
Effect of Wearable Technology-Based Physical Activity Interventions on Breast Cancer Survivors’ Physiological, Cognitive, and Emotional Outcomes: A Systematic Review




Abstract
1. Introduction
2. Methods
2.1. Study Eligibility Criteria
2.2. Information Sources and Literature Search
2.3. Data Collection Process
2.4. Data Items
2.5. Risk of Bias within Individual Studies
2.6. Summary Measures
2.7. Synthesis of Results
3. Results
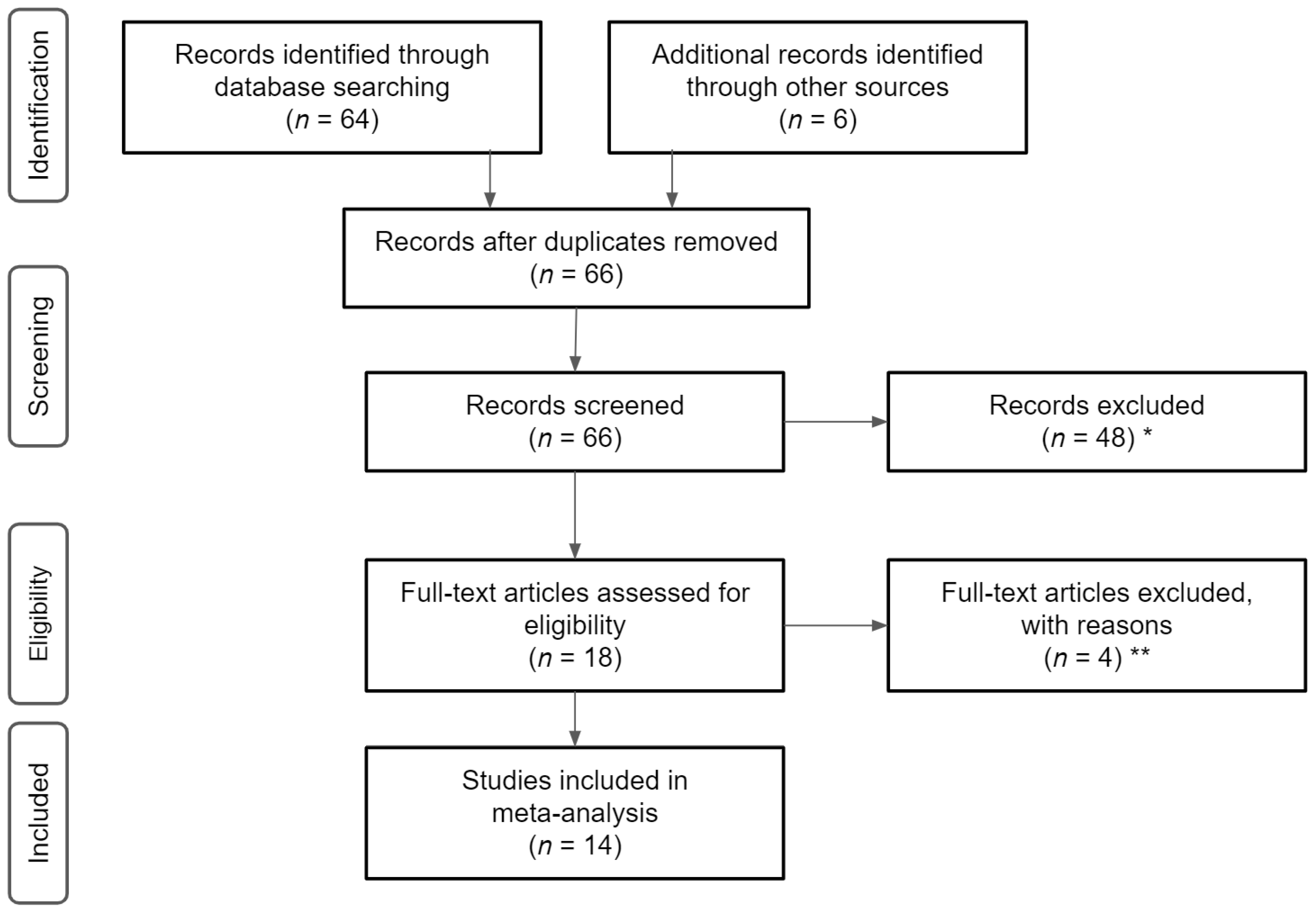
3.1. Study Selection
3.2. Study Characteristics and Quality
3.3. Data Items
3.4. Risk of Bias within Studies
3.5. Synthesis of Results
3.6. Effectiveness of Health-Wearable Interventions
3.6.1. Physiological Effects
3.6.2. Cognitive Effects
3.6.3. Emotional Effects
4. Discussion
Limitations and Recommendations
Author Contributions
Funding
Conflicts of Interest
References
- Blaes, A.; Beckwith, H.; Florea, N.; Hebbel, R.; Solovey, A.; Potter, D.; Yee, D.; Vogel, R.; Luepker, R.; Duprez, D. Vascular function in breast cancer survivors on aromatase inhibitors: A pilot study. Breast Cancer Res. Treat. 2017, 166, 541–547. [Google Scholar] [CrossRef]
- Phillips, S.M.; Courneya, K.S.; Welch, W.A.; Gavin, K.L.; Cottrell, A.; Nielsen, A.; Solk, P.; Blanch-Hartigan, D.; Cella, D.; Ackermann, R.T.; et al. Breast cancer survivors’ preferences for mHealth physical activity interventions: Findings from a mixed methods study. J. Cancer Surviv. 2019, 13, 292–305. [Google Scholar] [CrossRef]
- Lynch, B.M.; Nguyen, N.H.; Reeves, M.M.; Moore, M.M.; Rosenberg, D.E.; Wheeler, M.J.; Boyle, T.; Vallance, J.K.; Friedenreich, C.M.; English, D.R. Study design and methods for the ACTIVity And TEchnology (ACTIVATE) trial. Contemp. Clin. Trials 2018, 64, 112–117. [Google Scholar] [CrossRef] [PubMed]
- Pope, Z.C.; Zeng, N.; Zhang, R.; Lee, H.Y.; Gao, Z. Effectiveness of Combined Smartwatch and Social Media Intervention on Breast Cancer Survivor Health Outcomes: A 10-Week Pilot Randomized Trial. J. Clin. Med. 2018, 7, 140. [Google Scholar] [CrossRef]
- Hartman, S.J.; Natarajan, L.; Palmer, B.W.; Parker, B.; Patterson, R.E.; Sears, D.D. Impact of increasing physical activity on cognitive functioning in breast cancer survivors: Rationale and study design of memory & motion. Contemp. Clin. Trials 2015, 45, 371–376. [Google Scholar]
- Van Der Gucht, K.; Melis, M.; Ahmadoun, S.; Gebruers, A.; Smeets, A.; Vandenbulcke, M.; Wildiers, H.; Neven, P.; Kuppens, P.; Raes, F.; et al. A mindfulness-based intervention for breast cancer patients with cognitive impairment after chemotherapy: Study protocol of a three-group randomized controlled trial. Trials 2020, 21, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Hartman, S.J.; Weiner, L.S.; Nelson, S.H.; Hess, L.; Ehlers, D.; Dregan, A.; Natarajan, L.; Patterson, R.E.; Palmer, B.W.; Parker, B.A.; et al. Mediators of a physical activity intervention on cognition in breast cancer survivors: Evidence from a randomized controlled trial. JMIR Cancer 2019, 5, e13150. [Google Scholar] [CrossRef]
- Sweegers, M.G.; Boyle, T.; Vallance, J.K.; Chinapaw, M.J.; Brug, J.; Aaronson, N.K.; D’Silva, A.; Kampshoff, C.S.; Lynch, B.M.; Nollet, F.; et al. Which cancer survivors are at risk for a physically inactive and sedentary lifestyle? Results from pooled accelerometer data of 1447 cancer survivors. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 1–15. [Google Scholar] [CrossRef]
- Boyle, T.; Vallance, J.K.; Ransom, E.K.; Lynch, B.M. How sedentary and physically active are breast cancer survivors, and which population subgroups have higher or lower levels of these behaviors? Support. Care Cancer 2016, 24, 2181–2190. [Google Scholar] [CrossRef]
- 2018 Physical Activity Guidelines Advisory Committee. 2018 Physical Activity Guidelines Advisory Committee Scientific Report; U.S. Department of Health and Human Services: Washington, DC, USA, 2018. [Google Scholar]
