
Prospective Measures of Adherence by Questionnaire, Low Immunosuppression and Graft Outcome in Kidney Transplantation

 , , , , and
, , , , and
Abstract
1. Introduction
2. Patients and Methods
2.1. Study Design
2.2. CNI Regimens
2.3. Evaluation of Medication Non-Adherence
2.4. Outcomes
2.5. Statistical Analysis
3. Results
3.1. Patients’ Characteristics and Immunosuppression
3.2. Medication Non-Adherence
3.3. De Novo Donor-Specific Antibodies
3.4. Rejection
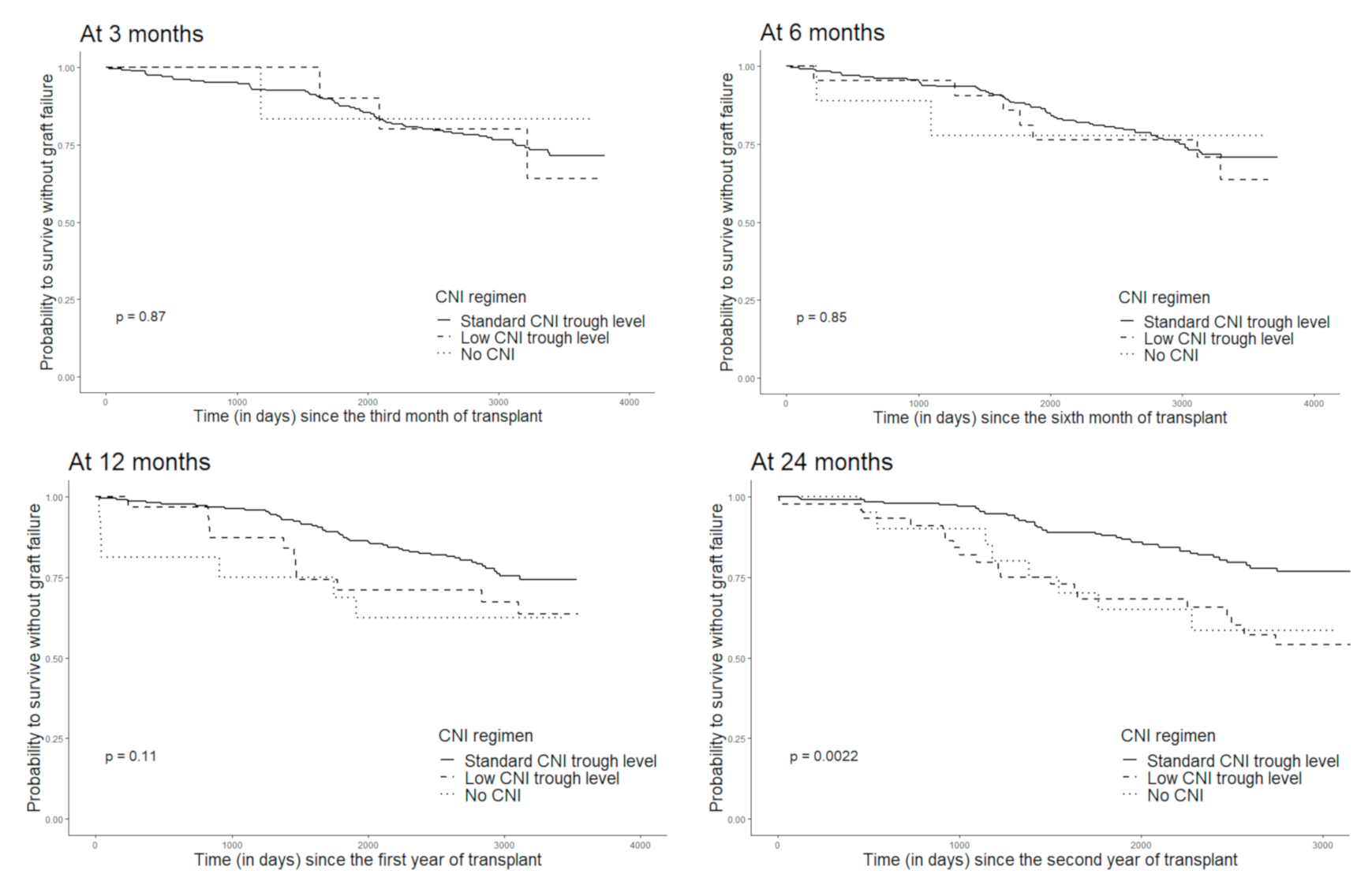
3.5. Graft Survival
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wiebe, C.; Gibson, I.W.; Blydt-Hansen, T.D.; Pochinco, D.; Birk, P.E.; Ho, J.; Karpinski, M.; Goldberg, A.; Storsley, L.; Rush, D.N.; et al. Rates and Determinants of Progression to Graft Failure in Kidney Allograft Recipients with De Novo Donor-Specific Antibody: Post- dn DSA Clinical Histologic Progression. Am. J. Transplant. 2015, 15, 2921–2930. [Google Scholar] [CrossRef] [PubMed]
- Loupy, A.; Hill, G.S.; Jordan, S.C. The impact of donor-specific anti-HLA antibodies on late kidney allograft failure. Nat. Rev. Nephrol. 2012, 8, 348–357. [Google Scholar] [CrossRef] [PubMed]
- Nankivell, B.J.; Shingde, M.; Keung, K.L.; Fung, C.L.; Borrows, R.J.; O’Connell, P.J.; Chapman, J.R. The causes, significance and consequences of inflammatory fibrosis in kidney transplantation: The Banff i-IFTA lesion. Am. J. Transplant. 2018, 18, 364–376. [Google Scholar] [CrossRef] [PubMed]
- Lefaucheur, C.; Gosset, C.; Rabant, M.; Viglietti, D.; Verine, J.; Aubert, O.; Louis, K.; Glotz, D.; Legendre, C.; Van Huyen, J.D.; et al. T cell–mediated rejection is a major determinant of inflammation in scarred areas in kidney allografts. Am. J. Transplant. 2018, 18, 377–390. [Google Scholar] [CrossRef]
- Mehta, R.; Bhusal, S.; Randhawa, P.; Sood, P.; Cherukuri, A.; Wu, C.; Puttarajappa, C.; Hoffman, W.; Shah, N.; Mangiola, M.; et al. Short-term adverse effects of early subclinical allograft inflammation in kidney transplant recipients with a rapid steroid withdrawal protocol. Am. J. Transplant. 2018, 18, 1710–1717. [Google Scholar] [CrossRef]
- Gosset, C.; Viglietti, D.; Rabant, M.; Vérine, J.; Aubert, O.; Glotz, D.; Legendre, C.; Taupin, J.-L.; Van-Huyen, J.-P.D.; Loupy, A.; et al. Circulating donor-specific anti-HLA antibodies are a major factor in premature and accelerated allograft fibrosis. Kidney Int. 2017, 92, 729–742. [Google Scholar] [CrossRef]
- Naesens, M.; Kuypers, D.R.; De Vusser, K.; Evenepoel, P.; Claes, K.; Bammens, B.; Björn, M.; Ben, S.; Jacques, P.; Diethard, M.; et al. The Histology of Kidney Transplant Failure: A Long-Term Follow-Up Study. Transplantation 2014, 98, 427–435. [Google Scholar] [CrossRef]
- Wiebe, C.; Gibson, I.W.; Blydt-Hansen, T.D.; Karpinski, M.; Ho, J.; Storsley, L.J.; Goldberg, A.; Birk, P.E.; Rush, D.N.; Nickerson, P.W. Evolution and Clinical Pathologic Correlations of De Novo Donor-Specific HLA Antibody Post Kidney Transplant: Clinical Pathologic Correlations of De Novo DSA. Am. J. Transplant. 2012, 12, 1157–1167. [Google Scholar] [CrossRef]
