1. Introduction
The conventional treatment modality for edentulous maxilla is conventional dentures (CD), but for several decades, implant dentistry has been able to restore edentulous maxillae with full fixed prostheses. Implant prosthodontic treatment in the edentulous maxilla is challenging due to anatomical limitations such as reduced alveolar bone and pneumatized paranasal sinuses. Additionally, socioeconomic limitations of patients and difficulties of zygomatic implant surgeries or lateral sinus floor elevation often prevent extensive surgery in the resorptive maxilla. In such cases, clinicians may consider restoring the edentulous maxilla with implant overdentures (IOD) using a few implants without bone augmentation or additional surgeries. Goodacre et al. reported that the highest failure rate (21.3%) for any type of prosthesis is associated with maxillary IOD [
1]. This low success rate is attributed primarily to bone quality in the edentulous maxilla, since a looser arrangement of trabecular bone with a thin, or even absent cortical plate, is generally less capable of stabilizing and supporting implants [
2]. The divergent implant axis due to adverse ridge morphology in the maxilla might cause excessive prosthesis loading.
To overcome these problems, the placement of more implants and implant splinting are recommended [
3]. However, fixed prosthesis rehabilitation with sufficient implant number may require excessive surgeries and cost in maxillary edentulous patients. Therefore, the application of few splinted bar implants in IOD may be a feasible alternative [
4,
5,
6]. Maxillary bar-retained IOD have been studied extensively, and a high implant survival rate of 96.3–98.2% per year was reported in a previous study [
7].
In previous reports, the survival of IOD implants was ascribed to bar splinting [
4,
8,
9,
10,
11]. A prospective study by Naert et al. found that the cumulative survival rate (CSR) of implants was 88.6% for IOD with bar type attachments, but only 40% for IOD with either balls or magnets after a mean loading time of 6.4 years [
8]. The favorable results for bar IOD in maxillary edentulous patients were attributed to the number of implants that were rigidly splinted. However, splinting implants with a bar also introduces problems including the need for sufficient inter-occlusal space, difficulty in maintenance, un-esthetic morphology, soft tissue hyperplasia, and increased cost [
12,
13,
14,
15,
16,
17]. For fabrication of bar attachment, excellent skill and high cost are needed. Therefore, for the limitations and complications of bar fabrication in IOD, some clinicians suggest that IOD could be retained with sufficient solitary implant attachments for greater retention and support compared to CD [
18,
19,
20,
21,
22]. A study of Kenney et al. [
23] evaluated the photo elastic stress patterns produced by IODs. They found that independent solitary attachments transferred less stress to implants than the splinted bar attachments.
In a previous study, four un-splinted implants showed high short-term implant survival [
18]. Tarnow et al. reported five consecutive cases illustrating that un-splinted (solitary) maxillary implants can be used to retain maxillary IOD [
19]. These results agree with those of a 10-year study demonstrating high maxillary implant survival rates for IOD installed by both splinted and un-splinted methods using only three maxillary implants [
20]. A longitudinal prospective study [
21] of 49 patients with IOD found no significant difference in implant survival rate between IOD groups restored with ball (solitary) or round-bar attachments (bar splinted). Consequently, positive results have been reported for IOD using un-splinted implants [
22].
However, a systematic review suggested that IOD with non-splinted anchorage and ≤4 implants increased risk of implant loss [
24]. A more recent systematic review indicated that implant loss was significantly higher for maxillary IOD supported by less than four implants than for IOD supported by four implants [
25]. Boven et al. assessed the masticatory ability of splinted implants in IOD and found that it was significantly better than that of un-splinted solitary implants [
26]. IOD using un-splinted solitary implants is still controversial for maxillary edentulous patients due to implant ability to endure force in poor bone quality and quantity as well as the unfavorable biomechanics of the anterior maxillary ridge [
12,
27]. However, despite these concerns, IOD using un-splinted solitary implants might be considered as a favorable treatment with advantages of easy maintenance, less sensitive technique and lower cost. Even though there are controversies, treatment modality of IOD using un-splinted solitary implants in maxilla has been conducted and reported.
Zou et al. verified that rigid double-crown implant prostheses connected to removable dentures showed good results in fully maxillary edentulous patients and that implant survival rates of double crowns were not significantly different from bar type IOD in the maxilla [
28]. However, double-crown prostheses required expensive maintenance and showed high rates of prosthetic complications [
29]. Therefore, double-crown implant prostheses with removable dentures are not often used.