- Delrieu, L.; Vallance, J.K.; Morelle, M.; Fervers, B.; Pialoux, V.; Friedenreich, C.; Dufresne, A.; Bachelot, T.; Heudel, P.; Trédan, O.; et al. Physical activity preferences before and after participation in a 6-month physical activity intervention among women with metastatic breast cancer. Eur. J. Cancer Care 2020, 29, e13169. [Google Scholar] [CrossRef]
- Nelson, S.; Pialoux, V.; Pérol, O.; Hartman, S.; Delrieu, L.; Morelle, M.; Martin, A.; Friedenreich, C.; Febvey-Combes, O.; Pérol, D.; et al. Feasibility and health benefits of an individualized physical activity intervention in women with metastatic breast cancer: Intervention study. JMIR mHealth uHealth 2020, 8, e12306. [Google Scholar]
- Fazzino, T.L.; Fabian, C.; Befort, C.A. Change in physical activity during a weight management intervention for breast cancer survivors: Association with weight outcomes. Obesity 2017, 25, S109–S115. [Google Scholar] [CrossRef] [PubMed]
- Walker, R.K.; Hickey, A.M.; Freedson, P.S. Advantages and limitations of wearable activity trackers: Considerations for patients and clinicians. Clin. J. Oncol. Nurs. 2016, 20, 606–610. [Google Scholar] [CrossRef]
- Kenfield, S.A.; Van Blarigan, E.L.; Ameli, N.; Lavaki, E.; Cedars, B.; Paciorek, A.T.; Monroy, C.; Tantum, L.K.; Newton, R.U.; Signorell, C.; et al. Feasibility, acceptability, and behavioral outcomes from a technology-enhanced behavioral change intervention (Prostate 8): A pilot randomized controlled trial in men with prostate cancer. Eur. Urol. 2019, 75, 950–958. [Google Scholar] [CrossRef]
- Weiner, L.S.; Takemoto, M.; Godbole, S.; Nelson, S.H.; Natarajan, L.; Sears, D.D.; Hartman, S.J. Breast cancer survivors reduce accelerometer-measured sedentary time in an exercise intervention. J. Cancer Surviv. 2019, 13, 468–476. [Google Scholar] [CrossRef]
- Hartman, S.J.; Nelson, S.H.; Weiner, L.S. Patterns of Fitbit use and activity levels throughout a physical activity intervention: Exploratory analysis from a randomized controlled trial. JMIR mHealth uHealth 2018, 6, 1–11. [Google Scholar] [CrossRef]
- Lynch, B.M.; Nguyen, N.H.; Moore, M.M.; Reeves, M.M.; Rosenberg, D.E.; Boyle, T.; Milton, S.; Friedenreich, C.M.; Vallance, J.K.; English, D.R. Maintenance of physical activity and sedentary behavior change, and physical activity and sedentary behavior change after an abridged intervention: Secondary outcomes from the ACTIVATE Trial. Cancer 2019, 125, 2856–2860. [Google Scholar] [CrossRef] [PubMed]
- Lynch, B.M.; Nguyen, N.H.; Moore, M.M.; Reeves, M.M.; Rosenberg, D.E.; Boyle, T.; Vallance, J.K.; Milton, S.; Friedenreich, C.M.; English, D.R. A randomized controlled trial of a wearable technology-based intervention for increasing moderate to vigorous physical activity and reducing sedentary behavior in breast cancer survivors: The ACTIVATE Trial. Cancer 2019, 125, 2846–2855. [Google Scholar] [CrossRef]
- Mcneil, J.; Brenner, D.R.; Stone, C.R.; O’Reilly, R.; Ruan, Y.; Vallance, J.K.; Courneya, K.S.; Thorpe, K.E.; Klein, D.J.; Friedenreich, C.M. Activity tracker to prescribe various exercise intensities in breast cancer survivors. Med. Sci. Sports Exerc. 2019, 51, 930–940. [Google Scholar] [CrossRef] [PubMed]
- Rogers, L.Q.; Courneya, K.S.; Anton, P.M.; Hopkins-Price, P.; Verhulst, S.; Vicari, S.K.; Robbs, R.S.; Mocharnuk, R.; McAuley, E. Effects of the BEAT Cancer physical activity behavior change intervention on physical activity, aerobic fitness, and quality of life in breast cancer survivors: A multicenter randomized controlled trial. Breast Cancer Res. Treat. 2015, 149, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Valle, C.G.; Deal, A.M.; Tate, D.F. Preventing weight gain in African American breast cancer survivors using smart scales and activity trackers: A randomized controlled pilot study. J. Cancer Surviv. 2017, 11, 133–148. [Google Scholar] [CrossRef]
- Kokts-Porietis, R.L.; Stone, C.R.; Friedenreich, C.M.; Froese, A.; McDonough, M.; McNeil, J. Breast cancer survivors’ perspectives on a home-based physical activity intervention utilizing wearable technology. Support. Care Cancer 2019, 27, 2885–2892. [Google Scholar] [CrossRef]