- Wiebe, C.; Rush, D.N.; Nevins, T.E.; Birk, P.E.; Blydt-Hansen, T.; Gibson, I.W.; Goldberg, A.; Ho, J.; Karpinski, M.; Pochinco, D.; et al. Class II Eplet Mismatch Modulates Tacrolimus Trough Levels Required to Prevent Donor-Specific Antibody Development. J. Am. Soc. Nephrol. 2017, 28, 3353–3362. [Google Scholar] [CrossRef]
- Nevins, T.E.; Nickerson, P.W.; Dew, M.A. Understanding Medication Nonadherence after Kidney Transplant. J. Am. Soc. Nephrol. 2017, 28, 2290–2301. [Google Scholar] [CrossRef]
- Snanoudj, R.; Kamar, N.; Cassuto, E.; Caillard, S.; Metzger, M.; Merville, P.; Thierry, A.; Jollet, I.; Grimbert, P.; Anglicheau, D.; et al. Epitope load identifies kidney transplant recipients at risk of allosensitization following minimization of immunosuppression. Kidney Int. 2019, 95, 1471–1485. [Google Scholar] [CrossRef]
- Girerd, S.; Schikowski, J.; Girerd, N.; Duarte, K.; Busby, H.; Gambier, N.; Ladrière, M.; Kessler, M.; Frimat, L.; Aarnink, A. Impact of reduced exposure to calcineurin inhibitors on the development of de novo DSA: A cohort of non-immunized first kidney graft recipients between 2007 and 2014. BMC Nephrol. 2018, 19, 232. [Google Scholar] [CrossRef]
- Kaneku, H.; O’leary, J.G.; Banuelos, N.; Jennings, L.W.; Susskind, B.M.; Klintmalm, G.B.; Terasaki, P.I. De novo donor-specific HLA antibodies decrease patient and graft survival in liver transplant recipients. Am. J. Transplant. 2013, 13, 1541–1548. [Google Scholar] [CrossRef]
- Gatault, P.; Kamar, N.; Büchler, M.; Colosio, C.; Bertrand, D.; Durrbach, A.; Albano, L.; Rivalan, J.; Le Meur, Y.; Essig, M.; et al. Reduction of Extended-Release Tacrolimus Dose in Low-Immunological-Risk Kidney Transplant Recipients Increases Risk of Rejection and Appearance of Donor-Specific Antibodies: A Randomized Study. Am. J. Transplant. 2016, 17, 1370–1379. [Google Scholar] [CrossRef]
- Liefeldt, L.; Brakemeier, S.; Glander, P.; Waiser, J.; Lachmann, N.; Schönemann, C.; Zukunft, B.; Illigens, P.; Schmidt, D.; Wu, K.; et al. Donor-Specific HLA Antibodies in a Cohort Comparing Everolimus With Cyclosporine After Kidney Transplantation. Am. J. Transplant. 2012, 12, 1192–1198. [Google Scholar] [CrossRef]
- Rostaing, L.; Hertig, A.; Albano, L.; Anglicheau, D.; Durrbach, A.; Vuiblet, V.; Moulin, B.; Merville, P.; Hazzan, M.; Lang, P.; et al. Fibrosis Progression According to Epithelial-Mesenchymal Transition Profile: A Randomized Trial of Everolimus versus CsA: IT/FA Progression: Everolimus vs. CsA. Am. J. Transplant. 2015, 15, 1303–1312. [Google Scholar] [CrossRef]
- Gupta, G.; Jawdeh, B.G.A.; Racusen, L.C.; Bhasin, B.; Arend, L.J.; Trollinger, B.; Edward, K.; Hamid, R.; Andrea, A.Z.; Robert, A.M.; et al. Late Antibody-Mediated Rejection in Renal Allografts: Outcome After Conventional and Novel Therapies. Transplantation 2014, 97, 1240–1246. [Google Scholar] [CrossRef]
- Low, J.K.; Williams, A.; Manias, E.; Crawford, K. Interventions to improve medication adherence in adult kidney transplant recipients: A systematic review. Nephrol. Dial. Transplant. 2015, 30, 752–761. [Google Scholar] [CrossRef]
