
Short Plate with Screw Angle over 20 Degrees Improves the Radiologic Outcome in ACDF: Clinical Study

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Surgical Indication and Technique
2.2. Evaluation of Radiologic Outcomes
- C2–7 Cervical Lordosis (CL): Cobb’s Method. This was measured by the angle formed by the perpendicular lines parallel to the inferior endplates of C2 and C7 [12].
- C2–7 Sagittal Vertical Axis (SVA): the distance between the C2 plumb line and the posterosuperior corner of C7 [12].
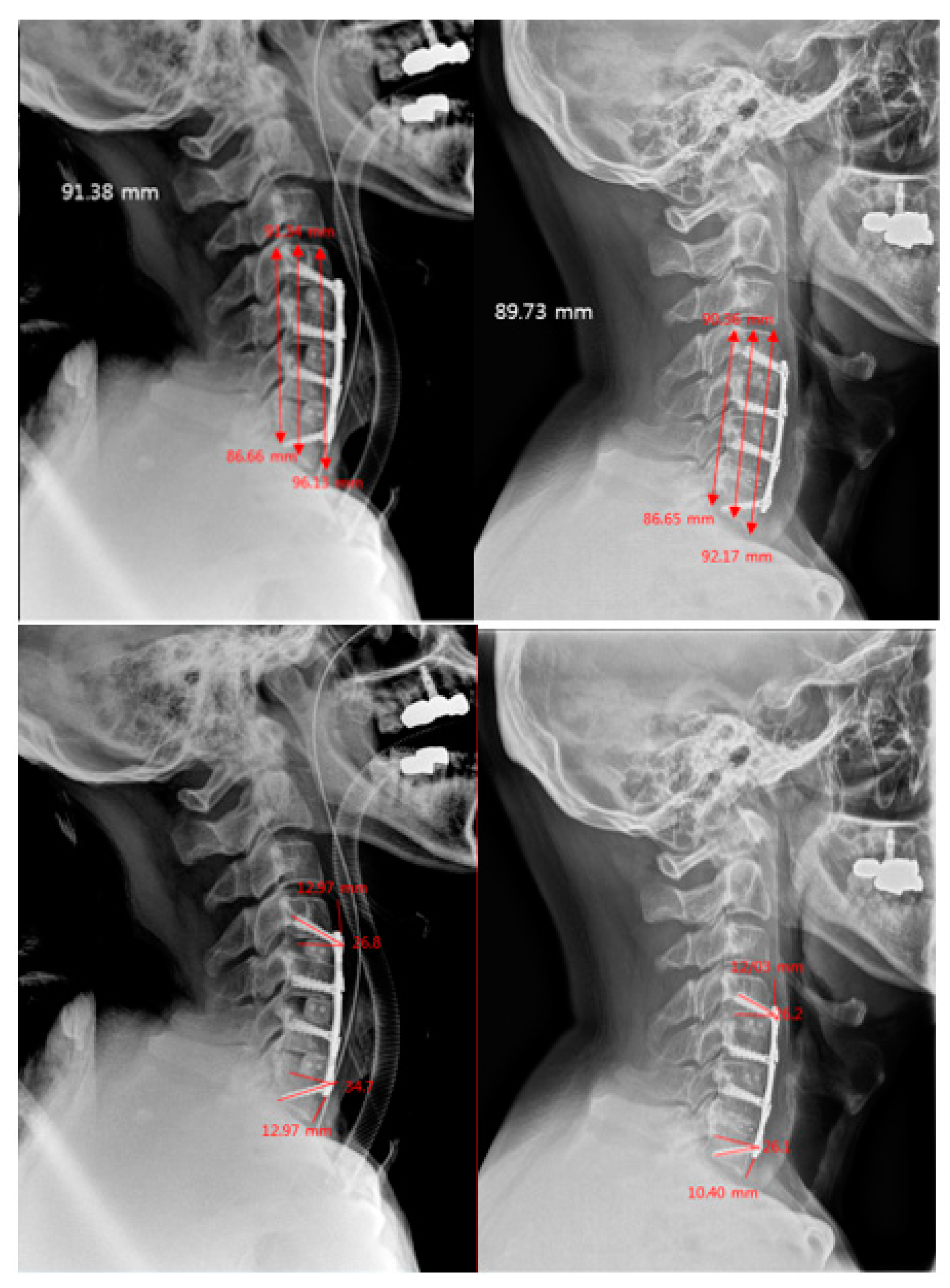
- Plate-to-Disc Distance: distance from the most proximal part and most distal part of the plate to the superior and inferior adjacent disc spaces, respectively [13].
