
Circulating Biomarkers for the Prediction of Abdominal Aortic Aneurysm Growth

 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligible Studies
2.2. Search Strategy
2.3. Data Extraction
2.4. Quality Assessment
2.5. Definitions
2.6. Definitions Working Group
2.7. Statistical Analysis
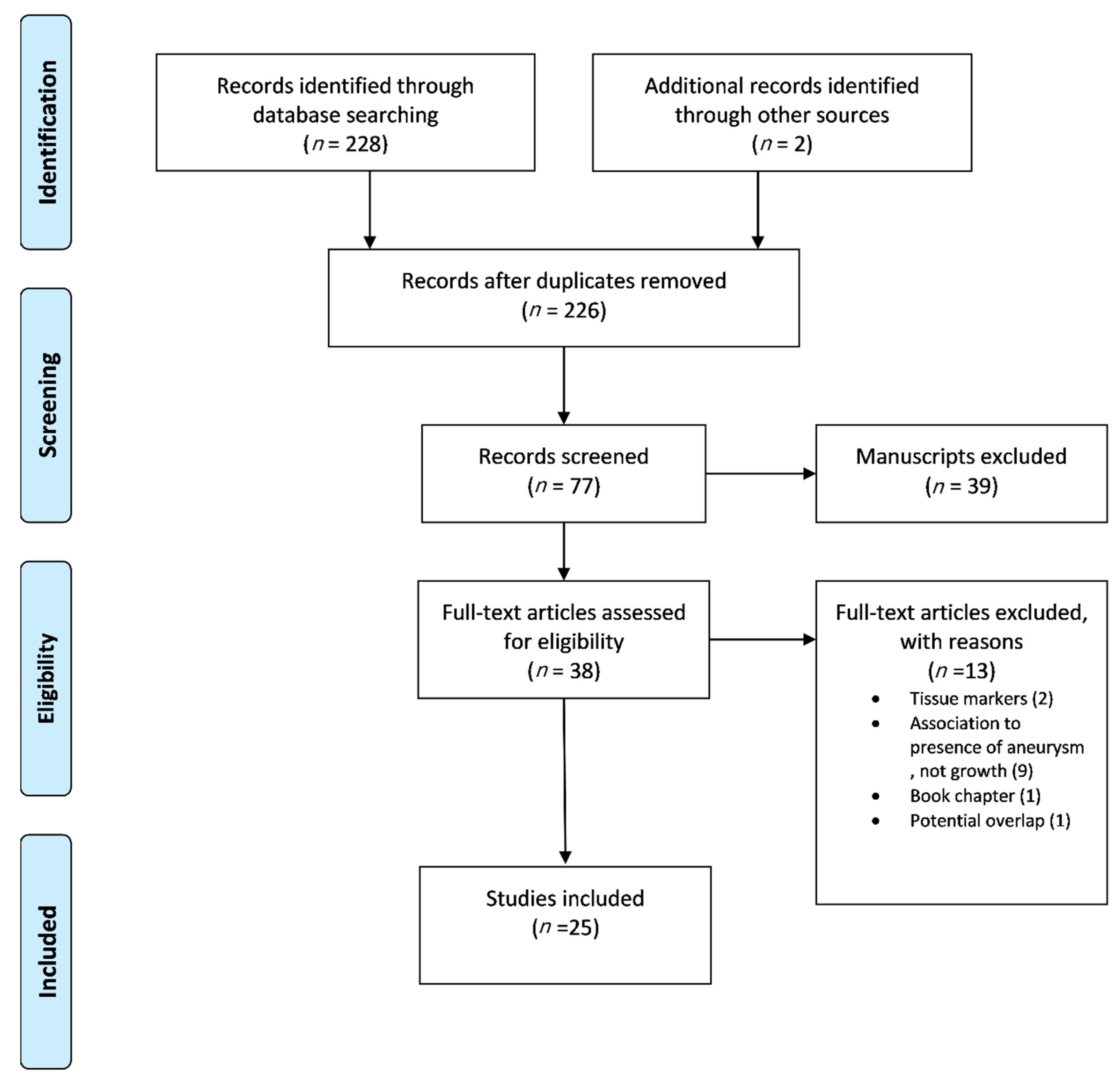
3. Results
Risk of Bias Evaluation
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Golledge, J. Abdominal aortic aneurysm: Update on pathogenesis and medical treatments. Nat. Rev. Cardiol. 2018, 16, 225–242. [Google Scholar] [CrossRef]
- Kurvers, H.; Veith, F.; Lipsitz, E.; Ohki, T.; Gargiulo, N.; Cayne, N.; Suggs, W.; Timaran, C.; Kwon, G.; Rhee, S. Discontinuous, staccato growth of abdominal aortic aneurysms. J. Am. Coll. Surg. 2004, 199, 709–715. [Google Scholar] [CrossRef]
- Olson, S.L.; Wijesinha, M.A.; Panthofer, A.M.; Blackwelder, W.C.; Upchurch, G.R.; Terrin, M.L.; Curci, J.A.; Baxter, B.T.; Matsumura, J.S. Evaluating Growth Patterns of Abdominal Aortic Aneurysm Diameter With Serial Computed Tomography Surveillance. JAMA Surg. 2021. [Google Scholar] [CrossRef] [PubMed]
- Spanos, K.; Eckstein, H.-H.; Giannoukas, A.D. Small Abdominal Aortic Aneurysms Are Not All the Same. Angiology 2019, 71, 205–207. [Google Scholar] [CrossRef]
- Forsythe, R.O.; Newby, D.E.; Robson, J.M.J. Monitoring the biological activity of abdominal aortic aneurysms beyond Ultrasound. Heart 2016, 102, 817–824. [Google Scholar] [CrossRef]
- Jalalzadeh, H.; Indrakusuma, R.; Planken, R.N.; Legemate, D.A.; Koelemay, M.J.W.; Balm, R. Inflammation as a Predictor of Abdominal Aortic Aneurysm Growth and Rupture: A Systematic Review of Imaging Biomarkers. Eur. J. Vasc. Endovasc. Surg. 2016, 56, 333–342. [Google Scholar] [CrossRef]
- Spanos, K.; Nana, P.; Kouvelos, G.; Mpatzalexis, K.; Matsagkas, M.; Giannoukas, A.D. Anatomical Differences Between Intact and Ruptured Large Abdominal Aortic Aneurysms. J. Endovasc. Ther. 2020, 27, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Wanhainen, A.; Verzini, F.; Van Herzeele, I.; Allaire, E.; Bown, M.; Cohnert, T.; Dick, F.; Van Herwaarden, J.; Karkos, C.; Koelemay, M.; et al. Editor’s Choice—European Society for Vascular Surgery (ESVS) 2019 Clinical Practice Guidelines on the Management of Abdominal Aorto-iliac Artery Aneurysms. Eur. J. Vasc. Endovasc. Surg. 2019, 57, 8–93. [Google Scholar] [CrossRef]
- Forsythe, R.O.; Newby, D.E. Imaging Biomarkers for Abdominal Aortic Aneurysms: Finding the Breakthrough. Vol. 12, Circulation: Cardiovascular Imaging. Lippincott Williams and Wilkins; 2019. Available online: https://pubmed.ncbi.nlm.nih.gov/30871335/ (accessed on 9 March 2021).
