [CrossRef]
- Ohji, S.; Aizawa, J.; Hirohata, K.; Ohmi, T.; Mitomo, S.; Jinno, T.; Koga, H.; Yagishita, K. Single-leg hop distance normalized to body height is associated with the return to sports after anterior cruciate ligament reconstruction. J. Exp. Orthop. 2021, 8, 26. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, E.M.; Dyke, J.; Karl, M.; Leung, A.; Lawrence, J.T.; Ganley, T. Limb symmetry is not enough: Establishment of height normalized hop distances within healthy youth athletes. Orthop. J. Sports Med. 2020, 8 (Suppl. S3), 2325967120S00190. [Google Scholar] [CrossRef]
- Narducci, E.; Waltz, A.; Gorski, K.; Leppla, L.; Donaldson, M. The clinical utility of functional performance tests within one-year post-acl reconstruction: A systematic review. Int. J. Sports Phys. Ther. 2011, 6, 333–342. [Google Scholar] [PubMed]
- Ebert, J.R.; Edwards, P.; Currie, J.; Smith, A.; Joss, B.; Ackland, T.; Buelow, J.U.; Hewitt, B. Comparison of the ‘back in action’ test battery to standard hop tests and isokinetic knee dynamometry in patients following anterior cruciate ligament reconstruction. Int. J. Sports Phys. Ther. 2018, 13, 389–400. [Google Scholar] [CrossRef] [Green Version]
- Scinicarelli, G.; Trofenik, M.; Froböse, I.; Wilke, C. The reliability of common functional performance tests within an experimental test battery for the lower extremities. Sports 2021, 9, 100. [Google Scholar] [CrossRef]
- Ross, M.D.; Langford, B.; Whelan, P.J. Test-retest reliability of 4 single-leg horizontal hop tests. J. Strength Cond. Res. 2002, 16, 617–622. [Google Scholar]
- Hopper, D.M.; Goh, S.C.; Wentworth, L.A.; Chan, D.Y.K.; Chau, J.H.W.; Wootton, G.J.; Strauss, G.R.; Boyle, J.J.W. Test–retest reliability of knee rating scales and functional hop tests one year following anterior cruciate ligament reconstruction. Phys. Ther. Sport 2002, 3, 10–18. [Google Scholar] [CrossRef]
- Brosky, J.A., Jr.; Nitz, A.J.; Malone, T.R.; Caborn, D.N.; Rayens, M.K. Intrarater reliability of selected clinical outcome measures following anterior cruciate ligament reconstruction. J. Orthop. Sports Phys. Ther. 1999, 29, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Hewett, T.E.; Webster, K.E.; Hurd, W.J. Systematic selection of key logistic regression variables for risk prediction analyses: A five-factor maximum model. Clin. J. Sport Med. 2019, 29, 78–85. [Google Scholar] [CrossRef]
- Webster, K.E.; Feller, J.A. Who passes return-to-sport tests, and which tests are most strongly associated with return to play after anterior cruciate ligament reconstruction? Orthop. J. Sports Med. 2020, 8, 2325967120969425. [Google Scholar] [CrossRef] [PubMed]
- McMulkin, M.L.; MacWilliams, B.A. Application of the gillette gait index, gait deviation index and gait profile score to multiple clinical pediatric populations. Gait Posture 2015, 41, 608–612. [Google Scholar] [CrossRef]
- Schutte, L.M.; Narayanan, U.; Stout, J.L.; Selber, P.; Gage, J.R.; Schwartz, M.H. An index for quantifying deviations from normal gait. Gait Posture 2000, 11, 25–31. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, M.H.; Rozumalski, A. The gait deviation index: A new comprehensive index of gait pathology. Gait Posture 2008, 28, 351–357. [Google Scholar] [CrossRef]
- Baker, R.; McGinley, J.L.; Schwartz, M.H.; Beynon, S.; Rozumalski, A.; Graham, H.K.; Tirosh, O. The gait profile score and movement analysis profile. Gait Posture 2009, 30, 265–269. [Google Scholar] [CrossRef] [PubMed]