- Screw Angles: angle between a line perpendicular to the plate and the direction of the screw [6].
- Subsidence: the vertical length from the superior endplate of the most superior vertebra to the inferior endplate of the most inferior vertebra [14].
2.3. Statistical Analysis
3. Results
3.1. Cervical Spine Sagittal Balance
3.2. Subsidence and Adjacent Level Ossified Disease (ALOD)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yuen, J.; Whitfield, P. Anterior Cervical Discectomy and Fusion (ACDF) for Degenerative Cervical Diseases—Six Decades on. ACNR 2017, 17, 5–10. [Google Scholar]
- Alimi, M.; Njoku, I.; Hofstetter, C.P.; Tsiouris, A.J.; Kesavabhotla, K.; Boockvar, J.; Navarro-Ramirez, R.; Härtl, R. Anterior Cervical Discectomy and Fusion (ACDF): Comparison Between Zero Profile Implants and Anterior Cervical Plate and Spacer. Cureus 2016, 8, e573. [Google Scholar] [CrossRef]
- Noordhoekl, I.; Koning, M.T.; Jacobs, W.C.H.; Vleggeert-Lankamp, C.L.A. Incidence and clinical relevance of cage subsidence in anterior cervical discectomy and fusion: A systematic review. Acta Neurochir. 2018, 160, 873–880. [Google Scholar] [CrossRef] [PubMed]
- Schmieder, K.; Wolzik-Grossmann, M.; Pechlivanis, I.; Engelhardt, M.; Scholz, M.; Harders, A. Subsidence of the wing titanium cage after anterior cervical interbody fusion: 2-year follow-up study. J. Neurosurg. Spine 2006, 4, 447–453. [Google Scholar] [CrossRef]
- Yang, J.J.; Yu, C.H.; Chang, B.S.; Yeom, J.S.; Lee, J.H.; Lee, C.K. Subsidence and nonunion after anterior cervical interbody fusion using a stand-alone polyetheretherketone (PEEK) cage. Clin. Orthop. Surg. 2011, 3, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Kwon, J.W.; Bang, S.H.; Kwon, Y.W.; Cho, J.Y.; Park, T.H.; Lee, S.J.; Lee, H.M.; Moon, S.H.; Lee, B.H. Biomechanical comparison of the angle if inserted screws and the length of anterior cervical plate systems with allograft spacers. Clin. Biomech. 2020, 76, 105021. [Google Scholar] [CrossRef] [PubMed]
- Kwon, J.-W.; Lee, H.-M.; Park, T.-H.; Lee, S.J.; Kwon, Y.-W.; Moon, S.-H.; Lee, B.H. Biomechanical Analysis of Allograft Spacer Failure as a Function of Cortical-Cancellous Ratio in Anterior Cervical Discectomy/Fusion: Allograft Spacer Alone Model. Appl. Sci. 2020, 10, 6413. [Google Scholar] [CrossRef]
- Patwardhan, A.G.; Khayatzadeh, S.; Nguyen, N.L.; Havey, R.M.; Voronov, L.I.; Muriuki, M.G.; Carandang, G.; Smith, Z.A.; Sears, W.; Lomasney, L.M.; et al. Is Cervical Sagittal Imbalance a Risk Factor for Adjacent Segment Pathomechanics After Multilevel Fusion? Spine 2016, 41, E580–E588. [Google Scholar] [CrossRef] [PubMed]
- Park, M.S.; Kelly, M.P.; Lee, D.H.; Min, W.K.; Rahman, R.K.; Riew, K.D. Sagittal alignment as a predictor of clinical adjacent segment pathology requiring surgery after anterior cervical arthrodesis. Spine J. 2014, 14, 1228–1234. [Google Scholar] [CrossRef]
