
Role of Different Antithrombotic Regimens after Percutaneous Left Atrial Appendage Occlusion: A Large Single Center Experience

 , , , , ,
, , , , ,  ,
,
Abstract
1. Introduction
2. Methods
- (1).
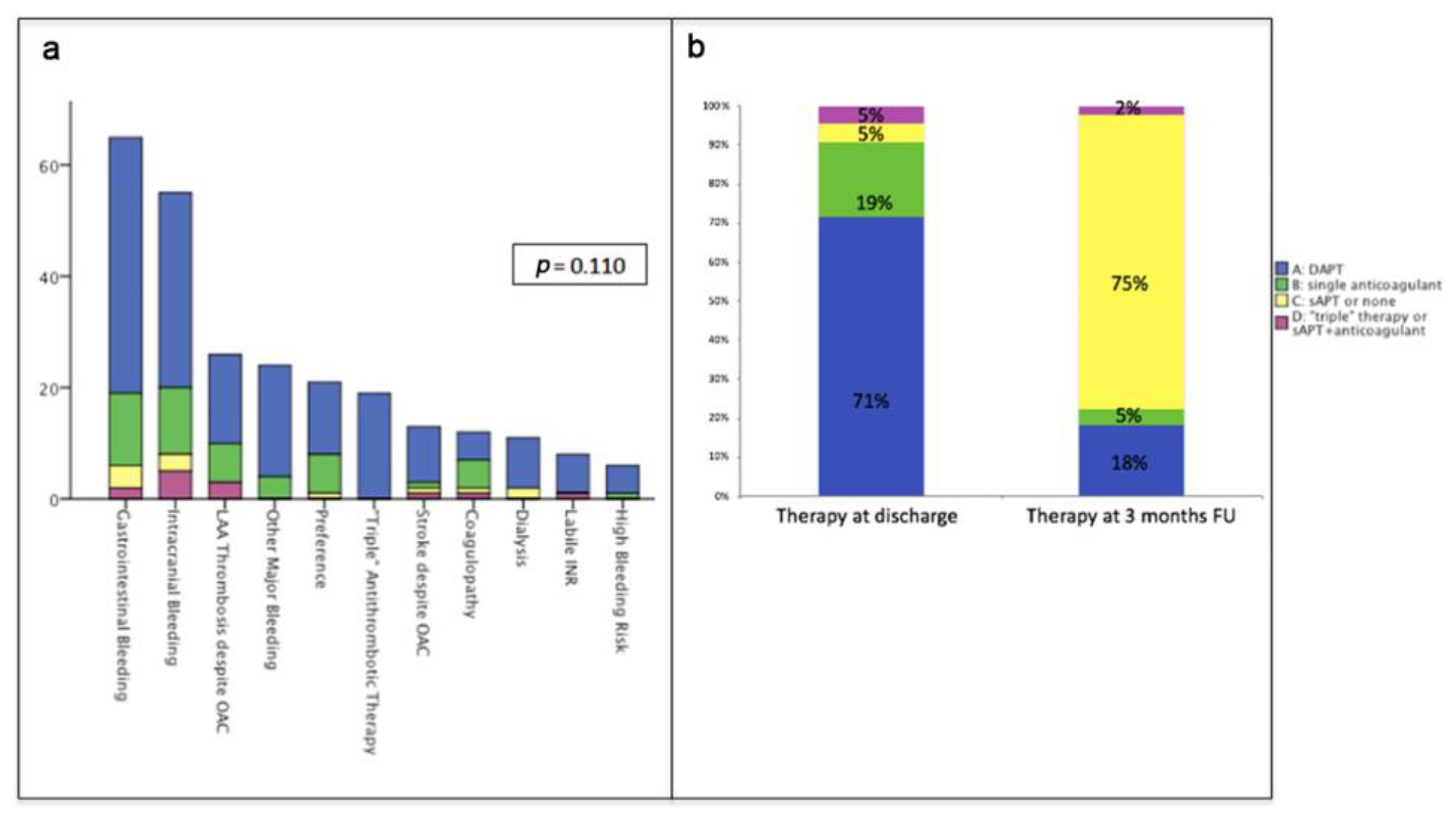
- Standard strategy was dual antiplatelet therapy (DAPT) including acetylsalicylic acid (ASS) 81-300 mg daily and clopidogrel 75 mg daily, without the administration of a loading dose. After three months, step down to single antiplatelet therapy (SAPT; usually ASS 81-300 mg daily) was recommended if follow up TEE showed absence of major leaks or device-related thrombosis. In this analysis, all patients on DAPT at discharge were summarized into group A.