- Torres-Fonseca, M.; Galan, M.; Martinez-Lopez, D.; Cañes, L.; Roldan-Montero, R.; Alonso, J.; Rodríguez, C.; Sirvent, M.; Miguel, L.; Martínez, R.; et al. Pathophisiology of abdominal aortic aneurysm: Biomarkers and novel therapeutic targets. Clin. Investig. Arterioscler. 2019, 31, 166–177. [Google Scholar] [PubMed]
- Wanhainen, A.; Mani, K.; Golledge, J. Surrogate Markers of Abdominal Aortic Aneurysm Progression. Arter. Thromb. Vasc. Biol. 2016, 36, 236–244. [Google Scholar] [CrossRef]
- Ahmed, R.; Ghoorah, K.; Kunadian, V. Abdominal aortic aneurysms and risk factors for adverse events. Cardiol. Rev. 2016, 24, 88–93. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.A.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef]
- Howard, C. Subject and Course Guides: Evidence Based Medicine: PICO. Available online: https://researchguides.uic.edu/c.php?g=252338&p=3954402 (accessed on 5 March 2021).
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Atkinson, A.J.; Colburn, W.A.; DeGruttola, V.G.; DeMets, D.L.; Downing, G.J.; Hoth, D.F.; Oates, J.A.; Peck, C.C.; Schooley, R.; Spilker, B.; et al. Biomarkers and surrogate endpoints: Preferred definitions and conceptual framework. Clin. Pharmacol. Ther. 2001, 69, 89–95. [Google Scholar]
- Deeg, M.A.; Meijer, C.A.; Chan, L.S.; Shen, L.; Lindeman, J.H.N. Prognostic and predictive biomarkers of abdominal aortic aneurysm growth rate. Curr. Med. Res. Opin. 2016, 32, 509–517. [Google Scholar] [CrossRef]
- Vega de Céniga, M.; Esteban, M.; Quintana, J.M.; Barba, A.; Estallo, L.; de la Fuente, N.; Martin-Ventura, J.L. Search for Serum Biomarkers Associated with Abdominal Aortic Aneurysm Growth—A Pilot Study. Eur. J. Vasc. Endovasc. Surg. 2009, 37, 297–299. [Google Scholar] [CrossRef] [PubMed]
- Golledge, J.; Muller, R.; Clancy, P.; McCann, M.; Norman, P.E. Evaluation of the diagnostic and prognostic value of plasma D-dimer for abdominal aortic aneurysm. Eur. Hear. J. 2010, 32, 354–364. [Google Scholar] [CrossRef] [PubMed]
- de Ceniga, M.V.; Esteban, M.; Barba, A.; Estallo, L.; Blanco-Colio, L.M.; Martin-Ventura, J.L. Assessment of Biomarkers and Predictive Model for Short-term Prospective Abdominal Aortic Aneurysm Growth—A Pilot Study. Ann. Vasc. Surg. 2014, 28, 1642–1648. [Google Scholar] [CrossRef] [PubMed]
- Burillo, E.; Lindholt, J.S.; Molina-Sánchez, P.; Jorge, I.; Martinez-Pinna, R.; Blanco-Colio, L.M. ApoA-I/HDL-C levels are inversely associated with abdominal aortic aneurysm progression. Thromb. Haemost. 2015, 113, 1335–1346. [Google Scholar]
- Moxon, J.V.; Jones, R.E.; Norman, P.E.; Clancy, P.; Flicker, L.; Almeida, O.P.; Hankey, G.J.; Yeap, B.B.; Golledge, J. Plasma ferritin concentrations are not associated with abdominal aortic aneurysm diagnosis, size or growth. Atherosclerosis 2016, 251, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Kristensen, K.L.; Dahl, M.; Rasmussen, L.M.; Lindholt, J.S. Glycated hemoglobin is associated with the growth rate of abdominal aortic aneurysms a substudy from the VIVA (Viborg vascular) randomized screening trial. Arter. Thromb. Vasc. Biol. 2017, 37, 730–736. [Google Scholar] [CrossRef]
- Sundermann, A.C.; Saum, K.; Conrad, K.A.; Russell, H.M.; Edwards, T.L.; Mani, K.; Björck, M.; Wanhainen, A.; Owens, A.P. Prognostic value of D-dimer and markers of coagulation for stratification of abdominal aortic aneurysm growth. Blood Adv. 2018, 2, 3088–3096. [Google Scholar] [CrossRef]
- Satta, J.; Haukipuro, K.; Kairaluoma, M.I.; Juvonen, T. Aminoterminal propeptide of type III procollagen in the follow-up of patients with abdominal aortic aneurysms. J. Vasc. Surg. 1997, 25, 909–915. [Google Scholar] [CrossRef]
- Lindholt, J.; Jørgensen, B.; Shi, G.-P.; Henneberg, E. Relationships between activators and inhibitors of plasminogen, and the progression of small abdominal aortic aneurysms. Eur. J. Vasc. Endovasc. Surg. 2003, 25, 546–551. [Google Scholar] [CrossRef][Green Version]
- Golledge, J.; Muller, J.; Shephard, N.; Clancy, P.; Smallwood, L.; Moran, C.; Dear, A.E.; Palmer, L.J.; Norman, P.E. Association Between Osteopontin and Human Abdominal Aortic Aneurysm. Arter. Thromb. Vasc. Biol. 2007, 27, 655–660. [Google Scholar] [CrossRef]
- Flondell-Sité, D.; Lindblad, B.; Kölbel, T.; Gottsäter, A. Markers of Proteolysis, Fibrinolysis, and Coagulation in Relation to Size and Growth Rate of Abdominal Aortic Aneurysms. Vasc. Endovasc. Surg. 2010, 44, 262–268. [Google Scholar] [CrossRef] [PubMed]
- Wiernicki, I.; Safranow, K.; Baranowska-Bosiacka, I.; Piatek, J.; Gutowski, P. Haptoglobin 2-1 phenotype predicts rapid growth of abdominal aortic aneurysms. J. Vasc. Surg. 2010, 52, 691–696. [Google Scholar] [CrossRef]
- Martinez-Pinna, R.; Lindholt, J.; Blanco-Colio, L.; Dejouvencel, T.; Madrigal-Matute, J.; Ramos-Mozo, P.; de Ceniga, M.V.; Michel, J.; Egido, J.; Meilhac, O.; et al. Increased levels of thioredoxin in patients with abdominal aortic aneurysms (AAAs). A potential link of oxidative stress with AAA evolution. Atherosclerosis 2010, 212, 333–338. [Google Scholar] [CrossRef]
- Martín-Ventura, J.; Lindholt, J.; Moreno, J.; de Céniga, M.V.; Meilhac, O.; Michel, J.; Egido, J.; Blanco-Colio, L. Soluble TWEAK plasma levels predict expansion of human abdominal aortic aneurysms. Atherosclerosis 2011, 214, 486–489. [Google Scholar] [CrossRef]
- Lindholt, J.S.; Martin-Ventura, J.L.; Urbonavicius, S.; Ramos-Mozo, P.; Flyvbjerg, A.; Egido, J.; Frystyk, J. Insulin-like growth factor i—A novel biomarker of abdominal aortic aneurysms. Eur. J. Vasc. Endovasc. Surg. 2011, 42, 560–562. [Google Scholar] [CrossRef]
- Ramos-Mozo, P.; Madrigal-Matute, J.; de Ceniga, M.V.; Blanco-Colio, L.M.; Meilhac, O.; Feldman, L.; Michel, J.-B.; Clancy, P.; Golledge, J.; Norman, P.E.; et al. Increased plasma levels of NGAL, a marker of neutrophil activation, in patients with abdominal aortic aneurysm. Atherosclerosis 2012, 220, 552–556. [Google Scholar] [CrossRef] [PubMed]