- Sellarés, J.; De Freitas, D.G.; Mengel, M.; Reeve, J.; Einecke, G.; Sis, B.; Hidalgo, L.G.; Famulski, K.; Matas, A.; Halloran, P.F.; et al. Understanding the Causes of Kidney Transplant Failure: The Dominant Role of Antibody-Mediated Rejection and Nonadherence: Attributing Causes of Kidney Transplant Loss. Am. J. Transplant. 2012, 12, 388–399. [Google Scholar] [CrossRef]
- Vlaminck, H.; Maes, B.; Evers, G.; Verbeke, G.; Lerut, E.; Van Damme, B.; Vanrenterghem, Y. Prospective Study on Late Consequences of Subclinical Non-Compliance with Immunosuppressive Therapy in Renal Transplant Patients. Am. J. Transplant. 2004, 4, 1509–1513. [Google Scholar] [CrossRef]
- Takemoto, S.K.; Pinsky, B.W.; Schnitzler, M.A.; Lentine, K.L.; Willoughby, L.M.; Burroughs, T.E.; Bunnapradist, S. A Retrospective Analysis of Immunosuppression Compliance, Dose Reduction and Discontinuation in Kidney Transplant Recipients. Am. J. Transplant. 2007, 7, 2704–2711. [Google Scholar] [CrossRef]
- Pinsky, B.W.; Takemoto, S.K.; Lentine, K.L.; Burroughs, T.E.; Schnitzler, M.A.; Salvalaggio, P.R. Transplant Outcomes and Economic Costs Associated with Patient Noncompliance to Immunosuppression. Am. J. Transplant. 2009, 9, 2597–2606. [Google Scholar] [CrossRef]
- Gaynor, J.J.; Ciancio, G.; Guerra, G.; Sageshima, J.; Hanson, L.; Roth, D.; Linda, C.; Warren, K.; Adela, M.; Lissett, T.; et al. Graft Failure Due to Noncompliance among 628 Kidney Transplant Recipients with Long-term Follow-up: A Single-Center Observational Study. Transplantation 2014, 97, 925–933. [Google Scholar] [CrossRef]
- Chisholm-Burns, M.A.; Spivey, C.A.; Rehfeld, R.; Zawaideh, M.; Roe, D.J.; Gruessner, R. Immunosuppressant Therapy Adherence and Graft Failure Among Pediatric Renal Transplant Recipients. Am. J. Transplant. 2009, 9, 2497–2504. [Google Scholar] [CrossRef]
- Osterberg, L.; Blaschke, T. Adherence to Medication. N. Engl. J. Med. 2005, 353, 487–497. [Google Scholar] [CrossRef]
- Kahan, B.D.; Welsh, M.; Urbauer, D.L.; Mosheim, M.B.; Beusterien, K.M.; Wood, M.R.; Schoenberg, L.P.; Dicesare, J.; Katz, S.M.; Van Buren, C.T. Low intraindividual variability of cyclosporin A exposure reduces chronic rejection incidence and health care costs. J. Am. Soc. Nephrol. 2000, 11, 1122–1131. [Google Scholar] [CrossRef]
- Rodrigo, E.; Segundo, D.S.; Fernández-Fresnedo, G.; López-Hoyos, M.; Benito, A.; Ruiz, J.C.; De Cos, M.-A.; Arias, M. Within-Patient Variability in Tacrolimus Blood Levels Predicts Kidney Graft Loss and Donor-Specific Antibody Development. Transplantation 2016, 100, 2479–2485. [Google Scholar] [CrossRef] [PubMed]
- Nevins, T.E.; Robiner, W.N.; Thomas, W. Predictive Patterns of Early Medication Adherence in Renal Transplantation. Transplantation 2014, 98, 878–884. [Google Scholar] [CrossRef] [PubMed]
- Nevins, T.E.; Kruse, L.; Skeans, M.A.; Thomas, W. The natural history of azathioprine compliance after renal transplantation. Kidney Int. 2001, 60, 1565–1570. [Google Scholar] [CrossRef] [PubMed]