- Nguyen, N.H.; Hadgraft, N.T.; Moore, M.M.; Rosenberg, D.E.; Lynch, C.; Reeves, M.M.; Lynch, B.M. A qualitative evaluation of breast cancer survivors’ acceptance of and preferences for consumer wearable technology activity trackers. Support. Care Cancer 2017, 25, 3375–3384. [Google Scholar] [CrossRef]
- Gresham, G.; Schrack, J.; Gresham, L.M.; Shinde, A.M.; Hendifar, A.E.; Tuli, R.; Rimel, B.; Figlin, R.; Meinert, C.L.; Piantadosi, S. Wearable activity monitors in oncology trials: Current use of an emerging technology. Contemp. Clin. Trials 2018, 64, 13–21. [Google Scholar] [CrossRef]
- Zeng, N.; Pope, Z.; Lee, J.E.; Gao, Z. A systematic review of active video games on rehabilitative outcomes among older patients. J. Sport Health Sci. 2017, 6, 33–43. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Rev. Esp. Nutr. Hum. Diet. 2016, 20, 148–160. [Google Scholar] [CrossRef] [PubMed]
- Pope, Z.; Zeng, N.; Gao, Z. The effects of active video games on patients’ rehabilitative outcomes: A meta-analysis. Prev. Med. 2017, 95, 38–46. [Google Scholar] [CrossRef]
- Pope, Z.; Lee, J.E.; Zeng, N.; Lee, H.Y.; Gao, Z. Feasibility of smartphone application and social media intervention on breast cancer survivors’ health outcomes. Transl. Behav. Med. 2019, 9, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Dong, X.; Yi, X.; Gao, D.; Gao, Z.; Huang, S.; Chao, M.; Ding, M. The effects of the combined exercise intervention based on internet and social media software (CEIBISMS) on quality of life, muscle strength and cardiorespiratory capacity in Chinese postoperative breast cancer patients: A randomized controlled trial. Health Qual. Life Outcomes 2019, 17, 109. [Google Scholar] [CrossRef]
- Vainshelboim, B.; Lima, R.M.; Myers, J. Cardiorespiratory fitness and cancer in women: A prospective pilot study. J. Sport Health Sci. 2019, 8, 457–462. [Google Scholar] [CrossRef]
- Joseph, R.P.; Keller, C.; Vega-López, S.; Adams, M.A.; English, R.; Hollingshead, K.; Hooker, S.P.; Todd, M.; Gaesser, G.A.; Ainsworth, B.E. A culturally relevant smartphone-delivered physical activity intervention for African American women: Development and initial usability tests of smart walk. JMIR mHealth uHealth 2020, 8, e15346. [Google Scholar] [CrossRef]
- Reeves, M.; Winkler, E.; McCarthy, N.; Lawler, S.; Eakin, E.; Healy, G. Living well after breast cancer: Changes in objectively-measured physical activity in a weight loss trial. J. Sci. Med. Sport 2012, 15, S334. [Google Scholar] [CrossRef]
- Hartman, S.J.; Ms, S.H.; Myers, E.; Natarajan, L.; Sears, D.D.; Palmer, B.W.; Ba, L.S.W.; Parker, B.A.; Patterson, R.E. Randomized controlled trial of increasing physical activity on objectively measured and self-reported cognitive functioning among breast cancer survivors: The memory & motion study. Cancer 2018, 124, 192–202. [Google Scholar] [PubMed]
- Fawcett, E.; van Velthoven, M.H.; Meinert, E. Long-term weight management using wearable technology in overweight and obese adults: Systematic review. JMIR mHealth uHealth 2020, 8, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Dong, X.; Yi, X.; Ding, M.; Gao, Z.; McDonough, D.J.; Yi, N.; Qia, W. A longitudinal study of a multicomponent exercise intervention with remote guidance among breast cancer patients. Intern. J. Environ. Res. Public Health 2020, 17, 3425. [Google Scholar] [CrossRef]
- Neil-Sztramko, S.E.; Winters-Stone, K.M.; Bland, K.A.; Campbell, K.L. Updated systematic review of exercise studies in breast cancer survivors: Attention to the principles of exercise training. Br. J. Sports Med. 2019, 53, 504–512. [Google Scholar] [CrossRef]
- Su, X.; McDonough, D.J.; Chu, H.; Quan, M.; Gao, Z. Application of network meta-analysis in the field of physical activity and health promotion. J. Sport Health Sci. 2020, 9, 511–520. [Google Scholar] [CrossRef]