- Ye, Z.; Austin, E.; Schaid, D.J.; Kullo, I.J. A multi-locus genetic risk score for abdominal aortic aneurysm. Atherosclerosis 2016, 246, 274–279. [Google Scholar] [CrossRef]
- Wanhainen, A.; Mani, K.; Vorkapic, E.; De Basso, R.; Björck, M.; Länne, T.; Wågsäter, D. Screening of circulating microRNA biomarkers for prevalence of abdominal aortic aneurysm and aneurysm growth. Atherosclerosis 2017, 256, 82–88. [Google Scholar] [CrossRef]
- Wang, Y.; Liu, C.L.; Lindholt, J.S.; Shi, G.P.; Zhang, J. Plasma Cystatin B Association With Abdominal Aortic Aneurysms and Need for Later Surgical Repair: A Sub-study of the VIVA Trial. Eur. J. Vasc. Endovasc. Surg. 2018, 56, 826–832. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, M.; Kuravi, S.; Hodson, J.; Rainger, G.E.; Nash, G.B.; Vohra, R.K.; Bradbury, A.W. The Relationship Between Serum Interleukin-1α and Asymptomatic Infrarenal Abdominal Aortic Aneurysm Size, Morphology, and Growth Rates. Eur. J. Vasc. Endovasc. Surg. 2018, 56, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Lindholt, J.S.; Madsen, M.; Kirketerp-Møller, K.L.; Schlosser, A.; Kristensen, K.L.; Andersen, C.B.; Sorensen, G.L. High plasma microfibrillar-associated protein 4 is associated with reduced surgical repair in abdominal aortic aneurysms. J. Vasc. Surg. 2020, 71, 1921–1929. [Google Scholar] [CrossRef] [PubMed]
- Memon, A.; Zarrouk, M.; Ågren-Witteschus, S.; Sundquist, J.; Gottsäter, A.; Sundquist, K. Identification of novel diagnostic and prognostic biomarkers for abdominal aortic aneurysm. Eur. J. Prev. Cardiol. 2020, 27, 132–142. [Google Scholar] [CrossRef]
- Eilenberg, W.; Zagrapan, B.; Bleichert, S.; Ibrahim, N.; Knöbl, V.; Brandau, A.; Martelanz, L.; Grasl, M.-T.; Hayden, H.; Nawrozi, P.; et al. Histone citrullination as a novel biomarker and target to inhibit progression of abdominal aortic aneurysms. Transl. Res. 2021. [Google Scholar] [CrossRef]
- Groeneveld, M.E.; Struik, J.A.; Musters, R.J.; Tangelder, G.J.; Koolwijk, P.; Niessen, H.W.; Hoksbergen, A.W.; Wisselink, W.; Yeung, K.K. The Potential Role of Neutrophil Gelatinase-Associated Lipocalin in the Development of Abdominal Aortic Aneurysms. Ann. Vasc. Surg. 2019, 57, 210–219. [Google Scholar] [CrossRef]
- Chaikof, E.L.; Dalman, R.L.; Eskandari, M.K.; Jackson, B.M.; Lee, W.A.; Mansour, M.A.; Mastracci, T.M.; Mell, M.; Murad, M.H.; Nguyen, L.L.; et al. The Society for Vascular Surgery practice guidelines on the care of patients with an abdominal aortic aneurysm. J. Vasc. Surg. 2018, 67, 2–77. [Google Scholar] [CrossRef]
- Lederle, F.A.; Kane, R.L.; MacDonald, R.; Wilt, T.J. Systematic review: Repair of unruptured abdominal aortic aneurysm. Ann. Intern. Med. 2007, 146, 735–741. [Google Scholar] [CrossRef]
- Cao, P.; De Rango, P.; Verzini, F.; Parlani, G.; Romano, L.; Cieri, E. Comparison of Surveillance Versus Aortic Endografting for Small Aneurysm Repair (CAESAR): Results from a Randomised Trial. Eur. J. Vasc. Endovasc. Surg. 2011, 41, 13–25. [Google Scholar] [CrossRef]
- Ouriel, K. The PIVOTAL study: A randomized comparison of endovascular repair versus surveillance in patients with smaller abdominal aortic aneurysms. J. Vasc. Surg. 2009, 49, 266–269. [Google Scholar] [CrossRef]
- Golledge, J.; Tsao, P.S.; Dalman, R.L.; Norman, P.E. Circulating Markers of Abdominal Aortic Aneurysm Presence and Progression. Circulation 2008, 118, 2382–2392. [Google Scholar] [CrossRef] [PubMed]
- Yagi, H.; Nishigori, M.; Murakami, Y.; Osaki, T.; Muto, S.; Iba, Y.; Minatoya, K.; Ikeda, Y.; Ishibashi-Ueda, H.; Morisaki, T.; et al. Discovery of novel biomarkers for atherosclerotic aortic aneurysm through proteomics-based assessment of disease progression. Sci. Rep. 2020, 10, 1–12. [Google Scholar] [CrossRef]
- Hellenthal, F.A.M.V.I.; Buurman, W.A.; Wodzig, W.K.W.H.; Schurink, G.W.H. Biomarkers of abdominal aortic aneurysm progression. Part 2: Inflammation. Nat. Rev. Cardiol. 2009, 6, 543–552. [Google Scholar] [CrossRef]
- Lindholt, J.S.; Jørgensen, B.; Fasting, H.; Henneberg, E.W. Plasma levels of plasmin-antiplasmin-complexes are predictive for small abdominal aortic aneurysms expanding to operation-recommendable sizes. J. Vasc. Surg. 2001, 34, 611–615. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Halazun, K.J.; Bofkin, K.A.; Asthana, S.; Evans, C.; Henderson, M.; Spark, J.I. Hyperhomocysteinaemia is Associated with the Rate of Abdominal Aortic Aneurysm Expansion. Eur. J. Vasc. Endovasc. Surg. 2007, 33, 391–394. [Google Scholar] [CrossRef] [PubMed]
- De Rango, P.; Farchioni, L.; Fiorucci, B.; Lenti, M. Diabetes and abdominal aortic aneurysms. Eur. J. Vasc. Endovasc. Surg. 2014, 47, 243–261. [Google Scholar] [CrossRef]
- Theivacumar, N.S.; Stephenson, M.A.; Mistry, H.; Valenti, D. Diabetes mellitus and aortic aneurysm rupture: A favorable association? Vasc. Endovasc. Surg. 2014, 48, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Dattani, N.; Sayers, R.D.; Bown, M.J. Diabetes mellitus and abdominal aortic aneurysms: A review of the mechanisms underlying the negative relationship. Diabetes Vasc. Dis. Res. 2018, 15, 367–374. [Google Scholar] [CrossRef]
- Lederle, F.A.; Johnson, G.R.; Wilson, S.E.; Chute, E.P.; Littooy, F.N.; Bandyk, D.F.; Krupski, W.C.; Barone, G.W.; Acher, C.W.; Ballard, D.J. Prevalence and Associations of Abdominal Aortic Aneurysm Detected through Screening. Ann. Intern. Med. 1997, 126, 441–449. [Google Scholar] [CrossRef]
- Dobrin, P.B. Elastin, collagen, and some mechanical aspects of arterial aneurysms. J. Vasc. Surg. 1989, 9, 396–398. [Google Scholar] [CrossRef]
- Theocharis, A.D.; Karamanos, N.K. Decreased biglycan expression and differential decorin localization in human abdominal aortic aneurysms. Atherosclerosis 2002, 165, 221–230. [Google Scholar] [CrossRef]