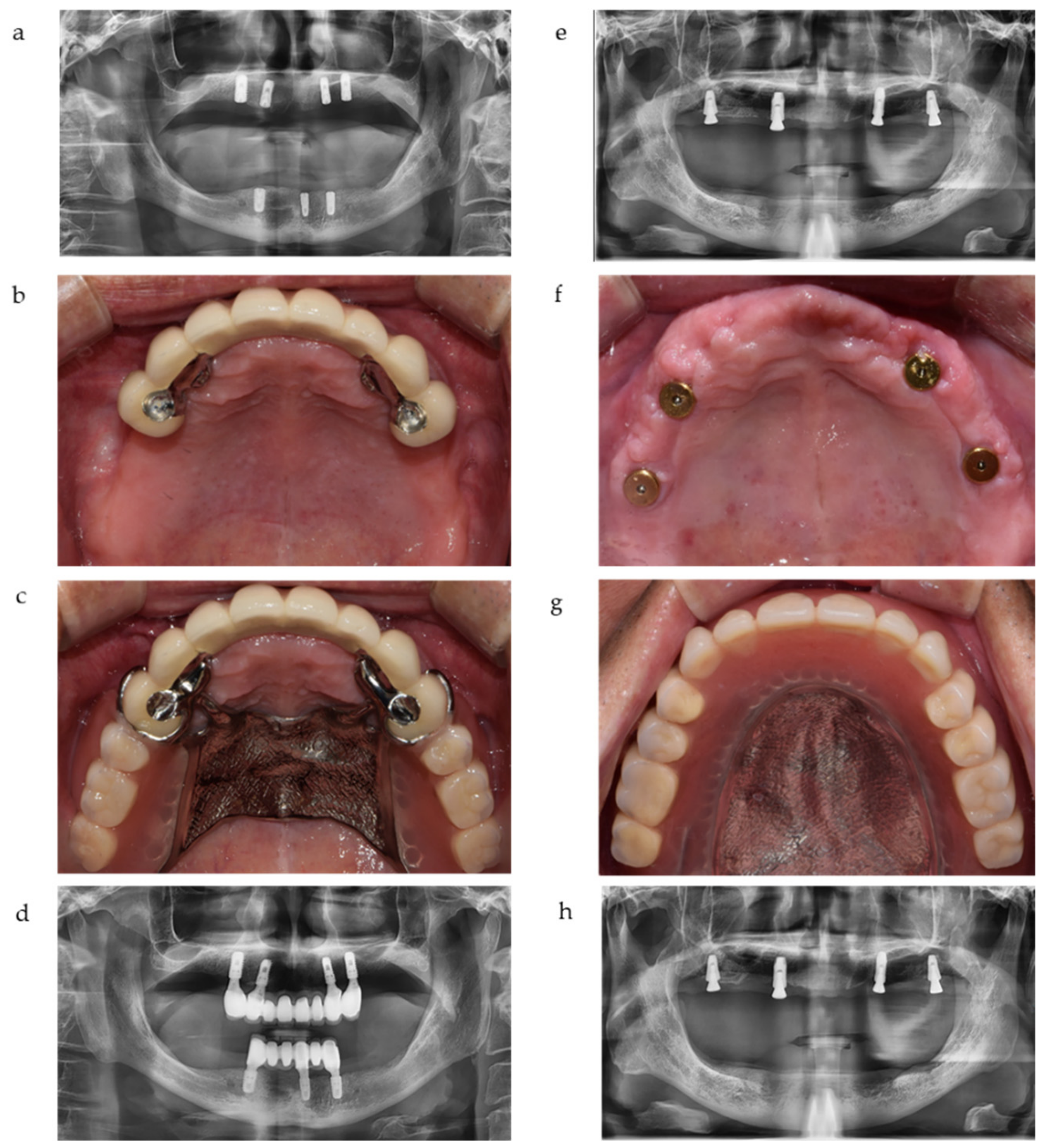
To overcome many of the problems described above, we may design a new treatment modality for maxillary edentulous patients: a combination of removable partial dentures with implant crowns. These implant crowns are surveyed for rests, retentive arms, and proximal plates of removable partial dentures (RPDs) as abutments. We define this new treatment modality as implant-crown-retained removable partial dentures (IC-RPD) in this study. By fabricating a few implant crowns and placing them at specific areas (usually canine or premolar positions) that had sufficient alveolar ridge, we could avoid extensive surgical interventions such as sinus lift, bone augmentation, or zygomatic surgery in posterior ridge of maxilla. In such cases, clinicians need only to choose the implant position where residual alveolar bone is suitable for simple implant surgery. Another edentulous area was restored with tissue supported RPD to avoid long fixed prostheses cantilever arm, which might cause unfavorable force. Additionally, the prosthodontic procedures necessary to apply surveyed crowns and RPD are well known by clinicians, therefore, treatment procedures and maintenance are relatively easy for IC-RPD.