- Gao, Z.; Lee, J. Emerging technology in promoting physical activity and health: Challenges and opportunities. J. Clin. Med. 2019, 8, 1830. [Google Scholar] [CrossRef] [PubMed]
- Latorre-Rojas, E.J.; Prat-Subirana, J.A.; Peirau-Terés, X.; Mas-Alòs, S.; Beltrán-Garrido, J.V.; Planas-Anzano, A. Determination of functional fitness age in women aged 50 and older. J. Sport Health Sci. 2019, 8, 267–272. [Google Scholar] [CrossRef] [PubMed]
- McDonough, D.J.; Su, X.; Gao, Z. Health wearable devices for weight and BMI reduction in individuals with overweight/obesity and chronic comorbidities: Systematic review and network meta-analysis. Br. J. Sports Med. 2021. [Google Scholar] [CrossRef]


{kind=link}
| Title | Authors (Date) | Purpose and Intervention(s) | Sample and Setting | Design/Method | Findings |
|---|---|---|---|---|---|
| Effectiveness of Combined Smartwatch and Social Media Intervention on BCS Health Outcomes: A 10-Week Pilot Randomized Trial | Pope, Zeng, Zhang, Lee, Gao (2018) [4] | Goal: To determine effectiveness of combined smartwatch and social media-based intervention on BCS health outcomes. Intervention: Smartwatch combined with Facebook (FB) social media health education interventions. | 30 middle aged BCS participants. Control group (n = 14) in FB group but did not have smartwatch, intervention group (n = 16) given Polar M400 smartwatch and in FB group. Mean age: 52.6 years old | 10-week 2 arm randomized controlled trial. Outcomes measured at baseline and after 10-week trial. Physiological, psychosocial, and quality of life (QoL) factors measured by validated instruments. Physical activity (PA), energy expenditure (EE), and steps measured by ActiGraph GT3X+ and Polar M400. Primary end point: 10 weeks | Both groups had slightly increased daily LPA, ZMVPA, EE, and steps but there was no significant difference between groups. intervention group demonstrated improved sleep quality and reduced social life limitations. There were significant group differences for social support and barriers, control group improved in both areas, intervention group had decreased social support. Several BCS found the Polar M400 difficult to use. |
| Living Well after Breast Cancer: Changes in Objectively Measured Physical Activity in a Weight Loss Trial | Reeves, Winkler, McCarthy, et al. (2012) [33] | Goal: To determine if weight loss and PA are effective in improving BCS outcomes. Intervention: Accelerometer combined with telephone-delivered weight loss intervention. | 90 overweight/obese women diagnosed with BC 9–15 months prior to study. Control group (n = 45) received usual care. Intervention group (n = 45) received behavior-focused weight loss interventions over the phone (goal >30 min MVPA per day). Mean age = 55.3 years old | Participants are from a convenience sample recruited from Queensland Cancer Registry. 6 month randomized controlled trial. GT3X+ ActiGraph measured PA at baseline and after 6-month intervention. Freedson cut-offs determined total MVPA per day. Daily lifestyle and walking/running MVPA identified using Crouter’s two-step regression. Linear mixed models used to examine intervention effects (only used for n = 983 valid days with 10+ h wear). Primary end point: 6 months | Both groups experienced significant increase in MVPA after trial, increase in MVPA was greater in intervention group than control group. Intervention significantly increased walking/running MVPA but not lifestyle MVPA. |