- Lu, H.; Aikawa, M. Many faces of matrix metalloproteinases in aortic aneurysms. Arterioscler. Thromb. Vasc. Biol. 2015, 35, 752–754. [Google Scholar] [CrossRef] [PubMed]
- Klaus, V.; Schmies, F.; Reeps, C.; Trenner, M.; Geisbüsch, S.; Lohoefer, F.; Eckstein, H.-H.; Pelisek, J. Cathepsin S is associated with degradation of collagen I in abdominal aortic aneurysm. Vasa 2018, 47, 285–293. [Google Scholar] [CrossRef]
- Lindholt, J.S.; Erlandsen, E.J.; Henneberg, E.W. Cystatin C deficiency is associated with the progression of small abdominal aortic aneurysms. BJS 2001, 88, 1472–1475. [Google Scholar] [CrossRef] [PubMed]
- Jana, S.; Hu, M.; Shen, M.; Kassiri, Z. Extracellular matrix, regional heterogeneity of the aorta, and aortic aneurysm. Exp. Mol. Med. 2019, 51, 1–15. [Google Scholar] [CrossRef]
- Paige, E.; Clément, M.; Lareyre, F.; Sweeting, M.; Raffort, J.; Grenier, C.; Finigan, A.; Harrison, J.; Peters, J.E.; Sun, B.B.; et al. Interleukin-6 Receptor Signaling and Abdominal Aortic Aneurysm Growth Rates. Circ. Genom. Precis. Med. 2019, 12, e002413. [Google Scholar] [CrossRef]
- Duellman, T.; Warren, C.L.; Matsumura, J.; Yang, J. Analysis of multiple genetic polymorphisms in aggressive-growing and slow-growing abdominal aortic aneurysms. J. Vasc. Surg. 2014, 60, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Shang, T.; Huang, C.; Yu, T.; Liu, C.; Qiao, T.; Huang, D.; Liu, Z.; Liu, C. Plasma microRNAs serve as potential biomarkers for abdominal aortic aneurysm. Clin. Biochem. 2015, 48, 988–992. [Google Scholar] [CrossRef] [PubMed]
- Kin, K.; Miyagawa, S.; Fukushima, S.; Shirakawa, Y.; Torikai, K.; Shimamura, K.; Sawa, Y. Tissue- and plasma-specific MicroRNA signatures for atherosclerotic abdominal aortic aneurysm. J. Am. Heart Assoc. 2012, 1, e000745. [Google Scholar] [CrossRef] [PubMed]
- Hauzer, W.; Witkiewicz, W.; Gnus, J. Calprotectin and Receptor for Advanced Glycation End Products as a Potential Biomarker in Abdominal Aortic Aneurysm. J. Clin. Med. 2020, 9, 927. [Google Scholar] [CrossRef]
- Hauzer, W.; Ferenc, S.; Rosińczuk, J.; Gnus, J. The Role of Serum Calprotectin as a New Marker in Abdominal Aortic Aneurysms—A Preliminary Report. Curr. Pharm. Biotechnol. 2020, 21. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author | Year of Publication | Journal | Type of Study | Number of Patients | Study Cohort |
|---|---|---|---|---|---|
| Ceniga et al. [19] | 2009 | European Journal of Vascular and Endovascular Surgery | Prospective observational (case-control) | 70 | 35 patients (AAA 30–49 mm)—35 healthy controls (AAA < 30 mm) |
| Colledge et al. [20] | 2011 | European Heart Journal | Prospective observational (case-control) | 299 | 299 patients (AAA 30–40 mm) (261; AAA 30–39 mm—38; AAA 40–49 mm) |
| Ceniga et al. [21] | 2014 | Annals of Vascular Surgery | Prospective observational (case ceries) | 96 | 96 patients (AAA 30–49 mm) |
| Burillo et al. [22] | 2015 | Thrombosis and Hemostasis | Retrospective observational (case-control) | 122 | 122 patients (AAA > 30 mm) (86; AAA 30–49 mm—36; AAA > 50 mm) |
| Moxon et al. [23] | 2016 | Atherosclerosis | Retrospective observational (case-control) | 250 | 250 Patients (AAA 30–39 mm) (65; AAA with iron overload (Ferritin > 200 ng/mL)—185 without IO) |
| Kristensen et al. [24] | 2017 | Arteriosclerosis, Thrombosis, and Vascular Biology | Retrospective observational (case-ontrol) | 319 | 319 patients (AAA 30–49 mm) (61 AAA with DM—258 without DM) |
| Deeg et al. [18] | 2016 | Current Medical Research and Opinion | Randomized controlled trial (RCT) | 93 | 93 patients (AAA 35–50 mm) (44 AAA with doxycycline—49 AAA without doxycycline) |
| Sundermann et al. [25] | 2018 | Blood Advances | Retrospective observational (case-control) | 352 | 169 patients (AAA > 25 mmm) (84 slow growing AAA, <2 mm/year, 85 fast growing AAA, >2 mm/year)—68 subaneurysmal aorta (25–29 mm)—115 healthy control (AA < 25 mm) |
| Author | Year of Publication | Journal | Type of Study | Number of Patients | Study Cohort |
|---|---|---|---|---|---|
| Satta et al. [26] | 1997 | Journal of Vascular Surgery | Prospective observational (case-control) | 139 | 139 patients with AAA under surveillance and or hospital referrals (AAA > 40 mm) |
| Lindholt et al. [27] | 2003 | European Journal of Vascular & Endovascular Surgery | Prospective observational (case series) | 70 | 70 patients from the Viborg cohort (screening program) (AAA 30–49 mm) |
| Colledge et al. [28] | 2007 | Arteriosclerosis, Thrombosis and Vascular Biology | Prospective observational (case-control) | 198 | 146 patients from the Western Australia Screening Study and 52 referrals from a tertiary hospital (AAA > 30 mm) |
| Flondell–Site et al. [29] | 2010 | Vascular and Endovascular Surgery | Prospective observational (case series) | 397 | 178 patients with AAA, referrals at the Malmo Hospital and 219 control healthy individuals |
| Wiernicki et al. [30] | 2010 | Journal of Vascular Surgery | Prospective observational (case series) | 83 | 83 patients with AAA under surveillance (AAA diameter, non-applicable) |
| Martinez–Pinna et al. [31] | 2010 | Atherosclerois (TRX) | Prospective observational (case series) | 166 | 88 patients from a Spanish screening cohort and 78 patients from the Viborg cohort (screening program) (AAA > 30 mm) |
| Martin–Ventura et al. [32] | 2011 | Atherosclerois (sTWEAK) | Prospective observational (case series) | 150 | 43 patients with AAA vs. 28 healthy controls and 79 patients from the Viborg cohort (AAA 30–49 mm) |
| Lindholt et al. [33] | 2011 | European Journal of Vascular & Endovascular Surgery (IGF) | Prospective observational (case series) | 115 | 115 patients with AAA from a screening program (AAA > 30 mm) |