- Prill, R.; Michel, S.; Schulz, R.; Coriolano, H.A. Body composition and strength parameters in elite judo athletes 5 years after anterior cruciate ligament reconstruction. Int. J. Sports Med. 2019, 40, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Oleksy, Ł.; Mika, A.; Królikowska, A.; Kuchciak, M.; Stolarczyk, M.; Kielnar, R.; Racheniuk, H.; Szczegielniak, J.; Łuszczki, E.; Stolarczyk, A. Composite score of readiness (csr) as holistic profiling of functional deficits in footballers following acl reconstruction. J. Clin. Med. 2021, 10, 3670. [Google Scholar] [CrossRef] [PubMed]
- Wing, C.E.; Turner, A.N.; Bishop, C.J. Importance of strength and power on key performance indicators in elite youth soccer. J. Strength Cond. Res. 2020, 34, 2006–2014. [Google Scholar] [CrossRef]
- Burgi, C.R.; Peters, S.; Ardern, C.L.; Magill, J.R.; Gomez, C.D.; Sylvain, J.; Reiman, M.P. Which criteria are used to clear patients to return to sport after primary acl reconstruction? A scoping review. Br. J. Sports Med. 2019, 53, 1154. [Google Scholar] [CrossRef]
- Grassi, A.; Quaglia, A.; Canata, G.L.; Zaffagnini, S. An update on the grading of muscle injuries: A narrative review from clinical to comprehensive systems. Joints 2016, 4, 39–46. [Google Scholar] [CrossRef] [Green Version]
- Nuhu, A.; Jelsma, J.; Dunleavy, K.; Burgess, T. Effect of the fifa 11+ soccer specific warm up programme on the incidence of injuries: A cluster-randomised controlled trial. PLoS ONE 2021, 16, e0251839. [Google Scholar] [CrossRef]
- Noyes, F.R.; Barber, S.D.; Mangine, R.E. Abnormal lower limb symmetry determined by function hop tests after anterior cruciate ligament rupture. Am. J. Sports Med. 1991, 19, 513–518. [Google Scholar] [CrossRef]
- Munro, A.G.; Herrington, L.C. Between-session reliability of four hop tests and the agility t-test. J. Strength Cond. Res. 2011, 25, 1470–1477. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, S.W.; Fleet, N.A.; Brooks, V.A.; Bido, J.; Nwachukwu, B.U.; Brubaker, P.H. Comparison of different functional tests for leg power and normative bilateral asymmetry index in healthy collegiate athletes. Open Access J. Sports Med. 2021, 12, 119–128. [Google Scholar] [CrossRef]
- Ceroni, D.; Martin, X.E.; Delhumeau, C.; Farpour-Lambert, N.J. Bilateral and gender differences during single-legged vertical jump performance in healthy teenagers. J. Strength Cond. Res. 2012, 26, 452–457. [Google Scholar] [CrossRef] [PubMed]
- Mukaka, M.M. Statistics corner: A guide to appropriate use of correlation coefficient in medical research. Malawi Med. J. 2012, 24, 69–71. [Google Scholar] [PubMed]
- Wilk, K.E.; Romaniello, W.T.; Soscia, S.M.; Arrigo, C.A.; Andrews, J.R. The relationship between subjective knee scores, isokinetic testing, and functional testing in the acl-reconstructed knee. J. Orthop. Sports Phys. Ther. 1994, 20, 60–73. [Google Scholar] [CrossRef] [PubMed]
- Ageberg, E.; Zätterström, R.; Fridén, T.; Moritz, U. Individual factors affecting stabilometry and one-leg hop test in 75 healthy subjects, aged 15-44 years. Scand. J. Med. Sci. Sports 2001, 11, 47–53. [Google Scholar] [CrossRef]
- Tegner, Y.; Lysholm, J.; Lysholm, M.; Gillquist, J. A performance test to monitor rehabilitation and evaluate anterior cruciate ligament injuries. Am. J. Sports Med. 1986, 14, 156–159. [Google Scholar] [CrossRef]
- Paterno, M.V.; Greenberger, H.B. The test-retest reliability of a one legged hop for distance in young adults with and without acl reconstruction. Isokinet. Exerc. Sci. 1996, 6, 1–6. [Google Scholar] [CrossRef]
- Nawasreh, Z.; Logerstedt, D.; Cummer, K.; Axe, M.; Risberg, M.A.; Snyder-Mackler, L. Functional performance 6 months after acl reconstruction can predict return to participation in the same preinjury activity level 12 and 24 months after surgery. Br. J. Sports Med. 2018, 52, 375. [Google Scholar] [CrossRef]