| A Randomized Controlled Trial of Wearable Technology-Based Intervention for Increasing Moderate to Vigorous Physical Activity and Reducing Sedentary Behavior in BCS: The ACTIVATE Trial | Lynch, Nguyen, Moore, Reeves, Rosenberg, Boyle, Vallance, Milton, Friedenreich, English. (2019) [19] | Goal: Use active smartwatch and other interventions to increase MVPA and reduce sedentary behavior in BCS. Intervention: Garmin Vivofit 2 activity tracker, behavioral feedback, goal setting, 5 telephone health coaching sessions. | 80 inactive, postmenopausal BCS who had completed primary breast cancer treatment. Control group (n = 40) had no interventions, intervention group (n = 40) had described interventions. Age: ≥50 years old | 12-week randomized controlled trial, GT3X+ ActiGraph and ActivPAL were used to measure physiological outcomes at baseline and after 12 weeks. Outcomes measured include PA and sitting and standing time. See Lynch et al. ACTIVATE methods paper for more information. Primary end point: 12 weeks | Significant change for both groups in MVPA with intervention group having greater MVPA increase. Significant change occurred in sitting time and prolonged bouts of sitting observed in both groups with intervention group having greater change from baseline. |
| Maintenance of Physical Activity and Sedentary behavior Change, and Physical Activity and Sedentary Behavior Change After an Abridged Intervention: Secondary Outcomes from the ACTIVATE Trial | Lynch, Nguyen, Moore, Reeves, Rosenberg, Boyle, Milton, Friedenreich, Vallance, English (2019) [18] | Goal: Determine if intervention from ACTIVATE trial had long lasting effects on MVPA and sedentary behavior after trial completion. Intervention: Garmin Vivofit 2, behavioral feedback, 5 telephone coaching sessions, goal setting | Participants from original trial, 80 inactive, postmenopausal BCS who had completed primary breast cancer treatment. Control group (n = 40) had no interventions, intervention group (n = 40) had described interventions. Age: ≥50 years old | MVPA and sedentary behavior were measured and compared from conclusion of 12-week trial to 12 weeks post-trial. MVPA and sedentary behavior were measured using ActiGraph and ActivPAL (worn for 7 days). Both groups received Garmin Vivofit 2 to use during post-intervention time. Linear mixed model with random effects were used to examine within-group changes in MVPA and sitting time. Primary end point: 12 weeks | 12 weeks post-trial, women in intervention group had maintained increased levels of MVPA). At 12 weeks post-trial, sitting time had increased slightly but did not return to baseline. Control group when using smartwatch increased MVPA and reduced sitting time over 12-week post-intervention period. |
| Effects of The BEAT Cancer Physical Activity Behavior Change Intervention on Physical Activity, Aerobic Fitness, and Quality of Life in BCS: a Multicenter Randomized Controlled Trial | Rogers, Courneya, Anton, et al. (2015) [21] | Goal: Determine if BEAT Cancer intervention can change BCS PA, aerobic fitness, and QoL factors. Intervention: BEAT Cancer program vs. usual care. BEAT Cancer included supervised exercise, in-person counseling, group discussion, transition to home-based exercise. | 222 post-primary treatment BCS. Control group (n = 112) did not receive intervention. Intervention group (n = 110) received BEAT Cancer program intervention. Age: 18–70 years old | 3-month randomized controlled trial. Assessments measured at baseline, after 3-month intervention, and 3 months post-intervention. Baseline measurements made with use GT3X+ accelerometer and self-reported PA submaximal treadmill test, and QoL assessment as measurements. Adjusted linear mixed-model analysis used. Primary end point: 3 months | BEAT Cancer at 3 mo. showed significant increase in weekly minutes of MVPA (accelerometer measured) and self-reported exercise. Significant increase remained at 6 mo. only for self-reported PA. BEAT Cancer groups were significantly more likely to meet PA suggested standards at both the 3- and 6-month mark. BEAT Cancer significantly improved fitness at mo. 6 and QoL at 3 and 6 mo. BEAT Cancer intervention significantly improved PA, fitness, and QoL continuing up to 3 mo. post-intervention |