| Ramos–Mozo et al. [34] | 2012 | Atherosclerois (NGAL) | Prospective observational (case series) | 100 | 100 patients with AAA under surveillance from a screening program (AAA median diameter 37.5 mm) |
| Ye et al. [35] | 2016 | Atherosclerois(SNPs) | Prospective observational (case series) | 651 | 651 patients participants in the Mayo Clinic Vascular Disease Biorepository, with AAA with at 2 least to diameter measurements on surveillance program (AAA > 30 mm or with a history of open or endovascular AAA repair) |
| Wainhanen et al. [36] | 2017 | Atherosclerois | Prospective observational (case-control) | 242 | 192 patients with AAA and 50 healthy controls from a screening program and hospital referral (AAA > 30 mm) |
| Wang et al. [37] | 2018 | European Journal of Vascular & Endovascular Surgery | Prospective observational (case-control) | 749 | 551 male patients with AAA and 198 age-matched healthy controls from the Viborg cohort (screening program) (AAA > 30 mm) |
| Ahmad et al. [38] | 2018 | European Journal of Vascular & Endovascular Surgery | Prospective observational (case series) | 97 | 97 patients—NHS referrals under surveillance for AAA (mean diameter 39 mm) |
| Groeneveld et al. [42] | 2019 | Annals of Vascular Surgery | Retrospective observational (case series) | 7 | 7 patients from hospital referrals with intact AAA (AAA diameter: Non-applicable) |
| Lindholt et al. [39] | 2020 | Journal of Vascular Surgery | Prospective observational (case-control) | 692 | 504 male patients with AAA and 188 healthy controls in the Viborg cohort (screening program) (AAA > 30 mm) |
| Memon et al. [40] | 2020 | European Journal of Preventive Cardiology | Prospective observational (case-control) | 170 | 134 patients with AAA and 136 healthy control from a screening program (AAA > 30 mm) |
| Eilenberg et al. [41] | 2021 | Translational Research | Prospective observational (case series) | 28 | 28 patients with AAA patients under surveillance from the Vienna General Hospital (AAA diameter: Non-applicable) |
| Author | Aim | Etiology | Biomarker | Method | Growth Rate Definition | Type of Imaging |
|---|---|---|---|---|---|---|
| Ceniga et al. [19] | Identification of possible association of CRP, Α1at, Lpa with AAA growth | CRP; independet risk factor for atherosclerosis, CVD, symptomatic/ruptured AAA, Α1at; conflicting data on CVD, Lpa; established role in CVD, CHD, atherothrombosis, stroke | CRP, A1at, Lpa | CRP, Lpa; immunoturbidimetric method, A1at; immunonephelometric method | Millimeter difference of maximum transverse and anteroposterior external diameters of the infrarenal aorta, perpendicular to the aortic axis, in ultrasound/CT scans taken 12 months apart (mm/year); (FUP: 1 year) | DUS (AAA 30–39 mm), CT (AAA 40–49 mm) |
| Colledge et al. [20] | Identification of possible association of D-dimers, CRP, creatinine in AAA growth | D-dimers; indicator of thrombosis-thrombolysis (DVT, CVD, AAA) | D-dimers | D-dimers: ELISA or latex-enhanced immunoassay | Millimeter difference of the greatest diameter of the infrarenal aorta in ultrasound scans every 6 or 12 months (mm/year). (Median FUP: 5.5 years) | DUS |
| Ceniga et al. [21] | Identification of possible association of various biomarkers in AAA growth rate | D-dimers; indicator of thrombosis-thrombolysis (DVT, CVD, AAA), cystatin-C; recent biomarker of CVD (MCI, stroke, HF, PAD), PAP complex; possible role in atherosclerosis | D-dimers, cystatin-C, A1at, MMP2, MMP9, myeloperoxidase, MCP-1, homocysteine, PAP complex, CRP | D-dimers; ELISA, cystatin-C; N latex cystatin C assay, PAP complex; ELISA | Millimeter difference of measured maximum outer-to-outer transverse, anteroposterior, and lateral aortic diameters, perpendicular to the aortic axis, in US/CT scans taken 12 months apart (mm/year); (FUP: 1 year) | DUS (AAA 30–39 mm), CT (AAA 40–49 mm) |
| Burillo et al. [22] | Identification of possible association of HDL-C to AAA growth | HDL-C; inversily associated with CVD, atheromatosis, atherothrombosis | HDL-C | ELISA | Millimeter difference of measured maximal perpendicular anteroposterior diameter, in US/CT scans taken 12 months apart (mm/year); mean FUP: 8.1 years | DUS (AAA 30–50 mm), CT (AAA > 50 mm) |
| Moxon et al. [23] | Identification of possible assocation between ferritin and AAA diagnosis, size, growth | Ferritin; marker of CVD, iron deposition in histologic examination of AAA | Ferritin | ELISA | Yearly AAA growth rate was calculated as a percentage of the size of the AAA in the preceding year (e.g., AAA growth rate between screening and year 1 rescan = 100 × (year 1 AAA diameter/AAA diameter at screening)-1) | DUS |
| Kristensen, et al. [24] | Identification of possible association of HbA1c to AAA growth | HbA1c; risk factor for atherosclerosis, CVD—possible protective factor in AAA pathogenesis | HbA1c | Not stated | Millimeter difference in maximal anterior-posterior AAA diameter in US scans taken 12 months apart (mm/year); mean FUP: 3.88 years | DUS |
| Deeg et al. [18] | Identification of possible association of various biomarkers in AAA growth rate between AAA patients receiving and not receiveing doxycycline | TC, LDL, biglycan; atherosclerosis and CVD association, elastin products; degradation products associated with AAA pathogenesis | Total cholesterol, ApoB, elastin DP, biglycan DP, cathrepsin S, LDL | Multi-analyte profiling technology | Millimeter difference of measured maximal anteroposterior AAA diameter, perpendicular to the blood flow, from inner-to-inner wall, in US scans taken 6–12–18 months apart (mm/month); FUP: 18 months | DUS |
| Sundermann et al. [25] | Identification of possible association of D-dimers, TAT, PF4 with AAA stratification and growth | D-dimers; indicator of thrombosis-thrombolysis (DVT, CVD, AAA), TAT; increased levels in CD, stroke, PAD, atherothrombosis, PF4; inflammatory/coagulative role in AAA thrombus | D-dimers, TAT complex, PF4 | ELISA | Millimeter difference of measured maximum AAA diameter, in US scans taken 12 months apart (mm/year); slow-growing: <2 mm/year; fast-frowing: > 2 mm/year | DUS |