- Davies, W.T.; Myer, G.D.; Read, P.J. Is it time we better understood the tests we are using for return to sport decision making following acl reconstruction? A critical review of the hop tests. Sports Med. 2020, 50, 485–495. [Google Scholar] [PubMed] [Green Version]
- Toole, A.R.; Ithurburn, M.P.; Rauh, M.J.; Hewett, T.E.; Paterno, M.V.; Schmitt, L.C. Young athletes cleared for sports participation after anterior cruciate ligament reconstruction: How many actually meet recommended return-to-sport criterion cutoffs? J. Orthop. Sports Phys. Ther. 2017, 47, 825–833. [Google Scholar] [CrossRef] [Green Version]
- Vereijken, A.; van Trijffel, E.; Aerts, I.; Tassignon, B.; Verschueren, J.; Meeusen, R. The non-injured leg can be used as a reference for the injured leg in single-legged hop tests. Int. J. Sports Phys. Ther. 2021, 16, 1052–1066. [Google Scholar] [CrossRef] [PubMed]
- Edwards, P.K.; Ebert, J.R.; Joss, B.; Ackland, T.; Annear, P.; Buelow, J.U.; Hewitt, B. Patient characteristics and predictors of return to sport at 12 months after anterior cruciate ligament reconstruction: The importance of patient age and postoperative rehabilitation. Orthop. J. Sports Med. 2018, 6, 2325967118797575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benjaminse, A.; Holden, S.; Myer, G.D. Acl rupture is a single leg injury but a double leg problem: Too much focus on ‘symmetry’ alone and that’s not enough! Br. J. Sports Med. 2018, 52, 1029–1030. [Google Scholar] [CrossRef] [PubMed]
- Welling, W.; Benjaminse, A.; Seil, R.; Lemmink, K.; Gokeler, A. Altered movement during single leg hop test after acl reconstruction: Implications to incorporate 2-d video movement analysis for hop tests. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 3012–3019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaminski, T.W.; Hertel, J.; Amendola, N.; Docherty, C.L.; Dolan, M.G.; Hopkins, J.T.; Nussbaum, E.; Poppy, W.; Richie, D. National athletic trainers’ association position statement: Conservative management and prevention of ankle sprains in athletes. J. Athl. Train. 2013, 48, 528–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myer, G.D.; Paterno, M.V.; Ford, K.R.; Quatman, C.E.; Hewett, T.E. Rehabilitation after anterior cruciate ligament reconstruction: Criteria-based progression through the return-to-sport phase. J. Orthop. Sports Phys. Ther. 2006, 36, 385–402. [Google Scholar] [CrossRef] [Green Version]
- Fitzgerald, G.K.; Lephart, S.M.; Hwang, J.H.; Wainner, R.S. Hop tests as predictors of dynamic knee stability. J. Orthop. Sports Phys. Ther. 2001, 31, 588–597. [Google Scholar] [CrossRef] [Green Version]
- Lisee, C.; Slater, L.; Hertel, J.; Hart, J.M. Effect of sex and level of activity on lower-extremity strength, functional performance, and limb symmetry. J. Sport Rehabil. 2019, 28, 413–420. [Google Scholar] [CrossRef]
- Wellsandt, E.; Failla, M.J.; Snyder-Mackler, L. Limb symmetry indexes can overestimate knee function after anterior cruciate ligament injury. J. Orthop. Sports Phys. Ther. 2017, 47, 334–338. [Google Scholar] [CrossRef] [Green Version]
- Till, K.; Jones, B.L.; Cobley, S.; Morley, D.; O’Hara, J.; Chapman, C.; Cooke, C.; Beggs, C.B. Identifying talent in youth sport: A novel methodology using higher-dimensional analysis. PLoS ONE 2016, 11, e0155047. [Google Scholar] [CrossRef] [PubMed]
- Sonesson, S.; Lindblom, H.; Hägglund, M. Performance on sprint, agility and jump tests have moderate to strong correlations in youth football players but performance tests are weakly correlated to neuromuscular control tests. Knee Surg. Sports Traumatol. Arthrosc. 2020, 29, 1659–1669. [Google Scholar] [CrossRef] [PubMed]
- Myers, B.A.; Jenkins, W.L.; Killian, C.; Rundquist, P. Normative data for hop tests in high school and collegiate basketball and soccer players. Int. J. Sports Phys. Ther. 2014, 9, 596–603. [Google Scholar] [PubMed]