- (2).
- In case of higher embolic than hemorrhagic risk (such as repeated ischemic events) and the absence of contraindications to OAC therapy, the preferred strategy was oral anticoagulation with VKA or NOACs at discharge, followed by de-escalation therapy (to DAPT or SAPT) after 3 months. Those patients were stratified into group B.
- (3).
- In case of prohibitive hemorrhagic risk (such as recent major bleeding), patients were discharged on SAPT or without any antithrombotic medication (group C)
- (4).
- A minor number of patients with an indication for both anticoagulant and antiplatelet therapy (mainly those with concomitantly treated coronary artery disease), was discharged on triple antithrombotic therapy (including OAC, ASS, and clopidogrel) or on the combination of OAC and clopidogrel. Patients with combination of OAC with ASS, clopidogrel or both were summarized into group D.
3. Results
4. Discussion
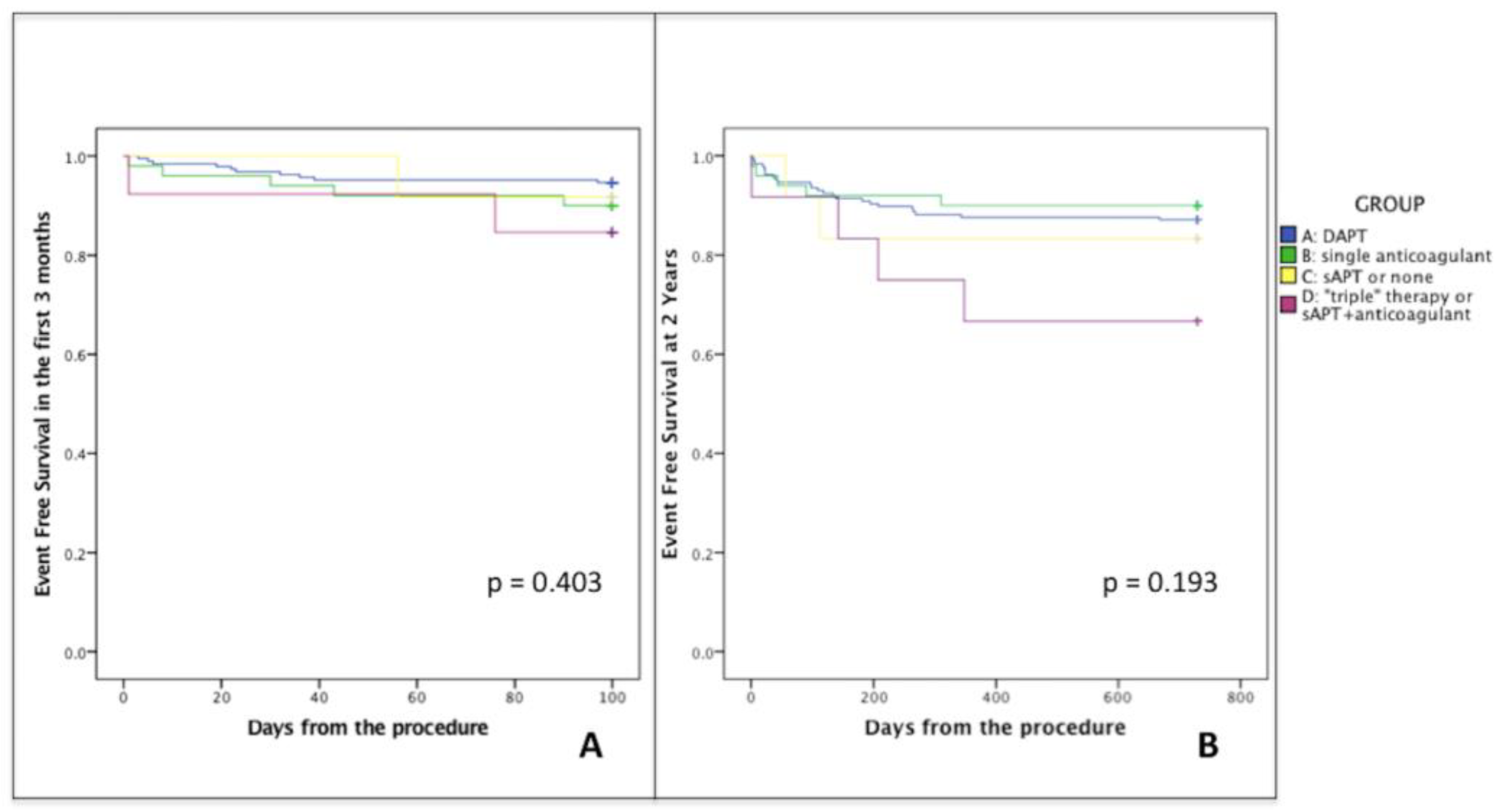
- The incidence of both hemorrhagic and ischemic events after percutaneous LAA closure was low, irrespective to chosen antithrombotic therapy. The predicted high risk (mean CHA2DS2-VASc 3.8 ± 1.7, mean HAS-BLED 3.6 ± 1.4) did not reflect in a high incidence of bleedings or embolic events.
- The majority of hemorrhagic events in our population occurred early after the procedure; actually, over 70% of bleedings happened in the first three months.
- Moreover, we observed a low rate of adverse events in the group discharged with single antiplatelet or without any therapy, and those were only bleeding events.
- First of all, the relatively small sample size and the retrospective nature of the study do not allow these data to be generalized and can only support a hypothesis generating role of the present analysis.
- Being an observational study, the choice of antithrombotic therapy was not based on a randomization but was left to the operator’s preference and usually based on ischemic and hemorrhagic risk evaluation. This led to a different distribution of patients in each group, with some differences in baseline characteristics. Our study enrolled a real-world population, which could however lead to some biases, such as missing follow-up data.
- Different LAA occlusion devices were implanted in our center. While no data support the necessity for different antithrombotic regimens, we must underline that evidences obtained from one device may not be necessarily applicable to others.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Disclosure Statement:
References
- Wolf, P.A.; Abbott, R.D.; Kannel, W.B. Atrial fibrillation as an independent risk factor for stroke: The Framingham Study. Stroke 1991, 22, 983–988. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.J.; Wolf, P.A.; Kelly-Hayes, M.; Beiser, A.S.; Kase, C.S.; Benjamin, E.J.; D’Agostino, R.B. Stroke severity in atrial fibrillation. The Framingham Study. Stroke 1996, 27, 1760–1764. [Google Scholar] [CrossRef] [PubMed]
- Hart, R.G.; Pearce, L.A.; Aguilar, M.I. Meta-analysis: Antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Ann. Intern. Med. 2007, 19, 857–867. [Google Scholar] [CrossRef] [PubMed]
- Connolly, S.J.; Ezekowitz, M.D.; Yusuf, S.; Eikelboom, J.; Oldgren, J.; Parekh, A.; Pogue, J.; Reilly, P.A.; Themeles, E.; Varrone, J.; et al. RE-LY Steering Committee and Investigators. Dabigatran versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2009, 361, 1139–1151. [Google Scholar] [CrossRef]
- Patel, M.R.; Mahaffey, K.W.; Garg, J.; Pan, G.; Singer, D.E.; Hacke, W.; Breithardt, G.; Halperin, J.L.; Hankey, G.J.; Piccini, J.P.; et al. ROCKET AF Investigators. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N. Engl. J. Med. 2011, 365, 883–891. [Google Scholar] [CrossRef] [PubMed]
- Granger, C.B.; Alexander, J.H.; McMurray, J.J.; Lopes, R.D.; Hylek, E.M.; Hanna, M.; Al-Khalidi, H.R.; Ansell, J.; Atar, D.; Avezum, A.; et al. ARISTOTLE Committees and Investigators. Apixaban versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2011, 365, 981–992. [Google Scholar] [CrossRef] [PubMed]
- Healey, J.S.; Crystal, E.; Lamy, A.; Teoh, K.; Semelhago, L.; Hohnloser, S.H.; Cybulsky, I.; Abouzahr, L.; Sawchuck, C.; Carroll, S.; et al. Left Atrial Appendage Occlusion Study (LAAOS): Results of a randomized controlled pilot study of left atrial appendage occlusion during coronary bypass surgery in patients at risk for stroke. Am. Heart J. 2005, 150, 288–293. [Google Scholar] [CrossRef] [PubMed]
- Ostermayer, S.H.; Reisman, M.; Kramer, P.H.; Matthews, R.V.; Gray, W.A.; Block, P.C.; Omran, H.; Bartorelli, A.L.; Della Bella, P.; Di Mario, C.; et al. Percutaneous left atrial appendage transcatheter occlusion (PLAATO system) to prevent stroke in high-risk patients with non-rheumatic atrial fibrillation: Results from the international multi-center feasibility trials. J. Am. Coll. Cardiol. 2005, 46, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Holmes, D.R.; Reddy, V.Y.; Turi, Z.G. Percutaneous closure of the left atrial appendage versus warfarin therapy for prevention of stroke in patients with atrial fibrillation: A randomised non-inferiority trial. Lancet 2009, 374, 534–542. [Google Scholar] [CrossRef]