| Author | Aim | Etiology | Biomarker | Method | Growth Rate Definition | Imaging |
|---|---|---|---|---|---|---|
| Satta et al. [26] | Identification of the association between serial changes in the concentration of the aminoterminal propeptide of type III procollagen (PIIINP) in serum to the rate of AAA growth | PIIINP; synthesis of type III collagen; increased turnover of in patients with AAAs when compared with patients with atherosclerotic aorto-iliac occlusive disease | Serum PIIINP | Equilibrium-type radioimmunoassays | No definition recorded in text (FUP:NA) | DUS |
| Lindholt et al. [27] | Identification of the activating pathways of plasminogen as predictors of AAA progression | tPA, IgA and CP and S-cotinine; markers of fibrinolytic function in plasma and activation of the degenerative processes in tissues-proteolysis; plasmin and antiplasmin complex (PAP) correlates with aneurysmal expansion and prediction for cases expanding to operation recommendable sizes | tPA, IgA ± CP, and S-cotinine | ELISA | Change in anterior-posterior diameter during the whole observation divided by years in annual units (FUP: 3.5 years) | DUS |
| Colledge et al. [28] | Identification of the relationship between serum osteopontin (OPN) concentrations, polymorphisms of the OPN gene, and AAA presence and growth in humans | OPN: Bone remodeling, vascular calcification, and tumor metastasis; inflammation, proteolysis, and atherosclerosis, integral processes in AAA and animal models | OPN (osteopontin) | ELISA | Maximum transverse and anteroposterior diameter measurements (FUP: 3 years) | DUS |
| Flondell–Site et al. [29] | Quantification plasma metalloproteinases (MMP)-2 and -9 and their endo-genous tissue inhibitors (TIMP-1, serpine-1, tPa-serpine-1, and the APC-PCI complex) in patients with AAA and their relationship between these markers and AAA diameter and growth | APC-PCI; physiological inhibitors of free tissue plasminogen activator (tPA) with proteolytic and fibrinolytic activity; increased concentrations of the APC-PCI complex in patients with AAA and imbalances between MMPs and their inhibitors have been reported to occur in AAA | APC-PCI (acivated C protein–protein C inhibitor), MMP-2, MMP-9, and their endo- genous tissue inhibitors, TIMP-1, serpine-1, tPa-serpine-1 | Biotrak activity assay systems, ELISA, DELFIA | Change in anterior-posterior diameter during the whole observation divided by years in annual units (FUP: 7 years) | NA |
| Wiernicki et al. [30] | Identification of the association between haptoglobin polymorphism (Hp) phenotype to AAA growth rate and assessment of serum elastase activity and markers of inflammation in patients with newly diag- nosed AAA | Hp gene; hemoglobin-binding protein expressed by a genetic polymorphism as three major phenotypes: Hp 1-1, Hp 2-1, and Hp 2-2; suppression of inflammatory responses; influences the dilatation of the abdominal aorta and probably has a direct effect on the degradation of elastin in the atherosclerotic aorta | HP (haptoglobin polymorphism) | Starch-gel electrophoresis | Growth rate identified as mm/y = max diameter at last scan- max diameter at first scan/time interval (FUP:NA) | DUS |
| Martinez–Pinna et al. [31] | Identification of thiorexodin (TRX) in conditioned media from the different layers of AAA thrombus, and in serum of patients with AAA | TRX; reactive oxygen species in inflammation and hemolysis in luminal layer of the thrombus; intracellular antioxidant enzyme elevated in CAD and intraplaque hemorrhage | Thioredoxin (TRX) | ELISA | Change in anterior-posterior diameter during the whole observation divided by years in annual units (FUP: NA) | DUS |
| Martin–Ventura et al. [32] | Identification of the association of the soluble tumor necrosis factor-like weak inducer of apoptosis (sTWEAK) with AAA growth rate | sTWEAK; cellular growth, proliferation, migration, osteoclastogenesis, angiogenesis, apoptosis; marker of CVD, CAD, carotid stenosis, and PAD that may have an association to AAA | sTWEAK (soluble tumor necrosis factor-like weak inducer of apoptosis) | ELISA | Change in anterior-posterior diameter during the whole observation divided by years in annual units (FUP: 5 years) | DUS |
| Lindholt et al. [33] | Estimation of the potential role of insulin-like growth factor I (IGF-1) and IGF-2 as biomarkers for AAA | IGF-1; mediator of CVD; vascular protective factor in AAA | Insulin-like growth factor 1 (IGF-1) and 2 (IGF-2) | Validated, in-house time-resolved immunofluorometric assays | Change in anterior-posterior diameter during the whole observation divided by years in annual units (FUP: 10 years) | DUS |
| Ramos–Mozo et al. [34] | Identification of the relationship of NGAL concentrations in the plasma of three groups of patients and related them to the presence, size and growth of AAAs | Plasma NGAL; neutrophil-derived protein during inflammation; marker of CV risk factors in asymptomatic atherosclerosis | NGAL (neutrophil gelatinase-associated lipocalin) | ELISA | NA | DUS |
| Ye et al. [35] | Association of multi-locus generic risk score (GRS) based on single nucleotide polymorphisms (SNPs) associated with AAA in genome-wide association studies (GWAS) with AAA growth prediction beyond conventional risk factors | Genome-wide association studies (GWAS); several common single nucleotide polymorphisms (SNPs); known association with AAA presence | Multi-locus GRS | Illumina Infinium Human core Exome Array, and Illumina Human 610 and 660 W Quad-v1 | Latest assessed diameter (mm)/pre-operation minus first diameter(mm)/time interval (years) (FUP: NA) | DUS, CT, MRI, DSA |