For decades, extensive studies on implants combined with removable dentures were performed but were usually focused on IOD using ball, locator, or magnet attachments under the denture base for partially edentulous patients or fully mandibular edentulous patients. There were no long term studies of IC-RPDs for maxillary edentulous patients. By using the new concept of placing implants in strategic positions and restoring them as splinted surveyed crowns with retentive arms, implants could be made more rigid to resist loading and dislodgement in edentulous ridges by reducing the length of the free end saddle [
30]. Therefore, we investigated IC-RPDs closely as a potential new treatment modality.
In this study, we evaluated IC-RPDs and compared them to IODs in maxillary edentulous patients. Variables that influence survival and marginal bone loss (MBL) of implants such as first year pathologic condition, location of implants (anterior vs. posterior), age (older than 65 years vs. younger than 65 years), and sex were analyzed in both treatment modalities. The functional/esthetic satisfaction of patients and prosthetic complications after treatments were also observed.
4. Discussion
We investigated the survival rates and MBL of implants according to removable prostheses treatment modalities in maxillary edentulous patients. Restorations with IC-RPD or IOD in this study were determined by cost and patients’ opinions. Due to the relatively high cost of fixed prosthesis in IC-RPD compared to attachments in IOD, even though some patients wanted to restore few implants with crowns to comfort dejection, they could not choose IC-RPD but still wanted IOD for better support and retention instead of CD. Similarly, patients who wanted IC-RPD could not choose full arch fixed prostheses due to relatively high cost of fixed prostheses and need for extensive surgeries.
The overall implant survival rate of combined IC-RPD and IOD groups in this study was 84.1% (up to 147 months), which is consistent with previously reported implant survival rates of 86.3% by Fabrro et al. and 85% by Rammelsberg et al. [
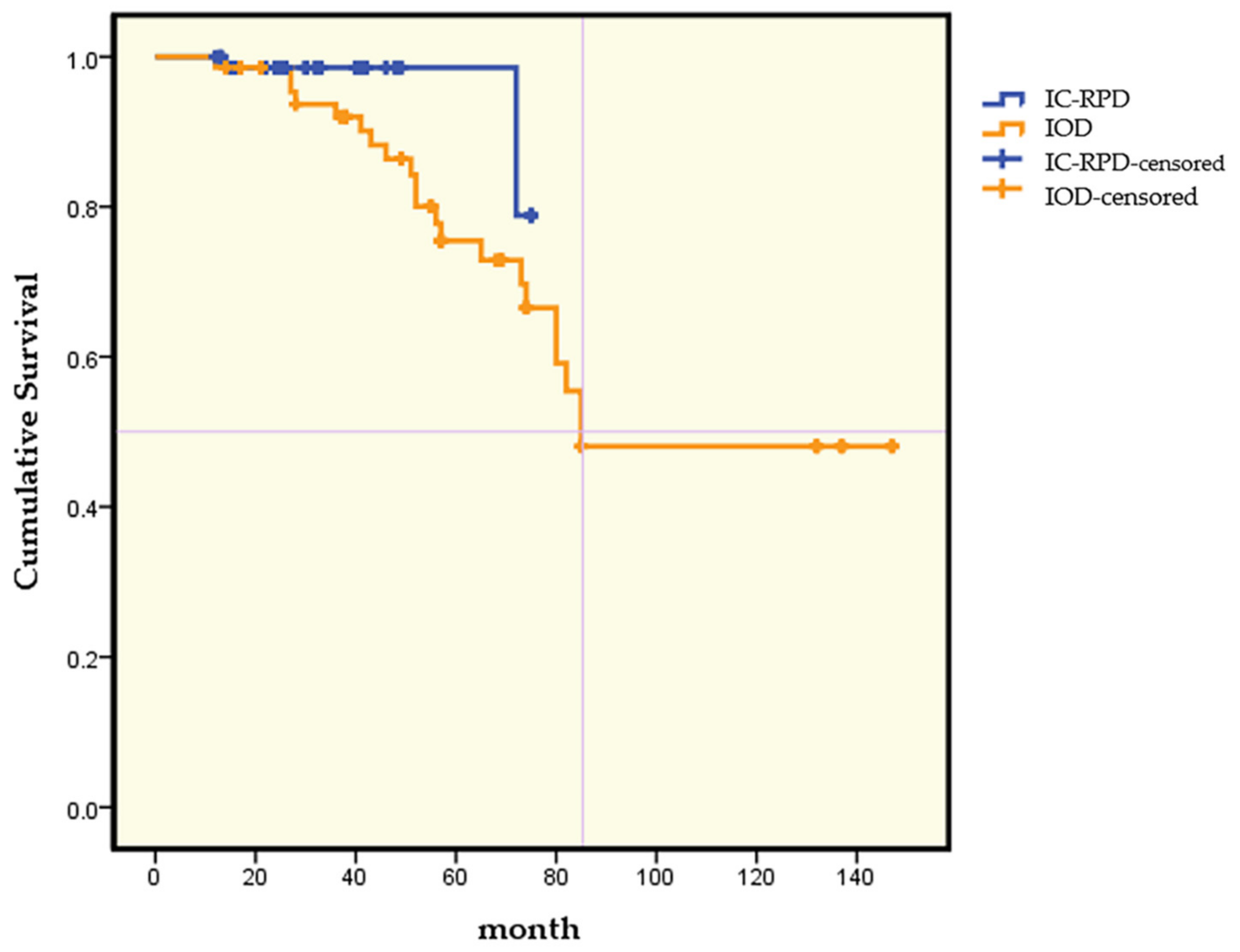
41]. There were significant differences in implant survival rates according to treatment modality: IC-RPD (97.3% during a mean 32.3 months) compared to IOD (70.4% during a mean 64.7 months), even though observation time differed according to treatment modality (
p < 0.001). The Kaplan–Meier analysis showed that in 3 years the CSR of implants was 98.6% in the IC-PRD group and 92% in the IOD group. This agrees with the results of the 2015 Clinical Oral Implants Research consensus that in the edentulous maxilla, removable prostheses with four implants were associated with high implant survival estimates at 5 years [