- Syed, F.F.; DeSimone, C.V.; Friedman, P.A.; Asirvatham, S.J. Left atrial appendage exclusion for atrial fibrillation. Cardiol. Clin. 2014, 32, 601–625. [Google Scholar] [CrossRef] [PubMed]
- Akin, I.; Nienaber, C.A. Left atrial appendage occlusion: A better alternative to anticoagulation? World J. Cardiol. 2017, 9, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Phillips, K.P.; Paul, V. Dealing with the Left Atrial Appendage for Stroke Prevention: Devices and Decision-Making. Heart Lung Circ. 2017. [CrossRef]
- Leon, M.B.; Piazza, N.; Nikolsky, E.; Blackstone, E.H.; Cutlip, D.E.; Kappetein, A.P.; Krucoff, M.W.; Mack, M.; Mehran, R.; Miller, C.; et al. Standardized endpoint definitions for Transcatheter Aortic Valve Implantation clinical trials: A consensus report from the Valve Academic Research Consortium. J. Am. Coll. Cardiol. 2011, 57, 253–269. [Google Scholar] [CrossRef] [PubMed]
- Camm, A.J.; Lip, G.Y.; De Caterina, R.; Savelieva, I.; Atar, D.; Hohnloser, S.H.; Hindricks, G.; Kirchhof, P. ESC Committee for Practice Guidelines (CPG). 2012 focused update of the ESC Guidelines for the management of atrial fibrillation: An update of the 2010 ESC guidelines for the management of atrial fibrillation. Developed with the special contribution of the European Heart Rhythm Association. Eur. Heart J. 2012, 33, 2719–2747. [Google Scholar]
- Reddy, V.Y.; Holmes, D.; Doshi, S.K.; Neuzil, P.; Kar, S. Safety of percutaneous left atrial appendage closure: Results from the Watchman Left Atrial Appendage System for Embolic Protection in Patients with AF (PROTECT AF) clinical trial and the Continued Access Registry. Circulation 2011, 123, 417–424. [Google Scholar] [CrossRef] [PubMed]
- Holmes, D.R., Jr.; Kar, S.; Price, M.J.; Whisenant, B.; Sievert, H.; Doshi, S.K.; Huber, K.; Reddy, V.Y. Prospective randomized evaluation of the Watchman Left Atrial Appendage Closure device in patients with atrial fibrillation versus long-term warfarin therapy: The PREVAIL trial. J. Am. Coll. Cardiol. 2014, 64, 1–12. [Google Scholar] [CrossRef]
- Reddy, V.Y.; Möbius-Winkler, S.; Miller, M.A.; Neuzil, P.; Schuler, G.; Wiebe, J.; Sick, P.; Sievert, H. Left atrial appendage closure with the Watchman device in patients with a contraindication for oral anticoagulation: The ASAP study (ASA Plavix Feasibility Study With Watchman Left Atrial Appendage Closure Technology). J. Am. Coll. Cardiol. 2013, 61, 2551–2556. [Google Scholar] [CrossRef]