| Mediators of a Physical Activity Intervention on Cognition in Breast Cancer Survivors: Evidence from a Randomized Controlled Trial | Hartman, Weiner, Nelson, et al. (2019) [7] | Goal: Determine the mechanism through which PA influences BCS cognition. Intervention: ActiGraph GT3X+ accelerometer | 87 sedentary BCS. Intervention group (n = 43) received the accelerometer and PA schedule. Control (n = 44) did not. Mean age: 57 years old | 12-week randomized controlled trial. Outcomes measured include processing speed (NIH), self-reported cognition (PROMIS), physiological and psychological function (PROMIS), plasma biomarkers. Measurements collected at baseline and after 12-week intervention. Statistical methods include linear mixed-effect model and bootstrapping. See BEAT Cancer methods paper for more information. Primary end point: 12 weeks | Exercise arm group showed significant improvement in physical functioning and reduced anxiety. Anxiety significantly mediated intervention’s effect on cognitive abilities. Physical activity does not act as a mediator. No biomarkers had changes relevant to the study. Cognitive ability/processing speed did not have any mediated effect from PA. |
| Patterns of Fitbit Use and Activity Levels Throughout a Physical Activity Intervention: Exploratory Analysis from a Randomized Controlled Trial | Hartman, Nelson, Weiner, (2018) [17] | Goal: Explore the relationship between Fitbit activity trackers and success with PA interventions based on ActiGraph and determine if these interventions are sustainable. Intervention: Fitbit One worn daily throughout entire 12-week trial; ActiGraph used to create baseline and 12-week assessment | 87 female BCS randomized into intervention and control arm groups. Control group (n = 44) did not receive a fitness tracker. Intervention group (n = 43) received Fitbit One, mobile app, website or combination thereof. Mean age: 57 years old | 12-week randomized controlled trial. Data collected at baseline and at week 12. Fitbit One was worn daily to collect the metabolic equivalent of tasks (MET) on a per-minute basis all day. ActiGraph GT3X+ worn by both groups for 7 days at beginning and end to create baseline and 12-week assessments which measured the quantity of MVPA. Participants self-reported how frequently they checked their Fitbits using 8-point Likert scale. Mixed effects ANOVA used and linear mixed effects model. Primary end point: 12 weeks | Adherence to wearing Fitbit was high (~88%). Increased adherence to wearing Fitbit associated with increased MVPA (as measured by ActiGraph). 68% participants reported looking at tracker or website 1+ times per day. Changes in MVPA were significant with the wearable fitness trackers but not significant when checking app or website. More frequent checking of Fitbit associated to smaller changes in MVPA. |
| Breast Cancer Survivors Reduce Accelerometer-measured Sedentary Time in an Exercise Intervention | Weiner, Takemoto, Godbol, et al. (2019) [16] | Goal: Assess whether tech-based PA interventions can significantly increase MVPA. Intervention: ActiGraph accelerometer | 87 BCS that were insufficiently active, were diagnosed less than 5 years prior to study enrollment, and had completed treatment. Control arm (n = 44) did not receive activity tracker while intervention arm (n = 43) did. Age: ≥21 years old | 12-week randomized controlled trial. Outcomes measured were total sedentary behavior, LPA and MVPA. Outcomes were measured at baseline and after 12-week intervention using ActiGraph GT3X+ accelerometer. Linear mixed-effect models tested effects of intervention on sedentary, LPA and MVPA, change in sedentary vs. change in MVPA, and potential relationships between outcomes and sedentary behavior. Primary end point: 12 weeks | Exercise arm had significant reduction in sedentary behavior compared to control arm. Larger MVPA increase associated to larger sedentary decrease. Women further from surgery had significantly greater sedentary reductions. No significant changes in LPA. |