42]. However, after 6 years, implant CSRs in the present study decreased to much lower values, which were 78.9% for the IC-RPD group and 66.5% for the IOD group.
Maxillary trabecular bone is not naturally conducive to primary implant stability, and bone resorption patterns can create unfavorable occlusal forces. Previous studies reported that lower maxillary implant survival rates were correlated with decreased quality and quantity of bone, implant angulation that followed the resorption pattern of bone, and increased abutment length caused by thickened maxillary mucosa [
43,
44]. To increase survival rates by balancing forces, we made splinted maxillary implant crowns in the present study. Grossmann et al. recommended that implants should be splinted to improve stress distribution when they are off-axis, including during canine restoration and when remnant natural tooth stops are reduced [
45]. Therefore, our findings of significantly higher survival rates of splinted implant crowns in the IC-RPD group compared to solitary implants in the IOD group led us to hypothesize that splinting with approximate implant crowns in IC-RPD allowed implant forces to be distributed more appropriately and therefore reduced failures.
Table 4 includes specific information for failed implants in IOD. Alsrouji et al. reported severe bone resorption of premaxillary residual ridges in IOD due to the high strain and total deformation of bone under off-set force caused by the unfavorable axes of implants [
46]. Failed implants beneath the IOD of the present study showed similar characteristics, with implants placed in the premaxilla failing earlier than implants in the posterior region, even the though numbers of failed anterior and posterior implants were similar.
A previous study showed when the opposing dentitions were RPD or CD, there were no implant failures, resulting in a 100% survival rate [
47]. In the present study, all opposing dentitions were natural teeth, fixed implant prostheses, or IOD, and overall implant survival rate was 84.1%. The differences might be due to the occlusal forces.
Adell reported that the MBL of successful implants disappeared after 1 year of abutment connection, so prognosis should be assessed after 1 year, and MBL at that time was 1.2 mm [
48]. There was another suggestion that MBL of functional implants should not exceed 2 mm [
36,
37,
38]. Alberktsson et al. defined MBL of less than 1.5 mm during the first year as successful [
35]. Recommended guidelines for determining the normal range of MBL remain controversial. In this study, we defined MBL greater than 1.5 mm as pathological and affected by peri-implantitis.