- Gadia, A.; Shah, K.; Nene, A. Cervical Kyphosis. Asian Spine J. 2019, 13, 163–172. [Google Scholar] [CrossRef]
- Gercek, E.; Arlet, V.; Delisle, J.; Marchesi, D. Subsidence of stand-alone cervical cages in anterior interbody fusion: Warning. Eur. Spine J. 2003, 12, 513–516. [Google Scholar] [CrossRef]
- Xing, R.; Liu, W.; Li, X.; Jiang, L.; Yishakea, M.; Dong, J. Characteristics of cervical sagittal parameters in healthy cervical spine adults and patients with cervical disc degeneration. BMC Musculoskelet. Disord. 2018, 19, 37. [Google Scholar] [CrossRef] [PubMed]
- Park, J.Y.; Zhang, H.Y.; Oh, M.C. New technical tip for anterior cervical plating: Make hole first and choose the proper plate size later. J. Korean Neurosurg. Soc. 2011, 49, 212–216. [Google Scholar] [CrossRef] [PubMed]
- Ha, S.K.; Park, J.Y.; Kim, S.H.; Lim, D.J.; Kim, S.D.; Lee, S.K. Radiologic Assessment of Subsidence in Stand-Alone Cervical Polyetheretherketone (PEEK) Cage. J. Korean Neurosurg. Soc. 2008, 44, 370–374. [Google Scholar] [CrossRef]
- Vernon, H.; Mior, S. The Neck Disability Index: A study of reliability and validity. J. Manip. Physiol. Ther. 1991, 14, 409–415. [Google Scholar]
- Jansson, K.-Å.; Granath, F. Health-related quality of life (EQ-5D) before and after orthopedic surgery. Acta Orthop. 2011, 82, 82–89. [Google Scholar] [CrossRef]
- Maharaj, M.M.; Phan, K.; Mobbs, R.J. Anterior cervical discectomy and fusion (ACDF) autograft versus graft substitutes: What do patients prefer?—A clinical study. J. Spine Surg. 2016, 2, 105–110. [Google Scholar] [CrossRef]
- Jang, S.R.; Lee, S.B.; Cho, K.S. A Comparison of Anterior Cervical Discectomy and Fusion versus Fusion Combined with Artificial Disc Replacement for Treating 3-Level Cervical Spondylotic Disease. J. Korean Neurosurg. Soc. 2017, 60, 676–683. [Google Scholar] [CrossRef]
- Woo, J.B.; Son, D.W.; Lee, S.H.; Lee, J.S.; Lee, S.W.; Song, G.S. Risk Factors of Allogenous Bone Graft Collapse in Two-Level Anterior Cervical Discectomy and Fusion. J. Korean Neurosurg. Soc. 2019, 62, 450–457. [Google Scholar] [CrossRef] [PubMed]
- Kao, T.H.; Wu, C.H.; Chou, Y.C.; Chen, H.T.; Chen, W.H.; Tsou, H.K. Risk factors for subsidence in anterior cervical fusion with stand-alone polyetheretherketone (PEEK) cages: A review of 82 cases and 182 levels. Arch. Orthop. Trauma Surg. 2014, 134, 1343–1351. [Google Scholar] [CrossRef]
- Daffner, S.D.; Wang, J.C. Anterior cervical fusion: The role of anterior plating. Instr. Course Lect. 2009, 58, 689–698. [Google Scholar] [PubMed]