| Randomized Controlled Trial of Increasing Physical Activity on Objectively Measured and Self-reported Cognitive Functioning among Breast Cancer Survivors: The Memory and Motion Study | Hartman, Nelson, Meyers, Natarajan, Sears, Palmer, Weiner, Parker, Patterson (2018) [34] | Goal: Determine if intervention in PA would benefit cognition in BCS as compared to control group. Intervention: ActiGraph GT3X+ accelerometer | 87 BCS, post-BC treatment, diagnosed at least 5 years prior to study, experiencing self-reported sedentary lifestyle or fogginess/depletion of cognitive function. Intervention group (n = 43) received accelerometer exercise intervention. Control (n = 44) did not. Age: ≥21 years old | 12-week randomized controlled trial. Outcomes measured at baseline and at 12 weeks. ActiGraph measured PA. Objective cognitive performance was measured with the NIH Cognitive Toolbox. Self-reported cognition collected using Patient-Reported Outcomes Measurement Information scales. Linear mixed-effects regression model tested intervention and cognition change. Primary end point: 12 weeks | Processing speed showed significant improvement in exercise arm. Improvement in self-reported cognition between groups was not statistically significant but were large enough to show potential differences. Participants 2+ years post-surgery had significantly greater improvement in processing speed than participants less than 2 years post-treatment. Within the intervention group, those who had greater increased physical activity showed significant improvements in both objective and self-reported cognition. |
| Preventing Weight Gain in African American Breast Cancer Survivors Using Smart Scales and Activity Trackers: A Randomized Controlled Pilot Study | Valle, Deal, Tate (2016) [22] | Goal: Determine feasibility of using smart scales and activity trackers to prevent weight gain in African American BCS. Intervention: Withings WS-30 smart scale for daily weighing that sent data to app/website, emailed lessons, feedback on objective weight. For mixed group only, Withings pulse activity tracker. | 35 AA BCS, diagnosed with stage 1–3 BC within the last 10 years, who have completed treatment, have no active cancer, and have a BMI of 20–45 kg/m3. There were two intervention groups and one control group. Group one (n = 11) received the activity tracker and other interventions. Group two (n = 13) did not receive the activity tracker, only the other interventions. The control group (n = 11) did not receive either. Age: ≥18 years old | 6 month randomized controlled trial. Online and in-person assessments were taken at baseline, 3 month, and 6-month mark. Throughout the trial, the activity tracker and scale objectively measured PA and weight. Primary end point: 6 months | Average weight loss at 6 months was −0.9% in intervention + tracker group. Average weight loss at 6 mo. was −0.2% in intervention only group. Control group gained on average +0.2%. Adherence rate to trial was very high. Daily self-weighing was perceived as positive by both intervention groups and 100% of participants recommend program to other BCS. |
| A Qualitative Evaluation of Breast Cancer Survivors’ Acceptance of and Preferences for Consumer Wearable Technology Activity Tracker | Nguyen, Hadgraft, Moore, Reeves, Rosenberg, Lynch, Reeves, Lynch (2017) [24] | Goal: Assess the usability of wearable activity trackers among postmenopausal BCS. Intervention: random selection of six trackers (Fitbit One, Jawbone Up 24, Garmin Vivofit 2, Garmin Vivosmart, Garmin Vivoactive, Polar A300). | 14 postmenopausal BCS women, stage 1–3 BC, post treatment completion at least 6 months prior. Age: ≥50 years old | Series of multiple 2-week randomized controlled trials. Women tested two or three randomly assigned trackers. The device was worn for 2 weeks with a 1-week break between wearing the next device. Each tracker had to count steps and notify the participants via a notification if they were sedentary for an extended period. Focus groups were held to interview women on perceptions and experience with each tracker. Thoughts were transcribed and grouped into themes and later analyzed statistically. Primary end point: 2 weeks | 5 primary themes -Trackers increased self-awareness and motivation -BCS confidence and comfort with wearable tech -Preferred and disliked features of WAT -Concerns related to disease -Peer support and doctor monitoring presented as activity tracker applications |