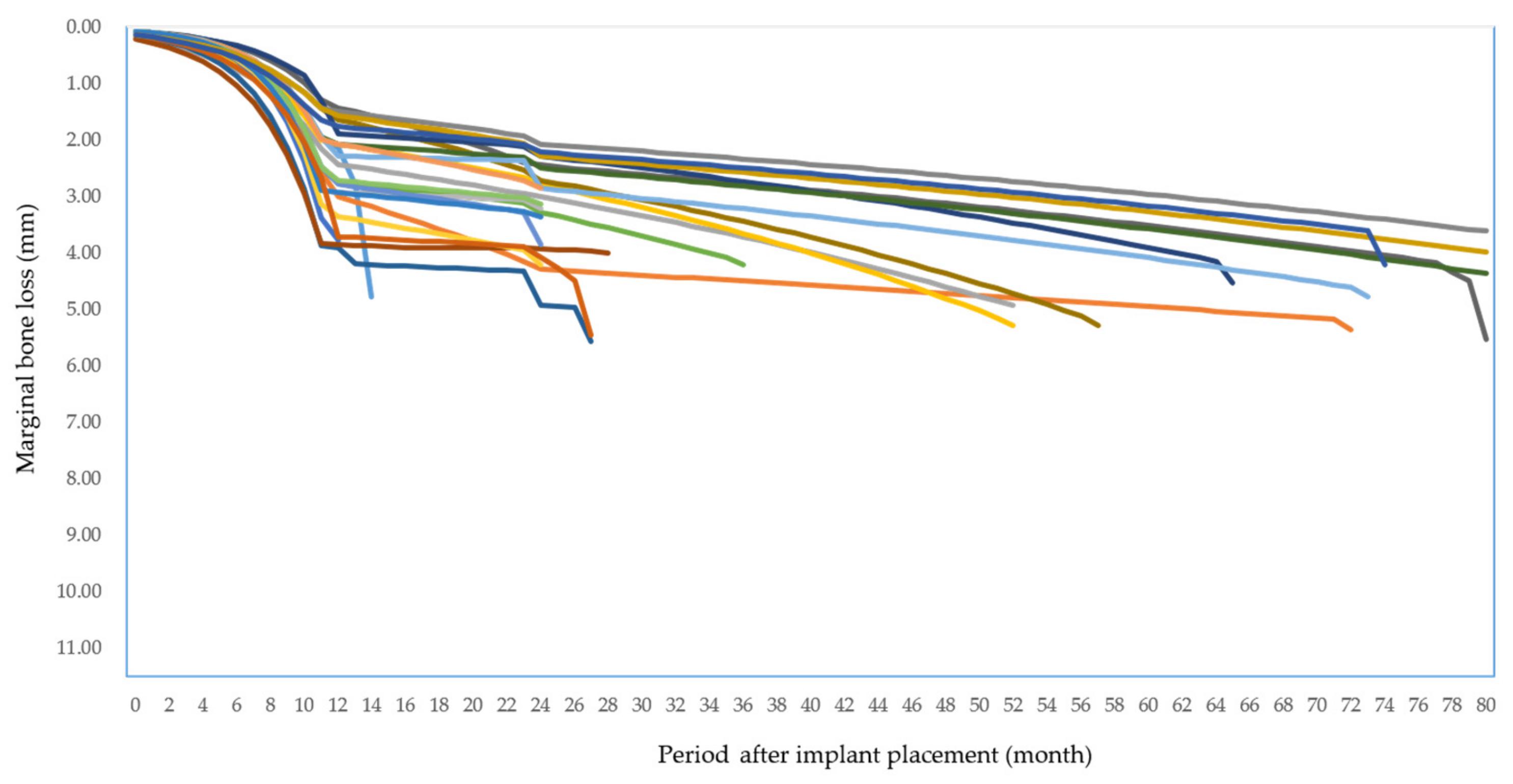
At the first year, 11% implants in the IC-RPD group and 50% of implants in the IOD group showed pathologic peri-implantitis (MBL greater than 1.5 mm with increased PD, BOP, and/or suppuration), 29.7% of 145 implants overall. MBL of implants with peri-implantitis at year 1 in IC-RPD and IOD groups showed significantly greater bone loss over time according to the post hoc T test after linear model analysis (significance level < 0.0125, or the p value of Bonferroni’s correction). We conclude that when MBL of implants with peri-implantitis at year 1 showed significantly greater bone loss they were associated with higher failure rates (p < 0.001).
In the present study, the MBL in 145 implants was 1.58 ± 1.02 mm, similar to previous studies [
49,
50]. When we compared MBL according to treatment modalities (IOD vs. IC-RPD), there was a significant difference between groups. A previous study by Bae et al. reported that the MBL around implants was significantly higher in solitary implants attached beneath IOD (1.99 ± 0.7 mm) than in splinted implants used as surveyed crowns in IC-RPD (1.44 ± 0.57 mm) [
51]. Our result was in accordance with these previous studies. The overall MBL in the IC-RPD group was significantly lower than in the IOD group (
p < 0.001). We hypothesized that the implants are connected to and fixed by splinted crowns, which reduces stress, causing micro-damage by efficiently dispersing the load generated during mastication [
52]. However, the mean observation period in the IOD group (63.4 months) was much longer than in the IC-RPD group (32.3 months), and therefore further cross-sectional studies with longer observation times are necessary.
In the present study, many cases with peri-implantitis at year 1 had common features such as immediate implant placements in narrow anterior regions or occluding dentition being natural teeth or implants. When the level of immediate implant placement was not deep enough to facilitate the bone remodeling healing process, there could be loss of bone around implants during healing of the narrowing buccal plate [
53]. If implants occluded with opposing natural teeth or implants as the only stop, excessive loading that could lead to micro fractures around implants could result in severe bone loss or failure. Therefore, for successful rehabilitation of patients treated by IC-RPD or IOD modalities, occlusal adjustment should be performed carefully while focusing on appropriate stress distribution by strategic implant positioning as well as designs intended to prevent excessive loading.