- Hakało, J.; Wroński, J.; Ciupik, L. Osiadanie i jego wpływ na układ stabilizacji płytkowej przedniej w przebiegu spondylodezy miedzytrzonowej kregosłupa szyjnego. Cześć 1: Definicja i przeglad piśmiennictwa [Subsidence and its effect on the anterior plate stabilization in the course of cervical spondylodesis. Part I: Definition and review of literature]. Neurol. Neurochir. Pol. 2003, 37, 903–915. [Google Scholar]
- Oh, K.; Lee, C.K.; You, N.K.; Kim, S.H.; Cho, K.H. Radiologic changes of anterior cervical discectomy and fusion using allograft and plate augmentation: Comparison of using fixed and variable type screw. Korean J. Spine 2013, 10, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Lee, N.J.; Vulapalli, M.; Park, P.; Kim, J.S.; Boddapati, V.; Mathew, J.; Amorosa, L.F.; Sardar, Z.M.; Lehman, R.A.; Riew, K.D. Does Screw Length for Primary Two-level ACDF Influence Pseudarthrosis Risk? Spine J. 2020, 20, 1752–1760. [Google Scholar] [CrossRef]
- Dipaola, C.P.; Jacobson, J.A.; Awad, H.; Conrad, B.P.; Rechtine, G.R., 2nd. Screw orientation and plate type (variable- vs. fixed-angle) effect strength of fixation for in vitro biomechanical testing of the Synthes CSLP. Spine J. 2008, 8, 717–722. [Google Scholar] [CrossRef] [PubMed]
- DiPaola, C.P.; Jacobson, J.A.; Awad, H.; Conrad, B.P.; Rechtine, G.R., 2nd. Screw pull-out force is dependent on screw orientation in an anterior cervical plate construct. J. Spinal Disord. Tech. 2007, 20, 369–373. [Google Scholar] [CrossRef] [PubMed]
- Park, J.B.; Cho, Y.S.; Riew, K.D. Development of adjacent-level ossification in patients with an anterior cervical plate. J. Bone Jt. Surg. Am. 2005, 87, 558–563. [Google Scholar] [CrossRef]
- Chung, J.Y.; Park, J.B.; Seo, H.Y.; Kim, S.K. Adjacent Segment Pathology after Anterior Cervical Fusion. Asian Spine J. 2016, 10, 582–592. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.H.; Kang, C.N. Degenerative Cervical Myelopathy: Pathophysiology and Current Treatment Strategies. Asian Spine J. 2020, 14, 710–720. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Short Plate (n = 47) | Medium Plate (n = 32) | Overall | p-Value | |
|---|---|---|---|---|
| Sex | 0.035 | |||
| Male | 29 (61.7) | 12 (37.5) | 41 (51.9) | |
| Female | 18 (38.3) | 20 (62.5) | 38 (48.1) | |
| Age | 55.3 ± 12.0 | 58.0 ± 11.3 | 56.4 ± 11.7 | 0.313 |
| Diagnosis | 0.003 | |||
| CSMR | 23 (48.9) | 27 (84.4) | 50 (63.3) | |
| OPLL | 3 (6.4) | 0 (0.0) | 3 (3.8) | |
| HCD | 21 (44.7) | 5 (15.6) | 26 (32.9) | |
| Myelopathy | 33 (70.2) | 24 (75.0) | 57 (72.2) | 0.641 |
| Operation Level | 0.476 | |||
| 1 | 13 (27.7) | 6 (18.8) | 19 (24.1) | |
| 2 | 22 (46.8) | 13 (40.6) | 35 (44.3) | |
| 3 | 9 (19.2) | 11 (34.4) | 20 (25.3) | |
| 4 | 3 (6.4) | 2 (6.3) | 5 (6.3) | |
| Plate-to-Disc Distance (mm) Superior | 10.7 ± 2.3 | 4.7 ± 1.8 | 8.3 ± 3.6 | <0.001 |
| Plate-to-Disc Distance (mm) Inferior | 9.0 ± 2.0 | 4.0 ± 1.0 | 7.0 ± 3.0 | <0.001 |