- Bergmann, M.W.; Betts, T.R.; Sievert, H.; Schmidt, B.; Pokushalov, E.; Kische, S.; Schmitz, T.; Meincke, F.; Stein, K.M.; Boersma, L.V.; et al. Early Anticoagulation drug regimens after WATCHMAN Left Atrial Appendage Closure: Safety and efficacy. EuroIntervention 2017. [Google Scholar] [CrossRef]
- Urena, M.; Rodés-Cabau, J.; Freixa, X.; Saw, J.; Webb, J.G.; Freeman, M.; Horlick, E.; Osten, M.; Chan, A.; Marquis, J.F.; et al. Percutaneous left atrial appendage closure with the AMPLATZER cardiac plug device in patients with nonvalvular atrial fibrillation and contraindications to anticoagulation therapy. J. Am. Coll. Cardiol. 2013, 62, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Gabella, T.; Nombela-Franco, L.; Regueiro, A.; Jiménez-Quevedo, P.; Champagne, J.; O’Hara, G.; Bernier, M.; Macaya, C.; Rodés-Cabau, J. Single Antiplatelet Therapy Following Left Atrial Appendage Closure in Patients with Contraindication to Anticoagulation. J. Am. Coll. Cardiol. 2016, 68, 1920–1921. [Google Scholar] [CrossRef] [PubMed]
- Korsholm, K.; Nielsen, K.M.; Jensen, J.M.; Jensen, H.K.; Andersen, G.; Nielsen-Kudsk, J.E. Transcatheter left atrial appendage occlusion in patients with atrial fibrillation and a high bleeding risk using aspirin alone for post-implant antithrombotic therapy. EuroIntervention 2017, 12, 2075–2082. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| OVERALL (n 260) | GROUP A (n 186) | GROUP B (n 50) | GROUP C (n 12) | GROUP D (n 12) | p Value | |
|---|---|---|---|---|---|---|
| Age, Mean ± SD | 72.7 ± 8.8 | 73 ± 8 | 73 ± 8 | 74 ± 9 | 72 ± 14 | 0.938 |
| Male, n (%) | 175 (67%) | 128 (69%) | 30 (60%) | 7 (58%) | 10 (83%) | 0.355 |
| NIDDM, n (%) | 53 (20%) | 34 (18.3%) | 11 (22%) | 6 (50%) | 2 (16.7%) | 0.117 |
| IDDM, n (%) | 22 (8.5%) | 18 (9.7%) | 3 (6%) | 1 (8.3%) | 0 | 0.603 |
| Hypertension, n (%) | 202 (77.7%) | 153 (82%) | 30 (60%) | 9 (75%) | 10 (83%) | 0.157 |
| Previous TIA, n (%) | 24 (9.2%) | 17 (9.1%) | 5 (10%) | 0 | 2 (16.7%) | 0.389 |
| Previous Stroke, n (%) | 66 (25.4%) | 44 (23.7%) | 12 (24%) | 6 (50%) | 4 (33.3%) | 0.255 |
| Previous Major Bleeding, n (%) | 147 (56.5%) | 103 (55.4%) | 31 (62%) | 8 (66.7%) | 5 (41.7%) | 0.514 |
| Congestive Heart Failure, n (%) | 74 (28.5%) | 60 (32%) | 10 (20%) | 1 (8.3%) | 3 (35%) | 0.137 |
| Coronary artery disease patients, n (%) | 84 (32%) | 71 (38%) | 4 (8%) | 2 (17%) | 7 (58%) | 0.005 |