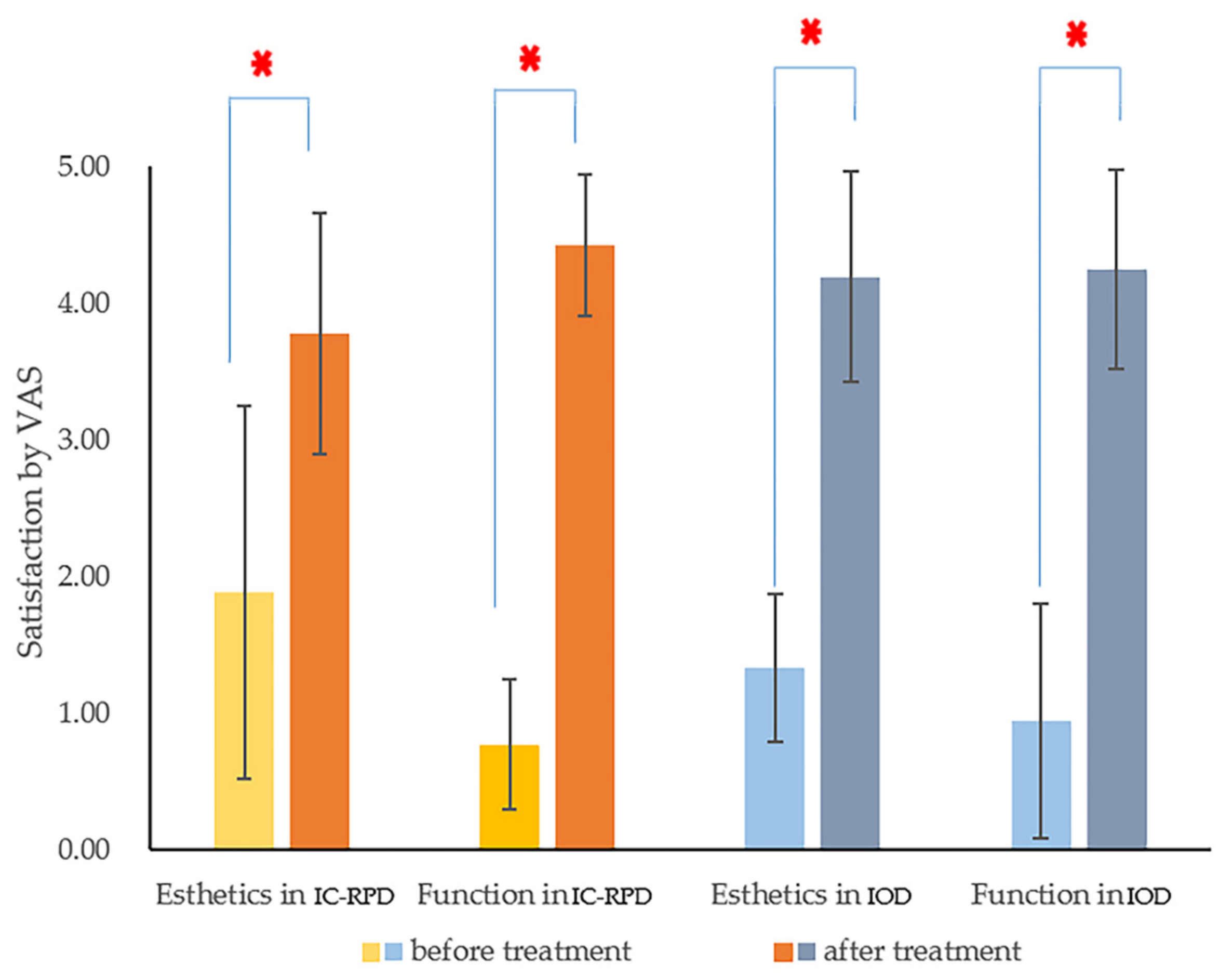
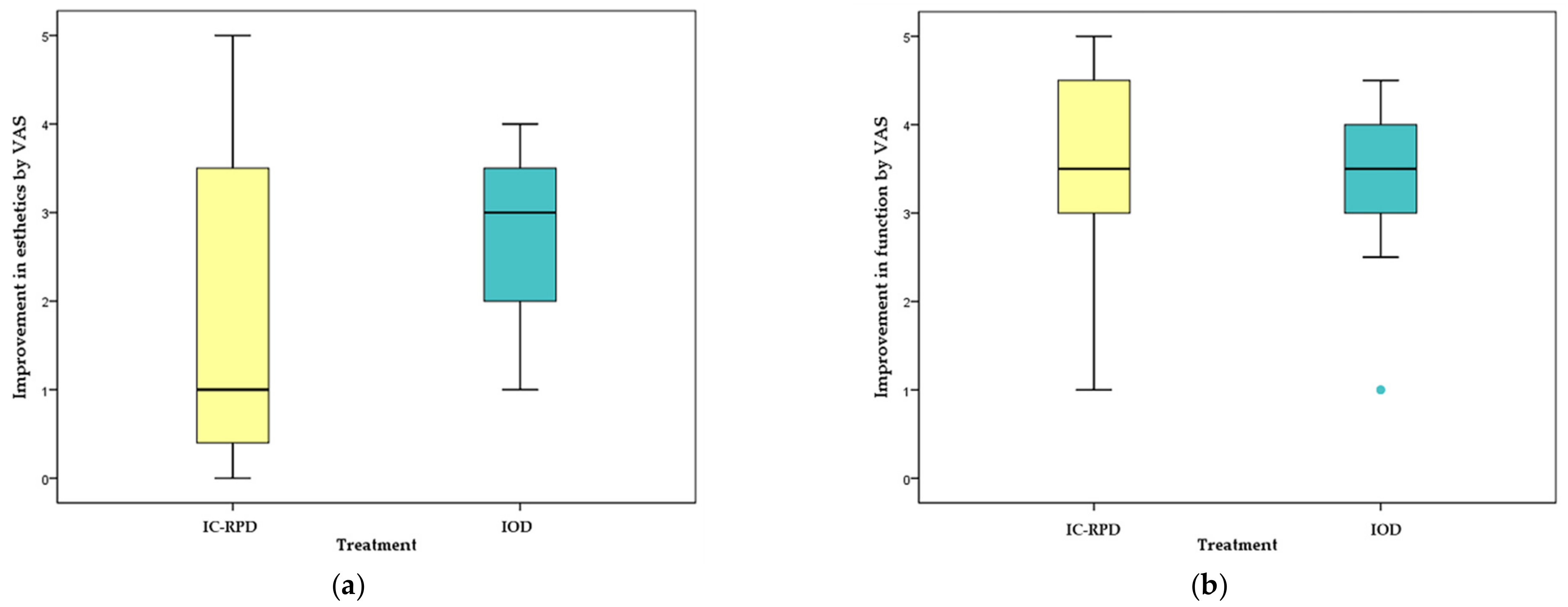
We investigated PROMs (assessing satisfaction with functional and esthetic changes after treatment) using a VAS scale at the first recall check (in most cases at 6 months). Patients were satisfied with their new implant prostheses regardless of the treatment modality and stated that they could eat better and looked younger. There was no difference between groups (IC-RPD or IOD) in functional improvement (p = 0.346), but there was a significant difference in perceived esthetic improvement (p = 0.041). Some patients were more satisfied with dentures, but the greatest increases in measurement values (differences of 5 points from 0 before treatment to 5 after treatment) for esthetics were all in the IC-RPD group among patients treated by anterior long span bridge (Br). For them, even without RPD, appearance after prosthesis placement was deemed good due to restored lip support.
Patients who received IC-RPD treatment with few implants expected their anterior teeth to be restored. However, cross arch anterior fixed prostheses could not be applied to all of these patients due to the lack of alveolar bone at the anterior position (premaxilla). When there were no implants placed at the four anterior teeth, long-span cross-arch Br with canine or premolar implant abutments were difficult to install, due to the anterior and posterior spread (AP spread) and cantilever. English et al. proposed a very reasonable rule of thumb for determining the length of cantilever, that it should be to 6–8 mm (0.7-8 fold of AP spread) due to low bone density [
54]. Khorshid et at. found that a cantilever extension to AP spread with 1:3 ratio induced the least crestal bone height loss around each implant in the maxilla [
55]. Therefore, in cases with unfavorable pre-maxillary bone, we placed implants symmetrically at only canine or premolar positions, and splinted them without anterior pontics.
Fabrication of IC-RPD might be harder than IOD. In this study, abutments for all implant surveyed crowns were manufactured in a customized manner due to the unfavorable axis followed by severe bone loss. Complicated surveying for implant crowns was also needed with poor interdental relationship because patients who had severe resorption of maxilla were indicated for IC-RPDs in this study. Resultantly, the surveyed crowns had unfavorable crown/implant ratio as well as bulged height of contour.