- Wiebe, C.; Nevins, T.E.; Robiner, W.N.; Thomas, W.; Matas, A.J.; Nickerson, P.W. The Synergistic Effect of Class II HLA Epitope-Mismatch and Nonadherence on Acute Rejection and Graft Survival: Class II Epitope-Mismatch and Nonadherence. Am. J. Transplant. 2015, 15, 2197–2202. [Google Scholar] [CrossRef] [PubMed]
- Israni, A.K.; Weng, F.L.; Cen, Y.Y.; Joffe, M.; Kamoun, M.; Feldman, H.I. Electronically measured adherence to immunosuppressive medications and kidney function after deceased donor kidney transplantation: Medication adherence after renal transplant. Clin. Transplant. 2011, 25, 124–131. [Google Scholar] [CrossRef]
- Weng, F.L.; Israni, A.K.; Joffe, M.M.; Hoy, T.; Gaughan, C.A.; Newman, M.; Abrams, J.D.; Kamoun, M.; Rosas, S.E.; Mange, K.C.; et al. Race and Electronically Measured Adherence to Immunosuppressive Medications after Deceased Donor Renal Transplantation. J. Am. Soc. Nephrol. 2005, 16, 1839–1848. [Google Scholar] [CrossRef]
- Denhaerynck, K.; Steiger, J.; Bock, A.; Schäfer-Keller, P.; Köfer, S.; Thannberger, N.; De Geest, S. Prevalence and Risk Factors of Non-Adherence with Immunosuppressive Medication in Kidney Transplant Patients. Am. J. Transplant. 2006, 7, 108–116. [Google Scholar] [CrossRef]
- Denhaerynck, K.; Burkhalter, F.; Schäfer-Keller, P.; Steiger, J.; Bock, A.; De Geest, S. Clinical consequences of non adherence to immunosuppressive medication in kidney transplant patients. Transpl. Int. 2009, 22, 441–446. [Google Scholar] [CrossRef]
- Myaskovsky, L.; Jesse, M.T.; Kuntz, K.; Leino, A.D.; Peipert, J.D.; Russell, C.L.; Spivey, C.A.; Sulejmani, N.; Dew, M.A. Report from the American Society of Transplantation Psychosocial Community of Practice Adherence Task Force: Real-world options for promoting adherence in adult recipients. Clin. Transplant. 2018, 32, e13353. [Google Scholar] [CrossRef]
- De Geest, S.; Borgermans, L.; Gemoets, H.; Abraham, I.; Vlaminck, H.; Evers, G.; Vanrenterghem, Y. Incidence, determinants, and consequences of subclinical noncompliance with immunosuppressive therapy in renal transplant recipients. Transplantation 1995, 59, 340–347. [Google Scholar] [CrossRef]
- Villeneuve, C.; Rousseau, A.; Rerolle, J.-P.; Couzi, L.; Kamar, N.; Essig, M.; Etienne, I.; Westeel, P.-F.; Büchler, M.; Esposito, L.; et al. Adherence profiles in kidney transplant patients: Causes and consequences. Patient Educ. Couns. 2020, 103, 189–198. [Google Scholar] [CrossRef]
- Fine, R.N.; Becker, Y.; De Geest, S.; Eisen, H.; Ettenger, R.; Evans, R.; Rudow, D.L.; McKay, D.; Neu, A.; Nevins, T.; et al. Nonadherence Consensus Conference Summary Report: Nonadherence Consensus Conference Summary Report. Am. J. Transplant. 2008, 9, 35–41. [Google Scholar] [CrossRef]
- Morisky, D.E.; Green, L.W.; Levine, D.M. Concurrent and Predictive Validity of a Self-reported Measure of Medication Adherence. Med. Care 1986, 24, 67–74. [Google Scholar] [CrossRef]