| Ejection Fraction, Mean ± SD | 52 ± 10 | 51 ± 10 | 54 ± 9 | 58 ± 3 | 53 ± 9 | 0.05 |
| Creatinine Clearance (mL/min), Mean ± SD | 59 ± 27 | 56 ± 27 | 68 ± 29 | 59 ± 32 | 64 ± 27 | 0.07 |
| Chronic Kidney Disease, n (%) | 83 (31.9%) | 64 (34.4%) | 11 (22%) | 4 (33.3%) | 4 (33.3%) | 0.593 |
| Dialysis, n (%) | 17 (6.5%) | 14 (7.5%) | 1 (2%) | 2 (16.7%) | 0 | 0.483 |
| Hepatic Failure, n (%) | 13 (5%) | 9 (4.8%) | 2 (4%) | 2 (17%) | 0 | 0.314 |
| Labile INR, n (%) | 27 (10.4%) | 23 (12.4%) | 2 (4%) | 0 | 2 (16.7%) | 0.190 |
| CHA2DS2-VASc score, Mean ± SD | 3.8 ± 1.7 | 3.9 ± 1.7 | 3.3 ± 1.7 | 4.5 ± 1.8 | 4 ± 1.5 | 0.102 |
| HAS-BLED score, Mean ± SD | 3.6 ± 1.4 | 3.7 ± 1.4 | 3 ± 1.3 | 4.2 ± 1.3 | 3.9 ± 1.4 | 0.005 |
| OVERALL (n 260) | GROUP A (n 186) | GROUP B (n 50) | GROUP C (n 12) | GROUP D (n 12) | p Value | |
|---|---|---|---|---|---|---|
| Devices implanted, n (%): Watchman, Watchman FLX Amplatzer Amulet | 82 (31%) | 57 (30%) | 19 (38%) | 3 (25%) | 3 (25%) | 0.641 |
| 5 (2%) | 1 (0.5%) | 4 (8%) | 0 | 0 | 0.028 | |
| 55 (21%) | 44 (23%) | 2 (4%) | 5 (42%) | 4 (33%) | 0.002 | |
| 118 (45%) | 84 (45%) | 25 (50%) | 4 (33%) | 5 (42%) | 0.709 | |
| Size Change, n (%) | 5 (2%) | 4 (2.1%) | 0 | 0 | 1 (8.3%) | 0.312 |
| Repositioning, n (%) | 14 (5.4%) | 10 (5.4%) | 1 (2%) | 2 (16.7%) | 1 (8.3%) | 0.235 |
| Procedural success, n (%) | 260 (100%) | 186 (100%) | 50 (100%) | 12 (100%) | 12 (100%) | N/A |
| Events, n (%) | OVERALL (n 260) | GROUP A (n 186) | GROUP B (n 50) | GROUP C (n 12) | GROUP D (n 12) | p Value |
|---|---|---|---|---|---|---|
| Device-related thrombosis | 3 (1.2%) | 2 (1.1%) | 1 (2.1%) | 0 | 0 | 0.892 |
| Ischemic Stroke | 1 (0.4%) | 0 | 1 (2.1%) | 0 | 0 | 0.232 |
| TIA | 1 (0.4%) | 0 | 0 | 0 | 1 (9.1%) | 0.005 |
| Stroke and TIA | 2 (0.8%) | 0 | 1 (2.1%) | 0 | 1 (9.1%) | 0.07 |
| Intracranial Bleeding | 2 (0.8%) | 0 | 2 (4.2%) | 0 | 0 | 0.08 |
| Major Bleeding | 5 (2%) | 2 (1.1%) | 1 (2.1%) | 1 (8.3%) | 1 (9.1%) | 0.107 |
| Minor Bleeding | 10 (4%) | 7 (3.8%) | 3 (6.3%) | 0 | 0 | 0.655 |
| Mortality | 1 (0.4%) | 1 (0.5%) | 0 | 0 | 0 | 0.942 |
| CV Mortality | 1 (0.4%) | 1 (0.5%) | 0 | 0 | 0 | 0.942 |
| OVERALL (n 260) | GROUP A (n 186) | GROUP B (n 50) | GROUP C (n 12) | GROUP D (n 12) | p Value | |
|---|---|---|---|---|---|---|
| Clinical FU, n (%) | 253 (97.3%) | 182 (97.8%) | 48 (96%) | 12 (100%) | 11 (91.7%) | 0.508 |
| Clinical FU (days) Median (IQR) | 420 (250–704) | 434 (265–704) | 382 (197–715) | 554 (255–904) | 347 (188–595) | 0.706 |