However, the overall frequency of mechanical complications was higher in the IOD group. In the IC-RPD group, mechanical complications included three cases of dislodgement of surveyed crowns and 19 cases of loosening of clasp arms. The dislodgement of crowns occurred because we cemented them with temporary implant cement (Premier Implant Cement, Plymouth Meeting, PA, USA.) and dislodgement occurred only when they occluded with natural teeth or implants. To address loosening of retentive arms due to repetitive insertion of dentures, we adjusted clasp arms with a utility appliance. Such complications could be resolved easily.
In IOD, most mechanical complications occurred in attachments. All attachments used in the IOD group were flat type magnets (MGT5515, Dentium Co., Seoul, Korea) because they alleviate detrimental lateral stresses to the fixture due to very low attractive horizontal forces [
56]. The influence of implant inclination on unfavorable lateral forces is limited in magnet attachment systems [
57]. Use of magnet attachments is easy due to reduced vertical dimension. Despite such advantages, in the present study, 27 magnets (44% patients in the IOD group) were re-attached beneath eight dentures and 16% of patients in the IOD group lost their attachments. In addition, 27% patients in the IOD group experienced denture base fractures that needed to be repaired in the lab. Most fractures occurred around implant attachments and we therefore hypothesized that lack of clearance due to the height of the attachment or stronger retentive and dislodging forces around the implant fulcrum affected the fracture. Other mechanical complications, e.g., screw loosening, were often observed to complicate the maintenance of IOD (
Table 8). The costs associated with maintenance of attachments in IOD are high [
58]. Among biological complications, several studies reported that implants in the IOD group also showed higher frequency of calculus deposition and clinical complications compared to implants in IC-RPD [
51,
59]. IC-RPD is easier to maintain than IOD.
The IC-RPD group had the advantage of lower decrease in retention compared to the IOD group. The retentive forces of the clasp arm can be adjusted relatively easily by the dentist, and if there is no defect in the laboratory process, no adjustments are needed for relatively long periods. However, as we found, the frequency of requirement maintenance of the implant attachment was high in the IOD group due to wear that occurs during the attachment and detachment of the denture, as well as functional load during mastication [
60].
Regarding the design of IOD, a recent systematic review concluded that a palate-less design supported by 4 to 6 implants was successful for the treatment of maxillary edentulism [
61]. However, palate-less (horse-shoe) CD designs might lead to insufficient support and retention due to the absence of the posterior palatal seal. In this study, 17 of the 18 IODs had full palatal coverage and only 1 IOD had horseshoe design at final recall check because 3 of 4 horse-shoe IODs were refabricated to full palatal coverage to improve the stress distribution to the tissue when patients started to lose implants. However, because severe MBL around implants had already occurred before the new full palatal coverage IOD was fabricated, 3 refabricated full palatal coverage IODs ended up with CD.
There are various suggestions regarding locations of implant placement for implant assisted removable prostheses. A previous study showed that implant placement in the residual alveolar ridge at the second molar decreases stresses around teeth [
62]. Yang et al. evaluated posterior implant supported fixed dental prostheses with Class IV RPD in fully maxillary edentulous patients and deemed them a good treatment option [
63]. However, posterior implant position in removable prostheses can lead to excessive forces on implants even if they decrease tissue bound movement [
64,
65,
66,
67], and in the maxilla they require additional procedures such as lateral sinus floor elevation.
Del’Arco Pignatta Cunha et al. reported that when the location of implants moved anteriorly from the molar to the premolar area, the force distribution around the abutment and tissue was more favorable [
67]. In the theoretical experimental model, as the implant moves to a more posterior position in the distal extension area, the stress on the implants and abutment teeth was increased [
68]. In the same context, previous studies found that implants located in the area of the second bicuspid were the least likely to displace the abutment tooth compared with other locations [
65,
66,
67,
69]. Another study reported the first premolar was mainly considered to improve stress distribution and retention [
70,
71,
72], while other case reports demonstrated the benefits of placing implants at the anterior region, which fulfilled the functional and esthetic requirements of the patient without jeopardizing the natural teeth [
73]. In the maxilla, posterior implant placement often entails maxillary sinus augmentation, which increases costs and surgical time. Implant placement in the premolar region without bone augmentation could be cost effective for surveyed crowns of IC-RPD.
Within the limits of this study, we demonstrated that anteriorly positioned (canine or premolar area) splinted implants used as surveyed crowns for IC-RPD yielded favorable results in severely resorptive maxilla. There are also advantages associated with transformation to fixed implant-supported restorations by adding more implants, in case patients change their minds and decide to restore edentulous ridges with fixed prostheses [
64]. And to salvage failed full arch fixed implant prostheses, IC-RPD can be a good option. With the help of implants, edentulous patients may benefit from more supportive, stable, and retentive prostheses. Therefore, clinicians should consider new treatment modalities (IC-RPD) with periodic recall checks and thorough oral hygiene (OH) instruction.










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}