- Couzi, L.; Moulin, B.; Morin, M.P.; Albano, L.; Godin, M.; Barrou, B.; Eric, A.; Emmanuel, M.; Sandrine, G.-S.; Laurence, M.; et al. Factors Predictive of Medication Nonadherence After Renal Transplantation: A French Observational Study. Transplantation 2013, 95, 326–332. [Google Scholar] [CrossRef]
- Leffondré, K.; Jager, K.J.; Boucquemont, J.; Stel, V.S.; Heinze, G. Representation of exposures in regression analysis and interpretation of regression coefficients: Basic concepts and pitfalls. Nephrol. Dial. Transplant. 2013, 29, 1806–1814. [Google Scholar] [CrossRef] [PubMed]
- Chapman, J.R. Compliance: The patient, the doctor, and the medication? Transplantation 2004, 77, 782–786. [Google Scholar] [CrossRef] [PubMed]
- Dobbels, F.; Berben, L.; De Geest, S.; Drent, G.; Lennerling, A.; Whittaker, C.; Kugler, C. The Psychometric Properties and Practicability of Self-Report Instruments to Identify Medication Nonadherence in Adult Transplant Patients: A Systematic Review. Transplantation 2010, 90, 205–219. [Google Scholar] [CrossRef] [PubMed]
- Vanhove, T.; Vermeulen, T.; Annaert, P.; Lerut, E.; Kuypers, D.R.J. High Intrapatient Variability of Tacrolimus Concentrations Predicts Accelerated Progression of Chronic Histologic Lesions in Renal Recipients. Am. J. Transplant. 2016, 16, 2954–2963. [Google Scholar] [CrossRef]
- Sapir-Pichhadze, R.; Wang, Y.; Famure, O.; Li, Y.; Kim, S.J. Time-dependent variability in tacrolimus trough blood levels is a risk factor for late kidney transplant failure. Kidney Int. 2014, 85, 1404–1411. [Google Scholar] [CrossRef]
- Schäfer-Keller, P.; Steiger, J.; Bock, A.; Denhaerynck, K.; De Geest, S. Diagnostic Accuracy of Measurement Methods to Assess Non-Adherence to Immunosuppressive Drugs in Kidney Transplant Recipients. Am. J. Transplant. 2008, 8, 616–626. [Google Scholar] [CrossRef]
- Guidicelli, G.; Guerville, F.; Lepreux, S.; Wiebe, C.; Thaunat, O.; Dubois, V.; Visentin, J.; Bachelet, T.; Morelon, E.; Nickerson, P.; et al. Non-Complement–Binding De Novo Donor-Specific Anti-HLA Antibodies and Kidney Allograft Survival. J. Am. Soc. Nephrol. 2015, 27, 615–625. [Google Scholar] [CrossRef]
- Ekberg, H.; Tedesco-Silva, H.; Demirbas, A.; Vítko, Š.; Nashan, B.; Guerkan, A.; Margreiter, R.; Hugo, C.; Grinyó, J.M.; Frei, U.; et al. Reduced Exposure to Calcineurin Inhibitors in Renal Transplantation. N. Engl. J. Med. 2007, 357, 2562–2575. [Google Scholar] [CrossRef]
- Nankivell, B.J.; Borrows, R.J.; Fung, C.L.-S.; O’Connell, P.J.; Allen, R.D.; Chapman, J.R. The Natural History of Chronic Allograft Nephropathy. N. Engl. J. Med. 2003, 349, 2326–2333. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Whole Cohort | By Occurrence of dnDSA between 2 and 3 Years Post Transplant | |||||
|---|---|---|---|---|---|---|
| N | N | No dnDSA n = 207 | dnDSA n = 19 | p Value | ||
| Age (years), median (IQR) | 301 | 51.0 (40.0–60.0) | 226 | 48.8 | 42.3 | 0.04 |
| Male, n (%) | 301 | 208 (69.1) | 226 | 145 (70.0) | 15 (79.0) | 0.60 |
| Primary kidney disease | 295 | 221 | 0.42 | |||
| Vascular, n (%) | 10 (3.4) | 6 (3.0) | 0 (0.0) | |||
| Diabetics, n (%) | 24 (8.1) | 16 (7.9) | 2 (10.5) | |||