| 3 months TEE FU, n (%) | 194 (74.6%) | 148 (79.6%) | 32 (64%) | 8(66.7%) | 6(50%) | 0.022 |
| TEE data, n (%): | ||||||
| leaks (any) | 41 (21%) | 30 (20%) | 8 (24%) | 1 (2.4%) | 2 (4.9%) | 0.753 |
| major leaks (>5 mm) | 3 (1.1%) | 1 (0.5%) | 1 (2%) | 1 (8.3%) | 0 | 0.090 |
| device related thrombosis | 4 (1.6%) | 2 (1%) | 1 (2%) | 0 | 1 (8.3%) | 0.092 |
| Events, n (%): | ||||||
| Ischemic Stroke | 5 (2%) | 3 (1.6%) | 2 (4%) | 0 | 0 | 0.926 |
| TIA | 3 (1.2%) | 0 | 1 (2%) | 0 | 2 (16.6%) | 0.005 |
| Stroke and TIA | 8 (3.1%) | 3 (1.6%) | 3 (6%) | 0 | 2 (16.6%) | 0.014 |
| Intracranial Bleeding | 3 (1.2%) | 1 (0.5%) | 2 (4%) | 0 | 0 | 0.217 |
| Major Bleeding | 7 (2.7%) | 3 (1.6%) | 1 (2%) | 2 (16.6%) | 1 (8.3%) | 0.016 |
| Minor Bleeding | 13 (5%) | 10 (5.4%) | 3 (6%) | 0 | 0 | 0.639 |
| Mortality | 15 (5.7%) | 12 (6.5%) | 0 | 0 | 3 (25%) | 0.059 |
| CV Mortality | 8 (3.1%) | 7 (3.8%) | 0 | 0 | 1 (8.3%) | 0.631 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazzone, P.; Laricchia, A.; D’Angelo, G.; Falasconi, G.; Pannone, L.; Limite, L.R.; Zweiker, D.; Regazzoli, D.; Radinovic, A.; Marzi, A.; et al. Role of Different Antithrombotic Regimens after Percutaneous Left Atrial Appendage Occlusion: A Large Single Center Experience. J. Clin. Med. 2021, 10, 1959. https://doi.org/10.3390/jcm10091959
Mazzone P, Laricchia A, D’Angelo G, Falasconi G, Pannone L, Limite LR, Zweiker D, Regazzoli D, Radinovic A, Marzi A, et al. Role of Different Antithrombotic Regimens after Percutaneous Left Atrial Appendage Occlusion: A Large Single Center Experience. Journal of Clinical Medicine. 2021; 10(9):1959. https://doi.org/10.3390/jcm10091959
Chicago/Turabian StyleMazzone, Patrizio, Alessandra Laricchia, Giuseppe D’Angelo, Giulio Falasconi, Luigi Pannone, Luca Rosario Limite, David Zweiker, Damiano Regazzoli, Andrea Radinovic, Alessandra Marzi, and et al. 2021. "Role of Different Antithrombotic Regimens after Percutaneous Left Atrial Appendage Occlusion: A Large Single Center Experience" Journal of Clinical Medicine 10, no. 9: 1959. https://doi.org/10.3390/jcm10091959
APA StyleMazzone, P., Laricchia, A., D’Angelo, G., Falasconi, G., Pannone, L., Limite, L. R., Zweiker, D., Regazzoli, D., Radinovic, A., Marzi, A., Agricola, E., Brugliera, L., Colombo, A., Della Bella, P., & Montorfano, M. (2021). Role of Different Antithrombotic Regimens after Percutaneous Left Atrial Appendage Occlusion: A Large Single Center Experience. Journal of Clinical Medicine, 10(9), 1959. https://doi.org/10.3390/jcm10091959