| Wainhanen et al. [36] | Associations between a wide range of micro-RNAs (miRNAs) and presence and growth of AAA | Circulating miR; 8–22 nucleotide short non-coding RNAs secreted by cells that regulate expression of target genes by interfering with transcription or inhibiting translation; associated with AAA presence (miR-155, miR-191-3p, miR-455-3p, miR-1281, and miR-411) | microRNA (miRNA) | miRCURYTM RNA isolation kit-biofluids/PCR | NA (FUP: NA) | DUS |
| Wang et al. [37] | Association of plasma cystatin B with AAA presence, size, growth rate, or need for later surgical repair | Cystatin B; marker of human malignant tumors in lipopolysaccharide (LPS) activated human blood monocytes and in interferon-g induced mouse macrophages, cystatin B deficiency in mice or loss of function mutation in humans associated with neurological dysfunction; aortic wall weakening process is mediated by proteases, including cysteinyl cathepsins, negative correlation of human plasma cystatin C levels with AAA size and annual expansion rate | Cystatin B | ELISA | Change in anterior-posterior diameter during the whole observation divided by years in annual units (FUP: 5 years) | DUS |
| Ahmad et al. [38] | Investigation of the relationship between serum interleukin (IL-1α) levels and asymptomatic infrarenal AAA growth rates, absolute size, and morphology | Il-1α; pro-inflammatory cytokine not normally detectable in the circulation in health individuals; non-specific CVD marker; marker of aortic disease related to AAA diameter | IL-1α | Boster immunoassay kit | Absolute (mm) change in maximum AP diameter and absolute (mm/year) change in maximum AP diameter over time (FUP:NA) | DUS |
| Groeneveld et al. [42] | Investigation of the role of neutrophil gelatinase-associated lipocalin (NGAL) in AAA development and rupture | NGAL; acute phase protein stored in neutrophils, diagnostic and prognostic tool for several CVD; potential prevention of metaloproteinase (MMP-9) from inactivation and aortic wall degeneration; NGAL inhibition in mice attenuation of AAA growth, protective role against apoptosis | NGAL (neutrophil gelatinase-associated lipocalin) | ELISA | NA (multiple measurements to assess the expansion rate, FUP: NA) | CT or DUS |
| Lindholt et al. [39] | Investigation of the potential role of plasma microfibrillar- associated protein 4 (pMFAP4) as a biomarker of AAA | MFAP4; factor expressed in human elastic fibers in blood vessels, induction of smooth muscle cell proliferation and migration and monocyte chemotaxis; marker of tissue remodeling-related diseases | Microfibrillar- associated protein 4 (MFAP4) | AlphaLISA | Change in anterior-posterior diameter during the whole observation divided by years in annual units (FUP: 5 years) | DUS |
| Memon et al. [40] | Identification of diagnostic and prognostic biomarkers for AAA diameter and growth | MPO, tissue-type plasminogen activator (t-PA), CSTB; proteolytic and fibrinolytic activity; pathophysiologic marker of CVDs | Myeloperoxidase (MPO), tissue- type plasminogen activator (t-PA), and cystatin-B (CSTB) | Proseek Multiplex CVD III96 × 96 panel | NA | DUS |
| Eilenberg et al. [41] | Identification of the diagnostic or prognostic role of neutrophil extracellular traps (NETs) in AAA patients | NETs; marker of excessive neutrophil activation in destruction of pathogens; marker of AAA development in a mouse model by propagating the local immune reaction in aneurysm tissue | Neutrophil extracellular traps (NETs) | ELISA | The AAA maximum diameter is measured with semi-automatic tools with mean intra- and interobserver variability ranging at 0.13 and 0.27 mm, respectively | CTA |
| Author | Association of Biomarker to Growth | Significance | Additional Information |
|---|---|---|---|
| Ceniga et al. [19] | Α1at; positive correlation with AAA growth | r = 0.55, p = 0.004 | CRP; no association, Lp(a); no association |
| Colledge et al. [20] | D-dimers; positive correlation with AAA growth: DD > 150 ng/mL -AG: 0.7 mm/DD~150–300 ng AG: 0.8/DD~300–900 ng/mL-AG: 1.3 mm/DD > 900 ng/mL-AG:1.7 mm, p < 0.001 | r = 0.39, p < 0.001 | Multiple linear regression analysis revealed significant positive associations of rank-transformed D-dimer (beta = 0.29, p, 0.001) with AAA growth |
| Ceniga et al. [21] | D-dimers; 1 ng/mL increase Growth 0.0062 mm/year b = 0.0062, β = 0.38 (95% CI 0.001–1.011) Adjusted R2 = 0.2)/cystatin-C; OR = 10.04 (CI 95% 1.18–85.73), PAP; OR = 1.004 (CI 95% 0.999–1.01) | D-dimers; p < 0.1/Cystatin-C; p < 0.05, PAP; p < 0.2 | Continuous variable: Growth rate mm/year/dichotomous variable: Stability = <2 mm/year, expansion = >2 mm/year |
| Burillo et al. [22] | HDL-C; higher HDL-C Levels associated with lower AAA growth rate | r = −0.18, p = 0.07 | |
| Moxon et al. [23] | No association | NS | |
| Kristensen et al. [24] | HbA1c; negative correlation with AAA growth: 1.8 mm/year (CI, 0.99–2.65; p < 0.000) less in HbA1c 44–77 mmol/mol vs. 28–39 mmol/mol | r = −0.177; p = 0.002) | |
| Deeg et al. [18] | Without DXC: TC, ApoB; positive correlation with AAA growth/with DXC: EP; positive correlation with AAA growth | r1 = 0.38, unadjusted p1 = 0.011, r2 = 0.41, unadjusted p2 = 0.005, r3 = 0.33, p3 = 0.031 | |
| Sundermann et al. [25] | D-dimers; b = 0.21 mm/year increase per 500 ng increase, (CI 95% 0.09–0.33)/TAT; b = 0.24 mm/year increase per 1μg/mL (95% CI 0.19–0.29)/fast/slow vs. Controls for D-dimers > 500 ng OR = 7.19 (2.9–17.83)/6.23 (2.72–14.27), fast vs. slow for TAT > 4.2 μg/mL: OR 5.37 vs. 240.02 | Continuous; p < 0.05, fast–slow; p < 0.001 | PF4; no association |
| Author | Association of Biomarker to Growth | Significance | Additional Information |
|---|---|---|---|