- Sueyoshi, T.; Nakahata, A.; Emoto, G.; Yuasa, T. Single-leg hop test performance and isokinetic knee strength after anterior cruciate ligament reconstruction in athletes. Orthop. J. Sports Med. 2017, 5, 2325967117739811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xergia, S.A.; Pappas, E.; Georgoulis, A.D. Association of the single-limb hop test with isokinetic, kinematic, and kinetic asymmetries in patients after anterior cruciate ligament reconstruction. Sports Health 2015, 7, 217–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kollock, R.; Van Lunen, B.L.; Ringleb, S.I.; Oñate, J.A. Measures of functional performance and their association with hip and thigh strength. J. Athl. Train. 2015, 50, 14–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grooms, D.R.; Myer, G.D. Upgraded hardware─what about the software? Brain updates for return to play following acl reconstruction. Br. J. Sports Med. 2017, 51, 418–419. [Google Scholar]
- Grooms, D.R.; Page, S.J.; Nichols-Larsen, D.S.; Chaudhari, A.M.; White, S.E.; Onate, J.A. Neuroplasticity associated with anterior cruciate ligament reconstruction. J. Orthop. Sports Phys. Ther. 2017, 47, 180–189. [Google Scholar] [CrossRef] [PubMed]
- Swanik, C.B. Brains and sprains: The brain’s role in noncontact anterior cruciate ligament injuries. J. Athl. Train. 2015, 50, 1100–1102. [Google Scholar] [CrossRef] [Green Version]
- Millikan, N.; Grooms, D.R.; Hoffman, B.; Simon, J.E. The development and reliability of 4 clinical neurocognitive single-leg hop tests: Implications for return to activity decision-making. J. Sport Rehabil. 2019, 28, 536–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| Analyzed Parameter | Studied Leg | x | SD |
|---|---|---|---|
| Normalized single-hop test distance (m*m−1) | Right | 1.18 | 0.10 |
| Left | 1.19 | 0.11 | |
| LSI | 96.46 | 3.53 | |
| Normalized triple-hop test distance (m*m−1) | Right | 3.80 | 0.26 |
| Left | 3.82 | 0.31 | |
| LSI | 95.56 | 3.50 | |
| Time of the six-meter timed hop test (s) | Right | 1.41 | 0.11 |
| Left | 1.41 | 0.13 | |
| LSI | 95.03 | 5.10 |
| Analyzed Test | Right-Leg Normalized Distance * or Time ** | Left-Leg Normalized Distance * or Time ** |
|---|---|---|
| Single-hop test distance LSI | p = 0.029; r = 0.333 | p = 0.164; r = 0.216 |
| Triple-hop test distance LSI | p = 0.837; r = 0.032 | p = 0.448; r = 0.119 |
| Six-meter timed hop test LSI | p = 0.056; r = −0.294 | p ≤ 0.001; r = −0.528 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oleksy, Ł.; Królikowska, A.; Mika, A.; Kuchciak, M.; Szymczyk, D.; Rzepko, M.; Bril, G.; Prill, R.; Stolarczyk, A.; Reichert, P. A Compound Hop Index for Assessing Soccer Players’ Performance. J. Clin. Med. 2022, 11, 255. https://doi.org/10.3390/jcm11010255
Oleksy Ł, Królikowska A, Mika A, Kuchciak M, Szymczyk D, Rzepko M, Bril G, Prill R, Stolarczyk A, Reichert P. A Compound Hop Index for Assessing Soccer Players’ Performance. Journal of Clinical Medicine. 2022; 11(1):255. https://doi.org/10.3390/jcm11010255
Chicago/Turabian StyleOleksy, Łukasz, Aleksandra Królikowska, Anna Mika, Maciej Kuchciak, Daniel Szymczyk, Marian Rzepko, Grzegorz Bril, Robert Prill, Artur Stolarczyk, and Paweł Reichert. 2022. "A Compound Hop Index for Assessing Soccer Players’ Performance" Journal of Clinical Medicine 11, no. 1: 255. https://doi.org/10.3390/jcm11010255
APA StyleOleksy, Ł., Królikowska, A., Mika, A., Kuchciak, M., Szymczyk, D., Rzepko, M., Bril, G., Prill, R., Stolarczyk, A., & Reichert, P. (2022). A Compound Hop Index for Assessing Soccer Players’ Performance. Journal of Clinical Medicine, 11(1), 255. https://doi.org/10.3390/jcm11010255