| Glomerulonephritis, n (%) | 82 (27.8) | 58 (28.7) | 9 (47.4) | |||
| Tubulo-interstitial, n (%) | 31 (10.5) | 24 (11.9) | 3 (15.8) | |||
| Hereditary (including polycystic kidney disease), n (%) | 64 (21.7) | 52 (25.7) | 2 (10.5) | |||
| Other or undetermined, n (%) | 84 (28.5) | 46 (22.8) | 3 (15.8) | |||
| Dialysis modality before transplant | 292 | 203 | 0.11 | |||
| Preemptive transplantation, n (%) | 27 (9.3) | 1 (0.5) | 0 (0.0) | |||
| Hemodialysis, n (%) | 221 (75.7) | 147 (79.5) | 18 (100.0) | |||
| Peritoneal dialysis, n (%) | 44 (15.1) | 37 (0.2) | 0 (0.0) | |||
| Number of previous graft(s) | 271 | 224 | 0.36 | |||
| 0, n (%) | 224 (82.7) | 172 (83.9) | 16 (84.2) | |||
| 1, n (%) | 41 (15.1) | 30 (14.6) | 2 (10.5) | |||
| ≥2, n (%) | 6 (2.3) | 2 (1.0) | 1 (5.3) | |||
| Sensitized patients, n (%) | 226 | 61 (27) | 226 | 0.11 | ||
| Yes | 59 (28.5) | 2 (10.5) | ||||
| No | 148 (71.5) | 17 (89.5) | ||||
| Donor age (years), mean (SD) | 278 | 49.2 (15.9) | 217 | 47.1 (15.5) | 45.8 (18.4) | 0.75 |
| Living donor, n (%) | 298 | 9 (3.0) | 225 | 6 (2.9) | 0 (0.0) | 1.00 |
| Expanded criteria donor, n (%) | 274 | 116 (42.3) | 213 | 67 (34.5) | 5 (26.3) | 0.61 |
| Number of HLA mismatches (A–B–DR) | 295 | 224 | 0.12 | |||
| 0, n (%) | 3 (1.0) | 1 (0.5) | 0 (0.0) | |||
| 1, n (%) | 10 (3.4) | 7 (3.4) | 0 (0.0) | |||
| 2, n (%) | 26 (8.8) | 14 (6.8) | 1 (5.3) | |||
| 3, n (%) | 48 (16.3) | 29 (14.1) | 4 (21.1) | |||
| 4, n (%) | 91 (30.8) | 64 (31.2) | 3 (15.8) | |||
| 5, n (%) | 85 (28.8) | 61 (29.8) | 11 (57.9) | |||
| 6, n (%) | 32 (10.8) | 29 (14.1) | 0 (0.0) | |||
| Total ischemia time (hours), median (IQR) | 269 | 15.8 (13.0–19.0) | 212 | 16.5 (6.0) | 16.2 (6.8) | 0.84 |
| Induction treatment | 276 | 206 | 0.41 | |||
| Basiliximab, n (%) | 168 (60.9) | 125 (66.1) | 9 (52.9) | |||
| rATG, n (%) | 108 (39.1) | 64 (33.9) | 8 (47.1) | |||
| Delayed graft function, n (%) | 292 | 61 (20.9) | 220 | 40 (19.8) | 5 (27.8) | 0.38 |
| Maintenance treatment at 3 months post-transplant | 296 | 219 | 0.002 | |||
| Cyclosporine | 64 (21.6) | 46 (23.0) | 11 (57.9) | |||
| Tacrolimus | 227 (76.7) | 151 (75.5) | 7 (36.8) | |||
| Without CNI | 5 (1.7) | 3 (1.5) | 1 (5.3) | |||
| Maintenance treatment at 6 months post-transplant | 294 | 219 | 0.004 | |||
| Cyclosporine | 61 (20.7) | 46 (23.0) | 9 (47.4) | |||
| Tacrolimus | 226 (76.9) | 150 (75.0)) | 8 (42.1) | |||
| Without CNI | 7 (2.4) | 4 (2.0) | 2 (10.5) | |||
| Maintenance treatment at 12 months post-transplant | 291 | 219 | 0.02 | |||
| Cyclosporine | 55 (18.9) | 42 (21.0) | 8 (42.1) | |||
| Tacrolimus | 224 (77.0) | 151 (75.5) | 9 (47.4) | |||
| Without CNI | 12 (4.1) | 7 (3.5) | 2 (10.5) | |||
| Maintenance treatment at 24 months post-transplant | 282 | 218 | 0.01 | |||
| Cyclosporine | 53 (18.8) | 41 (20.6) | 7 (36.8) | |||
| Tacrolimus | 214 (75.9) | 150 (75.4) | 9 (47.4) | |||
| Without CNI | 15 (5.3) | 8 (4.0) | 3 (15.8) | |||
| Corticosteroids at 3 months | 301 | 226 | 0.23 | |||
| Continued | 255 (84.7) | 190 (91.8) | 16 (84.2) | |||
| Discontinued | 46 (15.3) | 17 (8.2) | 3 (15.8) | |||