| Satta et al. [26] | Acceleration of AAA growth increased s-PIIINP correlation in the course of AAA disease (from 0.22–0.55) | p = 0.002 (p = 0.01 during the first year) | The correlation between thrombus changes and s-PIIINP tend to be lower than between diameter and s-PIIINP, except in the first year (p = 0.02 at the end of follow-up) |
| Lindholt et al. [27] | Positive correlation between annual expansion rate and tPA, IgA ± CP, and S-cotinine | r = 0.37-p = 0.002, r = 0.29-p = 0.006 and r = 0.24- p = 0.038, respectively | In multiple linear regression analyses adjusting for S-Cotinine, the correlation between tPA and expansion rate remained significantly correlated |
| Colledge et al. [28] | Serum OPN correlated with aortic diameter change | p < 0.001 | Adjustment for other known risk factors for aortic expansion, serum OPN predicted AAA growth (p < 0.001) |
| Flondell–Site et al. [29] | No significant correlations between levels of MMP-2 or -9, TIMP-1, serpine-1, tPa- serpine-1, or the APC-PCI complex and yearly AAA growth, TIMP-1 levels independent predictors of fatal AAA rupture | NS, only for TIMP-1; p = 0.036 | |
| Wiernicki et al. [30] | Hp 2-1 patients associated with significantly higher growth rate (3.69 [2.40] mm/y) of AAA compared with patients with Hp 2-2 (1.24 [0.79], p < 0.00001) and Hp 1-1 (1.45 [0.68], p < 0.00004) | p = 0.00001, p = 0.00004 | Hp 2-1 associated with higher serum elastase activity and CRP concentration, Hp 2-1 phenotype only independent predictor of a higher AAA growth rate in multivariate analysis |
| Martinez–Pinna et al. [31] | Spearman’s correlation coefficient between TRX and AAA-growth rate. TRX predictive of patients expanding > 2 mm/year (area under ROC curve = 0.67, 95% CI, 0.55–0.79, p = 0.01). | p = 0.03 | TRX optimal cutpoint of 30 ng/mL associated with a 62% sensitivity and specificity |
| Martin–Ventura et al. [32] | sTWEAK predictive for >2 mm/y growth rate (area under ROC curve = 0.71; 95%CI, 0.58–0.83); increase of 100 pg/mL of sTWEAK reduced risk of annual expansion rate above 2 mm by 38% (95% CI: 0.41–0.93) | p = 0.003 and p = 0.021, respectively | Inverse correlation between sTWEAK and AAA expansion rate (r = −0.263; p = 0.031 |
| Lindholt et al. [33] | Positive correlation between plasma NGAL and retrospective AAA growth (rho = 0.4, p = 0.01), significant after adjusting for other risk factors. NGAL plasma concentration weakly associated with averaged yearly AAA growth | p = 0.01 and p = 0.2, respectively | |
| Ramos–Mozo et al. [34] | Serum IGF-I correlated positively with growth rate adjustment for potential confounders | p = 0.004 | The adjusted growth rate increased by 0.53 + -0.23 mm annually between the IGF-1 tertiles (p = 0.013). Serum IGF-I level predicted cases needing later surgery (AOC: 0.63; 95% CI), no association of IGF-II and AAA growth |
| Ye et al. [35] | GRS (dichotomized by median), baseline size, diabetes, and family history associated with aneurysm growth rate (all, p < 0.05). Mean aneurysm growth rate 0.50 mm/year higher in those with GRS > median (5.78) than those with GRS median (p = 0.01), after adjustment for baseline size (p < 0.001), diabetes (p = 0.046), and family history of aortic aneurysm (p = 0.02) | p = 0.01 | |
| Wainhanen et al. [36] | 20 miRs differentially expressed between slow- and fast-growing AAAs (AUC 0.60–0.65) | p < 0.005 | Diabetes and current smoker, together with miR-335-5p and miR- 125a-5p, with AUC of 0.84 with a specificity of 70% and sensitivity of 80% |
| Wang et al. [37] | In Pearson’s correlation test, plasma cystatin B not associated with AAA growth rate | p = 0.1 | |
| Ahmad et al. [38] | No statistically significant relationship was detected between IL-1a and absolute AAA increase in maximum AP diameter (rho 1⁄4 0.127, p 1⁄4 0.214) or absolute growth rate (mm/year) (rho 1⁄4 0.123, p 1⁄4 0.230) | NS | |
| Groeneveld et al. [42] | AAA expansion rate not correlated with NGAL blood plasma (or tissue) | p = 0.34 | |
| Lindholt et al. [39] | pMFAP4 significantly inversely associated with annual aneurysmal growth rate | p = 0.0074 | No association of level of pMFAP4 in multivariate analysis |
| Memon et al. [40] | MPO, tissue-type plasminogen activator (t-PA) and CSTB levels significantly associated with AAA growth | p = 0.013, 0.016, and 0.007, respectively | MPO best prognostic value in terms of AUC (AUC, 0.71; 95% CI 0.61–0.81, with a sensitivity of 80% and specificity of 59%, higher levels of MPO (≥median) were associated with significantly faster growth of AAA median (IQR); 2.3 (2.9) mm/year) compared with lower MPO levels (median (IQR); 1.2 (1.1) mm/year) |
| Eilenberg et al. [41] | Prognostic value of citH3 ranged at AUROC = 0.707 (p = 0.015) citH3 superior to D-dimers (AUROC = 0.613, p = 0.186) | p = 0.015 | 194 ng/mL cut-off level for plasma citH3 to predict rapid progression (>2 mm/6 months) with 77% sensitivity und 64% specificity |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nana, P.; Dakis, K.; Brodis, A.; Spanos, K.; Kouvelos, G. Circulating Biomarkers for the Prediction of Abdominal Aortic Aneurysm Growth. J. Clin. Med. 2021, 10, 1718. https://doi.org/10.3390/jcm10081718
Nana P, Dakis K, Brodis A, Spanos K, Kouvelos G. Circulating Biomarkers for the Prediction of Abdominal Aortic Aneurysm Growth. Journal of Clinical Medicine. 2021; 10(8):1718. https://doi.org/10.3390/jcm10081718
Chicago/Turabian StyleNana, Petroula, Konstantinos Dakis, Alexandros Brodis, Konstantinos Spanos, and George Kouvelos. 2021. "Circulating Biomarkers for the Prediction of Abdominal Aortic Aneurysm Growth" Journal of Clinical Medicine 10, no. 8: 1718. https://doi.org/10.3390/jcm10081718
APA StyleNana, P., Dakis, K., Brodis, A., Spanos, K., & Kouvelos, G. (2021). Circulating Biomarkers for the Prediction of Abdominal Aortic Aneurysm Growth. Journal of Clinical Medicine, 10(8), 1718. https://doi.org/10.3390/jcm10081718