| Activity Tracker to Prescribe Various Exercise Intensities in Breast Cancer Survivors | McNeil, Brenner, Stone, et al. (2019) [20] | Goal: Determine if activity tracker can be used to effectively prescribe various PA intensities and increase PA, reduce sedentary time, improve health outcomes. Intervention: Either low or high intensity PA intervention with a PA tracker (Polar A360). | 45 BCS (survivors of stage 1–3 breast cancer) who are no longer in treatment (excluding hormone therapy), who currently take fewer than 10,000 steps per day. Intervention group one (n = 15) received low PA intervention with tracker (300 min/wk at 40–59% HR reserve). Intervention group two (n = 15) received high-intensity PA with tracker (150 min/wk at 60–80% HR reserve). Control group (n = 15) received no intervention. Age: ≥18 years old | 12-week randomized controlled trial. Measurements recorded at baseline, 12 weeks, and 24 weeks taken with ActiGraph GT3X+ trackers. Outcomes measured were sedentary time, health-related fitness, and patient-reported outcomes. Intervention groups received Polar A360 trackers. Linear mixed model used to adjust data Primary end point: 12 weeks | In high intensity group, MVPA significantly increased. In low intensity group, sedentary time significantly decreased. VO2 Max was also significantly increased at 12-week mark for both experiment groups, with the high intensity group seeing a greater increase. Changes in PA and VO2 Max were sustained at 24-week follow up but were no longer significant. |
| Article | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Total |
|---|---|---|---|---|---|---|---|---|---|---|
| Hartman et al. [34] | + | + | − | + | + | + | NA | + | − | 6 * |
| Hartman et al. [17] | + | + | + | + | + | + | + | − | − | 7 * |
| Hartman et al. [7] | + | + | − | + | + | + | − | + | − | 6 * |
| Lynch et al. [19] | + | + | − | + | + | + | + | + | − | 7 * |
| Lynch et al. [18] | + | + | − | + | + | + | + | − | − | 6 * |
| McNeil et al. [20] | + | + | − | + | + | NA | NA | NA | + | 5 * |
| Nguyen et al. [24] | + | − | + | NA | NA | − | + | − | − | 3 |
| Pope et al. [4] | + | + | − | + | + | − | NA | − | − | 4 |
| Reeves et al. [33] | + | + | − | + | + | NA | NA | − | − | 4 |
| Rogers et al. [21] | + | + | − | + | + | + | + | + | − | 7 * |
| Valle et al. [22] | + | + | − | + | + | + | + | − | − | 6 * |
| Weiner et al. [16] | + | + | + | + | + | + | NA | − | − | 6 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blount, D.S.; McDonough, D.J.; Gao, Z. Effect of Wearable Technology-Based Physical Activity Interventions on Breast Cancer Survivors’ Physiological, Cognitive, and Emotional Outcomes: A Systematic Review. J. Clin. Med. 2021, 10, 2015. https://doi.org/10.3390/jcm10092015
Blount DS, McDonough DJ, Gao Z. Effect of Wearable Technology-Based Physical Activity Interventions on Breast Cancer Survivors’ Physiological, Cognitive, and Emotional Outcomes: A Systematic Review. Journal of Clinical Medicine. 2021; 10(9):2015. https://doi.org/10.3390/jcm10092015
Chicago/Turabian StyleBlount, Daphne S., Daniel J. McDonough, and Zan Gao. 2021. "Effect of Wearable Technology-Based Physical Activity Interventions on Breast Cancer Survivors’ Physiological, Cognitive, and Emotional Outcomes: A Systematic Review" Journal of Clinical Medicine 10, no. 9: 2015. https://doi.org/10.3390/jcm10092015
APA StyleBlount, D. S., McDonough, D. J., & Gao, Z. (2021). Effect of Wearable Technology-Based Physical Activity Interventions on Breast Cancer Survivors’ Physiological, Cognitive, and Emotional Outcomes: A Systematic Review. Journal of Clinical Medicine, 10(9), 2015. https://doi.org/10.3390/jcm10092015