| Follow-Up Visits | ||||
| Immunosuppression Maintenance Treatment | ||||
| M3 (N= 299) | M6 (N= 298) | M12 (N= 294) | M24 (N= 286) | |
| Tacrolimus, n (%) | 227 (75.9) | 228 (76.5) | 225 (76.5) | 216 (75.5) |
| Cyclosporine, n (%) | 65 (21.7) | 61 (20.5) | 55 (18.7) | 53 (18.5) |
| MMF, n (%) | 283 (94.6) | 266 (89.2) | 263 (89.4) | 251 (87.8) |
| Steroids, n (%) | 255 (85.3) | 203 (68.1) | 166 (56.5) | 142 (49.7) |
| CNI withdrawal, n (%) | 7 (2.3) | 9 (3.0) | 14 (4.8) | 17 (5.9) |
| Trough levels of tacrolimus, med (IQR) | 8.8 (7.3–10.8) | 8.2 (6.7–9.7) | 7.6 (6.4–9.3) | 7.5 (6.2–8.9) |
| Trough levels of cyclosporine, med (IQR) | 156 (130–190) | 149 (112–171) | 128.5 (96–157) | 93 (65–125) |
| Treatment Medication Non-Adherence Assessed by the Morisky Scale | ||||
| M3 (N = 272) | M6 (N= 263) | M12 (N= 269) | M24 (N= 234) | |
| Positive response to questions of the Morisky scale, n (%) | ||||
| Do you ever forget to take your medicine? | 19 (7.0) | 29 (10.9) | 40 (14.9) | 46 (19.5) |
| Are you careless at times about taking your medicine? | 33 (12.1) | 40 (15.2) | 54 (20.1) | 49 (20.8) |
| When you feel better, do you sometimes stop taking your medicine? | 2 (0.7) | 0 (0.0) | 2 (0.7) | 1 (0.4) |
| Sometimes if you feel worse when you take your medicine, do you stop taking it? | 6 (2.2) | 2 (0.7) | 3 (1.1) | 2 (0.8) |
| Non-adherent patients †, n (%) | 48 (17.6) | 62 (23.6) | 84 (31.2) | 81 (34.6) |
| Always non-adherent patients ‡, n (%) | 12 (4.0) | |||
| Score of the Morisky scale, n (%) | ||||
| 4 | 224 (82.4) | 201 (76.4) | 185 (68.8) | 153 (65.4) |
| 3 | 41 (15.1) | 54 (20.5) | 72 (26.8) | 66 (28.2) |
| ≤2 | 7 (2.6) | 8 (3.1) | 12 (4.4) | 15 (6.4) |
| Global score *, n (%) | ||||
| 16 | 96 (48.7) | |||
| 15 | 42 (21.3) | |||
| 13–14 | 42 (21.3) | |||
| ≤12 | 17 (8.6) | |||
| 3 Months (N ‡ = 200) | 6 Months (N ‡ = 193) | 12 Months (N ‡ = 198) | 24 Months (N ‡ = 174) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR * | CI 95% | p-Value | OR * | CI 95% | p-Value | OR * | CI 95% | p-Value | OR * | CI 95% | p-Value | |
| Non adherent vs. adherent† | 1.16 | 0.31–4.45 | 0.73 | 1.40 | 0.43–4.56 | 0.44 | 0.48 | 0.14–1.66 | 0.31 | 2.01 | 0.59–6.83 | 0.19 |
| Maintenance treatment | 0.005 | 0.04 | 0.009 | 0.005 | ||||||||
| Tacrolimus | 1 | 1 | 1 | 1 | ||||||||
| Cyclosporine | 5.2 | 1.65–16.4 | 2.49 | 0.76–8.16 | 4.67 | 1.48–14.76 | 5.17 | 1.34–20.01 | ||||
| Without anticalcineurin | 15.3 | 0.84–279.6 | 15.5 | 1.46–165.2 | 7.39 | 1.08–50.47 | 11.8 | 1.34–69.6 | ||||
| Recipient age (per year) | 0.97 | 0.93–1.01 | 0.06 | 0.96 | 0.92–0.99 | 0.02 | 0.96 | 0.92–0.99 | 0.03 | 0.97 | 0.93–1.02 | 0.15 |
| HLA mismatch (per number of mismatch) | 1.04 | 0.66–1.64 | 0.75 | 1.06 | 0.67–1.67 | 0.62 | 1.02 | 0.66–1.58 | 0.91 | 0.94 | 0.59–1.50 | 0.96 |
| Sensitized patients vs. non-sensitized patients | 0.21 | 0.03–1.72 | 0.91 | 0.21 | 0.03–1.74 | 0.95 | 0.18 | 0.02–1.42 | 0.78 | 0.21 | 0.03–1.74 | 0.81 |