| Short Plate (n = 47) | Medium Plate (n = 32) | Overall | p-Value | |
|---|---|---|---|---|
| Immediate Post-op | ||||
| Screw Angle Superior | 22.8 ± 5.3 | 12.3 ± 2.5 | 18.5 ± 6.8 | <0.001 |
| Screw Angle Inferior | 23.3 ± 4.7 | 13.2 ± 3.2 | 19.2 ± 6.5 | <0.001 |
| Control for Subsidence | 61.6 ± 19.8 | 57.3 ± 22.5 | 59.9 ± 20.9 | 0.375 |
| 3 Months | ||||
| Screw Angle Superior | 21.4 ± 5.0 | 11.0 ± 2.5 | 17.2 ± 6.6 | <0.001 |
| Screw Angle Inferior | 22.0 ± 4.6 | 11.8 ± 3.6 | 17.9 ± 6.5 | <0.001 |
| Subsidence Rate | 2.1 ± 1.9 | 2.9 ± 2.8 | 2.4 ± 2.3 | 0.133 |
| Subsidence >3 mm (n, %) | 2 (4.26) | 4 (12.5) | 6 (7.59) | 0.179 |
| 1 Year | ||||
| Screw Angle Superior | 20.9 ± 5.0 | 10.7 ± 2.6 | 16.7 ± 6.6 | <0.001 |
| Screw Angle Inferior | 20.9 ± 5.0 | 11.2 ± 3.5 | 17.0 ± 6.5 | <0.001 |
| Subsidence Rate | 1.9 ± 1.8 | 3.2 ± 2.7 | 2.5 ± 2.3 | 0.017 |
| Subsidence >3 mm (n, %) | 4 (8.5) | 8 (25.0) | 12 (15.2) | 0.045 |
| ALOD | 6 (12.8) | 10 (31.2) | 16 (20.2) | 0.045 |
| Regression Coefficient | 95% Confidence Interval | p-Value | |
|---|---|---|---|
| 3 months | |||
| Subsidence Rate | 1.3 | 0.1 to 2.4 | 0.033 |
| C2–C7 SVA | −0.7 | −4.3 to 3.0 | 0.716 |
| Cervical Lordosis Angle | −1.8 | −6.0 to 2.4 | 0.388 |
| NDI | −0.05 | −0.1 to 0.02 | 0.162 |
| VAS | 6.4 | −0.9 to 13.8 | 0.087 |
| 1 year | |||
| Subsidence Rate | 1.4 | 0.2 to 2.5 | 0.018 |
| C2–C7 SVA | 0.04 | −3.2 to 3.3 | 0.981 |
| Cervical Lordosis Angle | 0.3 | −3.0 to 3.8 | 0.836 |
| NDI | −0.02 | −0.1 to 0.03 | 0.347 |
| VAS | 4.8 | −1.9 to 11.4 | 0.156 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jimenez, K.-A.; Kim, J.; Lee, J.; Lee, H.-M.; Moon, S.-H.; Suk, K.-S.; Kim, H.-S.; Lee, B.-H. Short Plate with Screw Angle over 20 Degrees Improves the Radiologic Outcome in ACDF: Clinical Study. J. Clin. Med. 2021, 10, 2034. https://doi.org/10.3390/jcm10092034
Jimenez K-A, Kim J, Lee J, Lee H-M, Moon S-H, Suk K-S, Kim H-S, Lee B-H. Short Plate with Screw Angle over 20 Degrees Improves the Radiologic Outcome in ACDF: Clinical Study. Journal of Clinical Medicine. 2021; 10(9):2034. https://doi.org/10.3390/jcm10092034
Chicago/Turabian StyleJimenez, Kathryn-Anne, Jihyeon Kim, Jaenam Lee, Hwan-Mo Lee, Seong-Hwan Moon, Kyung-Soo Suk, Hak-Sun Kim, and Byung-Ho Lee. 2021. "Short Plate with Screw Angle over 20 Degrees Improves the Radiologic Outcome in ACDF: Clinical Study" Journal of Clinical Medicine 10, no. 9: 2034. https://doi.org/10.3390/jcm10092034
APA StyleJimenez, K.-A., Kim, J., Lee, J., Lee, H.-M., Moon, S.-H., Suk, K.-S., Kim, H.-S., & Lee, B.-H. (2021). Short Plate with Screw Angle over 20 Degrees Improves the Radiologic Outcome in ACDF: Clinical Study. Journal of Clinical Medicine, 10(9), 2034. https://doi.org/10.3390/jcm10092034