| 3 Months (N ‡ = 190) | 6 Months (N ‡ = 183) | 12 Months (N ‡ = 191) | 24 Months (N ‡ = 169) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HR * | CI 95% | p-Value | HR * | CI 95% | p-Value | HR * | CI 95% | p-Value | HR * | CI 95% | p-Value | |
| Non adherent vs. adherent † | 0.89 | 0.40–2.00 | 0.84 | 1.08 | 0.53–2.23 | 0.73 | 0.97 | 0.50–1.88 | 0.46 | 0.93 | 0.49–1.79 | 0.92 |
| Recipient age (per year) | 1.01 | 0.98–1.05 | 0.78 | 1.01 | 0.97–1.04 | 0.63 | 1.01 | 0.97–1.04 | 0.75 | 1.00 | 0.97–1.04 | 0.72 |
| Donor age | 0.68 | 0.91 | 0.71 | 0.24 | ||||||||
| <38 years | 1 | 1 | 1 | 1 | ||||||||
| 39–50 years | 1.34 | 0.51–3.53 | 1.21 | 0.44–3.35 | 1.10 | 0.42–2.93 | 1.92 | 0.63–5.85 | ||||
| 51–59 years | 1.80 | 0.67–4.83 | 1.54 | 0.54–4.40 | 1.49 | 0.54–4.10 | 2.73 | 0.84–8.85 | ||||
| ≥60 years | 2.01 | 0.62–6.60 | 1.04 | 0.28–3.87 | 1.27 | 0.37–4.38 | 3.67 | 0.97–13.9 | ||||
| Maintenance treatment | 0.37 | 0.27 | 0.97 | 0.15 | ||||||||
| Tacrolimus | 1 | 1 | 1 | 1 | ||||||||
| Cyclosporine | 0.90 | 0.46–1.78 | 1.30 | 0.69–2.45 | 0.86 | 0.45–1.65 | 0.76 | 0.37–1.56 | ||||
| Any anticalcineurin | 0.46 | 0.06–3.56 | 0.26 | 0.03–2.02 | 0.71 | 0.21–2.38 | 1.20 | 0.45–3.23 | ||||
| Occurrence of acute rejection (time-dependent variable) | 2.64 | 1.34–5.16 | 0.0005 | 2.65 | 1.43–4.90 | 0.002 | 1.92 | 1.06–3.49 | 0.03 | 1.90 | 0.98–3.67 | 0.055 |
| Occurrence of dnDSA between 2 and 3 years post-transplant | 2.42 | 1.02–5.75 | 0.03 | 3.51 | 1.49–8.25 | 0.002 | 2.30 | 1.03–5.12 | 0.04 | 1.84 | 0.74–5.23 | 0.19 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prezelin-Reydit, M.; Dubois, V.; Caillard, S.; Parissiadis, A.; Etienne, I.; Hau, F.; Albano, L.; Pourtein, M.; Barrou, B.; Taupin, J.-L.; et al. Prospective Measures of Adherence by Questionnaire, Low Immunosuppression and Graft Outcome in Kidney Transplantation. J. Clin. Med. 2021, 10, 2032. https://doi.org/10.3390/jcm10092032
Prezelin-Reydit M, Dubois V, Caillard S, Parissiadis A, Etienne I, Hau F, Albano L, Pourtein M, Barrou B, Taupin J-L, et al. Prospective Measures of Adherence by Questionnaire, Low Immunosuppression and Graft Outcome in Kidney Transplantation. Journal of Clinical Medicine. 2021; 10(9):2032. https://doi.org/10.3390/jcm10092032
Chicago/Turabian StylePrezelin-Reydit, Mathilde, Valérie Dubois, Sophie Caillard, Anne Parissiadis, Isabelle Etienne, Françoise Hau, Laetitia Albano, Monique Pourtein, Benoît Barrou, Jean-Luc Taupin, and et al. 2021. "Prospective Measures of Adherence by Questionnaire, Low Immunosuppression and Graft Outcome in Kidney Transplantation" Journal of Clinical Medicine 10, no. 9: 2032. https://doi.org/10.3390/jcm10092032
APA StylePrezelin-Reydit, M., Dubois, V., Caillard, S., Parissiadis, A., Etienne, I., Hau, F., Albano, L., Pourtein, M., Barrou, B., Taupin, J.-L., Mariat, C., Absi, L., Vigneau, C., Renac, V., Guidicelli, G., Visentin, J., Merville, P., Thaunat, O., & Couzi, L. (2021). Prospective Measures of Adherence by Questionnaire, Low Immunosuppression and Graft Outcome in Kidney Transplantation. Journal of Clinical Medicine, 10(9), 2032. https://doi.org/10.3390/jcm10092032